
Abstract
Sarcopenia is associated with adverse health outcomes. This study investigated whether skeletal muscle gene expression was associated with lean mass and grip strength in community-dwelling older men. Utilising a cross-sectional study design, lean muscle mass and grip strength were measured in 88 men aged 68–76 years. Expression profiles of 44 genes implicated in the cellular regulation of skeletal muscle were determined. Serum was analysed for circulating cytokines TNF (tumour necrosis factor), IL-6 (interleukin 6, IFNG (interferon gamma), IL1R1 (interleukin-1 receptor-1). Relationships between skeletal muscle gene expression, circulating cytokines, lean mass and grip strength were examined. Participant groups with higher and lower values of lean muscle mass (n = 18) and strength (n = 20) were used in the analysis of gene expression fold change. Expression of VDR (vitamin D receptor) [fold change (FC) 0.52, standard error for fold change (SE) ± 0.08, p = 0.01] and IFNG mRNA (FC 0.31; SE ± 0.19, p = 0.01) were lower in those with higher lean mass. Expression of IL-6 (FC 0.43; SE ± 0.13, p = 0.02), TNF (FC 0.52; SE ± 0.10, p = 0.02), IL1R1 (FC 0.63; SE ± 0.09, p = 0.04) and MSTN (myostatin) (FC 0.64; SE ± 0.11, p = 0.04) were lower in those with higher grip strength. No other significant changes were observed. Significant negative correlations between serum IL-6 (R = −0.29, p = 0.005), TNF (R = −0.24, p = 0.017) and grip strength were demonstrated. This novel skeletal muscle gene expression study carried out within a well-characterized epidemiological birth cohort has demonstrated that lower expression of VDR and IFNG is associated with higher lean mass, and lower expression of IL-6, TNF, IL1R1 and myostatin is associated with higher grip strength. These findings are consistent with a role of proinflammatory factors in mediating lower muscle strength in community-dwelling older men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sarcopenia, the loss of muscle mass and function with age, is common in both men and women over the age of 65 with the estimated UK prevalence being 4.6 and 7.9 %, respectively [1]. There are a number of adverse physical and metabolic outcomes associated with sarcopenia [2], which are increasingly relevant in the context of global population ageing. Skeletal muscle strength is partly determined by muscle mass [3]. Several mechanisms have been proposed for the age-related decline in muscle mass and strength, including a decrease in physical activity, impaired nutrition (in particular, decreased dietary intake of protein), hormonal changes, oxidative stress and denervation [4, 5]. However, the precise contribution of each of these factors is uncertain. Attention is now focusing on the cellular and molecular aetiology of the loss of skeletal muscle mass and strength.
At a cellular level, multiple cell signalling pathways execute environmental and cellular cues that determine myofiber size through protein synthesis or degradation. These include the IGF-I/AKT/mTOR and the AKT/GSK-3 signalling pathways that promote protein synthesis and the maintenance of skeletal muscle mass [6]. Pathways associated with protein catabolism mainly involve activation of NFkB (nuclear factor kB) by the inflammatory mediators TNF (tumour necrosis factor) and IL-6 (interleukin 6), among others [7]. Downstream effects of NFkB include regulation of the E3 ubiquitin ligases MAFbx (atrogin-1) and MURF-1 that are involved in muscle atrophy [8].
Other proteins such as the VDR (vitamin D receptor) and MSTN (myostatin) have been shown to influence muscle development, growth as well as atrophy [9–11]. Vitamin D deficiency is associated with muscle weakness, reduced physical performance and falls [12, 13]. VDR is responsible for transmitting the effects of vitamin D into cells, and evidence for the roles for the VDR have been derived from VDR knockout mice that are characterised by reductions in body size, impaired motor coordination, metabolic abnormalities and smaller myofibers compared with wild-type littermates [13–15]. Single nucleotide polymorphisms (SNPs) in the VDR gene have been associated with altered body composition. For example, Roth et al [16] demonstrated that older men homozygous for the FF allele of the FokI polymorphism in VDR were at risk of having reduced fat-free mass, a marker of sarcopenia.
Myostatin is a critical negative regulator of skeletal muscle growth [17] and mutations within the MSTN gene leading to a lack of mature protein in mice as well as in some species of cattle, sheep and dog, increases muscle mass [18]. In humans, elevated myostatin has been associated with muscle atrophy in critically ill patients [19], and in chronic disease e.g. HIV [20]. Increased expression of myostatin has been identified in glucocorticoid-induced muscle atrophy [21]. In vitro studies suggest that myostatin upregulates the E3 ubiquitin ligases and activity of the proteasome pathway as well as NFkB activity, with concomitant down regulation of the growth promoting IGF-1/PI3k/Akt pathway [22]. Despite the evidence presented above, the functional roles of vitamin D and myostatin in mediating skeletal muscle loss in human ageing are less clear.
There is substantial evidence linking inflammation with sarcopenia [23]. Whereas the acute inflammatory response is beneficial to muscle repair and regeneration, persisting, chronic, low grade elevation of inflammatory cytokines appears to exert an adverse impact on muscle mass and strength [7, 23–25].
Although the molecular mechanisms associated with loss of skeletal muscle mass and function have been described in rodents [26], and patterns of transcriptional changes in younger vs older adults have been studied via microarray [27], there are few studies of gene expression in healthy community-dwelling older men or women who have had detailed phenotypic characterisation. Our aim was to investigate the association between the expression of genes related to anabolism, signalling and inflammation with lean mass and grip strength in a population-based sample of community-dwelling older men participating in the Hertfordshire Sarcopenia Study (HSS) [28]. The study was restricted to men in the first instance to maximise discovery power.
Methods
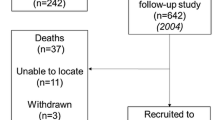
One hundred and five healthy community-dwelling older men, 68–76 years old, who participated in the UK Hertfordshire Cohort Study (HCS) [29] were prospectively recruited into this cross-sectional study (HSS) as previously described in detail [28].
The Hertfordshire Research Ethics Committee approved the study (approval number 07/Q0204/68). Each participant gave written informed consent. Investigations on participants were conducted in accordance with the principles expressed in the Declaration of Helsinki.
Data Collection
Collection and Analyses of Serum
Blood was taken from participants, processed and stored as previously described [28]. The Human Proinflammatory Ultra-Sensitive Kit, K15009C-2 (Meso-Scale Discovery, Gaithersburg, USA), an extensively validated multi-array sandwich immunoassay, was used to analyse the levels of the cytokines tumour necrosis factor (TNF), interleukin 6 (IL-6) and interferon gamma (IFNG). Levels of interleukin 1 receptor 1 (IL1R1) were analysed separately by ELISA (MBS263977, My Biosource, CA, USA). The samples were analysed in batches; quality control samples were analysed in each batch to monitor inter-assay and intra-assay precision. The coefficients of variation (%) were 5.05 (IFNG), 7.83 (TNF), 12.22 (IL-6) and 12.81 (IL1R1).
Vastus Lateralis Muscle Biopsies and TaqMan-PCR Arrays
Muscle biopsies were obtained from 99 out of 105 study participants after an overnight fast, as previously described [28]. A portion of the biopsy was snap frozen in liquid nitrogen and stored at −80 °C until further analysis.
Total RNA was extracted from TRIzol homogenates according to the manufacturer’s instructions (Invitrogen, CA, USA), and 30 ng of total RNA was used per reaction. RNA quality was tested using the ratio of absorbance at 260 and 280 nm (≥1.8 for all samples). RNA of sufficient abundance and quality was obtained from 88 participants. TaqMan RNA gene expression assays were performed using StepOnePlus systems (Applied Biosystems, Foster City, CA, USA). TaqMan® RNA-to-CT™ 1-Step Kit with standard TaqMan cycling conditions was used according to the manufacturer’s instructions (Applied Biosystems, Foster City, CA, USA). The PCR array was performed on pre-prepared 96-well array plates (Applied Biosystems, Foster City, CA, USA). Within each plate, two samples (corresponding to two individual participants) were tested for 44 genes of interest. These genes were selected based on the extensive literature pertaining to the molecular regulation of skeletal muscle [6]. Amplified cDNA was detected using SYBR green fluorescence (Applied Biosystems, Foster City, CA, USA). Expression levels measured by TaqMan RT-PCR were expressed as Ct (cycle threshold) with data output based on delta–delta Ct analyses as described by Livak et al [30]. All samples were analysed once. Duplicate (GHR and ELF-1) genes were incorporated to ensure consistency between assays. The coefficient of variation (CV) was calculated for GHR and ELF-1. If the CV was greater than 7.6 %, the values were not included in the analysis. Therefore, the means of the duplicate samples with CV of <7.6 % were used in subsequent analyses. The 44 genes and their corresponding accession numbers are presented in Table 1.
Anthropometry, Lean Mass and Grip Strength
Height in centimetres (cm) and weight in kilogrammes (kg) were measured once. Body composition was assessed by dual-energy x-ray absorptiometry (DXA) (Hologic Discovery, software version 12.5) and was performed on all participants to quantify total lean mass in kilograms. Isometric grip strength (kg) was measured three times in each hand using a standardised protocol.
Statistical Analysis
Raw data files (.txt) were visually inspected for completeness of data. Out of the genes studied, GSK3α as opposed to the usual assay standard 18s RNA, was associated with a stable expression profile with least variability and was, therefore, used as the reference gene. Raw cycle threshold (Ct) values obtained from the PCR array were normalised against GSK3α to obtain values of gene expression [delta Ct (ΔCt)]. Higher positive ΔCt values indicated lower gene expression relative to GSK3α. Normalisation of the Ct values enabled the use of the Livak method (2−ΔΔCt) [30] to calculate fold changes in gene expression in those individuals with high lean mass or muscle strength, relative to those with low lean mass or muscle strength. Higher and lower values of lean mass and grip strength were used in the subsequent analysis to calculate gene expression fold change. Smaller participant groups with extreme values of lean mass (8 participants with total lean mass ≤49.5 kg compared to 10 participants with total lean mass ≥64.2 kg) and muscle strength (8 participants with muscle strength ≤28 kg compared to 12 participants with muscle strength ≥49 kg) values were used in analyses to maximize participant contrast. Significant differences in the median delta Ct value of the two groups were determined by Mann–Whitney U tests.
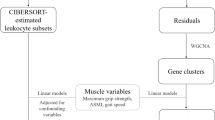
Univariate linear regression was then used on 88 participants to investigate associations between gene expression and muscle mass or grip strength. Genes used in the linear regression were standardized to a normal distribution with mean 0 and variance (1) and interpreted as z-scores. Robust variance estimators were used to account for heteroskedasticity. We also performed regression analysis adjusting for height. Principal component cluster analysis (PCCA) was used to group genes that had similar levels of gene expression [31]. Further, to identify functional themes in the gene clusters, the Database For Annotation, Visualization And Integrated Discovery (DAVID) [32] was used to identify enriched Gene Ontology terms and KEGG pathways in each cluster relative to the complete gene set background. Enriched terms and pathways were associated with both a p value and a Benjamini-corrected p value. Data were analysed using the statistical packages STATA (STATA release 11, StataCorp, Texas, USA) and SAS (version 9.1.3, SAS Institute Inc. NC, USA).
Results
Participant Characteristics
Age, height, weight, lean mass and grip strength for 88 participants in whom gene expression data were available are presented in Table 2. Mean (standard deviation, SD) participant age was 72.3 years (2.4 years), height was 174.8 cm (6.2 cm), weight 83.6 kg (12.6 kg), lean mass 57.2 kg (6.1 kg) and grip strength 39.1 kg (8.2 kg). When stratifying by lean mass, two subgroups were formed at the extremes of the data, with relatively higher [68.5 kg (4.27 kg); n = 10] or lower [47.7 kg (2.35 kg); n = 8] mean lean mass. Similarly, when stratifying by grip strength, two subgroups were identified with higher [52.9 kg (4.78 kg); n = 12] and lower [24.3 kg (2.49 kg); n = 8] mean grip strength (Table 3).
Gene Expression and Lean Mass
The vitamin D receptor (VDR) and IFNG showed lower relative gene expression in those with high lean mass (n = 10) compared with those with low lean mass (n = 8), with fold changes of 0.52 (SE ± 0.08); p = 0.01 and 0.31(SE ± 0.19); p = 0.01, respectively (Fig. 1). Using univariate regression analyses, lean mass in kg showed decreases of 1.52 kg, p = 0.005, [95 % confidence interval (CI) 0.46, 2.60] and 1.57 kg, p = 0.022, (95 % CI 0.23, 2.90) for each SD increase in IFNG and VDR expression, respectively (Table 4). Adjusting for height only marginally attenuated the associations between lean mass and both IFNG p = 0.02 (95 % CI 0.20, 2.52) and VDR p = 0.06 (95 % CI −0.06, 2.21) (Table 5).

Lean muscle mass and skeletal muscle gene expression. Lower fold change in muscle mRNA expression of the vitamin D receptor (VDR) and interferon gamma (IFNG) in men with high lean mass (n = 10) compared to those with low lean mass (n = 8). Values are expressed as 2−ΔΔCt normalised to GSK3α. Bars represent standard error (SE) for fold change. **Significantly different from those with lower lean mass, p = 0.01
Gene expression and grip strength
The genes for IL-6 [fold change 0.43 (SE ± 0.13), p = 0.02], TNF [fold change 0.52 (SE ± 0.10), p = 0.02], IL1R1 [fold change 0.63 (SE ± 0.09), p = 0.04] and MSTN [fold change 0.63 (SE ± 0.11), p = 0.04] showed lower relative expression in those men who were stronger (n = 12) compared with those who were weaker (n = 8) (Fig. 2). In regression analyses, grip strength in kg decreased by 1.63 kg, p = 0.06 (95 % CI −0.05, 3.31), 1.86 kg, p = 0.06 (95 % CI −0.04, 3.76) and 1.40 kg, p = 0.09 (95 %CI −0.20, 3.00) for every SD increase in IL1R1, IL-6 and MSTN gene expression, respectively, but these were not found to be statistically significant (Table 4). Similarly, there were no significant associations between grip strength SD scores and TNF (Table 4). Adjusting for height did not substantially alter these non-significant associations (Table 5).

Muscle strength and skeletal muscle gene expression. Lower fold change in muscle mRNA expression of interleukin 6 (IL-6), tumour necrosis factor (TNF), interleukin 1 receptor (IL1R1 and myostatin (MSTN) in men who were stronger (n = 12) compared to those who were weaker (n = 8). Values are expressed as 2−ΔΔCt normalised to GSK3α. Bars represent standard error (SE) for fold change. *Significantly different from those who were weaker, p < 0.05
Gene Expression and Serum Cytokine Levels
Cycle threshold values for the genes IL1R1, IFNG, IL-6 and TNF negatively correlated with their corresponding serum levels suggesting higher Ct values associated with lower serum cytokine levels; however, these correlations were weak and not statistically significant (Table 6).
Serum Cytokine Levels, Lean Mass and Grip Strength
Serum cytokine, lean mass and grip strength measurements were available for 96 participants. Spearman correlation analyses revealed a significant negative correlation between serum IL-6 (R = −0.29, p = 0.005), TNF (R = −0.24, p = 0.017) and grip strength (Table 6). The association between these cytokines and lean mass was not statistically significant (Table 7).
PCCA and Gene Function Enrichment
PCCA analyses identified three clusters of genes that accounted for approximately 53 % of the total variation within the sample (Fig. 1 and Table 1 in the supplementary file). These clusters could be broadly interpreted biologically as genes involved in anabolism (Cluster I), intracellular signalling (Cluster 2) and inflammation (Cluster 3). Genes in Cluster 3 were over-expressed in men with low lean mass (IFNG and VDR) and low grip strength (IL-6, TNF and IL1R1) (Fig. 1 and Table 1 in the supplementary file). There were no significantly enriched functions associated with the genes in Cluster 1 for any of the three Gene Ontology (GO) classes, Biological Process (BP), Cellular Content (CC) and Molecular Function (MF) compared to the total list of tested genes. Cluster 2 contained a number of significant GO terms for the Biological Process and Molecular Function categories. These terms generally related to transcription factors and responses to stimuli. Cluster 3 was characterised by several Gene Ontology terms and KEGG pathway terms relating to immune response. None of the terms were significant after correction of p values for multiple testing using the Benjamini method (data not shown). However, the analysis generally supports the differing functional assignments for the genes in two of the clusters.
Discussion
In this novel study, we investigated the relationship between skeletal muscle gene expression and lean mass or grip strength, in community-dwelling older men. The genes for IFNG and VDR showed significantly lower relative expression levels in men with higher lean mass, but not in men who were stronger while the genes IL-6, TNF, IL1R1 (responsible for transmitting the inflammatory effects of IL-1) and MSTN showed significantly lower relative expression levels in men who were stronger, but not in those with high lean mass.
The apparent uncoupling of gene expression between the mass and strength groups in our study is somewhat surprising but not entirely unexpected. Although muscle mass determines muscle strength, the relationship is not linear. Both cross sectional and longitudinal studies show that younger as well as older individuals can be stronger than would be predicted by their muscle mass alone [33]. This may be explained by changes in muscle quality, where differential gene expression could be a key underlying mechanism.
Ageing is associated with a chronic low grade inflammatory profile characterised by an increase in proinflammatory cytokines [23]. Leger et al [34] showed that in older men, compared to younger counterparts, TNF mRNA levels were increased by almost threefold, while IGF-1 mRNA was decreased by 45 % in tissue obtained from the vastus lateralis. There is extensive evidence both from animal and human studies for the association of inflammatory cytokines (e.g. TNF, IL-6, IL-1) with muscle catabolism and muscle atrophy. Rieu et al [35] showed that controlling low grade inflammatory response with anti-inflammatory treatment in older rats was associated with better postprandial protein anabolism and prevented the loss of muscle mass. A study by Schapp et al [24] showed that higher serum levels of TNF and IL-6 soluble receptor were associated with greater declines in grip strength in men over the course of 5 years. A recent longitudinal study by Bartali et al [36] suggested that in men and women aged 65 or over, low protein intake was associated with greater declines in muscle strength in those with high levels of systemic inflammatory markers. In our study in muscle, we demonstrated lower levels of the proinflammatory genes IL-6, TNF, IL1R1 in men who were stronger, but interestingly not in those who had higher lean mass. Using regression analysis, there were also trends suggesting increased expression of these proinflammatory genes was associated with lower grip strength. Although we did not determine protein levels in skeletal muscle, we were able to measure serum levels of IL-6, TNF and IL1R1. There were non-significant trends suggesting lower serum levels of these cytokines in men with corresponding higher delta Ct values of these genes (indicating lower gene expression relative to control). Furthermore, there were significant negative correlations between serum levels of IL-6, TNF and grip strength in support of our regression analyses as well as previous observations pertaining to the adverse influence of these inflammatory cytokines on muscle strength [23, 24].
Interferon gamma (IFNG) is a pleiotropic cytokine that regulates muscle homeostasis and repair [37–39]. Few studies of IFNG in relation to muscle mass are available in adult humans. One study of patients with chronic obstructive airways disease (COPD), a disease characterized by muscle weakness, found no difference in muscle levels of IFNG, between patients and controls [40]. Conversely, studies of the inflammatory myopathies suggest that IFNG as well as TNF are central in their pathogenesis [41, 42]. A study in rodents, whose hind limbs were damaged after exposure to cardiotoxin, a mechanism known to induce an inflammatory response, interferon blocking antibodies reduced muscle cell proliferation and the formation of regenerating fibres. [39]. We speculate that in our study, men with high lean mass have a lower inflammatory burden. This is supported by analyses showing lack of expression of the proinflammatory genes e.g. TNF, and IL-6 in men with high lean mass.
The absence of the vitamin D receptor in mice is characterised by reductions in body size, in part mediated by reductions in myofiber size. Conversely, selective deletion of VDR in rodent cardiomyocytes, resulted in larger cardiomyocytes and left ventricular hypertrophy [43]. In humans, polymorphisms of VDR have been associated with reductions in fat-free mass. In our study, a decrease in expression of VDR was present in men with higher lean mass while regression analyses suggested that increased VDR expression was associated with decreases in lean mass. This finding is surprising and opposite to the existing evidence pertaining to the effects of the VDR. We speculate that a similar mechanism to that seen in cardiomyocytes of VDR knockout mice, where lower VDR expression was associated with cardiomyocyte hypertrophy, may be occurring in myofibers in our skeletal muscle samples [43]. Clearly, more investigation is required to address this specific point.
Myostatin (MSTN) is a negative regulator of skeletal muscle growth. In the current study, lower expression of MSTN was present in men who were stronger but not in those with higher lean mass. Consistent with these results, a recent human study showed that the risk of low grip strength was almost 8-fold higher in patients aged 35–85 with higher serum levels of myostatin [44]. In mice, pharmacological treatment with a myostatin blocking antibody increased muscle mass and strength [45]. However, conflicting data exist. For example, although muscle mass was increased in mice depleted of myostatin, force generation was impaired and these mice were weaker than their wild-type littermates [46]. Recent evidence from ageing humans suggests that although myostatin deficiency positively impacts on the production of maximum force and power in the short term, this effect is not prolonged [47].
Despite the compelling data provided here, there are acknowledged limitations with the current study. Firstly, it was designed to be ‘pathway focused’ and we analysed a limited number of genes previously implicated in the regulation of skeletal muscle structure and function. This strategy has the potential of missing other relevant and important genes. We did consider applying a correction for multiple testing in addition to the Benjamini method we used for PCCA. Correction for multiple testing as seen in large scale studies such as microarrays accounts for false discovery rates when thousands of individual tests are investigated. Given the limitation of the cohort size as well as the fact that we studied 44 genes selected on the basis of strong pre-existing evidence for roles in muscle function, we did not pursue correction for multiple testing. Secondly, the study was conducted on relatively small sample of male participants, as a cohort as well as within lean mass and grip strength groups. Although we adjusted our regression analysis for height, measures of body size and function as well as other unmeasured confounding variables could have an impact on our results. However, we were limited by sample size and therefore statistical power to detect significant differences. Future studies will require validation of the current results in a substantially larger cohort.
To our knowledge, this discovery study is the largest ever undertaken to investigate gene transcript changes associated with sarcopenia in humans set within the context of a well characterized epidemiological cohort. The study has utilised comparison of the extremes of lean mass and grip strength as a discovery tool and identified a number of genes for further investigation. Larger studies that also include women are now needed to enable the influence of factors such as physical activity as well as gender to be explored and muscle protein levels ascertained.
Conclusions
This novel skeletal muscle gene expression study carried out within a well-characterized epidemiological birth cohort has demonstrated that lower expression of VDR and IFNG is associated with higher lean mass and lower expression of IL-6, TNF, IL1R1 and myostatin is associated with higher grip strength. These findings are consistent with a role of proinflammatory factors in mediating lower muscle strength in community-dwelling older men.
References
Patel HP, Syddall HE, Jameson K, Robinson S, Denison H, Roberts HC, Edwards M, Dennison E, Cooper C, Aihie Sayer A (2013) Prevalence of sarcopenia in community-dwelling older people in the UK using the European Working Group on Sarcopenia in Older People (EWGSOP) definition: findings from the Hertfordshire Cohort Study (HCS). Age Ageing 42:378–384
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinkova E, Vandewoude M, Zamboni M (2010) Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 39:412–423
Newman AB, Haggerty CL, Goodpaster B, Harris T, Kritchevsky S, Nevitt M, Miles TP, Visser M (2003) Strength and muscle quality in a well-functioning cohort of older adults: The Health, Aging and Body Composition Study. J Am Geriatr Soc 51:323–330
Grounds MD (2002) Reasons for the degeneration of ageing skeletal muscle: a central role for IGF-1 signalling. Biogerontology 3:19–24
Meng SJ, Yu LJ (2010) Oxidative stress, molecular inflammation and sarcopenia. Int J Mol Sci 11:1509–1526
Goodman CA, Mayhew DL, Hornberger TA (2011) Recent progress toward understanding the molecular mechanisms that regulate skeletal muscle mass. Cell Signal 23:1896–1906
Roubenoff R, Parise H, Payette HA, Abad LW, D’Agostino R, Jacques PF, Wilson PW, Dinarello CA, Harris TB (2003) Cytokines, insulin-like growth factor 1, sarcopenia, and mortality in very old community-dwelling men and women: The Framingham Heart Study. Am J Med 115:429–435
Gumucio JP, Mendias CL (2013) Atrogin-1, MuRF-1, and sarcopenia. Endocrine 43:12–21
Christakos S, Hewison M, Gardner DG, Wagner CL, Sergeev IN, Rutten E, Pittas AG, Boland R, Ferrucci L, Bikle DD (2013) Vitamin D: beyond bone. Ann N Y Acad Sci 1287:45–58
Huang Z, Chen X, Chen D (2011) Myostatin:a novel insight into its role in metabolism, signal pathways and expression regulation. Cell Signall 23:1441–1446
Lee SJ, McPherron AC (2001) Regulation of myostatin activity and muscle growth. Proc Natl Acad Sci U S A 98:9306–9311
Boland RL (2011) VDR activation of intracellular signaling pathways in skeletal muscle. Mol Cell Endocrinol 347:11–16
Ceglia L (2008) Vitamin D and skeletal muscle tissue and function. Mol Asp Med 29:407–414
Endo I, Inoue D, Mitsui T, Umaki Y, Akaike M, Yoshizawa T, Kato S, Matsumoto T (2003) Deletion of vitamin D receptor gene in mice results in abnormal skeletal muscle development with deregulated expression of myoregulatory transcription factors. Endocrinology 144:5138–5144
Song Y, Kato S, Fleet JC (2003) Vitamin D receptor (VDR) knockout mice reveal VDR-independent regulation of intestinal calcium absorption and ECaC2 and calbindin D9k mRNA. J Nutr 133:374–380
Roth SM, Zmuda JM, Cauley JA, Shea PR, Ferrell RE (2004) Vitamin D receptor genotype is associated with fat-free mass and sarcopenia in elderly men. J Gerontol A Biol Sci Med Sci 59:10–15
McPherron AC, Lawler AM, Lee SJ (1997) Regulation of skeletal muscle mass in mice by a new TGF-beta superfamily member. Nature 387:83–90
Kambadur R, Sharma M, Smith TP, Bass JJ (1997) Mutations in myostatin (GDF8) in double-muscled Belgian Blue and Piedmontese cattle. Genome Res 7:910–916
Constantin D, McCullough J, Mahajan RP, Greenhaff PL (2011) Novel events in the molecular regulation of muscle mass in critically ill patients. J Physiol 589:3883–3895
Gonzalez-Cadavid NF, Taylor WE, Yarasheski K, Sinha-Hikim I, Ma K, Ezzat S, Shen R, Lalani R, Asa S, Mamita M, Nair G, Arver S, Bhasin S (1998) Organization of the human myostatin gene and expression in healthy men and HIV-infected men with muscle wasting. Proc Natl Acad Sci U S A 95:14938–14943
Allen DL, Loh AS (2011) Posttranscriptional mechanisms involving microRNA-27a and b contribute to fast-specific and glucocorticoid-mediated myostatin expression in skeletal muscle. Am J Physiol Cell Physiol 300:C124–C137
Lokireddy S, Wijesoma IW, Bonala S, Wei M, Sze SK, McFarlane C, Kambadur R, Sharma M (2012) Myostatin is a novel tumoral factor that induces cancer cachexia. Biochem J 446:23–36
Beyer I, Mets T, Bautmans I (2012) Chronic low-grade inflammation and age-related sarcopenia. Curr Opin Clin Nutr Metab Care 15:12–22
Schaap LA, Pluijm SM, Deeg DJ, Harris TB, Kritchevsky SB, Newman AB, Colbert LH, Pahor M, Rubin SM, Tylavsky FA, Visser M (2009) Higher inflammatory marker levels in older persons: associations with 5-year change in muscle mass and muscle strength. J Gerontol A Biol Sci Med Sci 64:1183–1189
Visser M, Pahor M, Taaffe DR, Goodpaster BH, Simonsick EM, Newman AB, Nevitt M, Harris TB (2002) Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J Gerontol A Biol Sci Med Sci 57:M326–M332
Barns M, Gondro C, Tellam RL, Radley-Crabb HG, Grounds MD, Shavlakadze T (2014) Molecular analyses provide insight into mechanisms underlying sarcopenia and myofiber denervation in old skeletal muscles of mice. Int J Biochem Cell Biol 13(53C):174–185
Liu D, Sartor MA, Nader GA, Pistilli EE, Tanton L, Lilly C, Gutmann L, IglayReger HB, Visich PS, Hoffman EP, Gordon PM (2013) Microarray analysis reveals novel features of the muscle aging process in men and women. J Gerontol A Biol Sci Med Sci 68:1035–1044
Patel HP, Syddall HE, Martin HJ, Stewart CE, Cooper C, Sayer AA (2010) Hertfordshire Sarcopenia Study: design and methods. BMC Geriatr 10:43
Syddall HE, Sayer AA, Dennison EM, Martin HJ, Barker DJ, Cooper C (2005) Cohort profile: The Hertfordshire cohort study. Int J Epidemiol 34:1234–1242
Livak KJ, Schmittgen TD (2001) Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 25:402–408
Tichopad A, Pecen L, Pfaffl MW (2006) Distribution-insensitive cluster analysis in SAS on real-time PCR gene expression data of steadily expressed genes. Comput Methods Progr Biomed 82:44–50
Huang DW, Sherman BT, Tan Q, Kir J, Liu D, Bryant D, Guo Y, Stephens R, Baseler MW, Lane HC, Lempicki RA (2007) DAVID bioinformatics resources: expanded annotation database and novel algorithms to better extract biology from large gene lists. Nucleic Acids Res 35:W169–W175
Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, Tylavsky FA, Visser M, Newman AB (2006) The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 61:1059–1064
Leger B, Derave W, De BK, Hespel P, Russell AP (2008) Human sarcopenia reveals an increase in SOCS-3 and myostatin and a reduced efficiency of Akt phosphorylation. Rejuvenation Res 11:163–175B
Rieu I, Magne H, Savary-Auzeloux I, Averous J, Bos C, Peyron MA, Combaret L, Dardevet D (2009) Reduction of low grade inflammation restores blunting of postprandial muscle anabolism and limits sarcopenia in old rats. J Physiol 587:5483–5492
Bartali B, Frongillo EA, Stipanuk MH, Bandinelli S, Salvini S, Palli D, Morais JA, Volpato S, Guralnik JM, Ferrucci L (2012) Protein intake and muscle strength in older persons: does inflammation matter? J Am Geriatr Soc 60:480–484
Londhe P, Davie JK (2011) Gamma interferon modulates myogenesis through the major histocompatibility complex class II transactivator, CIITA. Mol Cell Biol 31:2854–2866
Schroder K, Hertzog PJ, Ravasi T, Hume DA (2004) Interferon-gamma: an overview of signals, mechanisms and functions. J Leukoc Biol 75:163–189
Cheng M, Nguyen MH, Fantuzzi G, Koh TJ (2008) Endogenous interferon-gamma is required for efficient skeletal muscle regeneration. Am J Physiol Cell Physiol 294:C1183–C1191
Barreiro E, Schols AM, Polkey MI, Galdiz JB, Gosker HR, Swallow EB, Coronell C, Gea J (2008) Cytokine profile in quadriceps muscles of patients with severe COPD. Thorax 63:100–107
Rayavarapu S, Coley W, Nagaraju K (2011) An update on pathogenic mechanisms of inflammatory myopathies. Curr Opin Rheumatol 23:579–584
Crescioli C, Sottili M, Bonini P, Cosmi L, Chiarugi P, Romagnani P, Vannelli GB, Colletti M, Isidori AM, Serio M, Lenzi A, Di LL (2012) Inflammatory response in human skeletal muscle cells: CXCL10 as a potential therapeutic target. Eur J Cell Biol 91:139–149
Chen S, Law CS, Grigsby CL, Olsen K, Hong TT, Zhang Y, Yeghiazarians Y, Gardner DG (2011) Cardiomyocyte-specific deletion of the vitamin D receptor gene results in cardiac hypertrophy. Circulation 124:1838–1847
Han DS, Chen YM, Lin SY, Chang HH, Huang TM, Chi YC, Yang WS (2011) Serum myostatin levels and grip strength in normal subjects and patients on maintenance haemodialysis. Clin Endocrinol (Oxf) 75:857–863
Whittemore LA, Song K, Li X, Aghajanian J, Davies M, Girgenrath S, Hill JJ, Jalenak M, Kelley P, Knight A, Maylor R, O’Hara D, Pearson A, Quazi A, Ryerson S, Tan XY, Tomkinson KN, Veldman GM, Widom A, Wright JF, Wudyka S, Zhao L, Wolfman NM (2003) Inhibition of myostatin in adult mice increases skeletal muscle mass and strength. Biochem Biophys Res Commun 300:965–971
Amthor H, Macharia R, Navarrete R, Schuelke M, Brown SC, Otto A, Voit T, Muntoni F, Vrbova G, Partridge T, Zammit P, Bunger L, Patel K (2007) Lack of myostatin results in excessive muscle growth but impaired force generation. Proc Natl Acad Sci U S A 104:1835–1840
Schirwis E, Agbulut O, Vadrot N, Mouisel E, Hourde C, Bonnieu A, Butler-Browne G, Amthor H, Ferry A (2012) The beneficial effect of myostatin deficiency on maximal muscle force and power is attenuated with age. Exp Gerontol 48(2):183–190
Acknowledgment
We are very grateful to the study participants and research staff at the Wellcome Trust Clinical Research Facility, University Hospital Southampton Foundation Trust.
Human and Animal Rights and Informed Consent
This study was ethically approved by the Hertfordshire Research Ethics Committee (Hertfordshire, UK) and performed in accordance with the criteria defined by the rules of the committee.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Patel, H.P., Al-Shanti, N., Davies, L.C. et al. Lean Mass, Muscle Strength and Gene Expression in Community Dwelling Older Men: Findings from the Hertfordshire Sarcopenia Study (HSS). Calcif Tissue Int 95, 308–316 (2014). https://doi.org/10.1007/s00223-014-9894-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-014-9894-z