
Abstract
It has been suggested that oxidative stress is associated with the pathogenesis of osteoporosis. The objective of this study was to explore the association between a marker of oxidative stress and either bone turnover markers or bone mineral density (BMD) in postmenopausal women. In addition, the effects of oxidative stress on the formation of osteoclasts in human bone marrow cell culture were examined. We performed a cross-sectional analysis in healthy postmenopausal women aged 60–78 years (n = 135, 68.2 ± 4.9). Oxidative stress was evaluated in the serum by measuring 8-hydroxy-2′-deoxyguanosine (8-OH-dG) levels. The biochemical markers of bone turnover and areal BMD were measured in all participants. Multivariate linear regression analysis revealed a negative association between 8-OH-dG levels and BMD of the lumbar spine, total hip, femoral neck, and trochanter and positive association with type I collagen C-telopeptide (ICTP) levels. The odds ratio of 8-OH-dG for osteoporosis was 1.54 (1.14–2.31, P = 0.003). In cultures of primary human marrow cells, H2O2 caused concentration-dependent activation of TRAP-positive multinucleated giant cells. H2O2 also increased the area of pits per osteoclast activity assay substrate. RT-PCR showed that H2O2 stimulated the expression of M-CSF and RANKL and increased the RANKL/OPG ratio. The data support the view that oxidative stress is associated with increased bone resorption and low bone mass in otherwise healthy women. In addition, RANKL and M-CSF stimulation induced by oxidative stress may participate in osteoclastogenesis in human bone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Oxidative stress occurs in a cellular system when the production of free radical moieties exceeds the antioxidant capacity of that system. The impairment caused by the increased concentration of reactive oxygen species (ROS) is believed to result from random damage to proteins, lipids, and DNA. In addition to these effects, an increase in ROS levels may constitute a stress signal that activates specific redox-sensitive signaling pathways. Once activated, these signaling pathways can have either damaging or potentially protective functions [1]. There is increasing evidence suggesting that oxidative stress is responsible for the pathophysiology of the aging process and may participate in the pathogenesis of atherosclerosis, neurodegenerative diseases, cancer, and diabetes [1]. Osteoporosis is associated with many etiological factors, such as nutrition, cytokines, hormones, and aging. Recently, ROS were suggested to be responsible for the development of osteoporosis. Some in vitro and animal studies have reported that oxidative stress decreases the level of bone formation by modulating the differentiation and survival of osteoblasts [2, 3]. Moreover, osteoclasts have been shown to be activated by ROS to enhance bone resorption [4, 5]. Recent evidence in a limited number of clinical studies has shown that ROS and/or antioxidant systems might be involved in the pathogenesis of bone loss [6–12].
8-Hydroxy-2′-deoxyguanosine (8-OH-dG) is a ROS-induced modification of a purine residue in DNA and a sensitive index of oxidative DNA damage [13]. 8-OH-dG is produced during DNA repair. High levels of 8-OH-dG have been found in patients receiving chemotherapy, smokers, patients exposed to whole-body irradiation, and patients with diabetes mellitus and rheumatoid arthritis [14–16]. The urinary or serum level of this molecule is now considered to be a reliable biomarker for the in vivo measurement of systemic oxidative stress [17]. Some in vivo studies have examined the biochemical link between oxidative stress and bone mineral density (BMD). These studies assessed a by-product of lipid peroxidation, such as malondialdehyde (MDA) [7–9, 12] or isoprostane [6, 10, 11]. However, there was a small number of subjects; both males and females were enrolled [6, 12], which would have rendered the group heterogeneous from a skeletal perspective; and some studies focused on male osteoporosis [8, 11] or on hypercholesterolemic patients [10]. In addition, very little is known about whether oxidative stress is associated with the biochemical markers of bone turnover in humans. This study measured serum 8-OH-dG as an oxidative stress marker and examined the relationship between 8-OH-dG levels and either BMD or bone turnover markers. Subjects were confined to only healthy postmenopausal women in order to exclude possible confounders.
It was reported that ROS stimulates bone resorption in mouse calvarial organ cultures and induces osteoclastogenesis in primary cultures of mouse bone marrow or a monocyte/macrophage linage cell line [18–20]. However, there are few reports on the role of oxidative stress on the differentiation of osteoclasts in primary human cells. In vitro studies were performed in parallel with clinical studies to determine the effects of ROS on the formation of osteoclasts in human bone marrow cell cultures. The role of ROS in expression of factors essential for osteoclast differentiation, such as receptor activator of NF-κB ligand (RANKL) and macrophage colony-stimulating factor (M-CSF), was also examined in cultures of primary human bone marrow stromal cells.
Subjects and Methods
Subjects
This cross-sectional study was approved by the institutional review board of St. Mary’s Hospital (Seoul, Korea), and all subjects provided written informed consent. Two hundred and seventy-six consecutive Korean women who visited the Health Promotion Center of St. Mary’s Hospital from January 2005 to July 2005 were enrolled in this study. The inclusion criteria were women aged 60 years or older, the cessation of menses for at least 5 years, and no previous hormone-replacement therapy. Women with cardiac, liver, or renal diseases; endocrine or metabolic abnormalities; or inflammatory diseases and/or who were receiving medicine known to influence bone mineralization were excluded. Smoking habits were categorized as current, ex-smokers, and never smokers. Only never smokers were included. Subjects who had used antioxidant supplements, such as vitamin E or C, within the 6 months prior to enrollment were also excluded. A physician examined each subject, and those having or suspected of having infectious diseases were excluded. Of the initial 276 women, 135 were considered eligible for the study.
In each woman, a blood sample was collected from the antecubital vein between 8:00 and 9:00 a.m., after an overnight fast. Blood was collected in tubes, placed on ice, and centrifuged immediately in the cold. Serum was stored immediately at −70°C until assayed. Samples from all women were analyzed at the same time.
Assays
Serum glucose, calcium, phosphorus, albumin, creatinine, aspartate aminotransferase, and alanine aminotransferase levels were determined using an autoanalyzer (747 automatic analyzer; Hitachi, Tokyo, Japan). Serum 8-OH-dG concentrations were determined in duplicate using an ELISA (Bioxytech 8-OHdG-EIA kit; OXIS Health Products, Portland, OR). The maximum inter- and intra-assay coefficients of variation (CVs) for the range of concentrations examined were 6.7 and 4.4%, respectively. Serum bone-specific alkaline phosphatase (BAP) concentrations were determined by an ELISA test (Metra BAP EIA kit; Quidel, San Diego, CA). The maximum inter- and intra-assay CVs for the range of concentrations that were evaluated were 5.8 and 7.6%, respectively. Type I collagen C-telopeptide (ICTP) concentrations were measured using a radioimmunoassay (Telopeptide ICTP; Orion Diagnostica, Espoo, Finland). The maximum inter- and intra-assay CVs were 10.7 and 3.6%, respectively.
Bone Densitometry
Areal BMD (g/cm2) of the lumbar spine (vertebrae L1–L4) and BMD of the total hip, femoral neck, and trochanter were measured by dual-energy X-ray absorptiometry using a Delphi W (Hologic, Bedford, MA). The precision of the method (CV) was determined to be 1.2% at the lumbar spine and 1.9% at the femoral neck.
Cell Culture and ROS Treatment
Bone marrow was harvested from the iliac crest of healthy donors for a bone marrow transplant. Informed consent was obtained from all donors. Mononuclear cells were separated using Ficoll-Hypaque (1.077 g/ml; Sigma-Aldrich, St. Louis, MO). Cells were seeded in culture flasks at a density of 4 × 105 cells/ml and incubated at 37°C in a humidified atmosphere containing 95% air and 5% CO2. The medium was composed of alpha-minimal essential medium (α-MEM, Sigma-Aldrich), containing 20% heat-inactivated fetal bovine serum (FBS; Life Technologies, Grand Island, NY) supplemented with 100 units/ml penicillin-streptomycin, 10−8 M vitamin K, 10 mM β-glycerophosphate, and 50 μg/ml ascorbic acid. Cells were then fed at 2-day intervals. Cells were subcultured until they reached approximately 90% confluence and seeded in six-well culture plates at a density of 5 × 104 cells/ml. In the secondary culture, cells were maintained in α-MEM containing 10% FBS, antibiotics, 10−8 M vitamin K, 10 mM β-glycerophosphate, and 50 μg/ml ascorbic acid. After they reached near confluence, they were exposed to α-MEM containing various H2O2 concentrations in the presence or absence of the inhibitor, 500 units/ml catalase. After a 24 h ROS treatment, RNA was extracted using TRIzol® (Invitrogen, Rockville, MD) and isolated according to the manufacturer’s protocol.
Reverse Transcriptase-Polymerase Chain Reaction
Total RNA (1 μg) was subjected to reverse transcription with d(T)16 and 1 μl of Superscript II enzyme (GIBCO-BRL, Gaithersburg, MD) in 20 μl reaction mixture. After 1 h at 42°C, 1 μl was subjected to PCR using the following cycling conditions: 94°C, 20 s; 60°C, 30 s; 72°C, 1 min for 35 cycles. The primers used for PCR are as follows: 5′-GCCAGTGGGAGATGTTAG-3′ and 5′-TTAGCTGCAAGTTTTCCC-3′ for RANKL; 5′-TGGAGATCGAATTCTGCTTG-3′ and 5′-TCAAGTGCTTGAGGGCATAC-3′ for osteoprotegerin (OPG); 5′-GGCCATGAGAGGCAGTCCGAGGG-3′ and 5′-CACTGGCAGTTCCACCTGTCTGTC-3′ for M-CSF. The glyceraldehyde-3-phosphate dehydrogenase (GAPDH) gene amplified with the primers 5′-ACCACAGTCCATGCCATCAC-3′ and 5′-TCCACCACCCTGTTGCTGTA-3′ was used as the control for the RNA input. PCR products were separated in a 3% agarose gel and visualized by ethidium bromide staining. Band intensities were quantified using Gel Doc 1000® and Molecular Analyst Software, version 1.4.1 (Bio-Rad, Hercules CA).
Osteoclast Culture and Enzyme Histochemistry
Mononuclear cells were separated from human bone marrow using Ficoll-Hypaque and cultured as described elsewhere [21]. Briefly, marrow mononuclear cells were cultured in α-MEM containing 20% horse serum at 106 cells/ml in 96-well multiwells (105 cells/200 μl/well). Cultures were maintained at 37°C in a humidified atmosphere containing 5% CO2–air for 3 weeks. The effect of H2O2 on osteoclastogenesis was assessed by inducing the marrow mononuclear cells to undergo osteoclastogenesis by culturing them in the presence of 10−9 or 10−8 M of 1α,25-dihydroxyvitamin D3 (1α,25-[OH]2D3) (Calbiochem, La Jolla, CA). 1α,25-(OH)2D3 was added to cultures at their initiation as well as at each change of medium. Cultures were fed weekly by removing half of the medium. Varying concentrations of H2O2 in the presence or absence of catalase were added to cultures when the medium was changed at 1 and 2 weeks. The level of osteoclast formation in cultures of marrow mononuclear cells was evaluated by measuring the number of tartrate-resistant acid phosphatase (TRAP)-positive multinuclear cells. Cytochemical staining of TRAP-positive cells was performed using the leukocyte acid phosphatase assay kit (Sigma-Aldrich) according to the manufacturer’s procedure. TRAP-positive cells with three or more nuclei (multinucleated cells) were counted using an optical microscope (Olympus Optical, Tokyo, Japan).
Resorption Assay
Human marrow mononuclear cells in α-MEM containing 20% horse serum were plated at 105 cells/300 μl/well into a calcium phosphate-coated 48-well plate, osteoclast activity assay substrate (OAAS; Oscotec, Cheonan, Korea). Cells were cultured for 3 weeks in the presence of 1α,25-(OH)2D3, H2O2, and catalase, as described above. After the culture period, osteoclasts were removed from the plate by lysis with 1 N NaOH. Photographs were taken under a light microscope at 40× magnification, and the total areas of the resorbed pits were analyzed using the image Pro-Plus program, version 4.0 (Media Cybernetics, Silver Spring, MD).
Statistical Analysis
Statistical analysis was carried out using SPSS, version 10.5 (SPSS, Inc., Chicago, IL). All data are reported as means ± SD. Bivariate associations between serum 8-OH-dG levels and clinical variables, BMD, and bone turnover markers were determined using a Spearman test. Standard linear regression analysis was used to examine the relationship between serum 8-OH-dG levels and either BMD or markers of bone turnover. Age, body mass index (BMI), years since menopause (YSM), and bone turnover markers were considered to be confounders. The association between serum 8-OH-dG levels and osteoporosis was determined by logistic regression analysis. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were estimated. Age, BMI, YSM, and bone turnover markers were included as covariates in this logistic regression analysis. In the in vitro experiments, differences between three or more groups were assessed by ANOVA with post hoc analysis using a Duncan’s multiple range test. P < 0.05 was considered significant.
Results
Table 1 summarizes the characteristics of the 135 women. The women’s age ranged 60–78 years (mean 68.2 ± 4.9), with an average BMI of 24.5 ± 2.8 kg/m2. Among the women, 45.9% were considered osteoporotic with a BMD t score > 2.5 SD below that of young normal women at any site.
Relationship Between Serum 8-OH-dG Levels and Either BMD or Bone Turnover Markers
Simple bivariate analyses revealed the serum 8-OH-dG concentration to have a positive correlation with ICTP (P < 0.001). Higher levels of 8-OH-dG were also associated with a lower BMD at the lumbar spine (P = 0.005), total hip (P = 0.003), femoral neck (P = 0.003), and trochanter (P = 0.003) (Fig. 1). There was no significant correlation between the oxidative stress marker and clinical variables such as age, BMI, YSM, and BAP (Table 2). After adjusting for important BMD-related covariates such as age, BMI, YSM, and bone turnover markers, the association remained at the lumbar spine (P = 0.014), total hip (P = 0.005), femoral neck (P = 0.005), and trochanter (P = 0.006). In addition, after multiple adjustments, there was still a significant association between 8-OH-dG levels and ICTP levels (P = 0.002) (Table 3).

Association between serum 8-OH-dG levels and BMD at the lumbar spine (a), total hip (b), and femoral neck (c), as well as serum ICTP levels (d)
8-OH-dG Levels and Risk of Osteoporosis
Figure 2 shows the results of multiple logistic regression analysis with osteoporosis as the dependent variable. According to the WHO classification, osteoporosis was diagnosed in patients with a T score of −2.5 or below. The lowest T score of the lumbar spine, total hip, femoral neck, or the trochanter for each participant was selected. After adjusting for age, BMI, YSM, and bone turnover markers, the risk of osteoporosis increased by 54% for each increase of 1 SD in 8-OH-dG concentration (OR = 1.54, 95% CI 1.14–2.31).

Adjusted ORs and 95% CIs for osteoporosis according to 8-OH-dG concentrations. Logistic regression analysis was carried out to determine the OR of osteoporosis relative to the oxidative stress marker 8-OH-dG
Effect of H2O2 on TRAP+ Multinucleated Osteoclast-Like Cells
A 3-week culture of human marrow mononuclear cells in the presence of 10−9 M 1α,25-(OH)2D3 induced the formation of osteoclast-like cells with multiple nuclei. Treatment of marrow mononuclear cells with 100, 300, or 500 μM H2O2 with 10−9 M 1α,25-(OH)2D3 resulted in a dose-dependent increase in the vitamin D–induced differentiation into TRAP+ osteoclast-like cells from 25 ± 7 (control, 10−9 M 1α,25-[OH]2D3) to 32 ± 10 (100 μM) to 44 ± 9 (300 μM) (P < 0.01 vs. control) and to 66 ± 12 (500 μM) (P < 0.01 vs. control). Besides the number, the sizes of the multinucleated cells increased with H2O2 in a dose-dependent manner. Catalase, which is a catabolic enzyme of H2O2, significantly suppressed the formation of TRAP+ multinucleated cells (Fig. 3).

The effect of H2O2 on osteoclast formation. Primary human marrow mononuclear cells (105/cells/well) were cultured with or without the indicated H2O2 concentrations in α-MEM containing 20% horse serum and 10−9 M 1α,25-(OH)2D3. Catalase was added as an antioxidant to a selected group. Cells were fixed and stained for TRAP, and the number of multinucleated TRAP-positive cells (more than three nuclei) was determined. Representative images (×400) from one of five experiments are shown (a control, b 100 μM, c 300 μM, d 500 μM, e 500 μM H2O2 + 500 units/ml catalase). f * P < 0.01 versus control, ** P < 0.01 versus group treated with 500 μM H2O2
Effect of H2O2 on Bone Resorption
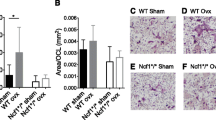
H2O2 stimulated bone resorption in a concentration-dependent manner. Maximum resorption was observed at 500 μM (P < 0.01 vs. control) on an OAAS plate. The increase in bone resorption stimulated by 500 μM H2O2 was significantly inhibited by addition of 500 units/ml catalase (P < 0.01 vs. 500 μM H2O2 with no catalase) (Fig. 4). Catalase alone had no significant effect on bone resorption (data not shown).

Effects of H2O2 and catalase on bone resorption. Human marrow mononuclear cells with 10−9 M 1α,25-(OH)2D3 in the presence or absence of the indicated concentrations of H2O2 were incubated for 3 weeks in medium containing 20% horse serum on calcium phosphate apatite–coated plates (OAAS). Shown are representative photographs (×40) (a control, b 100 μM, c 300 μM, d 500 μM, e 500 μM H2O2 + 500 units/ml catalase) from one of five experiments. f * P < 0.01 versus control, ** P < 0.01 versus group treated with 500 μM H2O2
Effects of H2O2 on Expression of RANKL, OPG, and M-CSF in Culture of Marrow Stromal Cells
Incubation of human marrow stromal cells with 500 μM H2O2 significantly increased cellular mRNA levels of M-CSF and RANKL by 1.5-fold (P < 0.01) and twofold (P < 0.01), respectively (Fig. 5). The effects of 500 μM H2O2 on the expression of M-CSF and RANKL were inhibited by the catalase treatment. Oxidative stress had no significant effect on the expression of OPG. However, after treatment with 500 μM H2O2, the RANKL/OPG ratio was significantly higher than that of control (P < 0.01).

Effects of H2O2 and catalase on the cellular mRNA expression of RANKL, OPG, and M-CSF. Human marrow stromal cells were cultured in α-MEM including 10% FBS and induced to differentiate to osteoblasts in the presence of 10−8 M vitamin K, 10 mM β-glycerophosphate, and 50 μg/ml ascorbic acid. Cells were treated with the indicated concentrations of H2O2 and 500 units/catalase for 24 h, and levels of RANKL, OPG, M-CSF, and GAPDH mRNA were measured by RT-PCR. Shown are representative blots (a) and the mean ± SD densitometry of three independent experiments (b RANKL, c OPG, d M-CSF, e ratio of RANKL/OPG). * P < 0.01 versus control, ** P < 0.01 versus group treated with 500 μM H2O2
Discussion
This study measured serum 8-OH-dG level as a marker of in vivo oxidative stress. “Oxidative stress” is a term used to define the imbalance in the production of free radicals through a number of cellular events [22] and the capacity of the cell to dispose of these oxidants. When not neutralized, these free radicals have the capacity to alter the integrity of several molecules, such as proteins and lipids. DNA can also be the target of free radical attack, and the levels of the oxidative DNA adduct 8-OH-dG in urine, tissue, and serum are often used as markers of oxidative stress [13–17].
In the clinical section of this study, the relationship between the amount of oxidative stress, serum 8-OH-dG levels, and BMD was investigated at four bone sites: lumbar spine, total hip, femoral neck, and trochanter. A significant negative association was found between 8-OH-dG levels and BMD at all sites examined using simple regression and multivariate models. These results show the close relationship between oxidative stress and low bone mass. These observations are also in line with recent in vivo studies, which examined the relationship between oxidative stress and bone mass [6–12, 23].
The strength of this study compared with previous studies is its relatively large size and the homogeneity of the group in view of the skeletal perspective. Confinement of the subjects to postmenopausal women, a narrow age range (60–78 years), and the exclusion of potential confounding factors (smoking, medications known to influence bone metabolism, and use of antioxidants) prior to enrollment rather than adjusting for these factors after enrollment might confer more reliability in statistical analysis. This study also exclusively included women who had ceased their menses for at least 5 years. This criterion was applied to exclude the period during which rapid changes of bone turnover might occur.
Age and YSM are usually strong predictors of osteoporosis. However, in this observation, only age showed marginal significance for risk of osteoporosis (Fig. 2); and this might be a limitation of the study. We think this happened because this study enrolled women aged 60 years or older and had a relatively narrow age range. When inclusion criteria were expanded to the immediate postmenopausal period, the data showed better statistical significance in terms of age and YSM (data not shown).
Interestingly, serum 8-OH-dG levels also showed a positive correlation with levels of the bone resorption marker, which was obvious even after multiple adjustments. This is the first study to examine the relationship between the status of oxidative stress and biochemical bone turnover markers in postmenopausal women. This result and the aforementioned negative relationship between 8-OH-dG levels and bone mass suggest that subjects with higher oxidant levels lost more bone through augmented osteoclast-mediated bone resorption. A previous animal study also confirmed this hypothesis. Giving postmenopausal rats a lactate diet for 4 weeks led to significantly higher levels of urinary deoxypyridinoline and 8-OH-dG excretion [4]. However, this finding contrasts with the results of a recent study reporting no significant correlation between free radical levels and bone turnover markers in a sample of osteoporotic males [8]. However, in the latter study, the smaller sample size precluded multivariate analysis. Therefore, important confounding variables, such as smoking, could not be adjusted for, even though as many as 50% of their subjects were smokers.
These results, showing that increased serum 8-OH-dG levels are associated with a low bone mass and increased bone resorption, strongly support the hypothesis that increased oxidative stress contributes to the development of osteoporosis. However, due to the cross-sectional nature of this study, no firm conclusions regarding the causal relationship can be drawn. Therefore, additional in vitro experiments were carried out to determine the effects of ROS on the formation of osteoclasts in primary human bone marrow cell cultures. A significant increase in the number and activity of osteoclasts was observed when H2O2 was added to cultures of human marrow mononuclear cells. This process was abolished by the administration of catalase, an antioxidant enzyme. Previous studies have shown that ROS stimulates osteoclast differentiation and bone resorption in cultures of mouse bone marrow cells [18], mouse calvarial cultures [19], and cocultures of mouse calvarial osteoblasts and spleen cells [24]. We also found, in human bone marrow stromal cells, that oxidative stress induced expression of RANKL and M-CSF, which are known to play an important role in osteoclastogenesis. These results are consistent with a previous report by Bai et al. [24], who demonstrated that ROS stimulates RANKL expression in mouse osteoblasts and human MG63 cells. However, they did not find any changes in M-CSF expression with ROS stimulation.
In the clinical part of this study we used 8-OH-dG as a marker of oxidative stress, and in the experimental part we used H2O2 to show that ROS stimulate bone resorption. H2O2 is known to diffuse into cells and to decompose to hydroxyl radical (HO•) in the presence of reduced Fe [25, 26]. The interaction of HO• with the nucleobases of the DNA strand, such as guanine, leads to the formation of 8-OH-dG [27]. Thus, we think this experiment which used H2O2 as a ROS supplier could support the results of clinical study.
ROS may play a role in bone-related diseases in two ways: the suppression of bone formation and the stimulation of bone resorption. Oxidative stress inhibited bone cell differentiation of a preosteoblastic cell line (MC3T3-E1) and rabbit bone marrow stromal cells that undergo osteoblastic differentiation [2, 3]. However, there were no such negative associations between the oxidative stress marker and the marker of bone formation in the clinical section of this study. The precise cause is unclear. However, other factors, such as growth factors, sex hormones, and age-related changes in osteoblasts, can have a larger effect on osteoblast function than oxidative stress itself. Besides, Mangiafico et al. [10] found a relationship between serum 8-isoprostaglandin F2α and a decrease in bone mass and bone formation markers in hypercholesterolemic subjects. This suggests that enhanced oxidative stress may have a negative impact on bone mass, possibly also via reduced bone formation.
In conclusion, there is a close association between oxidative stress (measured by the biomarker 8-OH-dG) and either BMD or marker of bone resorption. In vitro studies also demonstrate that ROS stimulates RANKL and M-CSF expression and induces osteoclastogenesis in a primary human bone marrow cell culture. These results have important implications for bone biology and treatment of osteoporosis. These results suggest that osteoporosis, at least in part, is a consequence of oxidative damage. In addition, treatments that increase the oxidant defenses in bone can prevent bone loss–related diseases.
References
Finkel T, Holbrook NJ (2000) Oxidants, oxidative stress and the biology of ageing. Nature 408:239–247
Mody N, Parhami F, Sarafian TA, Demer LL (2001) Oxidative stress modulates osteoblastic differentiation of vascular and bone cells. Free Radic Biol Med 31:509–519
Bai XC, Lu D, Bai J, Zheng H, Ke ZY, Li XM, Luo SQ (2004) Oxidative stress inhibits osteoblastic differentiation of bone cells by ERK and NF-κB. Biochem Biophys Res Commun 314:197–207
Isomura H, Fujie K, Shibata K, Inoue N, Iizuka T, Takebe G, Takahashi K, Nishihira J, Izumi H, Sakamoto W (2004) Bone metabolism and oxidative stress in postmenopausal rats with iron overload. Toxicology 197:93–100
Garrett IR, Boyce BF, Oreffo RO, Bonewald L, Poser J, Mundy GR (1990) Oxygen-derived free radicals stimulate osteoclastic bone resorption in rodent bone in vitro and in vivo. J Clin Invest 85:632–639
Basu S, Michaelsson K, Olofsson H, Johansson S, Melhus H (2001) Association between oxidative stress and bone mineral density. Biochem Biophys Res Commun 288:275–279
Maggio D, Barabani M, Pierandrei M, Polidori MC, Catani M, Mecocci P, Senin U, Pacifici R, Cherubini A (2003) Marked decrease in plasma antioxidants in aged osteoporotic women: results of a cross-sectional study. J Clin Endocrinol Metab 88:1523–1527
Yalin S, Bagis S, Polat G, Dogruer N, Cenk Aksit S, Hatungil R, Erdogan C (2005) Is there a role of free oxygen radicals in primary male osteoporosis? Clin Exp Rheumatol 23:689–692
Yousefzadeh G, Larijani B, Mohammadirad A, Heshmat R, Dehghan G, Rahimi R, Abdollahi M (2006) Determination of oxidative stress status and concentration of TGF-beta 1 in the blood and saliva of osteoporotic subjects. Ann N Y Acad Sci 1091:142–150
Mangiafico RA, Malaponte G, Pennisi P, Li Volti G, Trovato G, Mangiafico M, Bevelacqua Y, Mazza F, Fiore CE (2007) Increased formation of 8-iso-prostaglandin F2α is associated with altered bone metabolism and lower bone mass in hypercholesterolaemic subjects. J Intern Med 261:587–596
Ostman B, Michaëlsson K, Helmersson J, Byberg L, Gedeborg R, Melhus H, Basu S (2009) Oxidative stress and bone mineral density in elderly men: antioxidant activity of alpha-tocopherol. Free Radic Biol Med 47:668–673
Sánchez-Rodríguez MA, Ruiz-Ramos M, Correa-Muñoz E, Mendoza-Núñez VM (2007) Oxidative stress as a risk factor for osteoporosis in elderly Mexicans as characterized by antioxidant enzymes. BMC Musculoskelet Disord 8:124
Loft S, Fischer-Nielsen A, Jeding IB, Vistisen K, Poulsen HE (1993) 8-Hydroxydeoxyguanosine as a urinary biomarker of oxidative DNA damage. J Toxicol Environ Health 40:391–404
Fischer-Nielsen A, Jeding IB, Loft S (1994) Radiation-induced formation of 8-hydroxy-2′-deoxyguanosine and its prevention by scavengers. Carcinogenesis 15:1609–1612
Loft S, Vistisen K, Ewertz M, Tjonneland A, Overvad K, Poulsen HE (1992) Oxidative DNA damage estimated by 8-hydroxydeoxyguanosine excretion in humans: influence of smoking, gender and body mass index. Carcinogenesis 13:2241–2247
Dandona P, Thusu K, Cook S, Snyder B, Makowski J, Armstrong D, Nicotera T (1996) Oxidative damage to DNA in diabetes mellitus. Lancet 347:444–445
Djordjevic VB (2004) Free radicals in cell biology. Int Rev Cytol 237:57–89
Suda N, Morita I, Kuroda T, Murota S (1993) Participation of oxidative stress in the process of osteoclast differentiation. Biochim Biophys Acta 1157:318–323
Fraser JH, Helfrich MH, Wallace HM, Ralston SH (1996) Hydrogen peroxide, but not superoxide, stimulates bone resorption in mouse calvariae. Bone 19:223–226
Kim HJ, Chang EJ, Kim HM, Lee SB, Kim HD, Su Kim G, Kim HH (2006) Antioxidant alpha-lipoic acid inhibits osteoclast differentiation by reducing nuclear factor-kappaB DNA binding and prevents in vivo bone resorption induced by receptor activator of nuclear factor-kappaB ligand and tumor necrosis factor-alpha. Free Radic Biol Med 40:1483–1493
MacDonald BR, Takahashi N, McManus LM, Holahan J, Mundy GR, Roodman GD (1987) Formation of multinucleated cells that respond to osteotropic hormones in long term human bone marrow cultures. Endocrinology 120:2326–2333
Moller P, Wallin H, Knudsen LE (1996) Oxidative stress associated with exercise, psychological stress and life-style factors. Chem Biol Interact 102:17–36
Sontakke AN, Tare RS (2002) A duality in the roles of reactive oxygen species with respect to bone metabolism. Clin Chim Acta 318:145–148
Bai XC, Lu D, Liu AL, Zhang ZM, Li XM, Zou ZP, Zeng WS, Cheng BL, Luo SQ (2005) Reactive oxygen species stimulates receptor activator of NF-kappaB ligand expression in osteoblast. J Biol Chem 280:17497–17506
Takeuchi T, Nakajima M, Morimoto K (1996) Relationship between the intracellular reactive oxygen species and the induction of oxidative DNA damage in human neutrophil-like cells. Carcinogenesis 17:1543–1548
Valko M, Izakovic M, Mazur M, Rhodes CJ, Telser J (2004) Role of oxygen radicals in DNA damage and cancer incidence. Mol Cell Biochem 266:37–56
Valavanidis A, Vlachogianni T, Fiotakis C (2009) 8-Hydroxy-2′-deoxyguanosine (8-OHdG): a critical biomarker of oxidative stress and carcinogenesis. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev 27:120–139
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have stated that they have no conflict of interest.
Rights and permissions
About this article
Cite this article
Baek, K.H., Oh, K.W., Lee, W.Y. et al. Association of Oxidative Stress with Postmenopausal Osteoporosis and the Effects of Hydrogen Peroxide on Osteoclast Formation in Human Bone Marrow Cell Cultures. Calcif Tissue Int 87, 226–235 (2010). https://doi.org/10.1007/s00223-010-9393-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-010-9393-9