
Abstract
Hypophosphatemic rickets (HR) is a group of rare disorders caused by excessive renal phosphate wasting. The purpose of this cross-sectional study of 38 HR patients was to characterize the phenotype of adult HR patients. Moreover, skeletal and endodontic severity scores were defined to assess possible gender differences in disease severity in patients with genetically verified X-linked HR. Compared to normal reference data, i.e., z = 0, HR patients had significantly lower final height, with a mean difference in z-score of −1.9 (95% CI −2.4 to −1.4, P < 0.001). Compared to paired z-scores of final height, z-scores of leg length were significantly lower and those of sitting height were significantly higher (P < 0.001), resulting in disproportion as indicated by the significantly elevated sitting height ratio, mean difference in z-score of 2.6 (95% CI 2.1–3.1, P < 0.001). Z-scores of head circumference (median 1.4, range −0.4 to 5.5, P < 0.001) and z-scores of bone mineral density (BMD) of the lumbar spine (median 1.9, range −1.5 to 8.6, P < 0.001) were significantly elevated compared to normal reference data. The relative risk (RR) of fracture was reduced (RR = 0.34, 95% CI 0.20–0.57, P < 0.001). The skeletal severity score tended to be higher in males compared to females (P = 0.07), and no gender difference in endodontic severity was found. In conclusion, adult HR patients were characterized by short stature and were disproportioned. They had elevated BMD of the lumbar spine and a reduced risk of fractures. We found a tendency for males to be more severely affected than females.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Hypophosphatemic rickets (HR) is a group of diseases sharing similar biochemical phenotypes with excessive renal phosphate (PO4) wasting, low serum PO4, and inappropriately low serum 1,25-dihydroxyvitamin D (1,25[OH]2D) when the hypophosphatemia is taken into account [1]. HR can be divided into fibroblast growth factor 23 (FGF23)—associated HR, where a disturbance in the regulation of the FGF23 synthesis is considered the primary factor determining the excessive renal PO4 wasting, and non-FGF23-associated HR, where factors other than FGF23 determine the excessive renal PO4 wasting. The most common inherited type is FGF23-associated X-linked HR, caused by mutation in the PHEX gene. HR is a rare disease, with an incidence of 3.9 per 100,000 live births and a prevalence of 4.8 per 100,000 [2]. The disease is usually diagnosed within the first years of life by recognition of the clinical signs of rickets: bowing of the weight-bearing extremities, widening of the methaphyses, and growth failure. The diagnosis is established by a persistently reduced renal tubular reabsorption of PO4 in the urine per milliliter glomerular filtration rate (TPO4/GFR), low serum PO4, in children elevated serum alkaline phosphatase (ALP), and, if possible, detection of a mutation in one of the genes known to cause HR [3].
Only a few studies describe HR in adults [4–8], and the skeletal and endodontic complications associated with the disease in adulthood are not well characterized. The dental term endodontic refers to the diseases of the pulp and periapical tissues. Also, diverging reports of possible gender differences in HR patients have been published, reporting no gender differences [9–11] or that males are more severely affected than females [7, 8, 12–17]. With the exception of one study of eight PHEX-positive children [11], these studies were all based on the assumption that the patients had X-linked HR but included no genetic analyses.
The aim of this study was to characterize the phenotype of adult HR patients. Moreover, we established skeletal and endodontic severity scores, enabling a comparison between genders.
Materials and Methods
Study Design and Recruitment of HR Patients
This cross-sectional study of HR was performed in Denmark at Odense University Hospital, the Hospital of Southwest Denmark, and the School of Dentistry, Aarhus University, during 2006–2008. The participants with potential HR were recruited in three different ways (Fig. 1): (1) by register search, based on the diagnosis codes 273.40 and E83.3 (International Statistical Classification of Diseases, revisions 8 and 10) in the Danish National Patient Registry in 1977–2005, with an identical survey performed in hospital registers in the region of Southern Denmark in 1985–2006 and in the former Aarhus County in 1989–2006; (2) by contact with doctors known to treat patients with HR; and (3) by screening of first-degree relatives and symptomatic second-degree relatives of participating HR patients.

Flow diagram of patient inclusion
The criteria for inclusion were hereditary and FGF23-associated HR. The diagnostic criteria were (1) genetically verified HR by detection of a disease-causing mutation in the PHEX, FGF23, or DMP1 gene and/or (2) biochemically verified HR with at least one of the following: serum PO4 below normal range, low TPO4/GFR, or elevated serum FGF23. In addition, a history of childhood rickets or spontaneous endodontic abscesses was required to exclude acquired HR, e.g., tumor-induced osteomalacia. Ten previously undiagnosed adult patients were included from a large kindred of HR exhibiting an X-linked dominant trait, in which the genetic mutation has yet to be detected. From this family, four females had no history of rickets or spontaneous endodontic abscesses, but they all had children with verified HR.
The exclusion criteria were non-FGF23-associated HR, acquired HR, and sporadic, nonhereditary HR, e.g., McCune-Albright syndrome. Patients with these differential diagnoses were excluded by review of their medical records, screening for mutations in the SCL34A3 gene (hereditary HR with hypercalciuria) and the CLCN5 gene (X-linked recessive HR), and biochemical evaluation. Children (aged < 18 years) were excluded from the present study.
Genetic Analysis
Genomic DNA was extracted from full blood using a DNA purification robot (Maxwell®; Promega, Ramcon, Birkeroed, Denmark) and analyzed for mutations in the PHEX, FGF23, DMP1, SCL34A3, and CLCN5 genes. Polymerase chain reaction was used, covering all introns and intron–exon boundaries, followed by denaturing high-performance liquid chromatography (dHPLC) analysis (WAVE 3500HT High Sensitivity System; Transgenomic, Elancourt, France), testing for small deletions, insertions, or point mutations in all exons and exon–intron boundaries of all genes. Samples with deviating chromatographic profiles were sequenced in both directions using the BigDye® Terminator v3.1 Cycle Sequencing Kit and analyzed on a 3730XL DNA Analyzer (Applied Biosystems, Foster City, CA). Sequence analysis was performed using SeqMan software (DNA STAR, Madison, WI). Mutational analysis of the PHEX and FGF23 genes was performed by use of the primers described by Goji et al. [18], and mutational analysis of the CLCN5 gene was performed by use of the primers published by Lloyd et al. [19]. We designed primers using Primer Select Software (DNA STAR) for mutational analysis of the DMP1, FGF23, and SCL34A3 genes. To detect larger deletions of the PHEX and FGF23 genes, a multiplex ligation–dependent probe amplification (MLPA) analysis was performed in patients with no mutations detected by dHPLC. The MLPA procedure was performed according to the manufacturer’s recommendations (MRC-Holland, Amsterdam, The Netherlands) and run on the 3730XL DNA analyzer using GeneMarker software (Softgenetics, State College, PA) for the analysis.
Variables Collected
We obtained a medical history including age at presentation, previous and current treatment, endodontic complications, fractures, and surgical treatment. The following clinical observations were obtained: height, sitting height, leg length, arm span, head circumference, and leg deformities. Sitting height ratio was calculated as sitting height divided by height. To allow comparison between genders, calculations of z-scores for height were done by the following equation:
z = (Patient's height − mean normal reference height for sex) / SD of reference height
Other z-scores were calculated using a corresponding equation.
Z-scores of anthropometric data were calculated using reference data as follows: height, Denmark [20]; sitting height, sitting height ratio, leg length, and arm span, Denmark [21]; and head circumference, UK [22]. One patient had a 10-cm surgical lengthening of the legs, and data on height, sitting height ratio, and leg length from this patient were omitted from analysis. Z-scores of leg deformities were calculated by comparing to reference data, France [23]. The following measures were obtained: genu varum, distance between medial femoral condyles; genu valgum, distance between medial tibial malleolus. Ranges of movement (ROM) of the hip were assessed and when different ROM in the right and left hips were recorded, the lowest was used.
We defined a skeletal severity score based on the presence of surgical corrections of leg deformities, severity of leg deformities, and height reduction (Table 1). Joint pain was graduated as follows: 0, no pain; 1, mild with no limitation of activities; 2, moderate with limitation of activities; 3, severe with serious limitation of activities.
X-rays of the ankles, knees, pelvis including hips, and lumbar spine (anterior and posterior projections) were obtained. Osteoarthrosis of the ankles, knees, and hips and enthesopathies, defined as bone proliferation at sites of ligament attachments or calcification of ligaments, were recorded. Dual-energy X-ray absorptiometric (DEXA) scans of bone mineral density (BMD) of the lumbar spine and hip were obtained by use of two DEXA scanners (Delphi W and Discovery A; Hologic, Waltham, MA).
Fractures were defined as any clinical fracture and based on self-reports. The number of fractures in each HR patient was compared to the number of fractures experienced by three age- and gender-matched Danish normal controls [24]. The relative risk (RR) of fractures in patients was compared to that of controls using incidence rate ratios. Numbers of childbirths and cesarean sections were recorded.
Biochemistry
In patients on current medical treatment, phosphate and alfacalcidol treatment was paused from the evening before the examination. After 2 hours of fasting, blood samples were drawn and urine samples were collected. Serum samples were stored at −80°C and urine samples at −20°C until analysis. All analyses were performed in the same run. Serum FGF23 was analyzed by ELISA (Kainos Laboratories, Tokyo, Japan) with coefficients of variation (CVs) 3.0% and 2.0% at 14.2 and 33.6 pg/mL, respectively. We analyzed serum 25-hydroxyvitamin D (25[OH]D2+3) using an isotope dilution liquid chromatography-tandem mass spectrometry (LC-MS/MS) method. CVs for serum 25(OH)D3 were 9.4% and 8.8% at levels of 32.0 and 59.7 nmol/L and for serum 25(OH)D2 8.6% and 8.0% at levels of 23.4 and 64.4 nmol/L, respectively [25]. Serum 1,25(OH)2D was measured by radioimmunoassay (IDS, Phoenix, AZ) with CVs of 6.8% and 9.0% at levels of 90 and 220 pmol/L, respectively [26]. Serum bone-specific ALP activity (bone ALP) was measured using an enzyme immunoassay (Metra BAP EIA kit; Quidel, San Diego, CA) with CVs of 5.7% and 6.7% at levels of 41.9 and 64.8 U/L [27]. Due to different normal reference values in males and females, z-scores were calculated to allow comparison between genders. According to the method described by Stark et al. [28], TPO4/GFR based on 2-hour fasting blood and urine samples was calculated by use of the equation
where Sp is serum PO4, Up is urine PO4, Scr is serum creatinine, and Ucr is urine creatinine.
Dental Examination
All patients were offered a clinical examination in the Department of Pediatric Dentistry, School of Dentistry, University of Aarhus. Furthermore, a digital panoramic radiograph was performed and examined for endodontically treated teeth and teeth with periapical bone lesions (apical periodontitis). An endodontic severity score was calculated as the number of permanent teeth with apical periodontitis or previous endodontic treatment divided by the total number of teeth (Table 1).
Grouping of Participants
Presence of enthesiopathies was limited to patients aged 40+ years. As this influenced the z-scores of BMD lumbar spine, these data were analyzed according to age above (n = 19) or below 40 years. Mutations in different HR genes might variably influence anthropometric measures. Therefore, the exact measures were reported for PHEX-positive adults only. In the analysis on possible gender differences, only patients with positive PHEX mutation or established X-linked disease were included. Medical treatment with phosphate and alfacalcidol increases serum FGF23 [29–31]; therefore, when biochemical values were compared between genders, only patients not treated medically for the past 6 months were included.
Statistical Analysis
Statistical analysis was performed using SPSS 16.0 (SPSS, Inc., Chicago, IL) and STATA, version 11 (StataCorp, College Station, TX). Normally distributed data were presented as means (95% CI) and skewed data, as medians (range). Student’s t-test was used when comparing normally distributed data, and the Mann–Whitney test was used when comparing skewed variables between groups. Wilcoxon’s paired t-test was used when comparing paired variables following a normal distribution, and Wilcoxon’s signed rank test was used when comparing paired, skewed variables. Pearson’s chi-squared test was used for analysis of bivariate variables, and Fisher’s exact test was used when observed frequencies were less than 5. Odds ratios (ORs) were used when comparing binary outcomes between groups. For categorical responses with more than two outcomes, the OR was estimated using the proportional odds model. For correlation analysis of skewed variables, Spearman’s correlation coefficient (Rho) was calculated. In order to assess gender differences in outcome, controlling for heterogeneity between families (e.g., due to difference in genetic background), standard random effects modeling was applied, taking family as a random intercept [32]. Due to small groups, this adjustment of between-family variations could not be applied when considering gender differences in biochemical values.
Ethics
The study was approved by the Ethics Committee of Southern Denmark (M-2678-05) and by the Danish Data Protection Agency (2004-41-4699). Written informed consent was obtained from all patients before entering the study.
Results
Patients Identified with HR
A register search identified 52 patients with potential HR (Fig. 1). Contact with treating doctors identified further 14 patients not found by the register search as they were entered with diagnosis codes other than 273.40 or E83.3. Finally, family screening identified 31 relatives suspected of having HR. Overall, 11 patients did not respond to the invitation or refused to participate. Subsequently, 27 cases were excluded as they did not fulfill the diagnostic inclusion criteria of hereditary, FGF23-associated HR. Of the 59 patients with HR, 38 were adults. Thus, this report is based on 38 adults with genetically and/or biochemically confirmed HR. They originated from 11 families comprising 32 patients, and in six patients HR was sporadic, giving a total of 17 probands.
Results from the Genetic Mutation Analyses
PHEX mutations were identified in 14 of the 17 probands. Five of the PHEX mutations have been reported previously in the literature or entered in the PHEXdb (http://www.phexdb.mcgill.ca/, accessed May 28, 2009). PHEX mutations were also identified in all 11 family members of the nine PHEX-positive probands. The PHEX mutation was found by the dHPLC method in 12 of 14 probands, and in two probands with larger deletions it was identified by MLPA analysis. Three probands were tested negative for mutation in the PHEX, FGF23, DMP1, SCL34A3, and CLCN5 genes by dHPLC and for larger PHEX and FGF23 deletions by MLPA analysis. In one family, where no mutation to date has been found, the trait was inherited in an X-linked dominant fashion. The family is referred to as “family X” and comprises 10 adults and six children with verified HR. A genomewide linkage scan in this family revealed strong evidence of linkage to the PHEX locus (Lod score +4.8), and their disease is considered as FGF23-associated and most probably due to a mutation in PHEX that was not detected by either the dHPLC or the MLPA analysis. Overall, 25 patients had a PHEX mutation identified and 10 had X-linked disease according to the linkage scan, adding up to a total of 35 patients with verified X-linked disease.
Anthropometric Characteristics in HR Patients
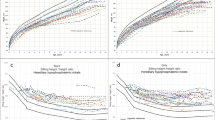
Patients with HR had a significantly lower final height, with a mean difference in z-score of −1.9 (95% CI, −2.4 to −1.4, P < 0.001) compared to reference data, i.e., z = 0. Compared to paired z-scores of final height, z-scores of leg length (median −2.7, −7.5 to −0.8) were significantly more reduced (P < 0.001) and paired z-scores of sitting height (mean −1.1, −3.5 to 1.7) were significantly higher (P < 0.001). Accordingly, the patients appeared disproportioned, as indicated by the significantly elevated z-scores of sitting height ratio (mean difference 2.6, 95% CI 2.1–3.1, P < 0.001), compared to reference data. The paired z-scores of height and arm span indicated relatively short arms compared to height (P = 0.06). The median z-scores of head circumference (1.4, −0.4 to 5.5) were significantly elevated compared to reference data (P < 0.001), and in 13 (34%) patients the z-score exceeded 2 SD (Fig. 2). To calculate the possible contribution of the deformities of the legs to the shortness of stature, Spearman’s correlation coefficient of paired z-scores of leg deformities and z-scores of height was calculated in patients with no previous surgeries. No correlation was found in the total HR group or in the group comprising PHEX-positives only, with Rho = −0.31, P = 0.2 and −0.11, P = 0.8, respectively. The anthropometric measures, according to gender in PHEX-positive patients, are listed in Table 2.

Z-scores of anthropometric data and BMD in adult HR patients. HR patients had a reduced final height, short legs, and reduced arm span compared to final height and appeared disproportioned as indicated by the elevated sitting height ratio. They had very large head circumferences, and lumbar spine BMD was elevated, in some cases markedly so
Assessing Skeletal Severity Score and Pain Score
The skeletal severity score was 1.6 (1–2). One or more surgical corrections of the leg deformities by osteotomy were performed in 18 (47%) of the HR patients. The joint pain score was 1.4 (0–3), where pain in the knees was reported by 23 (61%), followed by painful ankles and hip pain in 19 (50%) and 15 (40%), respectively. Only four patients, all aged 40+ years, reported severe pain with serious limitation of activities (score 3). There was no difference in the joint pain score when comparing HR patients aged less than 40 years with patients aged 40+ years, pain scores 1.2 (0–2) and 1.6 (0–3), respectively. ROM of the hip was assessed in 37 patients, and all had an internal rotation below the normal 40 degrees. In 14 (38%), no internal rotation of at least one hip was present. Limited flexion (below 140 degrees) was present in 36 (97%), and extension below 15 degrees was seen in 18 (49%), of whom eight (44%) had no extension in both hips. Patients aged 40+ years with decreased ROM had significantly lower ROM of internal rotation (P < 0.001), flexion (P = 0.03), and extension (P = 0.04) compared to patients younger than 40 years.
Presence of Arthrosis and Enthesiopathies
Skeletal X-rays were obtained in 35 adult patients. Radiologic signs of arthrosis were present in at least one hip, knee, or ankle in nine (26%), nine (26%), and four (11%) of the HR patients, respectively. Arthrosis of at least one of the above-mentioned joints was present in four (25%) of the 16 patients less than 40 years of age and in 11 (58%) of the 19 patients 40+ years of age (P = 0.05). Enthesiopathies and calcification of the collateral ligaments between the vertebrae were seen only in patients aged 40 years or more and were present in 16 (84%) in that age group.
BMD in HR Patients
The median z-score of lumbar spine BMD (L2–L4) was 1.9 (−1.5 to 8.6) and mean z-score of hip BMD was 0.9 (−2.1 to 5.1) (Fig. 2). Patients aged less than 40 years had significantly lower median lumbar spine z-score compared to patients aged 40+ years, 0.5 (−1.5 to 4.2) and 3.9 (−1.0 to 8.6), respectively (P < 0.01). There was no statistical difference in the mean z-scores of the hip comparing patients aged below and above 40 years, 0.8 (−2.1 to 5.1) and 1.0 (−1.7 to 2.9), respectively. A significant positive correlation was found between the z-scores for the lumbar spine and hip (Rho = 0.61, P < 0.001). The difference regarding z-scores in L2–L4 and hip was significantly larger in patients with enthesiopathies of the lumbar spine compared to patients without (median 2.9, −0.3 to 5.3, and 0.3, −3.4 to 3.5; P < 0.01).
Risk of Fracture
Overall, seven (18%) of the HR patients had experienced a fracture. Three patients suffered one fracture, three patients suffered two fractures, and one patient suffered five fractures. The RR of fracture among HR patients compared with controls was 0.34 (95% CI 0.20–0.57, P < 0.001). Patients from family X had not experienced any fractures, giving a reduced RR of fractures of 0.00 (95% CI 0.00–0.00, P < 0.001). In PHEX-positive patients, the RR of fractures was 0.46 (95% CI 0.26–0.81, P < 0.01).
Frequency of Cesarean Section and Spinal Stenosis
The 25 HR women had a total of 36 pregnancies, and in three women (representing five of the 36 deliveries [14%]) a cesarean section was performed. Two patients had a history of symptomatic spinal stenosis, diagnosed at age 46 years and 72 years, respectively. One underwent decompression by laminectomy, and in the other patient, the symptoms subsided and surgical treatment was withheld.
Dental Findings
The endodontic severity score was greater than 2 SD over the normal age-matched reference [33] in 26 (72%) of the 36 patients studied. A significantly milder endodontic severity score was found among patients of less than 40 years of age compared to patients aged 40+ years (median 0.11, 0.0–0.71, and 0.41, 0.0–0.88; P < 0.01).
Gender Differences
Overall, 35 patients (11 males and 24 females, giving a male-to-female ratio of 1:2.2) had verified X-linked disease, of whom 25 were PHEX-positive and 10 were from family X (Table 3). No age difference was found between males and females (P = 0.9). There were no significant differences according to gender in anthropometric measures. The OR of males having severe skeletal affection (skeletal severity score = 2) compared to females was 8.2 (95% CI 0.8–80, P = 0.07). The OR of males having one or more osteotomies performed compared to females was 3.5 (95% CI 0.8–16, P = 0.10). The z-scores of leg deformity were not different between genders (P = 0.6). Comparison of biochemical findings between males (n = 7) and females (n = 15) not treated during the past 6 months revealed no statistically significant differences. Endodontic examination was performed in 10 males and 23 females with X-linked HR. The endodontic severity score was not different between genders.
Discussion
The 38 HR patients studied were characterized by short stature, and they appeared disproportioned. Often, pain in the joints was reported, and arthrosis was demonstrated especially in patients aged 40+ years. HR patients were not prone to fractures, and they had an elevated lumbar BMD, sometimes markedly so. They experienced severe endodontic problems in terms of apical periodontitis, and several of their permanent teeth were root-filled. We demonstrated a tendency of males to be skeletally more severely affected compared to females, while the endodontic severity was equal between genders.
Methods of graduation of the skeletal severity among HR children have been proposed by Cho et al. [11]. Their graduation was based on a not further specified “need for orthopedic surgery.” In adults a graduation of skeletal severity upon history of osteotomies and mild or severe bowing of the legs has been proposed but with no definition of mild or severe bowing of the legs [34, 35]. Furthermore, this graduation was applied to the entire family according to the most severely affected family member. Our skeletal severity score is based on the most conspicuous objective findings in HR patients: history of surgical correction of leg deformities, present deformities of the legs, and height reduction. This skeletal severity score takes into account that a deformity of the lower legs exceeding 2 SD is of a severity where surgical correction might be indicated but not necessarily performed. Due to the observation of a great intrafamiliar variance in severity (data not shown), we find it most correct to apply this skeletal severity score to individuals and not to families.
Anthropometric measures among HR patients were overtly different from reference data. HR patients were short of stature and appeared disproportioned, as indicated by the elevated z-score of sitting height ratio caused by the z-score of sitting height being significantly higher than the paired z-score of leg length. Some of the reduction of leg length might be ascribed to deformities of the legs, but even in patients with a z-score of deformities of less than 2, the same significant association was seen. In accordance with the conclusions drawn by McNair and Stickler [36], we found no correlation between paired z-scores of leg deformities and z-scores of height. Their arm span was shorter than normal, indicated by relatively short arms compared to height. HR patients had elevated z-scores of head circumference. It is well known that the skull undergoes mainly membranous ossification. Since the skull grows abnormally more and the rest of the skeleton grows significantly less than normal, we suggest that the influence of HR upon the growth of bones is partly determined by membranous or endochondral ossification, respectively. Thus, our data indicate that the long bones of the legs as well as the arms are more severely growth-retarded than the axial skeleton and that increased growth is seen in the skull.
In HR adults, pain in the knees, ankles, and hips was frequent but severe pain was reported only by patients aged 40+ years. Pain in the same joints was also reported among HR patients from New Zealand [7]. These joints are all affected by a changed anatomical strain due to the deformities of the legs, and we also found a high percentage of arthrosis in these joints in HR patients. Especially ROM of the internal rotation of the hip was reduced in all HR adult patients, also reported in 10 of 13 adult HR patients by Reid et al. [7], and decreased further in patients aged 40+ years.
The z-scores of lumbar spine and hip BMD were elevated compared to Hologic reference data, most pronounced for the lumbar spine. Higher lumbar BMD has previously been demonstrated in two other studies [7, 14]. The HR patients in our study with very high BMD of L2–L4 were primarily aged 40+ years, and the majority had enthesiopathies of the spine visualized by X-ray. Z-scores of L2–L4 exceeding 2 SD were also seen in four patients aged less than 40 years and with no enthesiopathies demonstrated on X-ray. These findings indicate that the high lumbar spine BMD is not solely caused by extraskeletal calcifications. A histologic study of adult patients with HR revealed an elevated trabecular calcified volume, elevated trabecular osteoid volume, and osteoid seam thickness [37]. In some cases, we found a significant discrepancy between the extremely elevated z-score of L2–L4 and the more moderate elevation of z-score of the hip. Since the ratio of trabecular bone to cortical bone is higher in the lumbar spine compared to the hip, the elevated z-score of L2–L4 might reflect an overabundance of partially mineralized osteoid or an increased trabecular bone mass in addition to the presence of extraskeletal calcifications.
The percentage of HR patients suffering from fractures in our study (18%) was lower compared to a German study [4], where 39% of the patients suffered from one or more fractures. Their median age was 29 years, which was lower compared to the patients in our study; thus, the higher percentage of the German patients experiencing a fracture could not be ascribed to a prolonged risk time. Patients from family X did not experience any fractures, and among the PHEX-positive patients the percentage experiencing fractures was 24%, still considerably lower compared to the German HR patients. We calculated a lower RR of fractures in HR patients. Using the estimates by Marshall et al. [38] based on the observed spine BMD of +1.9 z-scores, the expected RR of any fracture was 1.5−1.9 = 0.46, i.e., within the range observed. Much of the decrease in the risk of fractures may, thus, be ascribed to the increased BMD.
In nutritional rickets, the pelvis might become narrowed, causing difficulty in vaginal delivery [39, 40]. A high frequency of cesarean section in 15 of 22 deliveries (68%) was described among HR women in New Zealand; however, only two of the cesarean sections were reported to be attributed to the presence of HR [7]. Nine HR woman from the United States had 31 children, all delivered vaginally [5]. In our study population, the percentage of cesarean section in deliveries in HR women was 14%. These deliveries took place during the time period 1946–2006 (median year 1992). In comparison, the overall percentage of cesarean section in Denmark in 1991 was 12% [41]. Our data support that HR women do not suffer from delivery complications due to contracted pelvis.
Several case reports have described spinal stenosis due to extraskeletal ossifications in HR patients [42–45]. Symptomatic spinal stenosis was a rare complication, seen in two HR patients in our study, both aged 40+ years.
Typical dental abnormalities in HR patients are endodontic complications such as apical periodontitis and numerous spontaneous endodontic abscesses not preceded by decay or trauma to the teeth [46]. As a consequence, the number of endodontically treated teeth is commonly reported to be high in HR patients [46–50]. This is substantiated in our study, in spite of the fact that the reference material used for comparison is considered more sensitive for diagnosing apical periodontitis. Histologically, the dentin appear poorly mineralized, with irregular areas of globular dentin [50]. In addition, the endodontic pulps are enlarged, significantly more in males compared to females [16], and sometimes the pulp horns extend to the dentinoenamel junction [51]. Once abrasion of the enamel has exposed the dentin tubules, the poorly mineralized dentin is a weak barrier to protect the dental pulp from infection by invading bacteria [46]. Formation of incomplete fractures of the enamel (infractions) may contribute to this [51]. In our study, patients aged less than 40 years had a significantly lower endodontic severity score compared to patients aged 40+ years. This might be due to several factors; half of the adults aged less than 40 years had received medical treatment throughout childhood compared to none of the patients aged 40+ years. A close to normal mineralization of the dentin in patients treated with phosphate and alfacalcidol since early childhood has been demonstrated histologically, indicating a treatment effect [52]. Another explanation may be that attrition increases with increasing age.
The male-to-female ratio of 1:2.2 reflects the inheritance of an X-linked disease. The locus on the X chromosome (Xp22.1-p22.2) to which the PHEX gene is mapped undergoes random X-chromosome inactivation [53]. Therefore, a gene dosage effect causing milder disease in females would be expected, but diverging results have been published. Several studies report no gender differences. Reid et al. [7] reported no differences between adult HR males and females regarding renal PO4 reabsorption, serum PO4, and height. Moreover, no difference in bone mass was seen [10]. In a study of children with HR, no gender differences in height, serum PO4, or TPO4/GFR were found [9]. One study of eight PHEX-positive HR children revealed no difference in skeletal or endodontic severity or in serum PO4 [11]. Studies in the HYP mouse (a murine homologue of PHEX gene mutation in humans) revealed no gene dosage effect on the mineralization defect [53]. Some studies have found males to be more affected than females. Rosenthall [14] described a higher lumbar BMD z-score in males, Hardy et al. [8] described more severe radiological disease manifestation in males, a tendency also described by Frymoyer and Hodgkin [12]. A lower TPO4/GFR in males has been described by Glorieux and Scriver [17]. We found no gender differences in anthropometric measures. The skeletal severity score tended to be greater in males compared to females, but this did not reach statistical significance. Osteotomies tended to be performed more often in males compared to females, and since no gender difference was seen in deformities of the legs, females probably avoided surgery, primarily because this was not indicated. There was a tendency of males to have higher BMD of the lumbar spine compared to females. There were no gender differences in the endodontic severity score or the biochemical measures. Since no data pointed toward females being more severely diseased compared to males, it is presumed that the weak statistical strength found in males being skeletally more severely affected compared to females is due to our small sample size. In addition, nonsymptomatic female patients may not be diagnosed and, therefore, not included in this study.
The cross-sectional design of this study gives rise to limitations in the evaluation of possible effects of medical treatment. It does not take differences in disease severity at time of treatment start into account, whereby those treated might be those more severely diseased. In addition, the never-treated patients were significantly older compared to treated patients, providing a higher risk time for e.g., the development of dental abscesses. The dental data obtained in this study will be published in detail separately.
Our study is the first to provide data according to gender in a large cohort of adult patients with verified X-linked HR. With the exception of one small study in children, the existing literature states that the studied cohort of HR patients had X-linked HR yet without demonstration of a corresponding disease-causing mutation in the PHEX gene. Often, the assumption of X-linked HR was based on a trait with X-linked inheritance and a female-to-male ratio greater than 1; but even though male-to-male transmission is not present, it does not exclude the possibility of the autosomal dominant trait of the FGF23 mutation. The three patients where X-linked HR was not proven might carry a PHEX mutation not detected by the dHLPC or MLPA genetic mutational analysis, excluding them from the comparison of severity between genders.
This study reports phenotype characteristics of patients either previously diagnosed with HR or diagnosed through family screening, some of whom displayed very few symptoms. It is likely that even milder cases escaped our attention, and thus, this and other studies presumably reflect the more severe cases of HR.
Adult HR patients were characterized by short stature and appeared disproportioned. They had elevated BMD, especially of the lumbar spine, and complications in terms of arthralgia. Arthrosis and endodontic problems were increasingly present with increasing age. HR patients had a reduced risk of fractures, and HR females had the same rate of cesarean section as the background population. Males tended to be skeletally more severely affected compared to females.
References
Bastepe M, Juppner H (2008) Inherited hypophosphatemic disorders in children and the evolving mechanisms of phosphate regulation. Rev Endocr Metab Disord 9:171–180
Beck-Nielsen SS, Brock-Jacobsen B, Gram J, Brixen K, Jensen TK (2009) Incidence and prevalence of nutritional and hereditary rickets in southern Denmark. Eur J Endocrinol 160:491–497
Drezner MK (2003) Hypophosphatemic rickets. Endocr Dev 6:126–155
Berndt M, Ehrich JH, Lazovic D, Zimmermann J, Hillmann G, Kayser C, Prokop M, Schirg E, Siegert B, Wolff G, Brodehl J (1996) Clinical course of hypophosphatemic rickets in 23 adults. Clin Nephrol 45:33–41
Stickler GB, Morgenstern BZ (1989) Hypophosphataemic rickets: final height and clinical symptoms in adults. Lancet 2:902–905
Sullivan W, Carpenter T, Glorieux F, Travers R, Insogna K (1992) A prospective trial of phosphate and 1,25-dihydroxyvitamin D3 therapy in symptomatic adults with X-linked hypophosphatemic rickets. J Clin Endocrinol Metab 75:879–885
Reid IR, Hardy DC, Murphy WA, Teitelbaum SL, Bergfeld MA, Whyte MP (1989) X-linked hypophosphatemia: a clinical, biochemical, and histopathologic assessment of morbidity in adults. Medicine 68:336–352
Hardy DC, Murphy WA, Siegel BA, Reid IR, Whyte MP (1989) X-linked hypophosphatemia in adults: prevalence of skeletal radiographic and scintigraphic features. Radiology 171:403–414
Whyte MP, Schranck FW, Armamento-Villareal R (1996) X-linked hypophosphatemia: a search for gender, race, anticipation, or parent of origin effects on disease expression in children. J Clin Endocrinol Metab 81:4075–4080
Reid IR, Murphy WA, Hardy DC, Teitelbaum SL, Bergfeld MA, Whyte MP (1991) X-linked hypophosphatemia: skeletal mass in adults assessed by histomorphometry, computed tomography, and absorptiometry. Am J Med 90:63–69
Cho HY, Lee BH, Kang JH, Ha IS, Cheong HI, Choi Y (2005) A clinical and molecular genetic study of hypophosphatemic rickets in children. Pediatr Res 58:329–333
Frymoyer JW, Hodgkin W (1977) Adult-onset vitamin D-resistant hypophosphatemic osteomalacia. A possible variant of vitamin D-resistant rickets. J Bone Joint Surg Am 59:101–106
Glorieux FH, Scriver CR, Reade TM, Goldman H, Roseborough A (1972) Use of phosphate and vitamin D to prevent dwarfism and rickets in X-linked hypophosphatemia. N Engl J Med 287:481–487
Rosenthall L (1993) DEXA bone densitometry measurements in adults with X-linked hypophosphatemia. Clin Nucl Med 18:564–566
Winters RW, Graham JB, Williams TF, McFalls VW, Burnett CH (1957) A genetic study of familial hypophosphatemia and vitamin D resistant rickets. Trans Assoc Am Physicians 70:234–242
Shields ED, Scriver CR, Reade T, Fujiwara TM, Morgan K, Ciampi A, Schwartz S (1990) X-linked hypophosphatemia: the mutant gene is expressed in teeth as well as in kidney. Am J Hum Genet 46:434–442
Glorieux F, Scriver CR (1972) Loss of a parathyroid hormone-sensitive component of phosphate transport in X-linked hypophosphatemia. Science 175:997–1000
Goji K, Ozaki K, Sadewa AH, Nishio H, Matsuo M (2006) Somatic and germline mosaicism for a mutation of the PHEX gene can lead to genetic transmission of X-linked hypophosphatemic rickets that mimics an autosomal dominant trait. J Clin Endocrinol Metab 91:365–370
Lloyd SE, Pearce SH, Gunther W, Kawaguchi H, Igarashi T, Jentsch TJ, Thakker RV (1997) Idiopathic low molecular weight proteinuria associated with hypercalciuric nephrocalcinosis in Japanese children is due to mutations of the renal chloride channel (CLCN5). J Clin Invest 99:967–974
Andersen E, Hutchings B, Jansen J, Nyholm M (1982) Heights and weights of Danish children [in Danish]. Ugeskr Laeger 144:1760–1765
Hertel NT, Scheike T, Juul A, Main KM, Holm K, Bach-Mortensen N, Skakkebaek NE, Muller JR (1995) Body proportions of Danish children. Curves for sitting height ratio, subischial length and arm span [in Danish]. Ugeskr Laeger 157:6876–6881
Bushby KM, Cole T, Matthews JN, Goodship JA (1992) Centiles for adult head circumference. Arch Dis Child 67:1286–1287
Cahuzac JP, Vardon D, de Sales GJ (1995) Development of the clinical tibiofemoral angle in normal adolescents. A study of 427 normal subjects from 10 to 16 years of age. J Bone Joint Surg Br 77:729–732
Vestergaard P (2003) Fracture risk secondary to disease. Thesis, Faellestrykkeriet for Sundhedsvidenskab, Aarhus
Hojskov CS, Heickendorff L, Moller HJ (2010) High-throughput liquid–liquid extraction and LCMSMS assay for determination of circulating 25(OH) vitamin D3 and D2 in the routine clinical laboratory. Clin Chim Acta 411:114–116
Fraser WD, Durham BH, Berry JL, Mawer EB (1997) Measurement of plasma 1,25 dihydroxyvitamin D using a novel immunoextraction technique and immunoassay with iodine labelled vitamin D tracer. Ann Clin Biochem 34:632–637
Gomez B Jr, Ardakani S, Ju J, Jenkins D, Cerelli MJ, Daniloff GY, Kung VT (1995) Monoclonal antibody assay for measuring bone-specific alkaline phosphatase activity in serum. Clin Chem 41:1560–1566
Stark H, Eisenstein B, Tieder M, Rachmel A, Alpert G (1986) Direct measurement of TP/GFR: a simple and reliable parameter of renal phosphate handling. Nephron 44:125–128
Burnett SA, Gunawardene SC, Bringhurst FR, Juppner H, Lee H, Finkelstein JS (2006) Regulation of C-terminal and intact FGF-23 by dietary phosphate in men and women. J Bone Miner Res 21:1187–1196
Alon US, Levy-Olomucki R, Moore WV, Stubbs J, Liu S, Quarles LD (2008) Calcimimetics as an adjuvant treatment for familial hypophosphatemic rickets. Clin J Am Soc Nephrol 3:658–664
Antoniucci DM, Yamashita T, Portale AA (2006) Dietary phosphorus regulates serum fibroblast growth factor-23 concentrations in healthy men. J Clin Endocrinol Metab 91:3144–3149
Rabe-Hesketh S, Skrondal A (1999) Practical statistics for medical research. Chapman & Hall, London
Kirkevang LL (2001) Periapical and endodontic status in Danish populations. Thesis, Royal Dental College, University of Aarhus
Holm IA, Nelson AE, Robinson BG, Mason RS, Marsh DJ, Cowell CT, Carpenter TO (2001) Mutational analysis and genotype–phenotype correlation of the PHEX gene in X-linked hypophosphatemic rickets. J Clin Endocrinol Metab 86:3889–3899
Song HR, Park JW, Cho DY, Yang JH, Yoon HR, Jung SC (2007) PHEX gene mutations and genotype–phenotype analysis of Korean patients with hypophosphatemic rickets. J Korean Med Sci 22:981–986
McNair SL, Stickler GB (1969) Growth in familial hypophosphatemic vitamin-D-resistant rickets. N Engl J Med 281:512–516
Marie PJ, Glorieux FH (1982) Bone histomorphometry in asymptomatic adults with hereditary hypophosphatemic vitamin D-resistant osteomalacia. Metab Bone Dis Relat Res 4:249–253
Marshall D, Johnell O, Wedel H (1996) Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 312:1254–1259
Hochberg Z (2003) Rickets—past and present. Introduction. Endocr Dev 6:1–13
Bishop N (1999) Rickets today—children still need milk and sunshine. N Engl J Med 341:602–604
Sundhedsstyrelsen (2005) Caesarean section on maternal request [on Danish]. Sundhedsstyrelsen, Copenhagen
Bradbury PG, Brenton DP, Stern GM (1987) Neurological involvement in X-linked hypophosphataemic rickets. J Neurol Neurosurg Psychiatry 50:810–812
Dunlop DJ, Stirling AJ (1996) Thoracic spinal cord compression caused by hypophosphataemic rickets: a case report and review of the world literature. Eur Spine J 5:272–274
Soehle M, Casey AT (2002) Cervical spinal cord compression attributable to a calcified intervertebral disc in a patient with X-linked hypophosphatemic rickets: case report and review of the literature. Neurosurgery 51:239–242
Velan GJ, Currier BL, Clarke BL, Yaszemski MJ (2001) Ossification of the posterior longitudinal ligament in vitamin D-resistant rickets: case report and review of the literature. Spine 26:590–593
Chaussain-Miller C, Sinding C, Wolikow M, Lasfargues JJ, Godeau G, Garabedian M (2003) Dental abnormalities in patients with familial hypophosphatemic vitamin D-resistant rickets: prevention by early treatment with 1-hydroxyvitamin D. J Pediatr 142:324–331
Baroncelli GI, Angiolini M, Ninni E, Galli V, Saggese R, Giuca MR (2006) Prevalence and pathogenesis of dental and periodontal lesions in children with X-linked hypophosphatemic rickets. Eur J Paediatr Dent 7:61–66
Goodman JR, Gelbier MJ, Bennett JH, Winter GB (1998) Dental problems associated with hypophosphataemic vitamin D resistant rickets. Int J Paediatr Dent 8:19–28
McWhorter AG, Seale NS (1991) Prevalence of dental abscess in a population of children with vitamin D-resistant rickets. Pediatr Dent 13:91–96
Abe K, Ooshima T, Lily TS, Yasufuku Y, Sobue S (1988) Structural deformities of deciduous teeth in patients with hypophosphatemic vitamin D-resistant rickets. Oral Surg Oral Med Oral Pathol 65:191–198
Chaussain-Miller C, Sinding C, Septier D, Wolikow M, Goldberg M, Garabedian M (2007) Dentin structure in familial hypophosphatemic rickets: benefits of vitamin D and phosphate treatment. Oral Dis 13:482–489
Gaucher C, Boukpessi T, Septier D, Jehan F, Rowe PS, Garabedian M, Goldberg M, Chaussain-Miller C (2009) Dentin noncollagenous matrix proteins in familial hypophosphatemic rickets. Cells Tissues Organs 189:219–223
Qiu ZQ, Travers R, Rauch F, Glorieux FH, Scriver CR, Tenenhouse HS (2004) Effect of gene dose and parental origin on bone histomorphometry in X-linked Hyp mice. Bone 34:134–139
Acknowledgements
We thank Elizabeth Hanmann, Bente Toet, Lise Gedebjerg, and Marianne Boetcher for performing the DEXA scans and collecting the laboratory samples and Inge Moeller for efficient assistance in organizing the dental examinations. This work was funded by grants from the A. J. Andersen og Hustrus Fond, A. P. Moeller Foundation for the Advancement of Medical Science, Herta Christensens Fond, Institute of Clinical Research of the University of Southern Denmark, Direktoer Jacob Madsen og Hustru Olga Madsens Fond, Karola Joergensens Forskningsfond, K. A. Rohde og Hustrus legat, Simon Fougner Hartmanns Familiefond, Else Poulsens mindelegat, Institut for Regional Sundhedsforskning, Danish Dental Association, and Aarhus University Research Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have stated that they have no conflict of interest.
Rights and permissions
About this article
Cite this article
Beck-Nielsen, S.S., Brusgaard, K., Rasmussen, L.M. et al. Phenotype Presentation of Hypophosphatemic Rickets in Adults. Calcif Tissue Int 87, 108–119 (2010). https://doi.org/10.1007/s00223-010-9373-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-010-9373-0