
Abstract
This study was conducted to determine the effectiveness of three forms of vitamin E supplements following nicotine treatment on bone histomorphometric parameters in an adult male rat model. Rats were divided into seven groups: baseline (B, killed without treatment), control (C, normal saline for 4 months), nicotine (N, nicotine for 2 months), nicotine cessation (NC), tocotrienol-enhanced fraction (TEF), gamma-tocotrienol (GTT), and alpha-tocopherol (ATF). Treatments for the NC, TEF, GTT, and ATF groups were performed in two phases. For the first 2 months they were given nicotine (7 mg/kg), and for the following 2 months nicotine administration was stopped and treatments with respective vitamin E preparations (60 mg/kg) were commenced except for the NC group, which was allowed to recover without treatment. Rats in the N and NC groups had lower trabecular bone volume, mineral appositional rate (MAR), and bone formation rate (BFR/BS) and higher single labeled surface and osteoclast surface compared to the C group. Vitamin E treatment reversed these nicotine effects. Both the TEF and GTT groups, but not the ATF group, had a significantly higher trabecular thickness but lower eroded surface (ES/BS) than the C group. The tocotrienol-treated groups had lower ES/BS than the ATF group. The GTT group showed a significantly higher MAR and BFR/BS than the TEF and ATF groups. In conclusion, nicotine induced significant bone loss, while vitamin E supplements not only reversed the effects but also stimulated bone formation significantly above baseline values. Tocotrienol was shown to be slightly superior compared to tocopherol. Thus, vitamin E, especially GTT, may have therapeutic potential to repair bone damage caused by chronic smoking.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Cigarette smoke contains high concentrations of oxidants and free radicals in both gas and particulate phases that may be important in the pathogenesis of smoking-related diseases [1, 2]. These oxygen free radicals may overwhelm antioxidant defenses in the body, resulting in a condition of oxidative stress [3, 4]. Oxygen-derived free radicals are involved in the bone remodeling process by inducing osteoclastogenesis [5, 6] and inhibiting osteoblastic differentiation [7].
Nicotine is the major toxic component of the tar phase of cigarette smoke [8]. Some researchers suggest that nicotine might have a direct action on bone metabolism by influencing the bone remodeling process. Nicotine inhibited collagen synthesis and alkaline phosphatase activity in osteoblast-like cells derived from embryonic chick calvariae [9] and suppressed cellular proliferation in UMR 106-01 rat osteoblastic osteosarcoma cells [10]. In contrast, nicotine appears to stimulate osteoclast resorption in a porcine marrow cell model [11], increase serum interleukin-1 levels [12], and reduce left femoral calcium content in male rats [13].
Animal studies have shown that nicotine exposure leads to oxidative stress. Increased free radical production, as evidenced by changes in intracellular oxidative stress parameters (glutathione [GSH] and malondialdehyde [MDA]) in pancreatic tissue of rats incubated with nicotine levels [14], and increased lipid peroxidation levels in tissues of intraperitoneal nicotine–administered rats have been reported [15]. In addition, nicotine exposure (25–100 μM) to cat ventricular myocytes resulted in free radical–induced DNA damage and an increase in DNA degradation [16]. Previous reports have shown depletion on antioxidants and enhancement of lipid peroxidation by subcutaneous injection of nicotine (2.5 mg/kg) during lung toxicity [17].
Vitamin E is a lipid-soluble natural antioxidant which exists in two forms: tocopherol and tocotrienol. Both forms can be further subdivided into alpha, beta, gamma, and delta subunits. Our own studies have found that a tocotrienol mixture was more potent than tocopherol in preventing the rise of serum interleukin-1 and the deleterious effects of free radicals on trabecular bone structure [18, 19]. Palm vitamin E was found to improve bone metabolism and survival rate in thyrotoxic rats [20]. It has also been found to prevent osteoporosis in orchidectomized growing male rats [21], ovariectomized female rats [22], and dexamethasone-treated rats [23]. In addition, vitamin E deficiency impaired bone calcification in ovariectomized and intact female rats [24], impaired vitamin D metabolism and bone calcium homeostasis in female rats [25], and reduced lumbar bone calcium content in female rats [26].
Based on our previous studies, vitamin E (60 mg/kg) given orally produced significant positive effects on bone metabolism in rats [18–20, 22, 25]. The laboratory animal has a higher metabolic rate due to the larger ratio of surface area to body weight than humans. The dosage comparable to 1 mg/kg in humans, after adjustment for differences in surface area, would be about 10 mg/kg for rodents such as rats and mice [27]. Thus, the vitamin E dose of 60 mg/kg in rats is equivalent to 6 mg/kg in humans or about 420 mg in a human with 70 kg body weight. Oral vitamin E supplementation even at 800 mg/day appears to be safe without producing any signs of toxicity in healthy older adults [28].
The purpose of this study was to determine the effects of nicotine administration through intraperitoneal injection for 2 months, followed by supplementation with three types of vitamin E (tocotrienol-enhanced fraction [TEF], gamma-tocotrienol [GTT], or alpha-tocopherol [ATF]) for 2 months on bone histomorphometric parameters in Sprague-Dawley male rats. The ability of TEF, GTT, and ATF to reverse the effects of nicotine was compared. We hope this study will provide a better understanding of the negative impact of smoking on bone health and offer evidence for the therapeutic potential of vitamin E in osteoporotic patients following cessation of smoking to improve bone health.
Materials and Methods
Animals and Treatment
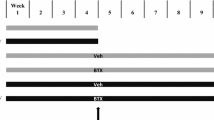
Forty-nine young adult (3 months old) male Sprague-Dawley rats weighing 250–300 g (weight range is not significantly different) at the start of the experiment were obtained from the Laboratory Animal Resource Unit, Faculty of Medicine, Universiti Kebangsaan Malaysia. Rats were randomly assigned to seven groups with seven rats in each group (Table 1). Group 1 was the baseline (B), which was killed at the commencement of the study. Groups 2 and 3 were the control (C) and nicotine (N) groups. The C group was treated with normal saline for 4 months, and the N group was treated with nicotine (7 mg/kg) for 2 months. The other four groups were nicotine cessation (NC), TEF, GTT, and ATF. Treatments for the NC, TEF, GTT, and ATF groups were performed in two phases. For the first 2 months they were given nicotine (7 mg/kg), and for the following 2 months nicotine administration was stopped and treatments with respective vitamin E preparations (60 mg/kg) were commenced except for the NC group, which was allowed to recover without treatment.
Nicotine and normal saline solutions were injected intraperitoneally, while vitamin E and olive oil were given by oral gavage. Rats were kept two to three per cage under 12-hour natural light–dark cycles and given tap water ad libitum. Rats were injected intraperitoneally with 20 mg/kg body weight calcein (Sigma, St. Louis, MO) at 9 days and 2 days before they were killed. After 4 months of treatment (except for B group, which was killed at the commencement of the study, and N group, which was killed after 2 months), rats were anesthetized with diethyl ether and killed by cervical dislocation. The left femora were removed and the distal parts fixed in 70% ethanol. This study was approved by the Universiti Kebangsaan Malaysia Animals Ethics Committee (UKMAEC: FAR/2002/IMA/23-JULY/076).
Diet, Nicotine, and Vitamin E
All rats received normal rat chow obtained from Gold Coin (Port Klang, Malaysia). The nicotine used was nicotine hydrogen tartrate salt, which was purchased from Sigma. Nicotine (7 mg/kg) was prepared by mixing 0.07 g of nicotine in 10 mL normal saline. A total of 0.1 mL/100 g body weight of the preparation was given intraperitoneally 6 days a week according to the respective treatment duration. Vitamin E (3 g) was dissolved in 50 mL olive oil (Bertolli, Lucca, Italy) to obtain a solution suitable for injection at 60 mg/kg rat weight. TEF (alpha-tocotrienol 43%, gamma-tocotrienol 31%, delta-tocotrienol 14%, and other oils 12%) was a gift from the Malaysian Palm Oil Board (Bandar Baru Bangi, Selangor, Malaysia), GTT 90% was supplied by Carotech (Ipoh, Malaysia), and ATF was purchased from Sigma.
Bone Histomorphometry
For structural parameter measurements, which included trabecular bone volume (BV/TV, bone volume over tissue volume), trabecular thickness (Tb.Th), and trabecular number (Tb.N), undecalcified bone samples were embedded in polymer methyl methacrylate (BDH, Poole, UK) according to Difford [29]. Bones were sectioned at 9 μm thickness using a microtome (Leica RM2155, Wetzlar, Germany), stained using a modification of von Kossa’s method [30] and analyzed using an image analyzer (Leica DMRXA2) with the VideoTest-Master software (VideoTest, St.-Petersburg, Russia).
For cellular parameter measurements, which include osteoclast surface (Oc.S/BS, osteoclast surface over bone surface) and eroded surface (ES/BS, eroded surface over bone surface), bone samples were decalcified with ethylene diamine tetraacetic acid (EDTA) for 2 months and embedded in paraffin wax. Paraffin blocks were sectioned at 5 μm thickness with a microtome (Leica RM2135) and stained with hematoxylin and eosin.
Dynamic parameter measurements were determined by using the technique of double fluorescent labeling with calcein at day 9 and day 2 before the rats were killed. Single labeled surface (sLS/BS, single labeled surface over bone surface), mineral appositional rate (MAR), and bone formation rate (BFR/BS, bone formation rate over bone surface) parameters were analyzed from undecalcified samples using a fluorescence microscope (Nikon, Tokyo, Japan). Both cellular and dynamic parameters were measured using the image analyzer (ECLIPSE 80i, Nikon) with software Pro-Plus 5.0 (Media Cybernetics, Silver Spring, MD) and the Weibel et al. technique [31, 32].
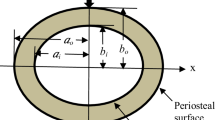
All histomorphometric parameter measurements were performed at the metaphyseal region, which was located 3–7 mm from the lowest point of the growth plate and 1 mm from the lateral cortex, excluding the endocortical region (Fig. 1) [33]. The selected area is the secondary spongiosa area, which is rich in trabecular bone. All parameters were measured according to the American Society of Bone Mineral Research Histomorphometry Nomenclature Committee 1987 [34].

Longitudinal section of distal femur showing margin for sampling in the metaphyseal region. The metaphyseal region was located 3–7 mm from the lowest point of growth plate and 1 mm from the lateral cortex, excluding the endocortical region
Statistical Analysis
Results were expressed as mean ± standard error of the mean (SEM). Data analysis was performed using Statistical Package for Social Sciences (12.0.1; SPSS, Inc., Chicago, IL) software. Data were tested for normality of distribution using the Kolmogorov test. For normally distributed data, the statistical test used was analysis of variance, followed by Tukey’s honestly significant difference test.
Results
Bone Histomorphometry
The C group showed no significant changes in all parameters compared to the B group (Figs. 2a, b and 3a, b, Table 2). Rats in the N and NC groups had lower BV/TV, MAR, and BFR/BS and higher Oc.S/BS, sLS/BS, and ES/BS compared to those in the C group (Figs. 2a–d and 3a–d, Table 2).

Photomicrographs of trabecular bone. Undecalcified section (100× magnification) shows trabecular bone (black) with white background stain using the von Kossa method in seven groups. Note that the vitamin E–treated groups (TEF, GTT, ATF) showed higher trabecular volume (BV/TV) and trabecular thickness (Tb.Th) relative to the other groups. B, baseline (killed without treatment); C, control (no treatment, 4 months); N, nicotine (7 mg/kg nicotine, 2 months); NC, nicotine cessation (7 mg/kg nicotine, 2 months, + no treatment, 2 months); TEF, tocotrienol-enhanced fraction (7 mg/kg nicotine, 2 months, + TEF 60 mg/kg, 2 months); GTT, gamma-tocotrienol (7 mg/kg nicotine, 2 months, + GTT 60 mg/kg, 2 months); ATF, alpha-tocopherol (7 mg/kg nicotine, 2 months, + ATF 60 mg/kg, 2 months)

Photomicrograph shows calcein labels along trabecular bone, demonstrated using fluorescence microscopy in an undecalcified section without staining in seven groups (magnification ×200). Note that N and NC groups showed thin mineral appositional rate (MAR, interlabeled distance) compared to the other groups, while the vitamin E-treated group differed. The vitamin E-treated groups (TEF, GTT, ATF) also have lower single labeled surface (sLS) relative to the other control groups. B, baseline (killed without treatment); C, control (no treatment, 4 months); N, nicotine (7 mg/kg nicotine, 2 months); NC, nicotine cessation (7 mg/kg nicotine, 2 months, + no treatment, 2 months); TEF, tocotrienol-enhanced fraction (7 mg/kg nicotine, 2 months, + TEF 60 mg/kg, 2 months); GTT, gamma-tocotrienol (7 mg/kg nicotine, 2 months, + GTT 60 mg/kg, 2 months); ATF, alpha-tocopherol (7 mg/kg nicotine, 2 months, + ATF 60 mg/kg, 2 months)
In contrast, vitamin E treatment reversed the nicotine effects by improving trabecular bone histomorphometric parameters. All vitamin E–treated groups (TEF, GTT, ATF) showed a significant increase in BV/TV, MAR, and BFR/BS but reduction in sLS/BS and Oc.S/BS compared to the C, N, and NC groups (Figs. 2b–g and 3b–g, Table 2). Both tocotrienol-treated groups (TEF, GTT) had significantly higher Tb.Th and Ob.S/BS but lower ES/BS than the C group. These changes were not observed in the ATF group (Fig. 2b, e–g, Table 2). Both tocotrienol-treated groups also had significantly reduced ES/BS to a greater extent than the ATF group. The ATF and GTT groups, but not the TEF group, showed significantly higher Tb.N compared to the NC group (Fig. 2d–g, Table 2). Furthermore, the GTT group showed a significantly higher MAR and BFR/BS than both the TEF and ATF groups (Fig. 3e–g, Table 2).
Discussion
The purpose of the study was to evaluate the effects of nicotine administration and vitamin E supplementation on bone histomorphometric parameters in the male rat model. The rat has become a widely accepted model of human bone disease because of the similar mechanism control gain and loss of bone mass in young and aged rats as in humans. An increase in bone mass is observed with longitudinal bone growth and modeling drifts with bone loss related to bone remodeling. Furthermore, the response to mechanical influences, hormones, drugs, and other agents is similar in rats and humans [35]. Boran et al. [36] also demonstrated that rats possess remodeling activity similar to higher mammals in caudal vertebrae cancellous bone, which was confirmed by Erben [37].
The C group showed no significant changes in all parameters compared to the B group. These results were consistent with those of Wronski et al. [38], which showed that cancellous bone volume remained constant at 25–30% until 12 months of age and then decreased to 10% at 21 months of age in untreated rats.
The results of the bone histomorphometric analysis showed that nicotine (7 mg/kg) for 2 months in both the N and NC groups increased osteoclastic bone resorption and decreased bone formation as indicated by significant reduction in BV/TV, MAR, and BFR/BS values, while Oc.S/BS, ES/BS, and sLS/BS were increased compared to the C group. Normal bone remodeling, or bone turnover, is an ongoing process that results from the continuous resorption of mineralized matrix coupled with the subsequent replacement of lost bone. Thus, these results showed an imbalance in bone remodeling in the N and NC groups, while cessation of nicotine treatment for 2 months prior to death in the NC group did not improve the bone histomorphometric parameters to control levels.
There is little information on animal studies regarding the effects of nicotine cessation on bone. Wing et al. [39] reported that, based on biomechanical and histological analyses, there were no significant differences on the effects of autogenous iliac crest bone graft on lumbar vertebrae bone fusion in rabbits between a group exposed to chronic nicotine for 8 weeks and another group which discontinued nicotine exposure for 1 week before surgery. In addition, human studies have reported that the risk of hip fracture in men only reduced after 5 years’ cessation of smoking [40] and that bone mineral density (BMD) in former smokers was lower compared with never smokers but similar to that of current smokers [41]. Szulc et al. [41] suggested that former smokers do not lose or regain BMD after cessation of smoking. Recently, Krall et al. [42] suggested that the risk of tooth loss decreases upon smoking cessation, but it may take at least 9–12 years of abstinence for the risk to return to the level of never smokers. Therefore, cessation of nicotine may present a positive impact on bone if the cessation period is prolonged.
The nicotine dose (7 mg/kg) chosen in this study was the optimum dose which affected the bone based on our preliminary studies. Treatment with nicotine 7 mg/kg body weight for 4 weeks was found to increase bone resorption by induction of the bone-resorbing cytokines interleukin-1 and interleukin-6 [12]. Serum calcium levels and normal body growth were impaired in the group given nicotine 7 mg/kg for 2 months, but no significant differences were observed at lower doses of 3 and 5 mg/kg body weight [13]. In addition, the 7 mg/kg dose used in this study is similar to that of humans who smoked moderately 10–20 cigarettes per day [43].
Although previous animal studies had shown that nicotine is a risk factor for osteoporosis [44–46], several animal studies also reported that nicotine did not cause any adverse effects on bone healing, mass, strength, and turnover rate [47–49]. This may be due to differences in species, dosage, treatment period, and method of nicotine administration. In studies done by Syversen et al. [47], Fung et al. [48], and Iwaniec et al. [49], female rats were given nicotine via implanted osmotic minipumps or inhalation. Based on a study by Riesenfeld [50], Fisher and Buffalo female rats tolerated nicotine better than male rats. Therefore, a study on male rats may give results faster than a study on female rats. The effects of nicotine on bones of female rats may only be observed if the treatment period is prolonged.
In addition, other researchers observed that cessation of smoking may reverse tobacco’s harmful effects on bone [51–53]. Studies done by Cesar-Neto et al. [51, 52], which measured the radiographic and histometric parameters of the tibial and mandibular bone of male Wistar rats, demonstrated that continuous exposure to cigarette smoke inhalation presented a reduced BMD and a decreased proportion of mineralized tissue compared to control and cessation groups and that cigarette smoke inhalation cessation results in a return toward the level of the control group. In 2006, Oncken et al. [53] reported that cessation of smoking for 1 year improved BMD at the femoral trochanter and total hip in postmenopausal women but that changes in BMD at the femoral neck, radius, spine, and total body did not significantly differ between quitters and those who continued smoking. We did not observe reversion of nicotine’s harmful effects in the NC group upon cessation of nicotine administration. This may be attributed to the differences in the mode of cigarette exposure, percentage of nicotine absorbed, genetics, types of bone studied, age, or measurement indices.
In the present study, the negative effects of nicotine on bone were found to be reversed in the vitamin E–treated groups. All vitamin E–treated groups showed a significant increase in BV/TV, MAR, and BFR/BS (indicators of bone formation) and a decrease in sLS/BS and Oc.S/BS (indicators of bone resorption) compared to the C, N, and NC groups. These results showed that vitamin E supplementation for only 2 months improved not only the damage caused by nicotine on bone but also trabecular bone parameters compared to the C group, which received normal saline for 4 months. It also showed that recovery after vitamin E supplementation was much better than unsupplemented recovery after cessation of nicotine treatment as observed in the NC group. Therefore, these findings suggest that vitamin E might act on bone via its antioxidant effects. Since previous studies showed that nicotine induced oxidative stress [14–17], which in turn led to bone loss [43–46], it is postulated that vitamin E reversed the effects of nicotine by means of its antioxidant activities. The above finding also suggested the possibility of anabolic effects of vitamin E. However, no studies have shown that vitamin E possesses this effect, and further studies might be needed.
Recently, Pasco et al. [54] suggested that vitamin E or C supplements may suppress bone resorption in nonsmoking posmenopausal women. Nafeeza et al. [55] found that daily supplementation with 200 mg of vitamin E for 8 weeks decreased oxidative stress in smokers. Vitamin E has been shown to increase MAR and BFR and maintain normal bone growth in young growing chicks [56] and to prevent osteoporosis in orchidectomized growing male rats [21] and in ovariectomized female rats [22]. Vitamin E supplementation was also shown to have positive effects on bone strength and bone metabolism in animal models [57, 58]. These studies on humans and other animals contribute to the growing evidence that vitamin E may play a role in preventing osteoporosis by increasing bone formation and suppressing bone resorption.
In the literature, previous animal studies have shown that vitamin E produces positive effects on bone metabolism [18–22, 56–58]; however, the anabolic effects of vitamin E on bone have not yet been clarified. It is well established that parathyroid hormone (PTH) induced anabolic effects on bone [59–63]. PTH given intermittently stimulated bone growth and differentiation of osteoprogenitor cells in bone marrow [59] and increased cancellous bone formation in rats [60]. Jiang et al. [61] and Neer et al. [62] have provided evidence that treatment with human PTH significantly increased cancellous bone volume and connectivity, improved trabecular morphology, increased cortical bone thickness [61], increased total-body BMD, and decreased the risk of nonvertebral (femur) and vertebral fractures [62, 63] in postmenopausal women with osteoporosis. At present, PTH is the only known clinical agent which is capable of increasing trabecular bone formation while reducing fracture incidence in osteoporostic humans [61–63]. Based on our results, it seems that vitamin E might have similar effects as PTH on bone metabolism. Thus, PTH therapy in combination with vitamin E might be an alternative therapeutic option for the osteoporotic patient. However, future studies, especially on humans, are needed to strengthen and validate these findings in human bone.
Comparison between vitamin E–treated groups showed that GTT improved the trabecular bone histomorphometric parameters better than TEF and ATF after nicotine administration by increasing MAR and BFR/BS. In addition, both tocotrienol groups (TEF, GTT), but not ATF, had higher Tb.Th but lower ES/BS than the C group. TEF and GTT also reduced ES/BS better than ATF. This finding was consistent with our previous studies on both biochemical and histomorphometric analyses, which found that a palm oil tocotrienol mixture was more potent than ATF at protecting the bone from the deleterious effects of free radicals on BV/TV and Tb.Th and preventing the rise of the bone-resorbing cytokine interleukin-1 [18, 19, 64]. Supplementation with GTT 60 mg/kg rat weight, but not ATF 60 mg/kg rat weight or a mixture of alpha-tocopherol and tocotrienols, was found to preserve vitamin D metabolism and maintain calcium homeostasis [25]. Recently, Norazlina et al. [65] found that a palm vitamin E mixture 60 mg/kg was better than alpha-tocopherol 60 mg/kg at reversing the effects of nicotine on bone-resorbing cytokines (IL-1 and IL-6).
In conclusion, treatment with nicotine 7 mg/kg for 2 months was found to adversely affect bone histomorphometric parameters and cessation of nicotine for 2 months did not return the histomorphometric parameters to control levels. On the other hand, treatment with vitamin E 60 mg/kg for 2 months reversed the adverse effects of nicotine by improving the structure and cellular properties of the trabecular bone. Vitamin E–treated groups also had better trabecular bone properties than the control group. Tocotrienols were shown to be slightly superior compared to tocopherol. Therefore, vitamin E, especially GTT, may have some therapeutic potential in patients following cessation of smoking to further improve bone health.
References
Church DF, Pryor WA (1985) Free-radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect 64:111–126
Pryor WA, Stone K (1993) Oxidants in cigarette smoke. Radicals, hydrogen peroxide, peroxynitrate, and peroxynitrite. Ann NY Acad Sci 28:12–27
Morrow JD, Frei B, Longmire AW, Gaziano JM, Lynch SM, Shyr Y, Strauss WE, Oates JA, Robert LJ (1995) Increase in circulating products of lipid peroxidation (F2-isoprostanes) in smokers. Smoking as a cause of oxidative damage. N Engl J Med 332:1198–1203
Duthie GG, Arthur JR, James WP (1991) Effects of smoking and vitamin E on blood antioxidant status. Am J Clin Nutr 53:1061S–1063S
Garrett IR, Boyce BF, Oreffo ROC, Bonewald L, Poser J, Mundy GR (1990) Oxygen-derived free radicals stimulate osteoclastic bone resorption in rodent bone in vitro and in vivo. J Clin Invest 85:632–639
Suda N, Morita I, Kurodo T, Murot S (1993) Participitation of oxidative stress in the process of osteoclast differentiation. Biochim Biophys Acta 1157:318–323
Mody N, Parhami F, Sarafian TA, Demer DL (2001) Oxidative stress modulates osteoblastic differentiation of vascular and bone cells. Free Radic Biol Med 31:509–519
Wynder EL, Hoffmann D (1979) Tobacco and health. A societal challenge. N Engl J Med 300:894–903
Ramp WK, Lenz LG, Galvin RJ (1991) Nicotine inhibits collagen synthesis and alkaline phosphatase activity but stimulates DNA synthesis in osteoblast-like cells. Proc Soc Exp Biol Med 197:36–43
Fang MA, Frost PJ, Iida-Klein A, Hahn TJ (1991) Effects of nicotine on cellular function in UMR 106-01 osteoblast-like cells. Bone 12:283–286
Henemyre CL, Scales DK, Hokett SD, Cuenin MF, Peacock ME, Parker MH, Brewer PD, Chuang AH (2003) Nicotines stimulates osteoclast resorption in a porcine marrow cell model. J Periondotol 74:1440–1446
Norazlina M, Nik-Farideh YMK, Arizi A, Faisal A, Ima-Nirwana S (2004) Effects of nicotine on bone resorbing cytokines in male rats. Int Med J 3:1–8. www.e.imj.com/Vol3-No2/Vo13-No2-B10.htm
Ima-Nirwana S, Cheng CT, Norazlina M (2005) Effects of nicotine on bone mineral density and calcium homeostasis in male Sprague–Dawley rats. Curr Top Pharmacol 9:125–129
Wetscher GJ, Bagchi M, Bagchi D, Perdikis G, Hinder PR, Glaser K, Hinder RA (1995) Free radical production in nicotine treated pancreatic tissue. Free Radic Biol Med 18:877–882
Helen A, Krishnakumar K, Vijayammal PL, Augusti KT (2000) Antioxidant effect of onion oil (Allium cepa. Linn) on the damages induced by nicotine in rats as compared to alpha-tocopherol. Toxicol Lett 116:61–68
Kozlovskis-Wade PL, Smets MJ, Myerburg RJ (1998) The effect of nicotine on DNA repair in adult myocytes. J Mol Cell Cardiol 30:1483–1491
Kalpana C, Menon VP (2004) Protective effect of circumin on circulatory lipid peroxidation and antioxidant status during nicotine-induced toxicity. Toxicol Mech Methods 14:339–343
Ahmad NS, Khalid BAK, Ima-Nirwana S (2004) Effects of vitamin E on interleukin-1 in ferric nitrilotriacetate treated rats. Malays J Biochem Biol 9:43–47
Ahmad NS, Khalid BAK, Luke DA, Ima-Nirwana S (2005) Tocotrienol offers better protection than tocopherol from free radical–induced damage of rat bone. Clin Exp Pharmacol Physiol 32:761–770
Ima-Nirwana S, Kiftiah A, Sariza T, Gapor MT, Khalid BAK (1999) Palm vitamin E improves bone metabolism and survival rate in thyrotoxic rats. Gen Pharmacol 32:621–626
Ima-Nirwana S, Norazlina M, Khalid BAK (2000) Palm vitamin E prevents osteoporosis in orchidectomized growing male rats. Natural Product Sci 694:155–160
Norazlina M, Ima-Nirwana S, Gapor MT, Khalid BAK (2000) Palm vitamin E is comparable to alpha-tocopherol in maintaining bone mineral density in ovariectomised female rats. Exp Clin Endocrinol Diab 108:305–310
Ima-Nirwana S, Fakhrurazi H (2002) Palm vitamin E protects bone against dexmethasone-induced osteoporosis in male rats. Med J Malaysia 57:136–144
Norazlina M, Ima-Nirwana S, Gapor MT, Khalid BAK (2002) Tocotrienols are needed for normal bone calcification in growing female rats. Asia Pacific J Clin Nutr 11:194–199
Norazlina M, Ng FW, Ima-Nirwana S (2005) Gamma-tocotrienol is required for normal vitamin D metabolism in female rats. Indian J Pharmacol 37:309–314
Norazlina M, Chua CW, Ima-Nirwana S (2004) Vitamin E deficiency reduced lumbar bone calcium content in female rats. Med J Malaysia 59:297–304
Fort FL (1991) Drug safety evaluation. In: Swarbrick J, Boylan JC (eds) Encyclopedia of pharmaceutical technology, vol 4. Marcel Dekker, New York, pp 416–421
Meydani SN, Meydani M, Rall LC, Morrow F, Blumberg JB (1994) Assessment of the safety of high-dose, short-term supplementation with vitamin E in healthy older adults. Am J Clin Nutr 60:704–709
Difford J (1974) A simplified method for the preparation of methyl methacrylate embedding medium. Med Lab Tech 31:79–81
Von Kossa J (1974) Nachweis von Kalk. Beitrage zur pathologischen Anatomie und zur allgemeinen. Pathologie 29:163
Weibel ER, Kistler GS, Scherle WF (1966) Practical stereological methods for morphometric cytology. J Cell Biol 30:23–38
Freere RH, Weibel ER (1967) Stereologic techniques in microscopy. J R Microsc Soc 87:25–34
Baldock PA, Morris HA, Need AG, Moore RJ, Durbridge TC (1998) Variation in the short-term changes in bone cell activity in three regions of the distal femur immediately following ovariectomy. J Bone Miner Res 13:1451–1457
Parfitt AM, Drezner MK, Glorieux FH, Kanis JA, Malluche H, Meunier PJ, Ott SM, Recker RR (1987) Bone histomorphometry: standardization of nomenclature, symbols and units. Report of the ASMBR Histomorphometry Nomenclature Committee. J Bone Miner Res 2:595–610
Frost HM, Jee WS (1992) On the rat model human osteopenias and osteoporosis. Bone Miner 18:227–236
Boran R, Tross R, Vignery A (1984) Evidence of sequential remodeling in rat trabecular bone: morphology, dynamic histomorphometry, and changes during skeletal maturation. Anat Rec 208:137–145
Erben R (1996) Trabecular and endocortical bone surfaces in the rat: modeling or remodeling? Ant Rec 246:39–46
Wronski TJ, Dann LM, Scott KS, Cintron M (1989) Long-term effects of ovariectomy and aging on the rat skeleton. Calcif Tissue Int 45:360–366
Wing KJ, Fisher GC, O’Connell JX, Wing PC (2000) Stopping nicotine exposure before surgery: the effect on spinal fusion in rabbit model. Spine 25:30–34
Hoidrup S, Prescott E, Sorensen TI, Gottschau A, Lauritzen JB (2000) Tobacco smoking and risk of hip fracture in men and women. Int Epidemiol Assoc 29:253–259
Szulc P, Garnero B, Claustraf F, Marchand F, Duboeuf F, Delmas PD (2002) Increased bone resorption in moderate smokers with low body weight: the minos story. J Clin Endocrinol Metab 87:666–674
Krall EA, Dietrich T, Nunn ME, Garcia RI (2006) Risk of tooth loss after cigarette smoking cessation. Prev Chronic Dis 3:1–8
Hapidin H, Othman F, Shuid AN, Soelaiman IN, Mohamed N (2007) Negative effects of nicotine on bone-resorbing cytokines and bone histomorphometric parameters in male rats. J Bone Miner Metab 25:93–98
Broulik PD, Jarab J (1993) The effect of chronic nicotine administration on bone mineral content in mice. Horm Metab Res 25:219–221
Akmal M, Kesani A, Anand B, Singh A, Wiseman M, Goodship A (2004) Effect of nicotine on spinal disc cells: a cellular mechanism for disc degeneration. Spine 29:568–575
Broulik PD, Rosenkrancova J, Ruzicka P, Sedlacek R, Kurcova I (2007) The effect of chronic nicotine administration on bone mineral content and bone strength in normal and castrated male rats. Horm Metab Res 39:20–24
Syversen U, Nordsletten L, Falch JA, Madsen JE, Nilsen OG, Waldum HL (1999) Effects of lifelong nicotine inhalation on bone mass and mechanical properties in female rats femurs. Calcif Tissue Int 65:246–249
Fung YK, Iwaniec UT, Cullen DM, Akhter MP, Haven MC, Timmins P (1999) Long-term effects of nicotine on bone and calciotropic hormones in adult female rats. Pharmacol Toxicol 85:181–187
Iwaniec UT, Fung YK, Akhter MP, Haven MC, Nespor S, Haynatzki GR, Cullen DM (2001) Effects of nicotine on bone mass, turnover and strength in adult female rat. Calcif Tissue Int 68:358–364
Riesenfeld A (1985) Growth-depressing effects of alcohol and nicotine in two strains of rats. Acta Anat 122:18–24
Cesar-Neto JB, Benatti BB, Manzi FR, Sallum EA, Sallum AW, Nociti FH Jr (2005) The influence of cigarette smoke inhalation on bone density. A radiographic study in rats. Braz Oral Res 19:47–51
Cesar-Neto JB, Benatti BB, Sallum EA, Casati ZM, Nociti FH Jr (2006) The influence of cigarette smoke inhalation and its cessation on the tooth-supporting alveolar bone: a histometric study in rats. J Periodontal Res 41:118–123
Oncken C, Prestwood K, Kleppinger A, Wang Y, Cooney J, Raizs L (2006) Impact of smoking cessation on bone mineral density in postmenopausal women. J Womens Health 15:1141–1150
Pasco JA, Hendry MJ, Wilkinson LK, Nicholson GC, Schneider HG, Kotowicz MA (2006) Antioxidant vitamin supplements and markers of bone turnover in a community sample of nonsmoking women. J Womens Health 15:295–300
Nafeeza MI, Asma H, Ahmad Asmadi Y, Zaitun Z, Alini M (2002) Role of vitamin E on oxidative stress in smokers. Malays J Med Sci 9:34–42
Xu H, Watkins BA, Seifert MF (1995) Vitamin E stimulates trabecular bone formation and alters epiphyseal cartilage morphology. Calcif Tissue Int 57:293–300
Arjmandi BH, Akhter MP, Chakkalakal D, Khalil DA, Lucas EA, Juma S, El-Osta M, Devareddy L, Stoecker BJ (2001) Effects of isoflavones, vitamin E, and their combination on bone in an aged rat model of osteopenia. J Bone Miner Res 16:S533
Arjmandi BH, Juma S, Beharka A, Bapna S, Akhter M, Meydani SN (2002) Vitamin E improves bone quality in the aged but not in young adult male mice. J Nutr Biochem 13:543–549
Nishida A, Yamaguchi A, Tanizawa T, Endo N, Mashiba T, Uchiyama Y, Suda T, Yoshiki S, Takahashi HE (1994) Increased bone formation by intermittent parathyroid hormone administration is due to the stimulation of proliferation and differentiation of osteoprogenitor cells in bone marrow. Bone 6:717–723
Schmidt IU, Dobnig H, Turner RT (1995) Intermittent parathyroid hormone treatment increases osteoblast number, steady state messenger ribonucleic acid levels for osteocalcin, and bone formation in tibial metaphysis of hypophysectomized female rats. Endocrinology 136:5127–5134
Jiang Y, Zhao JJ, Mitlak BH, Wang O, Genant HK, Eriksen EF (2003) Recombinant human parathyroid hormone (1–34) [teriparatide] improves both cortical and cancellous bone structure. J Bone Miner Res 18:1932–1941
Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, Hodsman AB, Eriksen EF, Ish-Shalom S, Genant HK, Wang O, Mitlak BH (2001) Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 10:1434–1441
Greenspan SL, Bone HG, Ettinger DA, Lindsay R, Zanchetta JR, Blosch CM, Mathisen AL, Morris SA, Marriott TB (2007) Effects of recombinant human parathyroid hormone (1–84) on vertebral fracture and bone density in postmenopausal women with osteoporosis. Ann Intern Med 146:326–339
Soelaiman IN, Ahmad NS, Khalid BAK (2004) Palm oil tocotrienol mixture is better than alpha-tocopherol acetate in protecting bones against free-radical induced elevation of bone-resorbing cytokines. Asia Pacific J Clin Nutr 13 Suppl:S111
Norazlina M, Lee PL, Lukman HI, Nazrun AS, Ima-Nirwana S (2007) Effects of vitamin E supplementation on bone metabolism in nicotine-treated rats. Singapore Med J 48:195–199
Acknowledgements
We thank Carotech (Ipoh, Malaysia) for supplying the gamma-tocotrienol and the Malaysian Palm Oil Board for providing the tocotrienol-enhanced fraction. We are also grateful to Mr. Rafizul Mohd Yusoff, Mr. Arizi Aziz, Ms. Hairi Ghazalli, Ms. Azizah Osman, and Mr. Faisal Ariffin for their technical assistance. We also thank the Ministry of Science, Technology, and Innovation for funding this project via research grant IRPA/UKM 06-02-02-051-EA243.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hermizi, H., Faizah, O., Ima-Nirwana, S. et al. Beneficial Effects of Tocotrienol and Tocopherol on Bone Histomorphometric Parameters in Sprague–Dawley Male Rats After Nicotine Cessation. Calcif Tissue Int 84, 65–74 (2009). https://doi.org/10.1007/s00223-008-9190-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-008-9190-x