
Abstract
The recommended dietary phosphorus intake is exceeded in the typical Western diet. However, few studies have been conducted on the bioavailability and metabolic consequences of dietary phosphorus from different food sources. In this study, acute effects of dietary phosphorus from three different food sources and a phosphate supplement on calcium and bone metabolism were investigated. Sixteen healthy women aged 20–30 years were randomized to five controlled 24-hour study sessions, each subject serving as her own control. At the control session, calcium intake was ca. 250 mg and phosphorus intake ca. 500 mg. During the other four sessions, phosphorus intake was about 1,500 mg, 1,000 mg of which was obtained from meat, cheese, whole grains, or a phosphate supplement, respectively. The foods served were exactly the same during the phosphorus sessions and the control session; only phosphorus sources varied. Markers of calcium and bone metabolism were followed. Analysis of variance with repeated measures was used to compare the study sessions. Only the phosphate supplement increased serum parathyroid hormone (S-PTH) concentration compared with the control session (P = 0.031). Relative to the control session, meat increased markers of both bone formation (P = 0.045) and bone resorption (P = 0.049). Cheese decreased S-PTH (P = 0.0001) and bone resorption (P = 0.008). These data suggest that the metabolic response was different for different foods.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In chronic renal disease, a low-phosphorus diet is essential for preventing and correcting secondary hyperparathyroidism and cardiovascular morbidity [1]. Moreover, we have earlier shown that in young healthy women the combination of 1,500 mg of phosphorus as a phosphate supplement coupled with 375 mg calcium intake increases serum parathyroid hormone (S-PTH) concentration and inhibits bone formation acutely [2]. In our recent controlled study in healthy females, we demonstrated that S-PTH increased in a dose-dependent manner with phosphorus intake [3]. Calvo et al. [4] observed a persistent rise in PTH secretion in young women after 4 weeks’ ingestion of a high-phosphorus (1,700 mg), low-calcium (400 mg) test diet. A high intake of phosphorus can also decrease the serum calcitriol concentration, as observed in healthy males [5]. In a cross-sectional study of young females, a negative association between phosphorus intake and radial bone measurements was found [6]. Hence, high phosphorus intake can negatively affect mineral metabolism in healthy subjects as well. Results of several animal studies also support this conclusion [e.g., 7–9].
The dietary reference intake of phosphorus for adults is 700 mg/day [10]. In Western countries, intakes exceed recommended levels substantially [11–14]. The best sources of phosphorus are whole-grain, meat, and milk products. The use of phosphate additives in commercially prepared foods also increases phosphorus intake. Calvo and Park [15] estimated that the intake of phosphorus from phosphate additives in the United States was 470 mg/day in 1990. Estimation of phosphorus intakes is difficult because the amounts of phosphate additives used in industrially prepared foods are not well known [15].
Of dietary phosphorus intake, 60–80% is considered to be absorbed from the intestine when phosphorus intake is at usual levels (775–1,860 mg P/day) [16]. Intestinal phosphate absorption occurs by both passive and active transport, the latter being stimulated by 1,25-dihydroxyvitamin D. The majority of dietary phosphate is absorbed by passive mechanisms. Phosphorus absorption remains relatively effective even with extremely low plasma 1,25-dihydroxyvitamin D concentrations [17].
Few studies have been conducted on the absorbability and metabolic consequences of dietary phosphorus from different food sources. Phosphorus in muscle protein foods, such as meat, poultry, and fish, occurs as phosphate bound to amino acid side chains and is released during digestion [18]. Meat phosphorus also consists of phospholipids and nucleotides. In contrast, much of the phosphorus in plant foods is found as phytate, which is poorly digested, and therefore, less phosphorus is absorbed. Calcium compounds are used to bind dietary phosphorus in renal disease [19], but the absorbability of phosphorus from calcium-containing dairy products is not well known. In previous interventions, phosphorus has been administered as supplements [2, 3, 5, 20–22] or foods containing phosphate additives [4, 23, 24]. The aim of this study was to evaluate the acute effects of dietary phosphorus from three different foodstuffs (meat, cheese, whole grains) and a phosphate supplement on calcium and bone metabolism.
Subjects and Methods
Subjects and Protocol
Sixteen healthy female volunteers aged 20–30 years participated in five separate 24-hour sessions. The subjects attended the sessions at 7-day intervals. The subjects had no medications or illnesses known to affect calcium or bone metabolism. Ten of the subjects used oral contraceptives. The basic characteristics of the participants are shown in Table 1. Before coming to the research unit, subjects fasted overnight. At the control session, both calcium and phosphorus intakes were low (approximately 250 and 500 mg/day, respectively). During the other four sessions, phosphorus intake was approximately 1,500 mg/day, 1,000 mg of which was obtained from meat, cheese, whole grains, or a phosphate supplement, respectively. The order of the study sessions was randomized. The phosphorus intake in this study represents the average intake in Finland, which is 1,312 mg/day for women and 1,728 mg/day for men [11]. The foods served during phosphorus sessions and the control session were identical, with the exception of differing phosphorus sources. At all sessions, the subjects had breakfast at 0800, lunch at 1200, a snack at 1400, dinner at 1700, and another snack at 2000 hours. Phosphorus intake was divided evenly between these meals at all phosphorus sessions. We used the food-composition database (Fineli) of the Finnish National Public Health Institute [25] and manufacturers’ information in designing the study diets. The phosphorus concentrations of the whole grains, meats, and cheese were analyzed at the laboratory of the Finnish Meat Research Institute. The intakes of selected nutrients during the study sessions are presented in Table 2.
We followed a whole-foods approach in designing the study diets. When feeding meat, whole grains, and cheese in separate sessions, the intakes of protein, fiber, and calcium varies among these sessions. We considered the possibility of equalizing the intakes of these nutrients by using supplements. However, if supplemented, the test diets would not be realistic in representing the nutrient content of the phosphorus sources. Furthermore, the absorbability of a nutrient could be different from food and from a dietary supplement. For this reason, i.e., a fiber supplement should have contained identical fibers as the whole-grain foods in the test diet. Such a supplement would also have increased phosphorus intake as a large part of whole-grain phosphorus can be found in the fiber part of a grain. The variations in nutrient intakes are reported in the conclusions of this study.
At the meat session, the main phosphorus sources were ham and beef steak, both prepared without phosphate additives. At the cheese session, the subjects were served fermented cheese (Edam type, 17% fat) because the amount of milk providing 1,000 mg of phosphorus is rather high (1.1 liters [25]) and, hence, could have been difficult to ingest for the subjects. Also, we preferred to use lactose-free dairy product, which would be suitable for lactose-intolerant subjects. At the whole-grain session, the main phosphorus sources were oatmeal porridge and nonfermented rye bread. The phosphate supplement was prepared from a mixture of disodium and trisodium phosphates (E450 and E451; Six Oy, Helsinki, Finland) commonly used in the food industry and served in a refreshment drink.
To increase protein intake at the control, whole-grain, and supplement sessions, cooked egg white was served to the subjects during these three sessions because egg white has a high but a low phosphorus content [25]. Energy intakes were balanced by using different amounts of oil, margarine, sugared and diluted berry juice, berry soups, and canned fruit. These foods are low in phosphorus, protein, and fiber. Lunch consisted of mashed potatoes and beef (meat session) or mashed potatoes and veggie burger (all other sessions) in addition to foods specific to each session mentioned earlier. For dinner, subjects received industrially prepared vegetable pasta with beef (meat session), cheese (cheese session), or egg white (all other sessions). Breakfast and snacks contained wheat toast, rice pasty, corn flakes, or rye bread and oatmeal porridge (only whole-grain session) together with the low-phosphorus foods mentioned above to balance nutrient intakes and foods specific to each session (meat/whole grains/cheese/phosphorus drink).
The diets during each session contained the same amounts of sodium (3.8 g/day). The amount of daily protein consumed was similar (82–95 g/day) during all sessions other than the meat session, when protein intake was higher (125 g/day) because of the high protein content of meat. Likewise, fiber intake was higher (59 g/day) during the whole-grain session than during the other sessions (19–21 g/day). Because the highest phosphorus concentrations in wheat products is found in whole grains, which also contain large amounts of fiber, a high fiber intake during the whole-grain session could not be avoided. Similarly, the calcium intake during the cheese session was high (2,044 mg/day) due to the high calcium content of cheese, and low during all other sessions (235–352 mg/day). Because milk products have a high content of both calcium and phosphorus, the intakes of these minerals during the cheese session reflect the diet of an individual consuming large amounts of milk products. The intake of calcium during other study sessions was kept low because oral calcium intake affects PTH secretion.
No extra meals or snacks were allowed during the study sessions, but tap water was provided ad libitum. For estimation of habitual calcium, phosphorus, and energy intakes, the volunteers kept a 4-day food record before the beginning of the experiment. The study protocol was approved by the Ethics Committee of Public Health and Epidemiology in the Hospital district of Helsinki and Uusimaa.
Sampling
The anaerobically handled blood samples were taken before meals at 0800 and 1400 hours and for practical reasons immediately after the meal at 1800 hours. The last sample was taken before the meal at 0800 hours on the following morning. Serum was separated from blood and stored at −20°C until analyzed. The 24-hour urine collections were obtained on the study day from 0800 to 0800 hours the following morning. Urine samples were kept at −20°C until analyzed.
Laboratory Methods
The ionized calcium (iCa) concentration was analyzed from anaerobically handled serum samples with an ion-selective analyzer (Microlyte 6; Thermo Electron, Espoo, Finland) within 90 minutes of sample collection. The intra-assay coefficient of variation (CV%) for iCa was 1.7. In the other measurements, all samples from the same person were analyzed in the same assay in a randomized order. Serum phosphate and creatinine concentrations and excretions of urinary calcium, phosphate, and creatinine were measured spectrometrically with an autoanalyzer (Konelab 20, Thermo Electron). The intra- and interassay CV% of these analyses were 1.5 and 2.6, respectively. Intact S-PTH concentration was measured by an immunoenzymometric assay using Octeia® Intact PTH Kits (Immunodiagnostic Systems, Boldon, UK). The intra- and interassay CV% were 1.0 and 4.2, respectively. Serum bone-specific alkaline phosphatase (BALP) concentration was determined by an enzyme immunoassay (Metra™ BAP EIA Kit; Quidel, San Diego, CA). Intra- and interassay CV% were 5.4 and 7.4, respectively. Excretion of urinary N-terminal telopeptide of type I collagen (NTx) was analyzed by an enzyme-linked immunosorbent assay using Osteomark® NTx Test Kits (Ostex International, Seattle, WA). The intra- and interassay CV% were 4.6 and 6.4, respectively.
Statistical Analysis
The data are expressed as means ± standard error of the mean (SEM). For serum variables, the area under the curve (AUC) for the difference from the morning fasting value was calculated. Non-normal distributions were normalized by logarithmic transformations. In addition to AUC values, the morning fasting values of serum phosphate, iCa, PTH, and BALP from the second-day (24 hours from the first blood sample) fasting samples were compared. To exclude the effect of the first fasting sample, the deltas of the 0-hour sample to the 24-hour sample were used in the analyses. Analysis of variance (ANOVA) with repeated measures was used to compare the study sessions. If the sphericity assumption was violated, a Huynh-Feldt adjustment was applied. Contrast analysis was used for pairwise comparisons between study sessions. Analyses were conducted with the SPSS 10.0 statistical package (SPSS Inc., Chicago, IL) in a Windows environment. We regarded P < 0.10 as a trend and P < 0.05 as a statistically significant difference. The results of serum variables are shown as two panels in the figures only for readability.
Results
One of the subjects did not participate in the whole-grain session because of a common cold. During all the other sessions, all 16 subjects participated. In the PTH results, the AUC value of one subject in the cheese session was approximately threefold lower than the value of other subjects at the same session. Therefore, we excluded this value from the analyses.
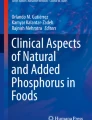
The serum phosphate concentrations (AUC) differed between the study sessions (P = 0.0001, ANOVA) (Fig. 1). The serum phosphate concentration was elevated during the meat (P = 0.0001), cheese (P = 0.0001), whole-grain (P = 0.006), and supplement (P = 0.0001) sessions compared with the control session. Cheese increased the serum phosphate concentration more than the other phosphate sources (P = 0.0001). Differences were present between study sessions in the serum phosphate concentrations at the second-day fasting samples (P = 0.0001, ANOVA). The serum phosphate concentration remained higher in the cheese session on the following morning than in all other sessions (P = 0.032–0.0001).

Changes in serum phosphate (S-P) concentration (A) and 24-hour urinary excretion of phosphate (U-P) (B) during the five study sessions. (A) Control (□), meat (•), supplement (▼), cheese (*), and grain (♦) session. Arrows indicate mealtimes. The different phosphorus sources affected the AUC values of S-P (ANOVA, P = 0.0001) and 24-hour U-P (ANOVA, P = 0.0001); asignificantly different from control session, bsignificantly different from grain and cheese sessions, csignificantly different from all other sessions.
Differences were found in urinary phosphate excretion between study sessions (P = 0.0001, ANOVA) (Fig. 1). Phosphate excretion was higher in all phosphate sessions than in the control session (P = 0.001–0.0001). Meat increased urinary phosphate excretion more than grain (P = 0.003) or cheese (P = 0.005). The phosphate supplement also increased urinary phosphate secretion more than grain (P = 0.001) or cheese (P = 0.027).
The different foods affected the serum iCa (AUC) (P = 0.0001, ANOVA) and urinary calcium excretions (P = 0.0001, ANOVA) (Fig. 2). Serum iCa concentration was greater in the cheese session due to high calcium intake than in the other sessions (P = 0.0001). During the phosphate supplement session, serum iCa concentration was lower than in the control session (P = 0.027). Whole grains (P = 0.682) and meat (P = 0.282) had no effect on serum iCa concentration relative to the control session. On the following morning, serum iCa concentration differed between study sessions (P = 0.039, ANOVA). The 24-hour morning fasting value was higher in the cheese session than in the supplement (P = 0.018), whole-grain (P = 0.023), or control (P = 0.025) sessions and tended to be higher in the cheese session than in the meat session (P = 0.050) but did not reach statistical significance. The urinary excretion of calcium was higher during the cheese session than during all other sessions (P = 0.0001) (Fig. 2). In the meat session, the calcium excretion was greater than in the phosphate supplement session (P = 0.003).

Changes in serum ionized calcium (S-iCa) concentration (A) and 24-hour urinary excretion of calcium (U-Ca) (B) during the five study sessions. (A) Control (□), meat (•), supplement (▼), cheese (*), and grain (♦) session. Arrows indicate mealtimes. The different phosphorus sources affected the AUC values of S-iCa (ANOVA, P = 0.0001) and 24-hour U-Ca (ANOVA, P = 0.0001); asignificantly different from control session; csignificantly different from all other sessions; dsignificantly different from phosphate supplement session.
The concentrations of PTH differed between the study sessions (AUC) (P = 0.0001, ANOVA) (Fig. 3). Compared with the other sessions, cheese decreased serum PTH most (P = 0.0001). Phosphate supplement, by contrast, increased serum PTH concentration compared with the control session (P = 0.039). Meat (P = 0.346) or grain (P = 0.498) had no effect on serum PTH. Differences were observed between study sessions in serum PTH concentrations of the second-day fasting samples (P = 0.018, ANOVA). The serum PTH concentration was lower in the cheese session on the following morning than in all other sessions (P = 0.048–0.004).

Changes in S-PTH concentration during control (□), meat (•), supplement (▼), cheese (*), and grain (♦) session. Arrows indicate mealtimes. The different phosphorus sources affected the AUC values of S-PTH (ANOVA, P = 0.0001); asignificantly different from control session; csignificantly different from all other sessions.
Based on ANOVA, the activity of serum BALP (AUC) tended to differ among study sessions (P = 0.094) (Fig. 4) but did not reach statistical significance. In contrast analysis, the activity of serum BALP was higher in the meat session than in the control (P = 0.045) or whole-grain (P = 0.013) session. The second-day fasting values of BALP were not different among sessions (P = 0.403, ANOVA).

Changes in serum BALP (S-BALP) activity from the morning fasting value (A) and 24-hour urinary excretion of NTx (U-NTx) (B) during the five study sessions. (A) Control (□), meat (•), supplement (▼), cheese (*), and grain (♦) session. Arrows indicate mealtimes. The different phosphorus sources tended to affect the AUC values of S-BALP (ANOVA, P = 0.094) and affected U-NTx (ANOVA, P = 0.0001); asignificantly different from control session.
The serum creatinine concentrations (P = 0.0001, ANOVA) and urinary excretion of creatinine (P = 0.0001, ANOVA) (Fig. 5) differed among study sessions. Because meat has a high creatine content, the serum creatinine concentration was higher in the meat session than any of the other sessions (P = 0.0001). The serum creatinine concentration was higher in the cheese session than in the control session (P = 0.038). The urinary excretion of creatinine was greater in the meat session than in all other sessions (P = 0.021–0.0001) (Fig. 5). Also, in the cheese session, the excretion of creatinine was higher than in the control (P = 0.030) or whole-grain (P = 0.019) sessions.

Changes in serum creatinine (S-Crea) concentration (A) and 24-hour urinary excretion of creatinine (U-Crea) (B) during the five study sessions. (A) Control (□), meat (•), supplement (▼), cheese (*), and grain (♦) session. Arrows indicate the mealtimes. The different phosphorus sources affected the AUC values of S-Crea (ANOVA, P = 0.0001) and 24-hour U-Crea (ANOVA, P = 0.0001); asignificantly different from control session; csignificantly different from all other sessions.
Differences were present in urinary NTx excretions among study sessions (P = 0.0001, ANOVA) (Fig. 4). The urinary excretion of NTx was higher in the meat session (P = 0.049) than in the control session. Urinary NTx excretion tended to increase in the whole-grain (P = 0.053) and phosphate supplement (P = 0.083) sessions compared with the control session but did not reach statistical significance. The NTx excretion was lower during the cheese session than during the control session (P = 0.008). Because there were statistically significant differences in urinary creatinine excretion among study sessions, we did not correct the NTx results for creatinine excretion as this would have skewed the results. Therefore, the NTx results are shown as bone collagen equivalents (nmolBCE). Because we used carefully collected 24-hour urinary samples, creatinine corrections should not be obligatory.
Discussion
We observed differences in the metabolic response to studied foods. These differences may be due to different bioavailability of phosphorus from different foods, or other substances found in the phosphorus sources used in this study. Based on serum phosphorus and urinary phosphate excretion, phosphorus from meat and supplements appears to absorb better than phosphorus from whole grains. The whole-grain foods given to our subjects (oatmeal porridge, rye bread) were unfermented. Because fermentation can enhance the absorption of minerals in phytate-containing foods, the bioavailability of phosphorus may be greater from fermented whole grains and even greater from low-fiber grains.
Estimation of the absorbability of phosphorus from cheese is more complex than that of whole grains because the high calcium content decreases PTH secretion, which decreases urinary phosphate excretion. Hence, the low urinary phosphate excretion in the cheese session was probably due to low serum PTH concentration caused by the high calcium intake. Serum phosphate increased at the cheese session more than during any other session. Decreased phosphate excretion caused by low PTH secretion may have caused an increase in serum phosphate by increasing the renal phosphorus threshold. At the same time, a decrease in bone resorption (as indicated by lowered NTx excretion) likely caused a drop in the release of phosphorus from bone, which could decrease serum phosphate concentration. The effects of these two mechanisms on serum phosphate are, therefore, contrary. Phosphorus intake at the cheese session (1,624 mg) was slightly higher than during other phosphorus sessions, which also may have increased serum phosphate concentration. In addition, the high calcium intake (290–602 mg/meal) may have partly inhibited the absorption of phosphorus in the intestine. Based on this study, we do not know whether this inhibition occurred. Probably many of these factors simultaneously affected serum phosphate at the cheese session, the outcome being increased serum phosphate.
Compared with the control session, S-PTH concentration was higher only in the phosphate supplement session. Therefore, the effect on mineral metabolism of phosphate additives apparently differs from that of foods containing phosphates naturally. In most phosphorus interventions, phosphorus has been administered as a supplement [2, 3, 5, 20, 21, 22]. In all of these studies, a rise in PTH secretion as a result of phosphorus administration was observed. At least two interventions have been conducted using diets assembled from common foods [4, 23]. Also, in these studies a rise in S-PTH concentration with the low-calcium, high-phosphate diet was found. However, the intake of phosphate additives was probably rather high because the high-phosphorus test diet included processed foods, such as processed cheese, instant pudding, and cola beverage, all of which contain phosphate additives. For this reason, the effects of the high-phosphorus diets can be due to phosphate additives in these studies, too. Moreover, Bell et al. [24] observed enhanced parathyroid activity as a response to foods containing phosphate additives compared to the same foods prepared without phosphates.
A low serum 25-hydroxyvitamin D (25[OH]D) status could have affected PTH results of the subjects [26]. We did not measure 25(OH)D of our subjects as each served as her own control and the order of the study sessions was randomized. We did not observe abnormally high fasting S-PTH concentrations, which should indicate severe vitamin D deficiency. In addition to this, as the study was conducted in October, the serum 25(OH)D concentrations had not declined very low after summer. As dietary intake data were based on 3-day food records, it was inappropriate to calculate dietary vitamin D intake data.
In our study, urinary NTx excretion tended to increase in the phosphate supplement session compared with the control session, implying greater bone resorption as a result of increased PTH secretion. Calvo et al. [23] observed increased excretion of hydroxyproline, another marker of bone resorption, with a low-calcium, high-phosphorus test diet compared with the control diet (820 mg Ca, 930 mg P) in their 8-day study; but in their 4-week study, no difference in the excretion of hydroxyproline between the low-calcium, high-phosphorus test diet and control diet (800 mg Ca, 900 mg P) was found [4]. In two other studies, high-phosphate diets had no effect on the concentrations of resorption markers [2, 21]. In our recent dose-response study, urinary excretion of NTx increased acutely as a response to 1,500 mg of phosphorus administered as supplements [3]. Therefore, the results of NTx in the supplement session in the present study are in accordance with our previous study. Urinary NTx may respond to oral phosphorus load more rapidly than other resorption markers used in previous studies. The differences in protocols of the phosphorus supplementation studies and sensitivities of different resorption markers probably explain the differences in results.
We earlier noted acutely a decrease in serum BALP activity after administration of 1,500 mg [2, 3] and 750 mg [3] of phosphorus as a supplement. In our present study, by contrast, the phosphate supplement had no effect on serum BALP. This could be due to the timing and fewer blood samples; when the 1400-hour blood sample (the first blood sample after the fasting sample) was taken, the subjects had only ingested ca. 500 mg of phosphorus from the phosphate supplement. The 1800-hour blood sample was taken immediately after the last phosphate supplement dose. As the next blood sample was taken the following morning, we do not know whether serum BALP activity had decreased in the evening after 1800 hours.
During the meat session, both bone formation and resorption increased, which may be due to the high protein intake from meat. The average protein intake in the meat session was 2.1 g/kg body weight, which comprised 25% of total energy. Because protein consumption increases urinary calcium excretion, high protein intake has been speculated to be detrimental to bone health [27]. The effect of protein intake on bone seems, however, to depend on the protein source as well as on other nutrients in the food [18]. Recently, Kerstetter et al. [28] concluded, based on their 10-day study of healthy women, that the rise in urinary calcium in response to increased dietary protein was mostly due to enhanced intestinal calcium absorption. We did not observe a significant increase in urinary calcium excretion during the meat session compared with the control session. Earlier, in a 10- to 15-day study, addition of meat to a diet low in protein, calcium, and phosphorus was observed to increase urinary calcium excretion [29].
The increase in both BALP and NTx probably indicates increased turnover of bone during the meat session. The effects of meat proteins and meat phosphates on bone should be confirmed in a longer-term study. Alternatively, some other substance in meat might have caused the increases in the markers of bone metabolism during the meat session. Our result is contrary to that of Kerstetter et al. [28], who observed a nonsignificant trend toward a reduction in the rate of bone turnover with a high-protein diet. For methodological reasons, our study is not comparable to that of Kerstetter et al. [28]. The reason for increased NTx excretion during the whole-grain session remains obscure. It is possible that the high intake of phytates from unfermented whole grain inhibited calcium absorption [30], which could have caused an increase in NTx excretion.
In conclusion, we observed acute differences in metabolic responses from different foods and a phosphorus supplement. The effects of high phosphorus intake appear to depend on the phosphorus sources consumed. Phosphate compounds commonly used by the food industry seem to absorb well and increase S-PTH, as shown in previous studies. By contrast, phosphorus from meat or whole grains appears not to affect S-PTH. Because of the high calcium content, cheese affects bone metabolism favorably. Meat increased bone turnover, possibly because of its high protein content. Limitations of this study include the short follow-up period and problems in designing diets with similar amounts of nutrients using different foods. Longer-term intervention studies are needed to confirm our results.
References
Barsotti G, Cupisti A (2005) The role of dietary phosphorus restriction in the conservative management of chronic renal disease. J Ren Nutr 15:189–192
Kärkkäinen M, Lamberg-Allardt C (1996) An acute intake of phosphate increases parathyroid hormone secretion and inhibits bone formation in young women. J Bone Miner Res 11:1905–1912
Kemi VE, Kärkkäinen MUM, Lamberg-Allardt CJE (2006) High phosphorus intakes acutely and negatively affect calcium and bone metabolism in a dose-dependent manner in healthy young females. Br J Nutr 96:545–552
Calvo MS, Kumar R, Heath H III (1990) Persistently elevated parathyroid hormone secretion and action in young women after four weeks of ingesting high phosphorus, low calcium diets. J Clin Endocrinol Metab 70:1334–1340
Portale AA, Halloran BP, Murphy MM, Morris RC Jr (1986) Oral intake of phosphorus can determine the serum concentration of 1,25-dihydroxyvitamin D by determining its production rate in humans. J Clin Invest 77:7–12
Metz JA, Anderson JJ, Gallagher PN Jr (1993) Intakes of calcium, phosphorus, and protein, and physical-activity level are related to radial bone mass in young women. Am J Clin Nutr 58:537–542
Huttunen MM, Pietilä PE, Viljakainen HT, Lamberg-Allardt CJ (2006) Prolonged increase in dietary phosphate intake increases alters bone mineralization in adult male rats. J Nutr Biochem 17:479–484
Katsumata S, Masuyama R, Uehara M, Suzuki K (2005) High-phosphorus diet stimulates receptor activator of nuclear factor-kappaB ligand mRNA expression by increasing parathyroid hormone secretion in rats. Br J Nutr 94:666–674
Koshihara M, Masuyama R, Uehara M, Suzuki K (2005) Reduction in dietary calcium/phosphorus ratio reduces bone mass and strength in ovariectomized rats enhancing bone turnover. Biosci Biotechnol Biochem 69:1970–1973
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine (1997) Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, and fluoride. National Academy Press, Washington DC
Männistö S, Ovaskainen M-L, Valsta L (eds) (2003) The National FINDIET 2002 Study. Kansanterveyslaitoksen julkaisuja B3/2003. National Public Health Institute, Helsinki
Henderson L, Irving K, Gregory J, Bates CJ, Prentice A, Perks J, Swan G, Farron M (2003) The National Diet & Nutrition Survey: Adults Aged 19 to 64 years. Vitamin and Mineral Intakes and Urinary Analytes. HMSO, London
Gronowska-Senger A, Kotanska P (2004) Phosphorus intake in Poland in 1994–2001 [abstract]. Rocz Panstw Zakl Hig 55:39–49
Calvo MS (2000) Dietary considerations to prevent loss of bone and renal function. Nutrition 16:564–566
Calvo MS, Park YK (1996) Changing phosphorus content of the US diet: potential for adverse effects on bone. J Nutr 126:1168S–1180S
Favus MJ, Bushinsky DA, Lemann J Jr (2006) Regulation of calcium, magnesium, and phosphate metabolism. In: Favus MJ (ed), Primer of the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 6th ed. American Society for Bone and Mineral Research, Washington DC, pp 76–83
Wilz DR, Gray RW, Dominguez JH, Lemann J Jr (1979) Plasma 1,25-(OH)2−vitamin D concentrations and net intestinal calcium, phosphate, and magnesium absorption in humans. Am J Clin Nutr 32:2052–2060
Massey LK (2003) Dietary animal and plant protein and human bone health: a whole foods approach. J Nutr 133:862S–865S
Nolan CR, Cunibi WY (2003) Calcium salts in the treatment of hyperphosphatemia in hemodialysis patients. Curr Opin Nephrol Hypertens 12:373–379
Silverberg SJ, Shane E, de la Cruz L, Segre GV, Clemens TL, Bilezikian JP (1989) Abnormalities in parathyroid hormone secretion and 1,25-dihydroxyvitamin D3 formation in women with osteoporosis. N Engl J Med 320:277–281
Brixen K, Nielsen HK, Charles P, Mosakilde L (1992) Effects of a short course of oral phosphate treatment on serum parathyroid hormone (1–84) and biochemical markers of bone turnover: a dose-response study. Calcif Tissue Int 51:276–281
Calvo MS, Heath H (1988) Acute effects of oral phosphate-salt ingestion on serum phosphorus, serum ionized calcium, and parathyroid hormone in young adults. Am J Clin Nutr 47:1025–1029
Calvo MS, Kumar R, Heath H III (1988) Elevated secretion and action of serum parathyroid hormone in young adults consuming high phosphorus, low calcium diets assembled from common foods. J Clin Endocrinol Metab 66:823–829
Bell RR, Draper HH, Tzeng DYM, Shin HK, Schmidt GR (1977) Physiological responses of human adults to foods containing phosphate additives. J Nutr 107:42–50
National Public Health Institute, Nutrition Unit (2006) Fineli. Finnish food composition database, release 5. National Public Health Institute, Helsinki, http://www.fineli.fi/ (accessed March 10, 2006)
Lamberg-Allardt CJ, Outila TA, Kärkkäinen MU, Rita HJ, Valsta LM (2001) Vitamin D deficiency and bone health in healthy adults in Finland: could this be a concern in other parts of Europe? J Bone Miner Res 16:2066–2073
Kerstetter JE, O’Brien KO, Insogna KL (2003) Dietary protein, calcium metabolism, and skeletal homeostasis revisited. Am J Clin Nutr 78:584S–592S
Kerstetter JE, O’Brien KO, Caseria DM, Wall DE, Insogna KL (2005) The impact of dietary protein on calcium absorption and kinetic measures of bone turnover in women. J Clin Endocrinol Metab 90:26–31
Schuette SA, Linkswiler HM (1982) Effects on Ca and P metabolism in humans by adding meat, meat plus milk, or purified proteins plus Ca and P to a low protein diet. J Nutr 112:338–349
Gueguen L, Pointillart A (2000) The bioavailability of dietary calcium. J Am Coll Nutr 19:119S–136S
Acknowledgment
This work was funded by the National Technology Agency of Finland (TEKES).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karp, H.J., Vaihia, K.P., Kärkkäinen, M.U.M. et al. Acute Effects of Different Phosphorus Sources on Calcium and Bone Metabolism in Young Women: A Whole-Foods Approach. Calcif Tissue Int 80, 251–258 (2007). https://doi.org/10.1007/s00223-007-9011-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-007-9011-7