
Abstract
The fear of falling can be manipulated by introducing a postural threat (e.g., an elevated support surface) during stance and gait. Under these conditions, balance parameters are altered in both young and elderly individuals. This study aimed to dissociate the physical and psychological aspects of the threat and show the impact of a verbal warning cue of imminent perturbation during gait among young and elderly healthy participants. Ten young subjects (29.4 ± 3.9 years) and ten subjects aged over 65 years (72.9 ± 3.5) participated in the study. Spatiotemporal and balance parameters were quantified during eight consecutive gait cycles using a motion analysis system and an instrumented treadmill. These parameters were compared twice in the control trial and before/after a verbal warning cue of imminent perturbation during gait (“postural threat”) in perturbation trials and between groups using repeated measure ANOVAs. Results: The verbal cue yielded reduced step length (p = 0.008), increased step width (p = 0.049), advanced relative position of the center of mass (p = 0.016), increased stabilizing force (p = 0.003), and decreased destabilizing force (p = 0.002). This warning effect was not observed in the older participant group analyses but was found for three participants based on individual data analyses. The warning effect in younger participants was not specific to impending perturbation conditions. Most gait and balance parameters were altered in the older group (p < 0.05) versus the younger group in each condition, regardless of the warning cue. A psychological threat affects gait and balance similarly to a physical threat among young participants but not among most older participants.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Between 20 and 30% of adults aged over 65 fall each year (Hamel 2001) and it is recognized that half of the people who have fallen will relapse in the future (Tinetti and Speechley 1989; Tinetti et al. 1995). Falls most commonly occur during locomotor activities, such as walking, in 90% of cases (Hyndman et al. 2002; Belgen et al. 2006) and are caused by slips, trips, or stumbles in 33% of cases [International Statistical Classification of Diseases and Related Health Problems (ICD-10)]. Fall risk increases with age due to motor, sensory, and cognitive changes associated with physiological aging (Rubenstein 2006).
With these changes, seniors may develop a fear of falling or reduced confidence in their balance. In a large cross-sectional study, 54.3% of community-dwelling seniors reported being afraid of falling (Zijlstra et al. 2007) and several of these seniors had not experienced a fall in the previous 6 months. Fear of falling can lead to activity restriction, which may cause a reduction in physical abilities through underutilization (Filiatrault et al. 2009). Reduced postural abilities may further increase the risk of falls during daily activities (Mendes de Leon et al. 1996; Cumming et al. 2000; Delbaere et al. 2004). Ultimately, this increased risk may lead to a fall and can further increase the fear of falling among seniors. A longitudinal study also supports that fear is a predictor of falls in the older adults (Friedman et al. 2002).
The fear of falling has been investigated and reproduced experimentally through a postural threat, defined as a physical or a psychological element that can disrupt the balance state of the subject (Brown and Frank 1997). An increase in the height of a surface is most commonly used in the literature to introduce a postural threat, as well as a decrease in the distance to the edge of the standing surface (Adkin et al. 2002; Brown et al. 2002a), the presentation of negative emotional pictures (Horslen et al. 2013; Lelard et al. 2014), or the application of destabilizing thrusts (Brown and Frank 1997; Adkin et al. 2008).
In both young and older healthy populations, the introduction of a threat induced a more backward position (Carpenter et al. 2001; Brown et al. 2007; Pasman et al. 2011), as well as reduced displacement (Brown and Frank 1997; Carpenter et al. 2001) of the center of mass and the alteration of other balance parameters (Adkin et al. 2000; Carpenter et al. 2001; Hauck et al. 2008; Davis et al. 2011; Cleworth et al. 2012) during standing. During walking, it also changed temporal and spatial parameters, such as reducing step length (McKenzie and Brown 2004; Caetano et al. 2009; Delbaere et al. 2009; Staab et al. 2013), increasing step width (Brown et al. 2006), increasing double support time (Brown et al. 2006; Caetano et al. 2009; Delbaere et al. 2009; Tersteeg et al. 2012), as well as reducing the speed of the center of mass (McKenzie and Brown 2004). These changes in standing balance and temporal and spatial parameters are similar to those found in participants with a fear of falling during gait without threat (Chamberlin et al. 2005).
There is an increase in the fear of falling and anxiety as well as a decrease in balance confidence and stability when the postural threat increases (Adkin et al. 2008). Both young and older adults alter their gait patterns under conditions of increased postural threat, but the modifications adopted by the two populations are different. The effect of anxiety on the control of locomotion has a greater impact on older participants and this additional difficulty could be more complex to manage among older people (Brown et al. 2002b). The type of postural threat and the order in which the threat is presented are factors influencing postural control (Adkin et al. 2000), and the alteration in postural control is more pronounced during the initial introduction of the postural threat (Adkin et al. 2000). When the postural threat is unpredictable, the impact on a young participant’s perception of his or her ability to maintain balance is more significant (Adkin et al. 2008). When perturbations are predictable, the effect is lower, and when perturbations are repeated, we note the presence of anticipation (Maki and Whitelaw 1993). A threatening environment, age, and the participant’s health status are, therefore, all factors that influence postural control (Shaw et al. 2012).
Given that the physical changes in gait conditions, i.e., reduced width or higher walking surface, could potentially modify gait characteristics (Brown et al. 2006) and introduce an alteration in the psychological state of the participants, the present study aimed to evaluate the effect of a psychological manipulation of balance confidence through warning of an imminent dangerous situation for balance, without concomitant physical manipulation of the environment.
The main objective of this study was to quantify the effect of a psychological manipulation on gait by comparing walking and balance parameters before and after the verbal warning cue of imminent gait perturbations in young and older healthy populations. We hypothesize that a psychological postural threat will have a similar, but lower magnitude, effect on gait and balance parameters than the effects previously shown in the literature of a postural threat induced by manipulation of the physical environment. A second objective was to evaluate the effect of age on these gait adaptations. We assume that the impact of a psychological postural threat will be more pronounced in older people. A final objective was to assess whether the impact of the verbal warning cue on walking and balance parameters differs between the first introduction of a perturbation not yet experienced by participants and the presentation of known but unpredictable perturbations. We assume that having already experienced the perturbations reduces the effect of the threat.
Methodology
Participants
Ten young participants (29.4 ± 3.9 years, seven men and three women) and ten participants aged over 65 years (72.9 ± 3.5, six men and four women) were recruited from the university population and local community centers. The dominant side of the participants was determined based on the leg used to kick a ball (Table 1). Participants had no current or past health problems that could affect their gait or balance abilities. Below normal scores obtained on the Balance Evaluation Systems Test (BESTest) (Horak et al. 2009; O’Hoski et al. 2014), Mini-Mental State Examination (MMSE) (Folstein et al. 1975) (performed only in the older participants), Activities-specific Balance Confidence (ABC) Scale (Powell and Myers 1995; Myers et al. 1998) and the Five Times Sit to Stand Test (FTSST) (Whitney et al. 2005; Bohannon 2006; Buatois et al. 2008) as well as a history of falls without an explanatory factor and a fear of falling (as evaluated using the question “Are you afraid of falling?”) were considered as exclusion criteria for the study (Table 1). Comfortable and fast walking over-ground speeds on a distance of 6 m were also evaluated (Rossier and Wade 2001) (Table 1). Free and informed consent was obtained from each participant according to local research ethics committee requirements.
Equipment
The walking trials were carried out on a Bertec FIT® dual-belt instrumented treadmill. Moments and ground reaction forces under each belt were recorded at a sampling frequency of 600 Hz. Body kinematics were recorded in three dimensions at a sampling frequency of 30 Hz, using Optotrak Certus cameras (Northern Digital Inc., Waterloo, Canada) and three to six infrared markers placed on each main body segment (head, trunk, pelvis, arms, forearms, hands, thighs, legs, and feet). A digitizing probe was used to locate additional anatomical points relative to the markers to complete the description of the body segments into a 3D-link segment biomechanical model (Winter 2009). Anthropometric data (height, mass of the participant, lengths, and circumferences of each limb segment and trunk) were used to adjust the biomechanical model with measurements of the participants (Table 1). The probe was also used to determine the contour of each shoe sole. The base of support was defined as the area bounded by the vertical projection on the ground of the outside contours of the two soles. Comfortable gait speed on the treadmill was determined before the control trial (C), by increasing the belt speed progressively by 0.10 m/s every 45–60 s. The participant was asked to indicate whether the speed was comfortable or not. Once found comfortable, the speed was increased once more to ensure a faster speed was not also comfortable. If so, belt speed was increased until it was deemed not comfortable by the participant. The last speed said to be comfortable was then tested again to confirm its status of comfortable speed on the treadmill.
Experimental protocol
The study was part of a larger research project on balance perturbations during walking. Perturbations were generated on a split-belt treadmill by a change in speed of one belt at a time, from heel strike to the consecutive toe-off of the perturbed foot. Comfortable belt speed was considered as 100%. Values less than 100 corresponded to a reduced belt speed and can be assimilated to slipping upon heel contact. Values higher than 100% corresponded to an increased belt speed, which can simulate tripping (Ilmane et al. 2015). Six types of perturbation were used, depending on the variation in belt speed: 50, 65, 80, 125, 150, and 175% of the comfortable gait speed of each participant.
A control trial (C) was performed before the perturbation sequences to obtain baseline data. In this trial, participants were told that no perturbation would be delivered. Two trial sequences were then used:
-
Familiarization trials: One trial consisted of 15 repetitions of the same type of perturbation. Perturbations were generated on the participant’s dominant side every 8–16 steps. Six familiarization trials were completed. Three trials were conducted first with faster-belt speed perturbations (P125, P150, and P175), then three trials with slower-belt perturbations (P80, P65, and P50).
-
Random perturbation trials: Each trial consisted of 20 repetitions (12 on the participant’s dominant side and 8 on the non-dominant side) and these perturbations were generated every 10–20 steps. Each type of perturbation was presented randomly to increase unpredictability. Four trials (R1–R4) were performed.
Participants were warned before each trial about the characteristics of the perturbation that would be applied (faster-belt or slower-belt perturbations; presented repeatedly (familiarization) or randomly) and their intensity (low, medium, or high). Participants were also told that the perturbations would occur only after a warning. The warning cue (representing the “psychological threat”) was the statement “Perturbations will start” (given in French as participants were francophone). At least eight gait cycles were performed before the warning, as well as between the warning cue and the first perturbation of each trial. A safety harness that did not relieve body weight was worn during all trials. Participants did not undergo familiarization trials before the first perturbation trial (P125).
Data analysis
Kinetic and kinematic data were filtered using a fourth-order Butterworth filter, with a cut-off frequency of 6 and 10 Hz, respectively, and re-sampled to 60 Hz. Reaction forces and moments and the kinematic data were translated based on treadmill speed (comfortable speed) to obtain data in the referential in the treadmill belts (van Ingen Schenau 1980).
Analysis was performed on the eight cycles performed pre- and post-warning, before any perturbation was generated in the first familiarization trial (P125) and random sequences (R1). Two sets of eight consecutive gait cycles were also analyzed from the beginning of the control trial to match the analyzed cycles in the perturbation trials despite the absence of a warning cue. This allowed the effect of the warning cue to be compared with the natural variability of gait between the two sets of eight gait cycles.
Step length, step width, and duration of double support were determined using foot kinematics and gait events detected through ground reaction forces. The anteroposterior and mediolateral distances between the markers placed on the lateral malleoli were calculated during two consecutive heel contacts based on the sharp increase in vertical ground reaction forces. The double support duration was calculated as the time between heel contact and the consecutive toe-off, as determined by the ground reaction forces returning to baseline. Ground reaction forces, center of mass position, and speed and center of pressure position relative to the base of support and mass of the participant were used to calculate the stabilizing and destabilizing forces (Duclos et al. 2009, 2012) to evaluate the difficulty of maintaining balance depending on the threat. Stabilizing and destabilizing forces have been used before and have shown sensitivity to changes in the difficulty in maintaining balance between various tasks (Desrosiers et al. 2014; Mullie and Duclos 2014; Ilmane et al. 2015).
Stabilizing force: \({{\vec{F}}_{\text{ST}}}~=~-~\frac{{{m}_{\text{global}}}.{{{\vec{v}}}^{2}}_{\text{CoM}}}{2{{D}^{2}}_{\text{CoP}}}~{{\vec{D}}_{\text{CoP}}}.\)
With \({{m}_{\text{global}}}\): body mass of the subject,
\({{\vec{v}}_{\text{CoM}}}\): velocity of the centre of mass,
\({{\vec{D}}_{\text{CoP}}}\): distance between the centre of pressure and the limit of the base of support in the direction of CoM velocity.
Destabilizing force: \({{\vec{F}}_{\text{D}}}=~\left( \frac{{{{\vec{F}}}_{r}}.\vec{n}}{{{h}_{\text{CoM}}}} \right){{\vec{D}}_{\text{CoP}}}\).
With \({{\vec{F}}_{r}}.\vec{n}\): vertical ground reaction forces,
\({{h}_{\text{CoM}}}\): height of the centre of mass,
\({{\vec{D}}_{\text{CoP}}}\): as above.
Demographic and clinical data were compared between groups using independent t tests. Balance and spatial–temporal parameters were compared between the pre- and post-warning periods (warning factor: two levels) of the control trial (C), the first trial of the familiarization (P125) and random (R1) sequences (trial factor: 3 levels) and between groups (young vs. older) using a three-factor ANOVA for repeated measures (ANOVA-RM). The statistical significance threshold was set at p = 0.05. Greenhouse-Geisser corrections were used when the sphericity assumption did not hold, as tested by the Mauchly test (p < 0.05). All statistical tests were performed using SPSS 13.0. Effect sizes (using Cohen’s d) with 95% confidence intervals (CI) were used to show the magnitude of the effects (Fritz et al. 2012). The cut-off values for interpretation of the Cohen’s d were: small ≥ 0.20, medium ≥ 0.50, large ≥ 0.80.
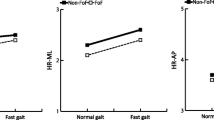
Results (Fig. 1)

Effect of the warning cue expressed using different balance variables (step length, step width, duration of double support, anteroposterior relative position of the center of mass and center of pressure, anteroposterior speed of the center of mass, and stabilizing and destabilizing forces) at two points in the control trial and before/after the warning cue of the first familiarization trial and first random trial. Black corresponds to young adults and gray to older adults. Data points and error bars represent the mean value of each variable and one standard deviation, respectively. C Control Trial, P125 First Familiarization Trial, R1 First Random Trial, Pre Pre-warning, Post Post-warning, COP center of pressure, COM center of mass, *p ≤ 0.05; **p ≤ 0.01; ***p ≤ 0.001
After the warning cue, step length was shorter (significant warning factor: F (1, 18) = 8.97, p = 0.008), step width was larger (F (1, 18) = 4.46, p = 0.049), relative position of the center of mass was further forward (F (1, 18) = 7.14, p = 0.016), the stabilizing force had increased (F (1, 18) = 11.94, p = 0.003), and the destabilizing force was smaller (F (1, 18) = 12.49, p = 0.002) compared to before the warning cue (Fig. 1). The effect of the warning cue was modulated between groups for the stabilizing force (group × warning interaction, F (1, 18) = 15.46, p = 0.001): the warning effect was only significant in younger adults (Student’s paired t test: t (9) = 5.34, p = 0.001 for younger adults, vs. t (9) = 0.32, p = 0.756 for older adults). The effect of the warning cue was also modulated between trials for step width (F (2, 36) = 8.97, p = 0.011), with a significant effect in the familiarization trial (P125: F (1, 18) = 9.12, p = 0.007) and the random trial (R1: F (1, 18) = 6.7, p = 0.019). However, no difference between the two sets of gait cycles of the control trial was found when no warning cue was given (C: t (19) = 1.46, p = 0.159).
While there was no interaction effect between trials and the warning cue, suggesting that a change in gait parameters was present between the two sets of gait cycles in the control trial evaluated, and before/after the warning cue, the effect size differed between trials (Table 2). Moreover, despite the absence of interaction between trials, warning cues and groups (F (1.6, 28.9) = 1.67, p > 0.20), the effect size differed between the trials and groups (Table 2). In younger adults, there was little or no change in gait parameters between the two sets of gait cycles in the control trial (ES < 0.06, except for step width: ES = 0.29), but the effect of the warning cue in the first familiarization trial was more significant (ES > 0.19) and in an opposite direction (except for the destabilizing force where ES = 0.04 in the control trial and ES = 0.22 in the first familiarization trial). This effect was maintained in the random trial after experiencing a series of perturbations (except for step length, ES = 0.28 in the first familiarization trial and ES = 0.00 in the random trial). In the older adults, the warning cue showed little or no effect in the three trials analyzed. In the trials with perturbations, the effect of the warning cue was not larger (ES < 0.11) and the direction was identical to the small changes observed in the control trial (except for step length).
The group factor (young vs. older) revealed a greater step length (F (1, 18) = 14.5, p = 0.001), a smaller step width (F (1, 18) = 8.68, p = 0.009), a shorter duration of double support (F (1, 18) = 5.42, p = 0.032), a higher stabilizing force (F (1, 18) = 7.58, p = 0.013), and a higher anteroposterior speed of the center of mass (F (1, 18) = 9.06, p = 0.008) in young adults compared to older adults, which was not modulated by the warning cue (F (1, 18) = 0.96, p > 0.34), except for the stabilizing force (see previous paragraph) between trials (F (2, 36) = 1.56, p > 0.21).
Changes were also observed between trials, with no effect on the warning cue (no interaction, except for step width; see above). The duration of double support decreased (F (1.6, 27.9) = 14.6, p = 0.001) between the control trial and the random trial (F (1, 18) = 18.17, p = 0.001). The relative position of the center of pressure was further back in the familiarization trial than in the control trial (trial effect: F (2, 36) = 4.78, p = 0.014, contrast: F (1, 18) = 6.95, p = 0.017). An effect of the trials was found for the destabilizing force (F (1.3, 22.9) = 4.1, p = 0.047) but without a significant effect between trials (F (1, 18) = 3.1, p > 0.09).
Discussion
The main objective of this study was to quantify the effect of psychological threat on gait by comparing walking and balance parameters before and after a verbal warning cue indicating imminent gait perturbations in young and older healthy populations. We hypothesized that psychological postural threat would have similar effect but with a lower magnitude as those observed during a postural threat induced by the manipulation of the physical environment, as previously published.
The changes found after the warning showed that it played its role as a postural threat. Young participants indeed reduced the length and increased the width of their steps, positioned their center of mass further forward in their base of support, while the stabilizing force increased and the destabilizing force decreased to confront the risk of balance destabilization (Adkin et al. 2002). Unlike most postural threats used until now, our protocol did not impose a more physically difficult situation during the warning cue but only introduces the risk of future danger: the gait conditions did not differ from control gait at the time of the warning cue in either perturbation trial. In addition, these results were obtained in individuals who declared having no fear of falling during clinical examination. Yet, following the changes in psychological conditions, as induced by the warning cue, the young participants adapted their gait, similarly to what is found using physical threats (Adkin et al. 2000; Hauck et al. 2008) or among persons who are afraid of falling (Adkin et al. 2002; Chamberlin et al. 2005). This demonstrates that as a physical threat, psychological threat has an effect on walking and balance.
The effect of the psychological postural threat was of a small magnitude, likely smaller than the effect of a physical postural threat, compared to mean values presented in the previous publications. A 5% decrease in step width caused by the possibility of a tripping reaction is described in the literature (Pijnappels et al. 2001). Our results showed a 3% decrease in step width among young participants following the introduction of the warning cue. This supports our first hypothesis but requires direct comparison in the same group of participants to be confirmed. Moreover, the effects found after the warning cue could not be attributed to familiarization of walking on the treadmill, because the adjustments between the two sets of gait cycles in the control trial and before/after the verbal warning cue were different; the warning thus had a greater effect than natural gait variations. This suggests that the impact of a physical postural threat measured in other studies may reflect both the physical and psychological aspects of the threat produced by the heightening or narrowing of the walking surface. The dissociation of the effects of physical and psychological threats, therefore, seems possible to evaluate only the impact of the psychological state on balance control.
The second objective was to evaluate the effect of age on gait adaptations following a psychological postural threat. We assumed that the impact of a psychological postural threat would be more significant among older people. In each trial, the older group showed smaller stride length, greater step width, longer duration of double support, lower stabilizing force, and anteroposterior speed of the center of mass than the younger group. Without postural threats, these differences in walking and balance parameters between young and older people are common due to slower gait speed (Brown et al. 2002a). It is well known that in an environment where the perception of a fall is greater, older people alter their gait to be in a safer balance situation (Delbaere et al. 2009). In addition, the older adults tend to have greater postural responses to conditions they perceive as threatening to their stability. In similar conditions, young adults perceive threats as less intimidating (Laufer et al. 2006). On the other hand, the amount of attention that the older persons dedicate to postural control when anxiety increases is more significant than in younger adults (Brown et al. 2006). Our older participants had a slower gait speed on the treadmill only, likely to reduce the risk of falling and increase their safety (Brown et al. 2002a). These alterations in balance due to reduced gait speed could have limited the possibility to further adapt gait to the psychological threat and to the impending perturbations in the older adults.
The analysis of effect sizes revealed that a psychological postural threat reproduced the same effect as a physical postural threat in young participants. Adjustments following the introduction of the warning cue were much smaller in the older participants. Analysis of the individual data revealed that only three out of ten older participants showed similar results to the young participants, and every young participant showed effects (8–10 out of 10 young subjects, depending on variable affected by the warning). In situations, where balance is threatened, older adults prefer to maintain postural control by adopting safer strategies rather than to complete the task (Adkin et al. 2002). This could explain the absence of the warning effect in most of the older people, because they already adapted their gait during the control trial at the beginning of the experiment. They might have already been more vigilant and changed their gait to maintain safer balance before the introduction of the warning cue (Adkin et al. 2002). One can consider the idea of a limit in feasible adaptations, such that the possibility of changes may be too small to adapt their gait when faced with a threat without affecting their balance or gait function. Based on these results, the older adults seem less sensitive to verbal warnings of an impending danger.
The final objective was to assess the impact of a verbal warning cue indicating an imminent perturbation in walking and balance changes under two conditions: the first introduced a perturbation not yet experienced by the participants, while the second introduced known but unpredictable perturbations. We assumed that having already experienced the perturbations alluding to the threat would change the effect. However, the effect of the warning cue did not change between the two perturbation conditions. Usually, adaptation to repeated perturbations is specific (Bhatt et al. 2013) and in the direction of the perceived threat (Laufer et al. 2006). Here, the type of adaptation was not dependent on the previous experience of perturbations or on the type of warning. Consequently, the observed adaptation may be a non-specific answer to a general threat to balance rather than a specific response to a known impending perturbation. Because the observed responses to the threat are generic and not modulated based on the content of the warning cue, one can question the beneficial effect of these strategies for the participants.
Study limitations
The presence of a harness and the experimental environment with the treadmill can be considered study limitations, because they fail to represent a real situation; they reduce the risk of injury in case of a fall and require maintenance of a steady gait speed, even though it is known that reducing speed is a strategy used to reduce the risk of falling (Espy et al. 2010). No direct stress level assessment (such as the galvanic skin response) or evaluation of the subjective perception of threat evoked by the warning cue was conducted. Hence, it is difficult to ensure that the warning was perceived as a threat by the participants other than by the similarity of the responses to the physical threat observed before. In addition, a direct comparison between a physical and psychological threat would be more valid to compare the magnitude of the effects of each situation. Only a comparison of mean values obtained in the previous studies could be performed. With a small sample size, this study lacked the statistical power to differentiate the effect between groups and yielded wide confidence intervals for sample sizes. In the absence of preliminary data on the effect of psychological threat, it was not possible to determine an adequate sample size. Despite that fact, calculation of effect size was used to show the magnitude of the effects and to facilitate comparisons with other studies on the same topic (Fritz et al. 2012). Analysis of the individual data showed that a few older adults exhibited the same behaviour as younger adults and the small sample size prevented this behaviour from being explained based on clinical characteristics.
Conclusion
The introduction of a psychological threat altered gait and balance parameters in the young participants. These effects were similar to those previously induced by a physical postural threat, only of lesser magnitude. This effect was not specific to the warning announcing perturbations and, therefore, seemed rather associated with the imminent, general danger it could represent for balance. The absence of the warning effect in most of the older group suggests that the differences between the young and older adults already observed in the control condition may limit the possibility of older adults generating small-magnitude changes induced by the threat in young adults or a low sensitivity of the older participants to verbal warning. Further studies on this topic are needed to confirm these observations in each population, particularly to determine whether the absence of response to a verbal warning cue depends on certain clinical characteristics in older participants.
References
Adkin AL, Frank JS, Carpenter MG, Peysar GW (2000) Postural control is scaled to level of postural threat. Gait Posture 12:87–93
Adkin AL, Frank JS, Carpenter MG, Peysar GW (2002) Fear of falling modifies anticipatory postural control. Exp Brain Res 143:160–170
Adkin AL, Campbell AD, Chua R, Carpenter MG (2008) The influence of postural threat on the cortical response to unpredictable and predictable postural perturbations. Neurosci Lett 435:120–125. doi:10.1016/j.neulet.2008.02.018
Belgen B, Beninato M, Sullivan PE, Narielwalla K (2006) The association of balance capacity and falls self-efficacy with history of falling in community-dwelling people with chronic stroke. Arch Phys Med Rehabil 87:554–561. doi:10.1016/j.apmr.2005.12.027
Bhatt T, Wang TY, Yang F, Pai YC (2013) Adaptation and generalization to opposing perturbations in walking. Neuroscience 246:435–450. doi:10.1016/j.neuroscience.2013.04.013
Bohannon RW (2006) Reference Values for the Five-Repetition sit-to-stand test : a descriptive meta-analysis of data from elders. Percept Mot Skills 103:215–222. doi:10.2466/pms.103.1.215-222
Brown LA, Frank JS (1997) Postural compensations to the potential consequences of instability: Kinematics. Gait Posture 6:89–97 doi:10.1016/S0966-6362%2896%2901106-X
Brown LA, Gage WH, Polych MA, Sleik RJ, Winder TR (2002a) Central set influences on gait. Age-dependent effects of postural threat. Exp Brain Res 145:286–296
Brown LA, Sleik RJ, Polych MA, Gage WH (2002b) Is the prioritization of postural control altered in conditions of postural threat in younger and older adults? J Gerontol Ser A Biol Sci Med Sci 57:M785–M792
Brown LA, Doan JB, McKenzie NC, Cooper SA (2006) Anxiety-mediated gait adaptations reduce errors of obstacle negotiation among younger and older adults: implications for fall risk. Gait Posture 24:418–423
Brown LA, Doan JB, Whishaw IQ, Suchowersky O (2007) Parkinsonian deficits in context-dependent regulation of standing postural control. Neurosci Lett 418:292–297
Buatois S, Miljkovic D, Manckoundia P et al (2008) Five times sit to stand test is a predictor of recurrent falls in healthy community-living subjects aged 65 and older. J Am Geriatr Soc 56:1575–1577. doi:10.1111/j.1532-5415.2008.01777.x
Caetano MJ, Gobbi LT, Sanchez-Arias Mdel R, Stella F, Gobbi S (2009) Effects of postural threat on walking features of Parkinson’s disease patients. Neurosci Lett 452:136–140. doi:10.1016/j.neulet.2009.01.053
Carpenter MG, Frank JS, Silcher CP, Peysar GW (2001) The influence of postural threat on the control of upright stance. Exp Brain Res 138:210–218
Chamberlin ME, Fulwider BD, Sanders SL, Medeiros JM (2005) Does fear of falling influence spatial and temporal gait parameters in elderly persons beyond changes associated with normal aging? J Gerontol Ser A Biol Sci Med Sci 60:1163–1167
Cleworth TW, Horslen BC, Carpenter MG (2012) Influence of real and virtual heights on standing balance. Gait Posture 36:172–176. doi:10.1016/j.gaitpost.2012.02.010
Cumming RG, Salkeld G, Thomas M, Szonyi G (2000) Prospective study of the impact of fear of falling on activities of daily living, SF-36 scores, and nursing home admission. J Gerontol Ser A Biol Sci Med Sci 55:M299–M305
Davis JR, Horslen BC, Nishikawa K, Fukushima K, Chua R, Inglis JT, Carpenter MG (2011) Human proprioceptive adaptations during states of height-induced fear and anxiety. J Neurophysiol 106:3082–3090. doi:10.1152/jn.01030.2010
Delbaere K, Crombez G, Vanderstraeten G, Willems T, Cambier D (2004) Fear-related avoidance of activities, falls and physical frailty. A prospective community-based cohort study. Age Ageing 33:368–373. doi:10.1093/ageing/afh106
Delbaere K, Sturnieks DL, Crombez G, Lord SR (2009) Concern about falls elicits changes in gait parameters in conditions of postural threat in older people. J Gerontol Ser A Biol Sci Med Sci 64:237–242. doi:10.1093/gerona/gln014
Desrosiers E, Nadeau S, Duclos C (2014) Balance during walking on an inclined instrumented pathway following incomplete spinal cord injury. Spinal Cord. doi:10.1038/sc.2014.215
Duclos C, Desjardins P, Nadeau S, Delisle A, Gravel D, Brouwer B, Corriveau H (2009) Destabilizing and stabilizing forces to assess equilibrium during everyday activities. J Biomech 42:379–382. doi:10.1016/j.jbiomech.2008.11.007
Duclos C, Miéville C, Gagnon D, Leclerc C (2012) Dynamic stability requirements during gait and standing exergames on the wii fit® system in the elderly. J NeuroEng Rehabil 9:1–7. doi:10.1186/1743-0003-9-28
Espy DD, Yang F, Bhatt T, Pai YC (2010) Independent influence of gait speed and step length on stability and fall risk. Gait Posture 32:378–382 doi:10.1016/j.gaitpost.2010.06.013
Filiatrault J, Desrosiers J, Trottier L (2009) An exploratory study of individual and environmental correlates of fear of falling among community-dwelling seniors. J Aging Health 21:881–894. doi:10.1177/0898264309340694
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198. doi:10.1016/0022-3956(75)90026-6
Friedman SM, Munoz B, West SK, Rubin GS, Fried LP (2002) Falls and fear of falling: which comes first? A longitudinal prediction model suggests strategies for primary and secondary prevention. J Am Geriatr Soc 50:1329–1335. doi:10.1046/j.1532-5415.2002.50352.x
Fritz CO, Morris PE, Richler JJ (2012) Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen 141:2–18. doi:10.1037/a0024338
Hamel D (2001) Évolution des traumatismes au Québec de 1991 à 1999. Institut national de santé publique du Québec, Montréal
Hauck LJ, Carpenter MG, Frank JS (2008) Task-specific measures of balance efficacy, anxiety, and stability and their relationship to clinical balance performance. Gait Posture 27:676–682. doi:10.1016/j.gaitpost.2007.09.002
Horak FB, Wrisley DM, Frank J (2009) The balance evaluation systems test (BESTest) to differentiate balance deficits. Phys Ther 89:484–498. doi:10.2522/ptj.20080071
Horslen BC, Murnaghan CD, Inglis JT, Chua R, Carpenter MG (2013) Effects of postural threat on spinal stretch reflexes: evidence for increased muscle spindle sensitivity? J Neurophysiol 110:899–906. doi:10.1152/jn.00065.2013
Hyndman D, Ashburn A, Stack E (2002) Fall events among people with stroke living in the community : Circumstances of falls and characteristics of fallers. Arch Phys Med Rehabil 83:165–170. doi:10.1053/apmr.2002.28030
Ilmane N, Croteau S, Duclos C (2015) Quantifying dynamic and postural balance difficulty during gait perturbations using stabilizing/destabilizing forces. J Biomech 48:441–448. doi:10.1016/j.jbiomech.2014.12.027
Laufer Y, Barak Y, Chemel I (2006) Age-related differences in the effect of a perceived threat to stability on postural control. J Gerontol Ser A Biol Sci Med Sci 61:500–504
Lelard T, Krystkowiak P, Montalan B et al (2014) Influence of postural threat on postural responses to aversive visual stimuli. Behav Brain Res 266:137–145. doi:10.1016/j.bbr.2014.02.051
Maki BE, Whitelaw RS (1993) Influence of expectation and arousal on center-of-pressure responses to transient postural perturbations. J Vestib Res Equilib Orientat 3:25–39
McKenzie NC, Brown LA (2004) Obstacle negotiation kinematics: age-dependent effects of postural threat. Gait Posture 19:226–234 doi:10.1016/S0966-6362%2803%2900060-2
Mendes de Leon CF, Seeman TE, Baker DI, Richardson ED, Tinetti ME (1996) Self-efficacy, physical decline, and change in functioning in community-living elders: a prospective study. J Gerontol B Psychol Sci Soc Sci 51:S183–S190
Mullie Y, Duclos C (2014) Role of proprioceptive information to control balance during gait in healthy and hemiparetic individuals. Gait Posture 40:610–615. doi:10.1016/j.gaitpost.2014.07.008
Myers AM, Fletcher PC, Myers AH, Sherk W (1998) Discriminative and evaluative properties of the activities-specific balance confidence (ABC) scale. J Gerontol Ser A Biol Sci Med Sci 53A:M287–M294. doi:10.1093/gerona/53A.4.M287
O’Hoski S, Winship B, Herridge L, Agha T, Brooks D, Beauchamp MK, Sibley KM (2014) Increasing the clinical utility of the BESTest, Mini-BESTest, and Brief-BESTest: normative values in canadian adults who are healthy and aged 50 years or older. Phys Ther 94:334–342. doi:10.2522/ptj.20130104
Pasman EP, Murnaghan CD, Bloem BR, Carpenter MG (2011) Balance problems with Parkinson’s disease: are they anxiety-dependent? Neuroscience 177:283–291. doi:10.1016/j.neuroscience.2010.12.050
Pijnappels M, Bobbert MF, van Dieën JH (2001) Changes in walking pattern caused by the possibility of a tripping reaction. Gait Posture 14:11–18. doi:10.1016/S0966-6362(01)00110-2
Powell LE, Myers AM (1995) The Activities-specific Balance Confidence (ABC) Scale. J Gerontol Ser A Biol Sci Med Sci 50A:M28–M34. doi:10.1093/gerona/50A.1.M28
Rossier P, Wade DT (2001) Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairment. Arch Phys Med Rehabil 82:9–13. doi:10.1053/apmr.2001.9396
Rubenstein LZ (2006) Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing 35:ii37–ii41. doi:10.1093/ageing/afl084
Shaw JA, Stefanyk LE, Frank JS, Jog MS, Adkin AL (2012) Effects of age and pathology on stance modifications in response to increased postural threat. Gait Posture 35:658–661. doi:10.1016/j.gaitpost.2011.12.020
Staab JP, Balaban CD, Furman JM (2013) Threat assessment and locomotion: clinical applications of an integrated model of anxiety and postural control. Semin Neurol 33:297–306. doi:10.1055/s-0033-1356462
Tersteeg MCA, Marple-Horvat DE, Loram ID (2012) Cautious gait in relation to knowledge and vision of height: Is altered visual information the dominant influence? J Neurophysiol 107:2686–2691. doi:10.1152/jn.00875.2011
Tinetti ME, Speechley M (1989) Prevention of falls among the elderly. N Engl J Med 320:1055–1059. doi:10.1056/NEJM198904203201606
Tinetti ME, Doucette J, Claus E, Marottoli R (1995) Risk factors for serious injury during falls by older persons in the community. J Am Geriatr Soc 43:1214–1221
van Schenau I (1980) Some fundamental aspects of the biomechanics of overground versus treadmill locomotion. Med Sci Sports Exerc 12:257–261
Whitney SL, Wrisley DM, Marchetti GF, Gee MA, Redfern MS, Furman JM (2005) Clinical measurement of sit-to-stand performance in people with balance disorders: validity of data for the five-times-sit-to-stand test. Phys Ther 85:1034–1045
Winter DA (2009) Biomechanics and motor control of human movement. Wiley, Hoboken
Zijlstra GAR, Van Haastregt JCM, Van Rossum E, Van Eijk JTM, Yardley L, Kempen GIJM (2007) Interventions to reduce fear of falling in community-living older people: a systematic review. J Am Geriatr Soc 55:603–615. doi:10.1111/j.1532-5415.2007.01148.x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Dubreucq, L., Mereu, A., Blanc, G. et al. Introducing a psychological postural threat alters gait and balance parameters among young participants but not among most older participants. Exp Brain Res 235, 1429–1438 (2017). https://doi.org/10.1007/s00221-017-4902-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-017-4902-y