
Abstract
Motor resonance is typically considered a modulation of motor activity during action observation, which mirrors the pattern of muscle activation occurring during execution of the observed action. There is preliminary evidence that motor activity accompanying action observation comprises two stages: an initial non-specific modulation, followed by a later change in excitability that is specific to the muscles involved in the action. We built on this previous work, with the aims of (1) clarifying the time-course of muscle specificity during action observation and (2) establishing whether modulation at each time point reflects significant changes (facilitation or suppression) from baseline. Motor-evoked potentials were elicited in two muscles—the first dorsal interosseous (FDI) and abductor digiti minimi (ADM)—while participants watched stimuli showing index or little finger abduction. Our results provide partial support for previous findings of muscle-specific modulation after, but not before, 200 ms. Interestingly, however, this was shown only by facilitation of the FDI during index finger observation; there was no significant facilitation of the ADM when little finger movement was observed. Furthermore, we found no facilitation of corticospinal excitability (specific or non-specific) at time points earlier than 200 ms (100–150 ms). We discuss these results in the context of previous work showing a non-specific increase in excitability at 90 ms during action observation. Together, these findings suggest a fast and short-lived facilitation of corticospinal excitability that occurs at around 60–90 ms and ends by 100–150 ms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
When an individual observes another agent performing an action, the observer’s motor system is activated in a manner that seems similar to the activation that would occur if the observer were performing the action themselves (e.g. Fadiga et al. 1995). This motor activation during observation is known as ‘motor resonance’ or ‘mirroring’ and might be involved in our ability to understand (Iacoboni et al. 1999) and imitate (Rizzolatti and Craighero 2004) the actions of others. For motor resonance to be a viable mechanism behind action understanding or imitation, it seems logical that the activation that occurs must be relatively specific to the observed action. For example, to ‘understand’ the difference between grasping a cup and pointing to a cup, the timing and muscle specificity of motor activation during observation of the two actions should be distinguishable. Although there is a large body of work on motor resonance, and a general assumption that such resonance is specific, questions remain as to what specificity means in the context of mirroring, and—more generally—what constitutes motor resonance. One question in particular relates to the time-course of muscle specificity when observing actions made by others.
There is preliminary evidence of different levels of specificity in early and later phases of excitability changes during action observation (Candidi et al. 2014; Cavallo et al. 2013; Lepage et al. 2010; Roy et al. 2008; van Schie et al. 2008). At the peripheral level, research suggests that early modulation of motor excitability is not specific to the muscles involved in the action, while later modulation—from around 200 ms—is muscle-specific (Cavallo et al. 2013; Lepage et al. 2010). In Cavallo et al.’s (2013) study, motor-evoked potentials (MEPs) were recorded from two intrinsic hand muscles—the abductor digiti minimi (ADM) and the first dorsal interosseous (FDI)—while participants observed little and index finger abductions. Previous research has shown the FDI to be significantly more active than the ADM during the execution of index finger abduction, while the opposite is true for little finger abduction (Romani et al. 2005). Assessing MEPs at five time points across the movement, Cavallo and colleagues found evidence of muscle-specific modulation at 200, 250, and 300 ms, but not at 100 or 150 ms, post-movement onset.
Cavallo et al.’s (2013) study is one of the few to investigate modulation at such early time points; the majority of studies have examined MEPs elicited 1 s or later after movement onset (for a review, see Naish et al. 2014). Nonetheless, muscle-specific modulation has been shown at later time points by a number of studies, and Cavallo and colleagues’ results suggest that this specificity is first evident at around 200 ms. The approach to data analysis taken by Cavallo and colleagues provides a useful way of quantifying muscle specificity. However, their report did not show whether motor excitability in the muscles was actually modulated relative to a non-action baseline. MEPs in each muscle were compared to each other, and specificity (or lack thereof) was defined based on the difference between the muscles in their relative responsiveness to each movement type. For each muscle, Cavallo and colleagues calculated a ratio of MEP size during index finger observation relative to MEP size during little finger observation (i.e. a ratio of 1 represented comparable responsiveness to both movements). Larger ratios (a ratio >1 indicating a greater response during index than during little finger observation) for the FDI than the ADM (evident at 200, 250, and 300 ms) were interpreted as muscle-specific modulation, while no difference in ratio size between the muscles (found at 100 and 150 ms) was interpreted as non-specificity.
As suggested by the authors themselves (Cavallo et al. 2013, p. 1), the muscle-specific nature of modulation is (or should be) what defines the response as “mirror”. However, to better explore the potential role of motor resonance in behaviour, it is important also to look at how activity is changed relative to a non-action baseline. Given that motor resonance is usually defined as some increase in motor activity above a non-action baseline, it is unclear whether differences between muscles or movement types (that are not necessarily different from baseline) should be regarded as indications of motor resonance at all. Muscle-specific modulation, such as that found from 200 ms by Cavallo et al. (2013), could arise in the absence of what has most often been regarded as motor resonance (i.e. facilitation of muscles involved in the action). For example, a ratio greater than 1 for the FDI—indicating larger MEPs during index than little finger observation—could be driven by facilitation of this muscle during index finger observation, suppression during little finger observation, or both. In the extreme case, a ratio of greater than 1 could arise with suppression of the FDI during index finger observation (but with greater suppression during little finger observation). In this case, there would be muscle specificity in the absence of motor facilitation.
Although non-facilitatory but muscle-specific responses could play a role in social functions such as action imitation or understanding, it seems that whether or not there is absolute facilitation of muscle excitability could have important implications for the role of these responses in behaviour. It is possible that what we consider ‘resonance’ sometimes reflects motor facilitation, other times suppression, and other times no significant change from baseline. It is also important to establish whether there is a change in excitability—be it specific or non-specific—at time points earlier than 200 ms. Although Cavallo and colleagues’ results showed non-specificity at 100 and 150 ms, it is not known whether there was non-specific facilitation, suppression, or simply no modulation of motor activity. The finding of non-specificity is, in fact, consistent with the results of Lepage et al. (2010), who found facilitation of MEPs in both the ADM and FDI during index finger observation at 90 ms from movement onset. In this case, MEPs in both muscles were facilitated during action observation compared to when participants watched a static hand or a moving dot. Interestingly, however, Lepage and colleagues’ study did not show any facilitation (relative to viewing a static hand or dot) at later time points (120–270 ms), so it is not completely clear how this early facilitation relates to later modulation found in other studies. As so few studies have examined early time points, the temporal progression of motor resonance—in terms of both muscle specificity and absolute change from baseline—needs to be clarified.
The present study sought to consolidate and build on existing work on the time-course of motor activity during action observation and was based largely on the experimental design of Cavallo et al. (2013) but with an additional ‘static hand’ baseline condition. The static hand was used as a baseline because we wanted to investigate effects of action observation, rather than just effects of seeing a hand. Using a lower-level baseline would not have allowed us to disentangle effects of movement per se. In addition, this allowed easier comparison with the results of Lepage et al. (2010). MEPs in the ADM and FDI were assessed at 100, 150, 200, 250, and 300 ms from movement onset, as participants watched index finger abduction, little finger abduction, or a static hand. A fourth condition—a moving shape—was also presented to the participants, but this condition was ultimately excluded from the analysis for reasons outlined in the “Method” section.Footnote 1 To keep the experiment at a manageable duration for the participants (considering the additional conditions), the number of trials per cell of the design was reduced to ten (compared to 12 per cell used by Cavallo et al.). As ten trials per condition was deemed too low to be able to compare between conditions, data for the first two and final two time points were collapsed to give an ‘early’ and a ‘late’ time bin (comprising 20 trials each).
Based on the work of Cavallo et al. (2013), we predicted that any differences between modulations in each of the muscles would be present in the later phase (after 200 ms) only. The novel question in this study was whether the changes in excitability at each stage of movement observation (early and late) reflect significant modulation relative to the static hand condition. Based on Lepage et al. (2010) findings, we should expect modulation at the early time point to be non-specific but significantly facilitated. As suggested above, however, the lack of significant facilitation at later time points in Lepage et al. (2010) brings into question the nature of modulation in this study, so the current investigation is necessary to clarify these previous findings.
Method
Participants
Our sample consisted of 16 staff and students of Wilfrid Laurier University (3 male, 13 female), who were recruited via online advertisements and emails. Participants were aged 18–40 years (M = 22.4, SD = 6.52), and all were right-handed. The study was approved by Wilfrid Laurier University’s Research Ethics Board and conformed to the guidelines of the Declaration of Helsinki.
Design
As noted above, the experimental design included an additional ‘moving shape’ condition, but the data from this condition were not included in the final analysis. The reason for this exclusion was that the stimuli in the shape condition were more variable than the stimuli comprising the other three conditions; specifically, the shape was stationary on some trials but moving on others. Due to this difference in variation within the shape condition, we decided retrospectively that it was not meaningful to compare this condition to the other (less visually variable) conditions. The shape condition will not be discussed further in this paper due to not being included in the final analysis, but a description of the stimuli can be found in the Supplemental Materials.
The experiment followed a 3 × 2 × 5 repeated-measures design, with the factors ‘action’ (little finger abduction, index finger abduction, static hand), muscle (ADM, FDI), and stimulation time (100, 150, 200, 250, 300 ms). Participants viewed 150 trials in total, which were presented in five blocks of 40 trials. There were equal number of trials of each condition; thus, ten trials contributed to each condition (i.e. each time point for each condition). The order of trials was randomised within each block for each participant, and the order of blocks was randomised for each participant. Due to the low number of trials per cell at the lowest level of the design, the early (100 and 150 ms) and late (250 and 300 ms) time points were collapsed, so that ‘time’ became a two-level factor for the final analysis. The results of analyses including all five individual time points can be found in the Supplementary Materials.
Apparatus and stimuli
Visual stimuli were presented using Superlab (version 4.2), which also controlled the timing of TMS delivery. TMS was delivered using a Magstim Rapid2 stimulator with a figure-of-eight coil (Magstim, Wales, UK), and muscle activity recorded using self-adhesive snap electrodes (23 × 22 mm). The data were acquired at a sampling rate of 5 kHz, amplified and filtered (band-pass 10–500 Hz), using Biopac MP150 hardware and Acqknowledge software (version 4.2.0; Biopac Systems, Inc). Offline analysis was performed using Matlab (version 2010a) and SPSS (version 16.0).
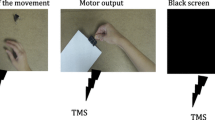
The hand stimuli were the same as those used by Cavallo et al. (2013) and showed a female Caucasian hand (visible from the wrist) prone on a black background. On the index and little finger abduction trials, an image of a prone hand was presented, followed after a variable delay by the presentation of the same prone hand with the index finger or little finger abducted. This gave the impression of index or little finger movement. To keep the design as similar as possible to Cavallo and colleagues’, we used the same presentation timings, with the static hand being presented for a randomly selected duration between 800 and 2800 ms. The abducted finger image was then presented for 960 ms, followed by a fixation cross for 7240 ms. The static hand trials followed the same design, but instead of an image of the hand with a finger abducted, the same static hand image remained on the screen. Thus, the static hand was present for 1760–3760 ms. An example of each trial type with a summary of timings is shown in Fig. 1. To ensure that participants were attentive to the stimuli, on a subset of trials, a dot of similar colour to the stimulus hand appeared on the second hand image. Four times per block, at a random point during the block, the text “Did you see a dot on the last trial? Press ‘1’ for yes or ‘2’ for no” appeared on the screen. This text remained on the screen until the participant made a (left-handed) key press response. The maximum trial duration was around 11 s, and each of the five blocks of trials lasted approximately 6–8 min. Participants were invited to take breaks in between the blocks.

Example of stimuli belonging to each of the three observation conditions, with presentation timings. The time of TMS delivery was relative to movement onset (or the equivalent on static trials), indicated by ‘0 ms’ on the figure
Procedure
Self-adhesive electromyography (EMG) electrodes were positioned to record from two muscles: the ADM and FDI. Two electrodes were placed on the skin overlaying each muscle, and one further electrode was placed over the ulnar styloid process of the wrist as the ground. The ‘hand’ area of the motor cortex was found by first measuring a distance 4 cm lateral and 1 cm anterior to the vertex, and eliciting MEPs in this approximate area to find the position from which responses could be elicited in both of the muscles. The resting motor threshold (RMT) was defined as the lowest intensity of stimulation required to evoke responses of above .05 mV in both of the muscles. Stimulation intensity during the experiment was set at 115 % of this RMT.Footnote 2
Participants were seated in front of a computer monitor on which the stimuli were displayed; their dominant hand and forearm rested (prone) on an armrest, such that their arm and hand were parallel to the sagittal plane (i.e. in the same orientation as the hand presented on the screen). They were told that they would see a hand or a shape on the screen, which would sometimes move, and that a few times per block they would be asked to indicate (by pressing a key using their left hand) whether they had seen a dot on the previous trial. The experimenter monitored the EMG recording throughout the blocks and reminded participants to relax their hand and arm if there was a visible increase in activity in the muscles.
Data analysis
MEP amplitude was defined as the difference between the minimum and maximum values of the EMG signal in the 10–40 ms window following the TMS pulse. Trials were excluded if EMG activity in the 100 ms preceding the TMS pulse exceeded 50 microvolts. Across all 16 subjects, this resulted in a total of nine trials (.3 %) being excluded. The average number of trials contributing to each cell of the design (i.e. for each ‘time’ and ‘action’ condition combination) was 18.9 (SD = .24; minimum = 17).
The data were normalised to the static hand condition by dividing MEP size by the mean amplitude of MEPs elicited during static hand trials for that participant and block. The 100 and 150 ms, and the 250 and 300 ms time points were collapsed to give an ‘early’ and a ‘late’ time bin. The normalised data were then submitted to a 2 × 2 × 2 repeated-measures ANOVA, with time (early, late), action (little finger abduction, index finger abduction), and muscle (ADM, FDI) as predictor variables. In addition, we conducted one-sample t tests to compare the normalised MEP values for each condition to 1, to assess directly modulation relative to the static hand. Because the comparisons to baseline at these relatively early time points were exploratory, the alpha criterion for significance was made more stringent (decreased to .006) for this analysis to account for the eight t tests that were performed.
Results
The average accuracy for the dot-detection task was 78.1 % (SD = 18.9). This performance level was shown (by a one-sample t test) to be significantly above chance [t(15) = 5.96, p < .001, Cohen’s d = 1.49], suggesting that the participants were paying attention to the stimuli.
The 2 × 2 × 2 ANOVA revealed an interaction between action and time (F(1,15) = 7.49, p = .015, η 2 = .333) and a three-way interaction between action, muscle, and time (F(1,15) = 16.55, p = .001, η 2 = .525). Collapsing across the two muscles to examine the two-way interaction showed that MEP size increased (from early to late) during index finger observation, but decreased during little finger observation. However, paired-sample t tests revealed that this change across time was not significant for either action type (index finger observation: t(15) = −1.40, p = .181; little finger observation: t(15) = 2.0, p = .063).
To explore the three-way interaction, subsequent analyses were conducted separately for the early and late time points. Consistent with the findings of Cavallo et al. (2013), these analyses revealed a significant interaction between action and muscle at the later (250–300 ms) point (F(1,15) = 8.43, p = .011, η 2 = .360), but not at 100–150 ms (F(1,15) = 1.41, p = .253, η 2 = .086). Because this interaction at the later time point was predicted, we did not apply corrections for multiple comparisons in the following comparisons.
Follow-up paired-sample t tests for the ‘late’ time point showed that (1) MEPs in the FDI were larger during index finger observation than during little finger observation [t(15) = 2.99, p = .009, Cohen’s d = .746]; and (2) during index finger observation, MEPs in the FDI were significantly larger than those elicited in the ADM [t(15) = 2.55, p = .022, Cohen’s d = .637]. There was also a nearly significant difference between muscles for the little finger observation condition [t(15) = 2.00, p = .064, Cohen’s d = .499], with MEPs in the ADM being larger than those elicited in the FDI. MEPs elicited in the ADM did not differ according to the action type that was being observed [t(15) = .402, p = .693; see Fig. 2].

MEP amplitude (normalised to the static hand condition) at early (left) and later (right) time points during the observation of index and little finger abduction. Data points represent the mean across participants, and error bars represent standard error. The dotted line at ‘1’ on the y-axis represents no modulation during action observation compared to viewing the static hand, and the asterisks indicate significance between the muscles (indicated also by the line referring to the two ‘muscle’ lines) or between action types (asterisk alone)
Comparisons to baseline
The one-sample t tests performed to assess the significance of MEP modulation from baseline (i.e. static hand) showed that the FDI was significantly facilitated at 250–300 ms during index finger observation [t(15) = 3.25, p = .005, Cohen’s d = .812; significant at the Bonferroni-corrected level].
Discussion
This study set out to build on previous work suggesting that action observation is associated with early, non-specific modulation, followed by a later, muscle-specific modulation of motor excitability (Cavallo et al. 2013; Lepage et al. 2010). More specifically, we aimed to establish the time at which changes in motor activity during action observation become muscle-specific, and whether the early non-specific (and, indeed, muscle-specific) modulation constitutes significant facilitation or suppression relative to baseline.
Our findings confirm what has been suggested by previous research, that motor activation during action observation does not become muscle-specific until after 200 ms. Interestingly, however, clear muscle specificity was only evident for index finger observation. When the participants watched index finger abduction, the muscle involved in this action (the FDI) was facilitated to a greater degree than the muscle not involved in the action (the ADM). In addition, comparison of MEPs elicited during index finger observation to those elicited during observation of the static hand showed that the FDI was significantly facilitated in response to viewing this movement. In contrast, little finger observation did not lead to significantly larger MEPs in the ADM relative to the FDI, nor were MEPs in the ADM significantly facilitated relative to baseline. It is important to note that the difference between the two muscles for little finger observation was close to significance and that statistical power for this comparison (calculated post hoc) was relatively low. Therefore, it is possible that with a larger dataset we would have seen muscle-specific resonance for observation of both index and the little finger abduction. However, it should also be noted that our pattern of results is in fact consistent with that of Kaneko et al. (2007), who found significant facilitation of the FDI during index finger observation, but not of the ADM during little finger observation.
Although other studies have found ADM facilitation during little finger observation using similar experimental designs (e.g. Romani et al. 2005), it is possible that the motor representation of the ADM (or of little finger movement) is weaker than that of the FDI, making this effect less stable across individuals and studies. A possible explanation for a more stable muscle-specific motor resonance associated with index finger compared to little finger observation is that the former is more frequently performed and observed. The index finger is commonly used in actions that require only one digit, such as pointing and button pressing and is often used in synergy with the thumb to grasp or manipulate objects. In contrast, the little finger is more often involved in movements together with the rest of the hand and rarely performs actions as an independent digit. Indeed, it has been found that index finger movement is more individuated than movement of the other digits; i.e. there is less movement in other fingers when a person attempts to move only their index finger, compared to movement in other fingers when the person is instructed to move only their little finger (Häger-Ross and Schieber 2000). It is possible, therefore, that the motor representations underlying index finger abduction are more defined than those underlying little finger abduction. There is indeed some evidence that visual (Jola et al. 2012) or motor (Cross et al. 2006) experience of an action enhances the motor resonance response to observing that action. This could explain why the present study, and some previous work (Kaneko et al. 2007) have failed to find significant facilitation of the ADM during the observation of little finger abduction, which is a relatively infrequent movement.
Another feature of the current design (and, indeed, most studies of this type) that must be considered when interpreting differences between muscles, is that the intensity of stimulation was set based on the intensity required to elicit responses in both muscles. As noted in the Method section, this means that the RMT from which stimulation intensity was calculated (stimulation was at 115 % of RMT) was based on the less excitable (higher threshold) muscle. Generally, a higher stimulation intensity is required to elicit MEPs in the ADM, so it is possible that in some subjects the FDI may have been ‘over-stimulated’, with respect to its motor threshold, compared to the ADM. This could have affected the extent of modulation that was detected. It should be noted, however, that this approach to determining stimulus intensity is standard in studies of this type, including studies in which clear muscle-specific responses have been found (e.g. Romani et al. 2005). Additionally, a recent study (Loporto et al. 2013) found that motor resonance was present during index finger abduction observation when stimulation intensity was set to 110 % of RMT, but not when it was at 130 %. Based on this finding, we would predict that if differences between the muscles in RMT-relative intensity had affected motor resonance, then we would be more likely to find resonance in the muscle stimulated at an intensity closer to 115 % of its RMT than the muscle stimulated at a higher intensity. Thus, if we speculate that the ADM (the higher threshold muscle) was stimulated at around 115 %, while the FDI was stimulated at a higher percentage of its threshold, then motor resonance would be greater for the ADM (if intensity had affected resonance). In fact, we found effects of action observation in the FDI but not the ADM, suggesting that differences in intensity would not explain our pattern of results. Nonetheless, it is possible that differences in relative stimulation intensity could have influenced our pattern of results, and this is a factor to bear in mind for future studies.
At the earlier time period (100–150 ms), there were no differences between the muscles during either movement observation condition. This finding is consistent with previous work (Cavallo et al. 2013; Lepage et al. 2010) showing no specificity at early time points (90, 100, or 150 ms) and suggests that any modulation occurring before this time could not underlie any function that distinguishes between similar actions. Crucially, our results showed that MEPs elicited at 100–150 ms were not significantly larger than those elicited during static hand observation. This is different to the modulation found at 90 ms by Lepage and colleagues, which was significantly facilitated relative to viewing a static hand. However, it is consistent with the modulation found by these researchers at later time points. At 120–150, 180–210, and 240–270 ms, Lepage et al. reported no differences between MEPs elicited during action observation compared to static hand observation. Our finding of no facilitation at 100–150 ms, together with the results reported by Lepage and colleagues, suggests that the early non-specific facilitation found at 90 ms might represent a very brief period of modulation, which is potentially over by (at the latest) 150 ms. This is supported by the lack of difference between movement versus static hand observation at time points between 120 and 270 ms reported in Lepage and colleagues’ paper.
It is important to note that the term ‘facilitation’ in this paper refers to facilitation relative to viewing the static hand; so, any modulation is specific to viewing biological movement rather than viewing just the effector itself. This suggests that the early and brief facilitation that purportedly occurs at around 90 ms is a response to movement observation. The lack of facilitation found here at 100–150 ms is only a lack of difference between movement and stationary stimuli; it is possible that at 90 ms, there is a rapid response to biological movement, but modulation at slightly later latencies reflects a response to viewing the static hand. Such modulation is in fact similar to that reported by Makin et al. (2009), who investigated effects on motor excitability of an object falling (unexpectedly) near to the hand when participants were due to make a manual response. In this case, there was a modulation of corticospinal excitability at 80 ms (relative to appearance of the falling object), but not at 100 ms, suggesting that this modulation was very short-lived. Although the modulation shown by Makin et al. (2009) was associated with an object approaching the hand as participants performed a manual task, their results show that modulation of motor activity in response to visual stimuli can occur as early as 80 ms, so a similar rapid modulation could well occur in response to action observation (see also Discussion in Naish et al. 2014).
In conclusion, we have confirmed previous findings that muscle-specific motor resonance does not occur until at least 200 ms. Therefore, it is unlikely that modulation occurring before this point could underlie any form of action processing that requires distinguishing between similar movements. Furthermore, comparing modulation at each time point directly to the static hand baseline revealed no facilitation of excitability in either muscle at 100–150 ms, suggesting that early non-specific facilitation reported earlier than this (Lepage et al. 2010) is transient in nature. Further research is required to explore the functional significance of this early modulation, and whether it predicts any aspects of later muscle-specific modulation.
Notes
Further details about the shape condition, as well as the data from this and the other conditions, can be obtained from the corresponding author if required.
Because the RMT was based on the intensity of TMS needed to evoke responses in both the ADM and the FDI, it actually reflected the lowest intensity required to elicit MEPs in the least excitable muscle. Thus, in some cases, the stimulation intensity would have reflected different percentages of the RMT for each muscle (i.e., what we consider to be ‘115 % of the RMT’ might in fact have reflected 120 % of the RMT for the muscle with the lowest threshold). The implications of this are mentioned briefly in the “Discussion” section.
References
Candidi M, Sacheli LM, Mega I, Aglioti SM (2014) Somatotopic mapping of piano fingering errors in sensorimotor experts: TMS studies in pianists and visually trained musical naïves. Cereb Cortex 24:435–443
Cavallo A, Heyes C, Becchio C, Bird G, Catmur C (2013) Timecourse of mirror and counter-mirror effects measured with transcranial magnetic stimulation. Soc Cogn Affect Neurosci. doi:10.1093/scan/nst085
Cross ES, Hamilton AFC, Grafton ST (2006) Building a motor simulation de novo: observation of dance by dancers. NeuroImage 31(1):1257–1267
Fadiga L, Fogassi L, Pavesi G, Rizzolatti G (1995) Motor facilitation during action observation: a magnetic stimulation study. J Neurophysiol 73(6):2608–2611
Häger-Ross C, Schieber MH (2000) Quantifying the independence of human finger movements: comparisons of digits, hands, and movement frequencies. J Neurosci 20(22):8542–8550
Iacoboni M, Woods RP, Brass M, Bekkering H, Mazziotta JC, Rizzolatti G (1999) Cortical mechanisms of human imitation. Science 286(5449):2526–2528
Jola C, Abedian-Amiri A, Kuppuswamy A, Pollick FE, Grosbras M (2012) Motor simulation without motor expertise: enhanced corticospinal excitability in visually experienced dance spectators. PLoS One. doi:10.1371/journal.pone.0033343
Kaneko F, Yasojima T, Kizuka T (2007) Kinesthetic illusory feeling induced by a finger movement movie effects on corticomotor excitability. Neuroscience 149:976–984
Lepage JF, Tremblay S, Theoret H (2010) Early non-specific modulation of corticospinal excitability during action observation. Eur J Neurosci 31(5):931–937
Loporto M, Holmes PS, Wright DJ, McAllister CJ (2013) Reflecting on mirror mechanisms: Motor resonance effects during action observation only present with low-intensity transcranial magnetic stimulation. PLoS ONE 8(5):e64911. doi:10.1371/journal.pone.0064911
Makin TR, Holmes NP, Brozzoli C, Rossetti Y, Farnè A (2009) Coding of visual space during motor preparation: approaching objects rapidly modulate corticospinal excitability in hand-centred coordinates. J Neurosci 29(38):11841–11851
Naish KR, Houston-Price C, Bremner AJ, Holmes NP (2014) Effects of action observation on corticospinal excitability: muscle specificity, direction, and timing of the mirror response. Neuropsychologia 64:331–348
Rizzolatti G, Craighero L (2004) The mirror-neuron system. Annu Rev Neurosci 27:169–192
Romani M, Cesari P, Urgesi C, Facchini S, Aglioti SM (2005) Motor facilitation of the human cortico-spinal system during observation of bio-mechanically impossible movements. Neuroimage 26:755–763
Roy AC, Craighero L, Fabbri-Destro M, Fadiga L (2008) Phonological and lexical motor facilitation during speech listening: a transcranial magnetic stimulation study. J Physiol (Paris) 102(1–3):101–105
van Schie HT, Koelewijn T, Jensen O, Oostenveld R, Maris E, Bekkering H (2008) Evidence for fast, low-level motor resonance to action observation: an MEG study. Soc Neurosci 3(3–4):213–228
Acknowledgments
This work was supported by a SSHRC grant awarded to SSO. We thank Dr Caroline Catmur for her permission to use the stimuli used in Cavallo et al. (2013), and Megan Grocholsky for her help with data collection.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Naish, K.R., Obhi, S.S. Timing and specificity of early changes in motor excitability during movement observation. Exp Brain Res 233, 1867–1874 (2015). https://doi.org/10.1007/s00221-015-4258-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-015-4258-0