
Abstract
The aim of this study was to determine whether there were significant changes in the time course of the functional magnetic resonance imaging (fMRI) signal in motor and non-motor regions of both cerebral hemispheres during a unilateral fatiguing exercise of the hand. Twelve subjects performed a submaximal (30%) intermittent fatiguing handgrip exercise (3 s grip, 2 s release, left hand) for ∼9 min during fMRI scanning. Regression analysis was used to measure changes in fMRI signal from primary sensorimotor cortex (SM1), premotor cortex and visual cortex (V1) in both hemispheres. Force declined to 77 ± 3.6% of prefatigue maximal force (P < 0.05). The fMRI signal from SM1 contralateral to the fatiguing hand increased by 1.2 ± 0.5% of baseline (P < 0.05). The fMRI signal from the ipsilateral SM1 did not change significantly. Premotor cortex showed a similar pattern but did not reach significance. The signal from V1 increased significantly for both hemispheres (contralateral 1.3 ± 0.9%, ipsilateral 1.5 ± 0.9% of baseline and P < 0.05). During the performance of a unimanual, submaximal fatiguing exercise there is an increase in activation of motor and non-motor regions. The results are in keeping with the notion of an increase in sensory processing and corticomotor drive during fatiguing exercise to maintain task performance as fatigue develops.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Functional magnetic resonance imaging (fMRI) studies of fatiguing hand exercises have shown changes in the fMRI signal that may be related to exercise-induced changes in descending motor drive and processing of sensory information, or alterations in neurohaemodynamic coupling. We have previously shown that performance of a motor task after a unilateral fatiguing exercise is associated with reduced activation in primary sensorimotor cortex (SM1) with movement of either the fatigued or non-fatigued hand. However these effects are not limited to SM1, and secondary motor regions (supplementary motor area, cerebellum), and even the primary visual cortex show a similar time course and magnitude of reduction in cortical activation (Benwell et al. 2006b). This reduction is associated with a post-exercise increase in the variance of the fMRI signal, which could have a neurophysiological and/or neurohaemodynamic basis (Benwell et al. 2005).
Central changes are also known to occur during fatiguing exercise, and these have been most widely studied with transcranial magnetic stimulation. During submaximal and intermittent maximal fatiguing exercise there is a steady increase in corticomotor excitability together with a reduction in short- and long-interval intracortical inhibition and a prolongation of the cortical silent period (Benwell et al. 2006a, c; Sacco et al. 1997; Taylor et al. 1996). Some of these effects are confined to the fatigued muscle whereas others are observed for non-fatigued muscles, and the patterns of change are consistent with a central adaptive response to fatigue as well as a central contribution to fatigue. An increase in the fMRI signal has been reported during fatiguing exercise and it has been found that these effects are not confined to primary motor areas but can extend to premotor areas (Liu et al. 2002, 2003). These results probably reflect a combination of changes in cerebral haemodynamics and oxygen consumption during exercise (Gonzalez-Alonso et al. 2004), and the central adaptive processes related to exercise. It is not clear how extensive these effects are, and whether, as with the post-exercise period, these changes can be observed outside the motor network.
In the present study, cortical activation during a unimanual submaximal, intermittent fatiguing task was investigated by measuring the time course of the fMRI signal from multiple sensorimotor regions and from visual cortex during exercise. The time-course approach was used in preference to a block-design analysis as the latter assumes a relatively stable level of activation during each task block and intervening rest period, which may not be the case during fatiguing exercise. The aim of the study was to determine whether there were significant changes in the time course of the fMRI signal in SM1 during unimanual fatiguing hand exercise, how this compared for the fatigued and non-fatigued hands, and whether any such changes were confined to motor areas.
Methods
With the approval of the Human Research Ethics Committee of the University of Western Australia 12 subjects (6M; 18–48 years of age) gave written informed consent to participate in this study.
Handgrip device
For the handgrip device, the thumb was isolated from the other fingers of the hand by a plastic padded bar which lay across the palm of the hand (refer to Benwell et al. 2006b for illustration of device). Subjects pulled on a lever with their four fingers towards the bar (distance 30 mm). The load subjects pulled against was determined by a set of interchangeable springs (1–30 kg) attached to the opposite side of the lever. Fibre optic cables were located 5 mm into the start and the end of the movement range and detected the onset of the movement, the duration and end of movement. From this, performance measures of squeeze time and release time for the fatigued hand during exercise were obtained.
Fatiguing exercise
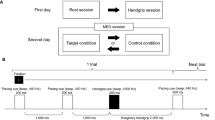
For the fatiguing exercise, the spring resistance in the handgrip of the left hand was set to ∼30% of maximum handgrip force (measured using a hand-held dynamometer; average spring load ∼9 kg). Subjects responded to a text cue (‘squeeze’ or ‘release’; blue font set on a black background and centred in the visual field), which signalled for subjects to squeeze or release the handgrip device and the lever was held in the final position until the next cue was displayed (squeeze 3 s and release 2 s). This cycle was repeated in 3-min blocks until subjects were fatigued (indicated by a doubling of the squeeze time or if the subject could not continue). An investigator remained in the scanner room during functional imaging to provide verbal encouragement and to ensure the exercise was continued throughout the imaging period.
Force decline during exercise was measured on a separate occasion outside of the scanner in a group of seven subjects matched for age, fatigue duration and spring load. Maximal handgrip strength (measured with a hand-held dynamometer) was measured twice before exercise, at 2-min intervals during the fatiguing exercise and once following exercise (at 1-min post-exercise). Measures of maximal force were made for both the left and right hand.
Functional imaging
Subjects lay supine within the bore of a 1.5 T Siemens Sonata scanner, with the head held in a bi-temporal clamp. Functional imaging was performed with a BOLD (Blood Oxygen-Level Dependent) gradient-recalled echo-planar sequence (90° flip angle, TR = 4 s, TE = 66 ms, 34 slices, 3 mm thick, 1 mm gap, 4 × 4 mm2 in-plane resolution, sagittal orientation and whole brain coverage).
During functional imaging subjects performed consecutive 3-min blocks of visually paced fatiguing left hand squeezes, each block consisting of 45 whole brain acquisitions. For each acquisition block, the first two sets were omitted from analysis to allow for the delay in BOLD signal.
Data analysis and statistics
Analysis was performed on three regions of interest (ROI). ROIs were drawn manually on the T1-weighted anatomical image with reference to activation observed during a non-fatiguing handgrip squeeze task performed prior to exercise. For the SM1, the ROI encompassed voxels lying within and around the gyri directly anterior and posterior to the central sulcus. For the premotor cortex, the ROI included the superior and middle frontal gyri immediately anterior to SM1 (Duvernoy 1999). The visual cortex ROI incorporated activated voxels in the gyri immediately superior and inferior to the calcarine fissure at the occipital pole, making up the primary visual cortex. Data from all subjects was corrected for head movement with Siemen’s Prospective Acquisition Correction (PACE) software.
For each subject, the data for the actual duration of the exercise was scaled to a standard 9-min duration, averaged in 30-s blocks and then across subjects. For each hand, a one-way repeated-measure’s ANOVA was performed for each ROI and performance data (squeeze and release time) to test for a significant change in the time course during fatigue (P < 0.05). Pearson’s product moment correlation coefficient was calculated to determine the magnitude of the signal change with fatigue. Measurements of the fMRI signal are presented as a percentage of the first minute of exercise and force as a % of baseline. All data are presented as group mean ± standard error of mean.
Results
The average exercise duration was 9 ± 1.4 min. During the fatiguing exercise maximal handgrip force declined significantly in the left hand to 77 ± 3.6% of baseline (recorded at minute 10, P < 0.05 and r 2 = 0.93). Force did not change significantly from baseline for the right hand (force at minute 10: 100 ± 3% of baseline, P > 0.05, Fig. 1a).

a Maximal force for the left (fatigued—closed diamond) and right (non-fatigued—open diamond) hand during and after unilateral fatiguing exercise. Four force measurements were collected during the 9-min fatiguing exercise (at second, fourth, sixth and eighth-min duration of fatiguing exercise shown as a grey box) and at 1-min post-exercise. Force (as a percentage of maximal force at baseline) declined linearly during exercise for the left hand but not for the right hand (regression line—dashed). b Performance measures collected during fatiguing exercise of the left hand. Squeeze time (open square) and release time (closed square) are shown for every 30 s during the fatiguing exercise (regression line—dashed). There was a significant increase in both measures as fatigue developed
Performance data
Squeeze and release time were collected for the left hand during the fatiguing exercise. Squeeze time was 154 ± 11 ms at baseline and increased to 332 ± 26 ms by the last minute of exercise (P < 0.05, Fig. 1b). There was a substantially greater increase in release time during fatiguing exercise (from 125 ± 10 to 766 ± 19 ms at minute 9 and P < 0.05).
Functional imaging data
The fMRI signal from the SM1 contralateral to the left hand (fatigued hand) increased linearly (r 2 = 0.96 and P < 0.05) by 1.2 ± 0.5% of baseline by the end of exercise (P < 0.05, Fig. 2a). In contrast, the fMRI signal from the ipsilateral SM1 did not change significantly (percentage increase at minute 9: −0.2 ± 0.6% of baseline and P > 0.05) although the data showed a slight and significant downward linear trend (r 2 = 0.42 and P < 0.05).

Functional MR signal collected for the contralateral (filled circle) and ipsilateral hemisphere (open circle) for each region during fatiguing exercise. The fMRI signal (as a percentage of the starting point of exercise; regression line—dashed) increased significantly in SM1 contralateral hemisphere to the fatigued hand (a) and bilaterally in the visual cortex during fatiguing exercise (c). There was no significant change in signal in the other areas measured
The fMRI signal measured in the premotor cortex showed a similar pattern of change to SM1, although this did not reach significance. The fMRI signal from the contralateral premotor cortex increased by 0.25 ± 0.6% of baseline (P > 0.05) and declined in the ipsilateral premotor cortex by −0.24 ± 0.6% of baseline by minute 9 (P > 0.05, Fig. 2b).
There was a significant linear increase in the fMRI signal for the visual cortex contralateral to the left hand during exercise that also extended to the ipsilateral visual cortex (percentage increase at minute 9: contralateral 1.3 ± 0.9%, r 2 = 0.94; ipsilateral 1.5 ± 0.9%, r 2 = 0.89; P < 0.05, Fig. 2c).
Discussion
The fMRI signal measured from the primary SM1 contralateral to the fatiguing hand increased progressively during the fatiguing exercise. The intensity of the fMRI signal increased by ∼1% throughout exercise, which is substantial considering that task-related signal changes with fMRI are normally in the order of ∼3–5%. An increase in SM1 signal during fatiguing exercise may represent an increase in sensory processing and enhanced corticomotor drive to maintain task performance as the exercising muscles fatigue. The increase in SM1 signal was associated with a reduction in maximal force output and a slowing in task performance (as shown by an increase in squeeze and release time). Previous EMG studies have shown that as fatigue develops there is slowing in the relaxation time of single unit twitches (Bigland-Ritchie et al. 1983), which may explain our finding of a greater prolongation of release, than squeeze time during exercise.
Liu et al. (2003) reported an increase in the number of activated pixels in SM1 contralateral to the fatiguing hand during an intermittent submaximal fatigue task. When the submaximal contraction was sustained, pixel number increased over the first half of exercise then plateaued. The increase in signal may represent the recruitment of additional motor neurons during exercise, however towards the end of exercise the plateau in the signal may be associated with the depletion of these reserves and parallel the suboptimal motor drive (central fatigue) reported in transcranial magnetic stimulation studies (Gandevia et al. 1996). When the task was performed intermittently the increase in SM1 activation was less pronounced but more linear than during the sustained task, but still plateaued over the last 2–5 min of the ∼16-min fatiguing exercise. We observed a steady linear increase in signal throughout the exercise period, without a plateau period, possibly because the exercise period was of a shorter duration (∼9 min). Overall, both studies are consistent with the idea of an increase in SM1 activation as fatigue develops, which could represent an increase in the magnitude of the signal (through excitatory or inhibitory pathways) and/or a spread of activation outside the representation of the forearm muscles during exercise.
The fMRI signal in the ipsilateral SM1 declined modestly during fatiguing exercise, although not significantly. Down regulation of blood flow to non-activated brain regions may occur to maintain a stable global cerebral blood flow during periods of greater oxygen consumption in active cortical regions (Jorgensen et al. 1992; Madsen et al. 1993). In this way, the subtle decline in fMRI signal that we measured from the ipsilateral SM1 may be associated with diversion of blood from the non-activated SM1 to supply the greater metabolic demands of the fatigued SM1 during unimanual fatiguing exercise. In contrast to our findings, Liu et al. (2003) reported a bilateral increase in SM1 activation during fatiguing exercise of the right hand. The reasons for this disparity may in some part be related to the difference between fatigue of the dominant and non-dominant hand. Liu et al. also used a block-designed experiment and measured changes in the number of significantly activated voxels during fatigue, and another possibility is that there could have been an increase in the number of activated voxels outside the ROI, without a change in the magnitude of the fMRI signal from the originally activated voxels.
The changes in fMRI signal in the premotor region followed a similar trend to SM1, with an increase contralateral to the fatigued hand and a reduction in the ipsilateral cortex that did not reach significance, although a more complex or demanding fatiguing exercise might produce a significant change in the premotor cortex. Changes in the fMRI signal in motor regions outside of M1 have been previously demonstrated during fatigue (Liu et al. 2003) and highlight the complexity and integration of multiple regions involved in motor control. In particular, changes in the fMRI signal of the premotor cortex may play a role in adapting movement preparation and planning to correlate with fatigue-induced changes within the muscle and may play some role in the central adaptations to fatigue.
Changes in the fMRI signal measured from the visual cortex, have not previously been investigated during fatiguing exercise. We found a bilateral increase in visual cortex signal throughout the exercise, which was of a similar magnitude to the changes in the contralateral SM1 signal. During the fatiguing exercise subjects squeezed the handgrip device in response to a visual cue (a word presented for ∼2 s in the centre visual field). Therefore, some of the increase in visual activation may be related to an increase in attention towards the visual cue as fatigue progressed and movement became more demanding, and which may have influenced visuomotor integration. Alternatively, changes in the fMRI signal from the visual cortex could be associated with changes in neurohaemodynamic coupling associated with the increasing metabolic demand during exercise, which we have previously hypothesised to explain the changes in the fMRI signal in non-motor areas following fatiguing exercise (Benwell et al. 2006b).
The approach used in this study to determine changes in the fMRI signal during fatigue differs from the block-design methods used in previous fatigue studies. Block-design analysis assumes a stable level of activation during each task block and during the intervening rest periods. However, it is unlikely that the fMRI signal will remain stable for any length of time during a fatiguing exercise, therefore we chose to acquire fMRI data continuously and used a regression analysis method to test for changes in signal during fatigue. This is a region of interest approach, rather than an image-generation method. The results are consistent with previous studies but are not dependent on baseline (resting) measures or on assumptions regarding signal stability.
To conclude, we have shown that during the performance of a submaximal fatiguing exercise there is an increase in the fMRI signal measured from the contralateral SM1. An increase in the SM1 signal is in keeping with the notion of an increase in sensory processing and corticomotor drive during fatiguing exercise to maintain task performance as fatigue develops. In parallel, cortical regions outside of the motor network, such as in the visual cortex, also demonstrate an increase in signal. These findings highlight the difficulties in disentangling haemodynamic and neuronal contributions to the fMRI signal, and reflect the contribution from a number of fatigue-related processes such as changes in central motor drive, attention and neurohaemodynamics.
References
Benwell NM, Byrnes ML, Mastaglia FL, Thickbroom GW (2005) Primary sensorimotor cortex activation with task-performance after fatiguing hand exercise. Exp Brain Res 167:160–164
Benwell NM, Mastaglia FL, Thickbroom GW (2006a) Differential changes in long-interval intracortical inhibition and silent period duration during fatiguing exercise. Exp Brain Res 179:255–262
Benwell NM, Mastaglia FL, Thickbroom GW (2006b) Reduced functional activation after fatiguing exercise is not confined to primary motor areas. Exp Brain Res 175:575–583
Benwell NM, Sacco P, Hammond GR, Byrnes ML, Mastaglia FL, Thickbroom GW (2006c) Short-interval cortical inhibition and corticomotor excitability with fatiguing hand exercise: a central adaptation to fatigue? Exp Brain Res 170:191–198
Bigland-Ritchie B, Johansson R, Lippold OC, Smith S, Woods JJ (1983) Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol 340:335–346
Duvernoy HM (1999) The human brain: surface, three-dimensional sectional anatomy with MRI, and blood supply. Springer, New York
Gandevia SC, Allen GM, Butler JE, Taylor JL (1996) Supraspinal factors in human muscle fatigue: evidence for suboptimal output from the motor cortex. J Physiol (Lond) 490:529–536
Gonzalez-Alonso J, Dalsgaard MK, Osada T, Volianitis S, Dawson EA, Yoshiga CC, Secher NH (2004) Brain and central haemodynamics and oxygenation during maximal exercise in humans. J Physiol 557:331–342
Jorgensen LG, Perko G, Secher NH (1992) Regional cerebral artery mean flow velocity and blood flow during dynamic exercise in humans. J Appl Physiol 73:1825–1830
Liu JZ, Dai TH, Sahgal V, Brown RW, Yue GH (2002) Nonlinear cortical modulation of muscle fatigue: a functional MRI study. Brain Res 957:320–329
Liu JZ, Shan ZY, Zhang LD, Sahgal V, Brown RW, Yue GH (2003) Human brain activation during sustained and intermittent submaximal fatigue muscle contractions: an FMRI study. J Neurophysiol 90:300–312
Madsen PL, Sperling BK, Warming T, Schmidt JF, Secher NH, Wildschiodtz G, Holm S, Lassen NA (1993) Middle cerebral artery blood velocity and cerebral blood flow and O2 uptake during dynamic exercise. J Appl Physiol 74:245–250
Sacco P, Thickbroom GW, Thompson ML, Mastaglia FL (1997) Changes in corticomotor excitation and inhibition during prolonged sub-maximal muscle contractions. Muscle Nerve 20:1158–1166
Taylor JL, Butler JE, Allen GM, Gandevia SC (1996) Changes in motor cortical excitability during human muscle fatigue. J Physiol (Lond) 490:519–528
Acknowledgements
We are grateful to Dr Vincent Low (Head) and radiographers at the MRI unit, Department of Radiology, Sir Charles Gairdner Hospital, for their support and assistance in carrying out these studies. Peter Clissa and Peter Proctor from the School of Psychology, University of Western Australia, are thanked for the design and construction of the handgrip device used in this study. This study was supported by the Neuromuscular Foundation of Western Australia. NMB is a recipient of an Australian Post-graduate Award, Jean Rogerson Post-graduate Scholarship and Woodside Neurotrauma Award for 2004.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Benwell, N.M., Mastaglia, F.L. & Thickbroom, G.W. Changes in the functional MR signal in motor and non-motor areas during intermittent fatiguing hand exercise. Exp Brain Res 182, 93–97 (2007). https://doi.org/10.1007/s00221-007-0973-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-007-0973-5