
Abstract
We compared the effect on reaction times of transient interference with function of the dorsal premotor cortex (PMd) using a pair (25-ms interval) of transcranial magnetic stimulation (TMS) pulses with long-term interference produced by a new repetitive TMS paradigm known as “theta burst stimulation” (TBS). Pairs of TMS pulses over left PMd increased choice but not simple reaction times of the right hand if given at the onset of the reaction interval. There was no effect of stimulation over right PMd or at a midline parietal control site (Pz). In contrast, TBS over either left or right PMd increased choice RTs of both hands for at least 5–10 min after the end of TBS. Pairs of TMS pulses over left PMd also increased error rates whereas TBS had no effect on error rates despite the effect on RTs. We suggest that TBS leads to widespread changes in activity and more complex effects on behaviour than expected from the paired pulse TMS and conclude that transient and long-term forms of interference with function may influence behavioural tasks in subtly different ways.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The term “virtual lesion” was introduced by Walsh and Cowey (2000) to describe the temporary interruption of processing that occurs during and after transcranial magnetic stimulation (TMS) of the human brain. In recent years, the technique has been used in two different ways. In the first, a small number of pulses (usually 1–4 pulses) at high frequency (10–50 Hz) have been used to disrupt function for a brief period (approx 50–200 ms) (Day et al. 1989; Priori et al. 1993; Terao et al. 2001; Oliveri et al. 2003). The second method has used repetitive TMS (rTMS) which leads to longer term changes in the underlying cortex that outlast the period of stimulation for several minutes or even hours depending on the parameters of stimulation (Pascual-Leone et al. 1994; Enomoto et al. 2001; Huang et al. 2005). The advantage of the first method is that it can be used to ask questions about when a particular area of brain is active in a task. If the TMS pulse is given to an area of cortex that is active at the time and is processing information relevant to the task, then performance will decline. However, a disadvantage of this design is that the TMS pulse causes a noise and a sensation on the scalp that can itself interfere with the subjects’ attention and indirectly influence the task. Although such effects can be controlled for by additional experiments, some authors have instead used the longer lasting disruption caused by rTMS. The advantage of this is that the effects on processing outlast the stimulation so that the task can be performed in the absence of TMS. The disadvantage is that the timing element is lost.
Although both techniques have been used successfully, there has never been any comparison between their effects; indeed the assumption has been that they are approximately equal. However, this may not be the case. As the effects of rTMS last for a considerable period there is plenty of time available for other areas of the brain to react to, or be influenced by, the disruption. It is also possible that repetitive stimulation will more readily produce activity in complex circuits than a single pulse (Kobayashi and Pascual-Leone 2003). Indeed, functional imaging studies have already shown that rTMS leads to widespread changes in patterns of neural activity at the site of stimulation as well as in connected sites at a distance (Chouinard et al. 2003).
In the present study we have compared the effect of short- and long-lasting “virtual lesions” of the dorsal premotor cortex (PMd) in a choice reaction time task. The experiments were based on the original observations of Schluter et al. (1998, 1999) who used TMS over PMd to investigate its role in selection of movements in a choice reaction time (RT) task. Their data suggested that during the first 100–200 ms after presentation of the choice signal, stimulation over the left PMd had a bilateral influence on choice RTs of either hand, whereas activity in right PMd only had a small effect on RTs of the left hand. Schluter et al. (1998, 1999) used a single high-intensity TMS pulse to interrupt function in PMd. However, we found that this often produced a twitch in contralateral hand muscles, presumably because of spread of the stimulus to the adjacent motor cortex, which made interpretation of the results difficult. To circumvent this, in the present experiments we used two smaller pulses of lower intensity over PMd and compared the effect on response accuracy and RTs with that seen after applying a new rTMS protocol termed “theta burst stimulation” (TBS), which has an effect on cortical excitability that outlasts the stimulation for 30 min (Huang et al. 2005).
Methods
Subjects
Twelve healthy volunteers (four women and eight men; 21–49 years old) participated in this study. All subjects were right handed based on the Edinburgh Handedness Inventory (Oldfield 1971) and they all gave written informed consent for the study. The experimental procedures used were approved by the local Ethics Committee and were carried out in accordance to the Declaration of Helsinki.
RT recording
Electromyographic (EMG) recordings were recorded bilaterally from the first dorsal interosseous (FDI) muscles using 9-mm diameter, Ag–AgCl surface cup electrodes. The active electrode was placed over the muscle belly and the reference electrode over the metacarpophalangeal joint of the index finger. Responses were amplified with a Digitimer D360 amplifier (Digitimer Ltd, Welwyn Garden City, Hertfordshire, UK) through filters set at 20 Hz and 2 kHz with a sampling rate of 5 kHz, then recorded by a computer using SIGNAL software (Cambridge Electronic Devices, Cambridge, UK). We analysed the onset latency of EMG in each trial.
TMS
Two Magstim 200 machines or one Magstim Super Rapid Package (Magstim Co., Whitland, Dyfed, UK) and a small custom-made figure-of-eight-shaped coil (mean diameter 5 cm) were used for the experiments.
The TMS was delivered to one of the three different locations, right or left PMd was regarded as active location; Pz of the international 10–20 system was used as a control site. In all cases, the coil was oriented to induce anteriorly directed current in the brain. First we defined the hand motor area of M1, where stimulation evoked the largest MEP from the contralateral FDI muscle. PMd was defined as being 2.5 cm anterior and 1 cm medial site to that point as recommended in previous reports (Fink et al. 1997; Picard and Strick 2001; Mochizuki et al. 2004). The stimulus intensity was adjusted to be 120% of resting motor threshold (RMT) for the double pulse experiments or 80% of active motor threshold (AMT) for the rTMS experiments. In some subjects, if TMS over PMd at an intensity of 120% RMT evoked small MEPs in the contralateral FDI muscle, we changed the angle of the coil by 10–30° until the MEP was no longer present. We defined RMT as the lowest intensity that evoked five small responses (about 50 μV) in the contralateral FDI muscle in a series of ten stimuli when the subject kept the FDI muscles relaxed in both hands. AMT was the lowest intensity that evoked five small responses (about 200 μV) in a series of 10 stimulations when the subject made a 5% maximal voluntary contraction.
Task (summarised in Fig. 1)
This study involved three experiments. The first experiment examined paired pulse TMS effects in a simple reaction task, the second examined paired pulse TMS effects in a choice reaction task and the third one examined the after effects of TBS in a choice reaction task. During all the experiments, subjects sat relaxed in a comfortable chair holding a 4 cm-diameter block on the table between the thumb and the forefinger of each hand with the FDI muscles relaxed (without any EMG activity). The task consisted of a rapid isometric squeeze of the block as soon as possible after an auditory reaction signal given via a loudspeaker. At the start of each block of trials, the high and low tones were assigned randomly to indicate that subjects had to react with the right or left hand; these instructions were counterbalanced within and across subjects and were written on a paper that was left in front of the subjects throughout each session (“high-right, low-left” or “low-right, high-left”). The order of different experimental blocks was counterbalanced across subjects. Before each test session, at least ten practice trials were given until at least five continuous RTs were within 150% of mean RT.

Experimental paradigms in this study. Experiment 1: first, subjects heard a selective sound (high or low sound) and prepared to contract right or left FDI muscle. Randomly, from 1 to 3 s later, subjects heard GO sound and must contract it as quickly as possible. Experiment 2: first, subjects heard a short warning sound. Randomly, from 1 to 3 s later, subjects heard high or low sound and would contract right or left FDI muscle as quickly as possible. Experiment 3: choice reaction task is same as experiment 2. Two sessions were recorded before (for baseline) and then 5 and 20 min after applying theta burst TMS (TBS)
Experiment 1: simple (fully pre-cued) RT with paired pulse TMS (Fig. 1a)
Ten subjects [three women and seven men; 33±8 years old (mean ± SD)] participated in this experiment. In each trial, subjects first heard a high (1,000 Hz, 80 ms) or a low (100 Hz, 80 ms) frequency warning tone (randomly presented) that indicated which hand was to be used to react in that trial according to the instructions printed on the paper before them. Randomly, from 1 to 3 s later, a GO sound (500 Hz, 40 ms) signalled subjects to contract the hand as quickly as possible. The inter-trial interval was 6 s.
Pairs of TMS pulses at an intensity of 120% RMT were given with an interstimulus interval of 25 ms. The first stimulus of the pair was delivered at −150 or −50 ms before or 50 ms after the onset of the GO sound. A block of trials consisted of eight conditions (one control without TMS and three different timings of TMS for right and left FDI muscles) with each condition repeated 10–20 times (i.e. a total of 80–160 trials). In addition we included about 15% random catch trials in which TMS was applied but no GO sound was given. These ensured that subjects reacted to the GO sound rather than the TMS pulses. If the subject inadvertently responded in any of the catch trials, all the responses between the previous and next catch trials were discarded. TMS was applied at only one location in each block: over either the left or right PMd (at 120% RMT) or over Pz (control site, at 130% RMT to give a similar scalp sensation).
Experiment 2: choice RT and paired pulse TMS (Fig. 1b)
Ten subjects (three women and seven men; 32±8 years old) participated in this experiment. Each trial began with an auditory warning (500 Hz, 40 ms). The reaction signal was given randomly 1–3 s later and consisted of either a high (1,000 Hz, 80 ms) or low (100 Hz, 80 ms) frequency tone pulse that indicated which hand to contract according to the instructions written on the paper in front of the subjects. The inter-trial interval was 6 s.
The first of the pair of TMS pulses was given over right or left PMd at 100, 150, 200 or 250 ms after the onset of the reaction signal. We did not apply TMS at 0 and 50 ms because this caused some subjects to confuse the frequency of the reaction tone. In two subjects whose expected RT was more than 340 ms, TMS pulses were also applied at 300 ms. As in experiment 1, the control site was Pz. Each block of trials had 10 or 12 conditions (one control without TMS and four or five different timings of TMS for right and left FDI muscles) repeated 10–20 times.
For the purposes of analysis the data were regrouped according to the interval between the onset of the TMS pulses and the mean RT in the control condition without TMS (control RT). Thus, if the subjects had a control RT of 300 ms, TMS pulses at 200 ms after the reaction signal occurred 100 ms before the expected time of reaction (i.e. −100 ms). Finally, these adjusted TMS timings were binned into 50 ms-bins (the −50 ms bin contained timings from −40 to −89 ms; −100 ms from −90 to −139 ms; −150 from −140 to −189 ms).
Experiment 3: TBS and choice RT (Fig. 1c)
Nine subjects (two women and seven men; 33±8 years old) participated in this experiment. The task was the same as in experiment 2. However, in this case, no TMS was given during the reaction session. Instead, RTs were measured before and then 5 min and 20 min after applying theta burst TMS over PMd at an intensity of 80% AMT. Theta burst TMS consisted of a three-pulse burst at 50 Hz repeated every 200 ms for 20 s (equivalent to “continuous theta burst stimulation, cTBS” in Huang et al. 2005). In each case, choice RTs were measured in two blocks of trials. In one of them (at random), the high tone indicated movement of the right hand whereas in the other it indicated movement of the left hand, and vice versa for the low tone. Each block consisted of 10–15 trials of each of the two conditions. TBS was applied over the Pz control site using 90% AMT. Each TBS experiment was performed on separate days.
Data analysis
First, comparisons of control simple or choice RT were performed with two factor analysis of variance (ANOVA) (main factors of high- or low-frequency TONE and left or right HAND) using the ratio (RT of each condition)/(mean RT of four conditions) in order to normalise data from each subject (and reduce intersubject variability). Next, all RTs with TMS were normalised to the control RT (experiments 1 and 2) or baseline before TBS (experiment 3) and expressed as a percentage change. In these experiments a three factor ANOVA (main factors of TMS site [left/right PMd and Pz (control)], left/right HAND, and TIME) was used to assess the effects on RT and a two factor ANOVA (main factors of TMS site and TIME) was used for accuracy measures. If an ANOVA showed significant main effects, we performed post hoc analyses with Scheffe’s method. The statistical significance was set at P=0.05.
Results
No subject noted any adverse effect during or after the experiments.
Comparison of control simple and choice RTs
Table 1 summarises the control RTs in the simple and choice reaction time tasks for the left and right hands and for the high and low reaction tones. As expected, the simple RTs were shorter than the choice RTs (global mean RTs: simple, 186±47 ms; choice, 266±42 ms). Interestingly, the right hand RTs were slightly faster than the left RTs in the choice but not the simple reaction task (two factor ANOVA on choice RT with HAND and TONE as main factors: main effect of HAND (F(1,32)=18.7, P<0.001)).
Simple RT with pairs of TMS pulses over left or right PMd or Pz
The results of experiment 1 are shown in Fig. 2. A three factor ANOVA with HAND (right, left), TIME and SITE (of TMS pulses) showed an effect of TIME but no other significant main or interaction effects (TIME, F(2,162)=7.45, P=0.001). Post hoc analysis showed that the RT at −50 ms was significantly longer than that at 50 ms (P=0.001). The accuracies of all sessions were almost 100% (always more than 97%; not illustrated).

Paired pulse TMS effects on simple reaction time (RT) in right (a) or left (b) FDI muscle. There was no significant TMS site effect, but RT at −50 ms was significantly longer than that at 50 ms. Error bars indicate standard errors
Choice RT with pairs of TMS pulses over left or right PMd or Pz
Results of one session of a subject when TMS were applied over left PMd are shown in Fig.3. In this subject since the average control RT was 306 ms on the right and 326 ms on the left, a TMS pulse that occurred 250 ms after the reaction tone was regarded as being −50 ms before the expected time of reaction etc. (see Methods). The RTs of right hand with TMS at −50 and −100 ms were delayed by more than 10% of the control RT (Fig. 3a). There was no obvious change in the distribution of the reaction times even though TMS at 200 ms prolonged mean RT by about 50 ms. The RTs of the left hand in trials with TMS were slightly shorter than control RT without TMS (Fig. 3b).

The distributions of choice reaction time (RT) of a subject when TMS was applied over left PMd. In right FDI muscle reaction (a), RTs with TMS at 200 and 250 ms were delayed more than 10% from control RT. In left FDI muscle reaction (b), there were no delay effects. Filled triangles indicate average values. Five vertical lines of each row indicate 10, 25, 50, 75 and 90% value of RT data. So, each box indicates 50% of RT data (from 25 to 75%)
The results of experiment 2 are shown for all subjects in Fig. 4. A three factor ANOVA revealed two significant interaction terms involving TMS×HAND (F(2,162)=3.96, P=0.02) and TMS×TIME (F(4,162)=2.60, P=0.04). In order to investigate these in further detail we performed separate two factor ANOVAs on the data from each HAND separately. These showed a significant TIME×TMS interaction for the right HAND (F(4,81)=2.44, P=0.05) which was due to the fact that stimulation over left PM cortex increased RT at −100 ms. The ANOVA on the data from the left HAND showed only a main effect of TIME but no interactions. The latter was due to the gradual decrease of choice RTs at longer intervals when compared with control RTs (Fig. 4b). Note also that the RTs of the Pz control site tended to be shorter than control (under 0%) at all time points: we presume this was caused by the phenomenon of intersensory facilitation (Nickerson 1973; Terao et al. 1997) due to the sound and sensation of the TMS coil on the head.

Paired pulse TMS effects on choice reaction time (RT) in right (a) or left (b) FDI muscle and accuracy (c). When TMS was delivered to left PMd, there were significant RT delays in right FDI muscle than those of the others. The accuracy of TMS over left PMd was lower than that observed after TMS over right PMd or stimulation over the Pz control site. Error bars indicate standard errors
Two factor ANOVA for performance accuracy (Fig. 4c) showed only a significant main effect of TMS site (TMS, F(2,108)=4.30, P=0.02). Post hoc analyses showed that the accuracy of TMS over left PMd was lower than that observed after TMS over right PMd (P=0.04) or Pz stimulation (P=0.04).
Choice RT before and after TBS over left or right PMd or Pz
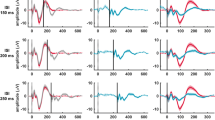
The results of experiment 3 are shown in Fig. 5. The only significant interaction term in the three factor ANOVA involved TMS×TIME (F(4,144)=9.86, P<0.001). There were no interactions or a main effect involving HAND, indicating that the reaction times in both hands were affected similarly. In a subsequent analysis we therefore averaged the data from both hands for a two factor ANOVA that revealed a highly significant TMS×TIME interaction (F(4,72)=10.35, P<0.001). Post hoc analyses showed that TBS over right and left PMds had larger delaying effects on RT than stimulation over the Pz control site at 5 min after TBS (right PMd, P<0.001; left PMd, P<0.001), and that the effect of TBS over left PMd was larger than that over right PMd (P=0.02). Two factor ANOVA for performance accuracy (Fig. 5c) showed no significant main effects or interactions.

Theta burst TMS (TBS) effects on choice reaction time (RT) in right (a) or left (b) FDI muscle and accuracy (c). TBS over right and left PMds increased choice RT significantly more than Pz stimulation at 5 min after TBS; the effect of left PMd was greater than that of right side. There were no significant main effects of TMS or TIME on accuracy. Error bars indicate standard errors
Discussion
The results show that RTs in a choice reaction task are affected less by a short-lasting “virtual lesion” over PMd with a pair of TMS pulses than they are during the long-lasting “virtual lesion” produced by theta burst conditioning. The short-lasting pair of TMS pulses increased RTs in the right hand if given over the left PMd during the reaction period of the choice task, but there was no effect if the pulses were given over the right PMd. In contrast, TBS of either hemisphere led to significant increases in RT of both hands that lasted for at least 5–10 min after the end of stimulation. The effect of TBS over left PMd was marginally larger than the effect of TBS over right PMd. The conclusion is that the two types of “virtual lesion” approach do not necessarily lead to similar conclusions about function. We speculate that it may be possible to generalise these conclusions into other situations. That is, long-lasting effects produced by repetitive TMS paradigms (such as the TBS paradigm) are likely to lead to more widespread effects on function than the short-lasting interference produced by a smaller number of pulses given during a reaction period. As we argue below, neither effect should be regarded as superior.
Comparison of the effect of a transient “virtual lesion” with previous results
Although our experimental paradigm was based on that of Schluter et al. (1998), it differed in that movement choices were indicated by the frequency of an auditory signal rather than by a visual cue. However, both types of cue are known to evoke activity in the PMd in a conditional motor task in monkeys (Vaadia et al. 1986) or in human beings (Iacoboni et al. 1998), so that they can both be considered as reasonable tests of premotor involvement in movement preparation. We also used a pair of smaller intensity TMS pulses rather than a single large pulse to interfere with function. This had the advantage that it reduced stimulus spread to motor cortex and never evoked any muscle twitches during the experiments in any subject that might have interfered with the interpretation of the data. Despite these differences, our results were consistent with the hypothesis of Schluter et al. (1998, 1999) that the left PMd plays a greater part in selecting movements in a choice RT involving either hand than the right PMd. In addition we confirmed that stimulation over PMd had no effect on simple RTs, as expected since these movements are fully pre-cued and therefore require no on-line selection of movement parameters during the reaction period.
In the experiments of Schluter et al. (1998, 1999) subjects had too few incorrect responses to allow analysis of error rates. However, in our choice RT experiments we found that pairs of TMS pulses led to a small but significant increase in error rate in trials with TMS over left PMd. In any choice reaction task there is a trade off between error rate and response latency, with faster responses being more likely to contain errors than slower ones (Mulert et al. 2003). The fact that TMS increases error rates as well as delaying response latency suggests that the stimulus not only delays neural processing but also introduces noise into the decision-making process that reduces mean accuracy.
Comparison of short- and long-term “virtual lesions”
In some ways it is surprising that TBS had a more widespread effect on RTs than the pair of TMS pulses. The pair of pulses was applied at almost twice the intensity of TBS (120% RMT vs 80% AMT) and would have activated a much larger population of neurones in PMd as well as projection fibres to and from that area. However, this disadvantage in terms of numbers of neurones activated may have been offset by two aspects of TBS. First, the stimulation frequency of TBS was much higher than for the double pulse TMS, and this would have had a much more powerful influence on the activity of the smaller population of neurones stimulated during TBS. Second, even though the low intensity of pulses used in TBS would have been unlikely to produce direct activation of output projections, they might nevertheless lead to changes in the ongoing activity of connections to or from PMd and secondarily influence activity in many distant areas of cortex. If any of these areas was providing background facilitation of task performance, then a reduction in their contribution would make behavioural performance much more sensitive to disruption of processing in PMd.
If this is the case, then short-lasting disruption of function, as with the double pulse protocol used in the present experiments, is more likely to give information on when the function of a cortical area is essential for a behavioural task. Long-lasting disruption, as after TBS, is more likely to give an insight into the changes that might occur after injury to an area of cortex: disruption of tonic connections to other regions would lead to widespread changes in activity (Kobayashi and Pascual-Leone 2003; Chouinard et al. 2003) and more complex effects on behaviour than expected from the short-lasting “lesion” approach.
It is interesting to note that in contrast to the short-lasting disruption produced by a pair of TMS pulses, TBS did not cause any increase in subjects’ error rates. As suggested above, an increase in error rates may well reflect the fact that the double pulse TMS introduces noise into the decision signal that is used to trigger movement. If so, then it is possible to imagine that TBS increases RT without an increase of neural noise. Alternatively, it may be that after TBS, subjects have time to adjust for increased neural noise and compensate by increasing the level of the signal that is needed to trigger a movement. Effectively, the decision process would be made less subject to error by waiting longer for more information before initiating a voluntary reaction movement.
Conclusion
The short-lasting pair of TMS pulses increased RTs in the right hand if given over the left PMd during the reaction period of the choice task, but there was no effect if the pulses were given over the right PMd. In contrast, TBS of either hemisphere led to significant increases in RT of both hands. We suggest that TBS leads to widespread changes in activity and more complex effects on behaviour than expected from the short-lasting “lesion” approach. Pairs of TMS pulses over left PMd also increased error rates whereas TBS had no effect on error rates despite the effect on RTs. Thus transient and long-term interference with function may lead to different conclusions about the role of cortical areas in behavioural tasks.
References
Chouinard PA, van der Werf YD, Leonard G, Paus T (2003) Modulating neural networks with transcranial magnetic stimulation applied over the dorsal premotor and primary motor cortices. J Neurophysiol 90:1071–1083
Day BL, Rothwell JC, Thompson PD, de Noordhout AM, Nakashima K, Shannon K, Marsden CD (1989) Delay in the execution of voluntary movement by electrical or magnetic brain stimulation in intact man. Brain 112:649–663
Enomoto H, Ugawa Y, Hanajima R, Yuasa Y, Mochizuki H, Terao Y, Shiio Y, Furubayashi T, Iwata NK, Kanazawa I (2001) Decreased sensory cortical excitability after 1 Hz rTMS over the ipsilateral primary motor cortex. Clin Neurophysiol 112:2154–2158
Fink GR, Frackowiak RSJ, Pietrzyk U, Passingham RE (1997) Multiple nonprimary motor areas in the human cortex. J Neurophysiol 77:2164–2174
Huang YZ, Edwards MJ, Runis E, Bhatia KP, Rothwell JC (2005) Theta burst stimulation of the human motor cortex. Neuron 45:201–206
Iacoboni M, Woods RP, Mazziotta JC (1998) Bimodal (auditory and visual) left frontoparietal circuitry for sensorimotor integration and sensorimotor learning. Brain 121:2135–2143
Kobayashi M, Pascual-Leone A (2003) Transcranial magnetic stimulation in neurology. Lancet Neurol 2:145–156
Mochizuki H, Huang YZ, Rothwell JC (2004) Interhemispheric interaction between human dorsal premotor and contralateral primary motor cortex. J Physiol 561:331–338
Mulert C, Gallinat J, Dorn H, Herrmann WM, Winterer G (2003) The relationship between reaction time, error rate and anterior cingulate cortex activity. Int J Psychophysiol 47:175–183
Nickerson RS (1973) Intersensory facilitation of reaction time: energy summation or preparation enhancement? Psychol Rev 80:489–509
Oldfield RC (1971) The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9:97–113
Oliveri M, Babiloni C, Filippi MM, Caltagirone C, Babiloni F, Cicinelli P, Traversa R, Palmieri MG, Rossini PM (2003) Influence of the supplementary motor area on primary motor cortex excitability during movements triggered by neutral or emotionally unpleasant visual cues. Exp Brain Res 149:214–221
Pascual-Leone A, Valls-Sole J, Brasil-Neto JP, Cammarota A, Grafman J, Hallett M (1994) Akinesia in Parkinson’s disease. II. Effects of subthreshold repetitive transcranial motor cortex stimulation. Neurology 44:892–898
Picard N, Strick PL (2001) Imaging the premotor areas. Curr Opin Neurobiol 11:663–672
Priori A, Bertolasi L, Rothwell JC, Day BL, Marsden CD (1993) Some saccadic eye movements can be delayed by transcranial magnetic stimulation of the cerebral cortex in man. Brain 116:355–367
Schluter ND, Ruthworth MFS, Passingham RE, Mills KR (1998) Temporary interference in human lateral premotor cortex suggests dominance for the selection of movements. A study using transcranial magnetic stimulation. Brain 121:785–799
Schluter ND, Rushworth MFS, Mills KR, Passingham RE (1999) Signal-, set-, and movement-related activity in the human premotor cortex. Neuropsychologia 37:233–243
Terao Y, Ugawa Y, Suzuki M, Sakai K, Hanajima R, Gemba-Shimizu K, Kanazawa I (1997) Shortening of simple reaction time by peripheral electrical and submotor-threshold magnetic cortical stimulation. Exp Brain Res 115:541–545
Terao Y, Ugawa Y, Enomoto H, Furubayashi T, Shiio Y, Machii K, Hanajima R, Nishikawa M, Iwata NK, Saito Y, Kanazawa I (2001) Hemispheric lateralization in the cortical motor preparation for human vocalization. J Neurosci 21:1600–1609
Vaadia E, Benson DA, Hienz RD, Goldstein MH Jr (1986) Unit study of monkey frontal cortex: active localization of auditory and of visual stimuli. J Neurophysiol 56:934–952
Walsh V, Cowey A (2000) Transcranial magnetic stimulation and cognitive neuroscience. Nat Rev Neurosci 1:73–79
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mochizuki, H., Franca, M., Huang, YZ. et al. The role of dorsal premotor area in reaction task: comparing the “virtual lesion” effect of paired pulse or theta burst transcranial magnetic stimulation. Exp Brain Res 167, 414–421 (2005). https://doi.org/10.1007/s00221-005-0047-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-005-0047-5