
Abstract
After injuries to the anterior cruciate ligament (ACL) a functional instability is frequently observed which has been attributed to a disturbed sensorimotor function. In light of the clinical importance of ACL injuries and the resulting functional instability, it is of enormous clinical interest to elucidate the role of sensorimotor pathways that involve the ACL. In animals and humans a direct reflex pathway between the ACL and the hamstrings has been shown. The onset latencies of responses reported after ventral tibia translation were around 40–50 ms (range 17.9–65) and were regarded as medium latency responses (MLR). However, ventral tibia translation should also induce a stretch of the hamstring muscles and evoke a short latency response (SLR). Before any muscle response after ventral tibia translation can be ascribed to anatomical structures, it is crucial to analyze the obtained muscle responses carefully. The aim of the present study was the development of an algorithm to differentiate SLR and MLR responses after ventral tibia translation. In ten healthy subjects reflex responses of the hamstrings after anterior tibia translation and after tendon taps on the biceps femoris tendon were evaluated. To investigate the influence of skin afferents, control experiments were performed after lidocain injection of the dorsal calf. The mean onset latency of the tendon jerk reflex was 21.9±3.1 ms (range 17.3–28.7 ms). Both SLR responses (mean onset latency: 20.3±3.5 ms; range 15.4–25.8) and MLR responses (mean onset latency: 38.9±4.2 ms; range 32.9–46.7) were obtained in all subjects. Skin afferents from the calf do not play a major role. The development of an evaluation algorithm is presented that allows a safe differentiation between these partly superimposed SLR and MLR components. It is demonstrated that by measuring the first part of the SLR from the onset to the first peak the end of the SLR can be predicted and that the onset latency of the MLR component can be assessed reliably. Possible reasons are discussed why previous studies only reported responses at MLR latencies. The fact that both SLR and MLR components can be observed after anterior tibia translation underlines the necessity to differentiate the responses before they can be ascribed to any anatomical structures. As a basis for future work the algorithm presented may become a useful tool to differentiate which afferent pathways play a role in initiating hamstring activity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Instability of the knee joint causes meniscal and chondral lesions which often require costly therapy. After injuries of the anterior cruciate ligament (ACL) a functional instability is frequently observed apart from a mechanical instability. This functional instability has been attributed to a disturbed sensorimotor function (Friden et al. 2001; Reider et al. 2003). Clinically it is characterized by a giving-way pathology, despite sufficient mechanical stability after reconstruction of the ACL. Beard et al. (1993) suggested that an altered reflex response of the hamstrings which are synergists of the ACL (More et al. 1993; Durselen et al. 1995; Imran and O’Connor 1998) may play an important role.
In animal and human studies a direct reflex pathway between the ACL and the hamstrings was shown (Gruber et al. 1986; Solomonow et al. 1987; Miyatsu et al. 1993; Dyhre-Poulsen and Krogsgaard 2000; Fujita et al. 2000; Krogsgaard et al. 2002). Histological studies identified numerous sensorimotor receptors such as Ruffini’s corpuscles, pacinian corpuscles, Golgi’s tendon organs and free nerve endings in the ACL and other ligamental structures of the knee joint (Freeman and Wyke 1967; Schultz et al. 1984; Zimny et al. 1986; Schutte et al. 1987; Sjolander et al. 1989; Haus and Halata 1990; Biedert et al. 1992; Haus et al. 1992; Raunest et al. 1998). Additionally the muscle spindles as well as the Golgi tendon organs play an essential role in the reflex responses of the knee joint (Solomonow and Krogsgaard 2001). On account of the different muscles which insert at the knee and the various receptors of the knee joint, a complex muscle response to a mechanically induced anterior tibia translation can be expected. Different studies have reported multiphasic muscle responses at the ankle joint. Depending on their latency they were classified as short latency response (SLR), medium latency response (MLR) and long latency response (LLR) (Dietz et al. 1980; Dietz and Berger 1982; Diener et al. 1984; Toft et al. 1989; Grey et al. 2001). The SLR and MLR responses in the M. soleus are superimposed. A clear differentiation between SLR and MLR is only possible in the more distal M. flexor digitorum brevis in taller subjects (Schieppati et al. 1995; Nardone et al. 1996).
Data of reflex responses of the hamstrings induced by ventral tibia translation are rare. Using similar methods, Beard et al. (1993, 1994c) and Jennings and Seedhom (1994) reported mean onset latencies of 49 and 41 ms, respectively. They suggested that the muscle responses are evoked by stimulation of the ACL and named it reflex hamstrings contraction latency without describing a polyphasic shape of the response. Bruhn (1999) reported mean latencies of 58–65 ms. Regarding the range of latencies, the question arises whether these responses correspond to SLR or MLR or simply to a mixture of both which has not been analyzed thoroughly in these previous studies. Before these responses can be assigned to ligamental structures of the knee joint such as the ACL it is crucial to thoroughly analyze the reflex response patterns in order to differentiate SLR and MLR, which helps to identify possible reflex pathways that mediate the complex response. The first part of this response may be influenced by the hamstring stretch reflex which occurs at latencies of 18–24 ms (Faist et al. 1999). Therefore, the aim of the present study was to develop an evaluation algorithm to differentiate and to quantify the hamstring reflex responses after anterior tibia translation.
Materials and methods
We investigated ten subjects (five male, five female, mean age ± SD: 22±3 years, range 19–25) with no history of orthopedic or neurological disease. The study was approved by the ethics committee of the University of Ulm (No. 77/2002) and all subjects gave written informed consent.
General experimental arrangement
The experimental setting was modified following the method reported by Beard et al. (1993). The subjects were standing upright with 30° knee flexion and 5° outer rotation of the feet. The thigh was blocked in ventral direction above the patella, which was pressed against a counter pressure plate. An accelerated piston driven by a pneumatic cylinder (Festo, Ulm, Germany), generated a force of 300 N in an posterior-anterior direction 10 cm below the knee joint gap parallel to the tibia plateau in an angle position of 30° (Fig. 1). The tibia translation was recorded by a potentiometric position transducer (stroke length: 0–30 mm; independent linearity ±0.25 to ±0.075%, repeatability 0.002 mm; Novotechnik, Ostfildern, Germany) applied to the tuberositas tibiae. This position system allowed for the assessment of the actual onset of the tibia translation and was used as a trigger for the calculation of latencies. In each subject 50 trials were performed on the left leg. One trial consisted of six consecutive single measurements, which were averaged off-line. A break of approximately 5 s was interspersed between the individual trials. Thus, 300 measurements were performed for each subject. By averaging six measurements to one trial, the variability of single measurements was eliminated. On the other hand, a number of 50 trials still allowed to identify different patterns of responses (see evaluation algorithm below). By visual control only trials with exactly superimposed trigger signals (sampling rate 5,000 Hz) were evaluated. The onset (SLR, MLR) was set manually for each trial using the criteria of the evaluation algorithm described below.

Experimental setup: the subjects were standing upright with 30° knee flexion and 5° outer rotation of the feet. The thigh was blocked in ventral direction above the patella, which was pressed against a counter pressure plate (1). The tibia translation was recorded by a position transducer motion sensor applied to the tuberositas tibiae (2). An accelerated piston (3) driven by a pneumatic cylinder (4) generated a force of 300 N in an posterior-anterior direction 10 cm below the knee joint gap parallel to the tibia plateau in an knee angle position of 30°
Pilot studies and additional experiments
In a pilot study with ten subjects we assessed the minimum translation velocity of the tibia in relation to the femur required to obtain a reproducible reflex response of the hamstrings. We found that the minimum velocity required to obtain a reliable reflex response in all subjects was 0.03 m/s. In a second set of experiments the force was varied from 50 to 300 N in seven steps by approximately 40 N to examine the effect on the EMG configuration and latencies. We found an increase of the amplitude with increasing force but no further systematic effect on the signal configuration or on the latencies. While for 50 N no reliable response could be obtained, for 90 N eight out of ten subjects showed a clear SLR and for more than 140 N a response was observed in all subjects. SLR latencies did not vary significantly between any of the six forces tested above 50 N (e.g., 19.4±3.8 ms for 90 N, 21.2±5.3 ms for 180 N, and 19.9±3.7 ms for 300 N; p =0.857; ANOVA). To obtain reproducible responses, a force of 300 N was chosen for the main study.
To investigate the influence of cutaneous afferents on the reflex response in five subjects, the skin of the dorsal calf was anesthetized by lidocaine injection. The efficiency of the anesthesia was assessed clinically by a painful stimulus to the skin using a needle. Other groups used acceleration sensors to trigger the EMG signal (Beard et al. 1993, 1994b; Jennings and Seedhom 1994). As we used a position transducer, we performed additional experiments in three subjects where we used both a position transducer and an acceleration sensor in parallel.
Tendon jerk reflex
In each subject the tendon jerk reflex as a mainly monosynaptic reflex (Burke et al. 1984) was evoked in the lateral and the medial hamstrings on the left leg with a reflex hammer. The reflex hammer was connected to an acceleration sensor (10 G, Biovision, Weilheim, Germany) to assess the latency of the tendon jerk reflex after the impact of the hammer. The subjects were tested in the same standing position as during the tibia translation experiment. A position transducer was used to check that in all subjects no tibial motion occurred. In three subjects additional experiments were performed using the Achilles tendon jerk reflex in the M. soleus in a prone position.
Electromyography
The surface EMG was recorded with pairs of disk electrodes (Arbo Ag/AgCl-Sensor, Tyco Healthcare, Neustadt, Germany, diameter 0.5 cm, distance 2 cm) placed above the muscle bulge of the medial and lateral hamstrings in the middle between knee joint gap and buttocks gap. Additionally, the m. vastus medialis was recorded 2–3 cm medially and 5 cm proximally from the upper patella rim. The reference electrode was placed on the malleolus medialis. The skin was shaved and grease was removed with alcohol (Basmajian and De Luca 1985). EMG signals were amplified and recorded at a sampling rate of 5,000 Hz. Raw data were taken without frequency filter and EMG analysis was performed with a measuring and evaluation software (Daisy Lab Biovision, Weilheim, Germany). For further analysis the EMG signals were rectified, averaged and a 10 Hz high pass filter (type: Butterworth; order: 6) was used.
Evaluation algorithm to differentiate SLR and MLR after tibia translation
Reflex pathways of the hamstrings are shorter than those of the ankle joint muscles and therefore the difference between the onset latency of SLR and MLR is smaller. To differentiate the superimposed responses, it is crucial to determine the end of the SLR part. Even at the ankle joint muscles with its longer reflex pathways this end of the SLR is not always recognizable reliably in the complex reflex response with a subsequent MLR (Grey et al. 2001). The reflex pathway of the SLR corresponds to the tendon jerk reflex arc. Therefore, as the first step, the hamstring tendon jerk reflex was analyzed in each subject in a separate experiment as described above. A typical EMG is shown in Fig. 2 with a biphasic reflex response. This was divided into three parts: i) from the first onset to the first peak (B); ii) the peak to peak (PP); and iii) from the second peak to the end (E). The duration of each of these three sections was determined. It is important to note that the onset latencies and the first peak latencies of the tendon jerk reflex (see part B in Fig. 2) are very similar to the corresponding latencies of the first part of the SLR component after tibia translation (Fig. 3). This first part of the SLR is not yet contaminated by the MLR. Therefore, it was checked whether the analysis of the first part (B) in the tendon jerk reflex was sufficient to predict reliably the end of the tendon jerk reflex. Assuming corresponding reflex pathways of the tendon jerk reflex and the SLR component, this would allow to predict the end of the SLR within the complex muscle response after tibia translation. In the tendon jerk reflexes a constant relation can be shown between the first part (see Fig. 2, B) and the remaining parts (see Fig. 2, PP and E). This constant relation allows for the assessment of the duration of the tendon jerk reflex by just measuring the first part (see Results).

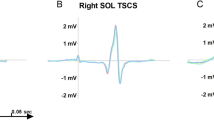
The tendon jerk reflex signal was subdivided into three sections: section ( B) of the signal until the first amplitude (B), the second from the first to the second amplitude ( PP) and the third section from the second amplitude until the end of the signal ( E). The duration of each of these three sections was determined. One single EMG response is shown. First row: rectified signal of medial hamstring. Second row: raw signal from medial hamstring

Signal configurations: group S: only SLR; group M: only MLR; group Sm: SLR higher than MLR (ratio: highest amplitude SLR/MLR>1.1); group sM: SLR smaller than MLR (ratio<0.9); group SM: SLR=MLR (ratio 0.9–1.1). First row: rectified signal of the medial hamstring. Second row: raw signal of the medial hamstring. Third row: trigger signal from the tibia. Fourth row: tibia translation
The more complex EMG response after tibia translation shows basically three different patterns: either peaks only at the SLR latency (group S) or at the MLR latency (group M) or most frequently a combination of both (group SM). If the amplitudes of the SLR and MLR responses are considered, group SM may be subdivided into three patterns: group Sm, i.e., SLR higher than MLR (ratio: highest amplitude SLR/MLR>1.1); group sM, i.e., SLR smaller than MLR (ratio<0.9); group SM: SLR = MLR (ratio 0.9–1.1) (Fig. 3). Each pattern may occur within the same subject. Each of the 50 trials obtained was classified and the distribution within the subjects is shown in Table 1. A reliable evaluation algorithm to differentiate the partly superimposed SLR and MLR responses should lead to constant latencies for each component irrespective of the ratio between SLR and MLR. The responses where only peaks at the SLR latency occurred (group S) were used to check whether assessing the duration from onset of the EMG response to the first peak and then calculating the end of the response was reliable to assess the duration of the SLR.
As a further criterion for the differentiation of SLR and MLR, the duration of section PP in the tendon jerk reflex was used. EMG peaks occurring later than the maximum duration of the PP were classified as MLR (see Fig. 2). In case the first peak of the MLR was on the descent of the SLR, the onset of the MLR was set at the turning point.
Statistical analysis
For statistical analysis SPSS® Software was used. After calculating the mean latencies for each subject group means, standard deviations, range, and the 95% confidence intervals were calculated. Significance levels for differences between means were assessed with Student’s t -test or the ANOVA procedure where appropriate. A p value <0.05 was considered significant.
Results
Tendon jerk reflexes
The onset of the tendon jerk reflex showed a mean latency of 21.9±3.1 ms (range 17–28 ms). In none of the tendon jerk reflex measurements were responses with an onset latency compatible with MLRs, i.e., longer than 30 ms, observed. There was no significant difference between the lateral and the medial hamstrings (lateral: 21.3±3 ms, medial 22.5±3.4 ms) or between the female and male subjects (women: 20.5±2.5 ms, men: 23.0±3.1 ms). The slightly shorter mean latency in female subjects may be due to the difference in height and thus leg length (height ± SD: female 164.3±3.3 cm, male 186±3.3 cm). All further mean values reported in this paper concerning the tendon jerk reflex showed no significant differences regarding the investigated side or gender. The overall duration of the tendon jerk reflex EMG response (section B, PP and E; see Fig. 2) was 15.7±4.5 ms (mean ± SD, range 9.9–22.6 ms).
The duration of the sections PP and E was expressed as a ratio of section B. For section B we found a mean ± SD duration of 4.8±1.3 ms; for section PP, 5.8±2 ms; and for section E, 5.0±1.7 ms. The duration of interval PP was significantly longer compared with B and E ( p <0.001). The mean ratio (± SD) PP/B was 1.24 (±0.34; range 0.67–1.68), the mean ratio (± SD) E/B was 1.04 (±0.2; range: 0.75–1.42). Thus, the mean factor to calculate the end of the tendon jerk reflex using the duration of section B is 3.28 (range 2.42–4.1). First we checked whether this factor of 3.28 can actually predict reliably the measured individual duration of each single tendon jerk reflex. The calculated values using simply this mean factor of 3.28 were compared to the measured individual duration of the tendon jerk reflexes. To determine the most reliable value for reflex duration time, we evaluated both the study group mean value (= mean of measured individual duration of all subjects, n =10) and the calculated value, which were expressed as a percentage of the measured individual duration. The calculated value for duration time showed a mean (± SD) percentage of 101% (±16%), and for study group a mean value of 108% (±31%). The 95% confidence interval of the calculated values was 89–114%, and of the study group mean values 84–132%. The calculated values ranged from 82 to 129%, and the study group mean values from 69 to 158%. Thus, the calculated value using simply the duration of section B and the mean factor of 3.28 was closer to the actually measured tendon jerk reflex duration of the individual subject than the group mean duration. In three subjects this method was also checked with the Achilles tendon jerk reflex. The mean factor to calculate the end of the reflex was 3.24 (subject 1:3.45±0.56, subject 2:3.14±0.34, subject 3:3.10±0.32; 45 reflexes analyzed per subject). The calculated value for duration time showed a mean (± SD) percentage of 101% (±5%), and for study group a mean value of 104% (±18%).
Reflex response after tibia translation
The mean anterior tibia translation was 3.2±0.8 mm (range 2.2–4.6 mm). The mean tibia velocity was 0.057 m/s (range 0.05–0.07) which is distinctly above the threshold value of 0.03 m/s necessary to evoke a reliable response in all subjects (see Methods). In the complex muscle response after tibia translation, the onset of the MLR is superimposed by the end of the SLR (see Fig. 3). Therefore, it is necessary to determine the end of the SLR within the complex muscle response individually. Assuming that the tendon jerk reflex is similar to the SLR part of the complex signal, the algorithm described above to calculate the end of the tendon jerk reflex response was used to estimate the end of the SLR. In the EMG response after tibia translation the first part of the SLR from onset to the first peak corresponds to section B in the tendon jerk reflex (Fig. 2) and is not yet contaminated by the MLR. In nine subjects we found trials that showed only SLR responses (Table 1). Using the same procedure as in the tendon jerk reflex we could show that the algorithm to predict the duration of the tendon jerk reflexes can also be used for the SLR. The mean overall duration of the SLR EMG response was 20.3±7.1 ms (mean ± SD, range 12.0–34.9 ms). The calculated value for duration time showed a mean (± SD) percentage of 99% (±11%), and the study group a mean value of 134% (±41%). Table 2 summarizes the algorithm that was used to assess the onset latencies of SLR and MLR after tibia translation.
The mean (± SD) onset latency of the SLR EMG response was 20.3 ms (±3.5; range 15.4–25.8). Compared with the mean onset latency of the tendon jerk reflex of 21.9 ms (±3.1; range 17.3–28.7) there was no statistically significant difference (p =0.088, Fig. 4). A detailed analysis of the onset latencies looking at the group S and group SM/sM/Sm signal configurations (Fig. 5) showed no statistically significant differences for the SLR latency between these groups.

The mean (± SD) onset latencies: tendon jerk reflex (TJR) 21.9±3.1 ms; SLR 20.3±3.5 ms. No statistically significant difference was found (p =0.088)

SLR latencies (mean ± SD) between the different signal configurations. No significant differences were found
The mean (± SD) onset latency of the MLR response was 38.9 ms (±4.2 ms; range 32.9–46.7). Again, the detailed analysis of the onset latencies looking at the group M and group SM/sM/Sm signal configurations (Fig. 6) showed no statistically significant differences for the MLR latency.

MLR latencies (mean ± SD) between the different signal configurations. No significant differences were found
Additional experiments
In the five subjects investigated after lidocain injection of the dorsal calf no significant differences of the SLR (18.1±4.4 ms) and the MLR (40.5±8.7 ms) latencies were found compared with the untreated trials (SLR 19.1±4 ms and MLR 38.8±7.1 ms).
In those three subjects that were investigated with a position transducer and an acceleration sensor in parallel, a difference of 14.9±4.3 ms (range 8.8–22.6) for the trigger point determination of the tibial movement between these two sensors was found, so that the acceleration sensor increases the latency values.
Discussion
In the present study we found that an anterior translation of the tibia evokes a reflex response that could consist of two main components: the first occurs at a latency of around 20 ms, which corresponds to the latency of a SLR; the second component occurs at 39 ms, which corresponds to the latency of a MLR. We developed an evaluation algorithm which allows a safe differentiation between the SLR and MLR components.
SLR
Faist et al. (1999) reported for the tendon jerk reflex of the biceps femoris latencies of 20 ms (range: 18–24), which is comparable to the present results. Our results of the tibia translation responses showed for the fastest component a mean latency of 20 ms, compatible with a SLR which is mainly mediated by the monosynaptic reflex arc. Taking into account the low range for tendon jerk reflex latencies (maximum 24 ms) reported by Faist et al. (1999), a latency of more than 30 ms after the onset of the tibial movement cannot be regarded as a SLR and was therefore regarded as a MLR and a missing SLR.
MLR
In our study the mean latency for the MLR was 38.9 ms. When we calculated the reflex times using the evaluation algorithm described above, we could clearly differentiate between SLR and MLR. Group M reflex responses represent isolated MLRs without superimposed SLRs (see Fig. 3). There was no significant difference between the latency of group M reflex responses and the MLR latency of the complex signals of the remaining groups (SM, Sm, sM). This demonstrates that with the developed evaluation algorithm it is possible to differentiate between SLR and MLR independent of the shape of the superimposed SLR/MLR response. Grey et al. (2001) argued that it is not possible to perform this differentiation merely by visual inspection. Because of this they gave no data for the latency of the MLR. Our results support the view that in many cases the visual differentiation is not possible. However, the presented evaluation algorithm allows it. Grey et al. (2001) reported a difference of the onset latency between SLR and MLR of 25 ms for the M. triceps surae. Toft et al. (1989) found a difference of 27 ms when they measured peak latencies. The reason for the smaller difference of 18.6 ms in our results can be explained sufficiently with the shorter reflex pathways from the knee joint (Grey et al.2001). Our reflex latencies of the MLR are similar to the latencies reported by Beard et al. (1994c) and Jennings and Seedhom (1994). Neither Beard nor Jennings (Beard et al. 1993, 1994a, c; Jennings and Seedhom 1994) reported mean latencies below 40 ms, while we have found in most measurements responses compatible with SLRs. In their studies the subjects were standing on one leg and the tibia translation was evoked with a lower force of 89 N. To rule out that the lower force is responsible for this difference, we performed additional experiments in ten subjects where we varied the force from 50 to 300 N. We found a substantial effect neither on the signal configuration nor on the latencies, while the amplitude was increasing with increasing force.
Beard et al. (1994c) and Jennings and Seedhom (1994) refer their latencies to the first distinguishable onset after the trigger signal and report latencies in the range of MLRs, while our results suggest that in most subjects SLRs should be found. A possible explanation can be the trigger signal. Beard et al. (1994c) and Jennings and Seedhom (1994) determined the onset of the tibial movement with an acceleration sensor. In our study the onset of the actual tibial movement was assessed by a position transducer. An acceleration sensor records an acceleration even if the examined structure has not yet covered a relevant distance. With that the trigger point is moved forward in time through the acceleration sensor and consequently the latency is prolonged. This may explain why the reflex latencies published by Beard (Beard et al. 1994c) and Jennings and Seedhom (1994) are in the range of the MLR although it actually may be a SLR. In additional experiments with three subjects we used in parallel a position transducer and an acceleration sensor attached to the tibia. Between these two sensors we found a difference of approximately 15 ms for the trigger point determination of the tibial movement.
In contrast to the pneumatic cylinders used by Beard (Beard et al.1993, 1994a, c; Jennings and Seedhom 1994), Bruhn (1999) induced a force impulse in posterior-anterior direction through a block-and-tackle-construction. Different from our experimental setting, the femur was not fixed ventrally. The subjects were standing freely with full weight bearing. Bruhn (1999) reported a latency of 58–65 ms. They also observed complex muscle responses with several peaks as we found in our results (unpublished data, personal communication Bruhn).
From the present experiments the pathways involved in the MLR evoked by an anterior tibial translation cannot be determined. Beard et al. (1993, 1994c), Jennings and Seedhom (1994) and Bruhn (1999) suggested that these reflex responses are related to the cruciate ligament—hamstring reflex. A contribution of the cruciate ligament to the hamstring reflex activity was shown by Krogsgaard et al. (2002) and Dyhre-Poulsen and Krogsgaard (2000). They showed EMG responses with different latencies after electrical stimulation of the cruciate ligaments. Jerosch and Prymka (1997) demonstrated that meniscal injuries may induce disturbances of the sensorimotor system which result in a disturbed regulation of the hamstring muscles. Valgus positional perturbations of the human knee can elicit reflex muscle contractions in the hamstrings (Dhaher et al. 2003). However, the actual influence of ligamental structures of the knee joint on reflex activity in the hamstrings that may be altered after knee injury remains unclear and requires further studies. To investigate the contribution of different anatomical structures to the muscle response after tibia translation, it is necessary to reliably differentiate the complex muscle response. The algorithm developed in this paper allows this clear differentiation between SLR and MLR.
References
Basmajian J, De Luca C (1985) Muscles Alive. Williams & Wilkins
Beard DJ, Kyberd PJ, Fergusson CM, Dodd CA (1993) Proprioception after rupture of the anterior cruciate ligament. An objective indication of the need for surgery? J Bone Joint Surg Br 75:311–315
Beard DJ, Dodd CA, Trundle HR, Simpson AH (1994a) Proprioception enhancement for anterior cruciate ligament deficiency. A prospective randomised trial of two physiotherapy regimes. J Bone Joint Surg Br 76:654–659
Beard DJ, Kyberd PJ, Dodd CA, Simpson AH, O’Connor JJ (1994b) Proprioception in the knee. J Bone Joint Surg Br 76:992–993
Beard DJ, Kyberd PJ, O’Connor JJ, Fergusson CM, Dodd CA (1994c) Reflex hamstring contraction latency in anterior cruciate ligament deficiency. J Orthop Res 12:219–228
Biedert RM, Stauffer E, Friederich NF (1992) Occurrence of free nerve endings in the soft tissue of the knee joint. A histologic investigation. Am J Sports Med 20:430–433
Bruhn S (1999) Improved measurement of knee-joint stability. The Michael-Jager Prize for a Stuttgart research group. Orthopade 28:819
Burke D, Gandevia SC, McKeon B (1984) Monosynaptic and oligosynaptic contributions to human ankle jerk and H-reflex. J Neurophysiol 52:435–448
Dhaher YY, Tsoumanis AD, Rymer WZ (2003) Reflex muscle contractions can be elicited by valgus positional perturbations of the human knee. J Biomech 36:199–209
Diener HC, Dichgans J, Bootz F, Bacher M (1984) Early stabilization of human posture after a sudden disturbance: influence of rate and amplitude of displacement. Exp Brain Res 56:126–134
Dietz V, Berger W (1982) Spinal coordination of bilateral leg muscle activity during balancing. Exp Brain Res 47:172–176
Dietz V, Mauritz KH, Dichgans J (1980) Body oscillations in balancing due to segmental stretch reflex activity. Exp Brain Res 40:89–95
Durselen L, Claes L, Kiefer H (1995) The influence of muscle forces and external loads on cruciate ligament strain. Am J Sports Med 23:129–136
Dyhre-Poulsen P, Krogsgaard MR (2000) Muscular reflexes elicited by electrical stimulation of the anterior cruciate ligament in humans. J Appl Physiol 89:2191–2195
Faist M, Blahak C, Duysens J, Berger W (1999) Modulation of the biceps femoris tendon jerk reflex during human locomotion. Exp Brain Res 125:265–270
Freeman MA, Wyke B (1967) Articular reflexes at the ankle joint: an electromyographic study of normal and abnormal influences of ankle-joint mechanoreceptors upon reflex activity in the leg muscles. Br J Surg 54:990–1001
Friden T, Roberts D, Ageberg E, Walden M, Zatterstrom R (2001) Review of knee proprioception and the relation to extremity function after an anterior cruciate ligament rupture. J Orthop Sports Phys Ther 31:567–576
Fujita I, Nishikawa T, Kambic HE, Andrish JT, Grabiner MD (2000) Characterization of hamstring reflexes during anterior cruciate ligament disruption: in vivo results from a goat model. J Orthop Res 18:183–189
Grey MJ, Ladouceur M, Andersen JB, Nielsen JB, Sinkjaer T (2001) Group II muscle afferents probably contribute to the medium latency soleus stretch reflex during walking in humans. J Physiol 534:925–933
Gruber J, Wolter D, Lierse W (1986) Anterior cruciate ligament reflex (LCA reflex). Unfallchirurg 89:551–554
Haus J, Halata Z (1990) Innervation of the anterior cruciate ligament. Int Orthop 14:293–296
Haus J, Halata Z, Refior HJ (1992) Proprioception in the anterior cruciate ligament of the human knee joint—morphological bases. A light, scanning and transmission electron microscopy study. Z Orthop Ihre Grenzgeb 130:484–494
Imran A, O’Connor J (1998) Control of the knee stability after ACL injury or repair: interaction between hamstrings contraction and tibial translation. Clin Biomech (Bristol, Avon) 13:153–162
Jennings AG, Seedhom BB (1994) Proprioception in the knee and reflex hamstring contraction latency. J Bone Joint Surg Br 76:491–494
Jerosch J, Prymka M (1997) Proprioceptive deficits of the knee joint after rupture of the medial meniscus. Unfallchirurg 100:444–448
Krogsgaard MR, Dyhre-Poulsen P, Fischer-Rasmussen T (2002) Cruciate ligament reflexes. J Electromyogr Kinesiol 12:177–182
Miyatsu M, Atsuta Y, Watakabe M (1993) The physiology of mechanoreceptors in the anterior cruciate ligament. An experimental study in decerebrate-spinalised animals. J Bone Joint Surg Br 75:653–657
More RC, Karras BT, Neiman R, Fritschy D, Woo SL, Daniel DM (1993) Hamstrings—an anterior cruciate ligament protagonist. An in vitro study. Am J Sports Med 21:231–237
Nardone A, Grasso M, Giordano A, Schieppati M (1996) Different effect of height on latency of leg and foot short- and medium- latency EMG responses to perturbation of stance in humans. Neurosci Lett 206:89–92
Raunest J, Sager M, Burgener E (1998) Proprioception of the cruciate ligaments: receptor mapping in an animal model. Arch Orthop Trauma Surg 118:159–163
Reider B, Arcand MA, Diehl LH, Mroczek K, Abulencia A, Stroud CC, Palm M, Gilbertson J, Staszak P (2003) Proprioception of the knee before and after anterior cruciate ligament reconstruction. Arthroscopy 19:2–12
Schieppati M, Nardone A, Siliotto R, Grasso M (1995) Early and late stretch responses of human foot muscles induced by perturbation of stance. Exp Brain Res 105:411–422
Schultz RA, Miller DC, Kerr CS, Micheli L (1984) Mechanoreceptors in human cruciate ligaments. A histological study. J Bone Joint Surg Am 66:1072–1076
Schutte MJ, Dabezies EJ, Zimny ML, Happel LT (1987) Neural anatomy of the human anterior cruciate ligament. J Bone Joint Surg Am 69:243–247
Sjolander P, Johansson H, Sojka P, Rehnholm A (1989) Sensory nerve endings in the cat cruciate ligaments: a morphological investigation. Neurosci Lett 102:33–38
Solomonow M, Krogsgaard M (2001) Sensorimotor control of knee stability. A review. Scand J Med Sci Sports 11:64–80
Solomonow M, Baratta R, Zhou BH, Shoji H, Bose W, Beck C, D’Ambrosia R (1987) The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 15:207–213
Toft E, Sinkjaer T, Andreassen S (1989) Mechanical and electromyographic responses to stretch of the human anterior tibial muscle at different levels of contraction. Exp Brain Res 74:213–219
Zimny ML, Schutte M, Dabezies E (1986) Mechanoreceptors in the human anterior cruciate ligament. Anat Rec 214:204–209
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Friemert, B., Bumann-Melnyk, M., Faist, M. et al. Differentiation of hamstring short latency versus medium latency responses after tibia translation. Exp Brain Res 160, 1–9 (2005). https://doi.org/10.1007/s00221-004-1980-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-004-1980-4