
Abstract
This study used repetitive transcranial magnetic stimulation (rTMS) to investigate the roles of the right dorsolateral prefrontal cortex (DLPFC) and supplementary motor area (SMA) in short (500 ms) and long (2 s) interval timing. The results were compared with rTMS over the leg area of motor cortex, an area not thought to be involved with time estimation. rTMS was delivered during one of two phases of a time reproduction task: at the onset of the Estimation Phase (presentation of the interval to be timed) and at the onset of the Reproduction Phase (subjects’ reproduction of the timed interval). There was a significant main effect of Site (SMA vs. right DLPFC vs. leg motor area) due to the fact that rTMS over the right DLPFC caused subjects to underestimate time intervals compared with rTMS over the leg motor area. There was also a significant three-way interaction between Site, Duration and Phase (Estimation Phase vs. Reproduction Phase) that post hoc analyses showed was due to underestimation of long intervals when rTMS was given over the right DLPFC at the start of the Reproduction Phase. There was no effect of rTMS over the right DLPFC or SMA in the short interval task. This is consistent with previous studies showing that the right DLPFC is important in estimating time intervals in the seconds-range. In addition, we suggest that the selectivity of the rTMS effect for the Reproduction Phase indicates that the right DLPFC plays a particular role in memory processes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A substantial body of research has investigated the areas of the brain involved in motor and perceptual timing in the milliseconds and seconds ranges. Traditionally, researchers have proposed that there must be some type of ‘internal clock’ that meters temporal behaviour (e.g. Gibbon et al. 1984; Treisman 1963). Clinical studies involving patients with Parkinson’s disease (Harrington et al. 1998; O’Boyle et al. 1996; Pastor et al. 1992a, b) and cerebellar disease (Casini and Ivry 1999; Ivry et al. 1988; Mangels et al. 1998) have implicated the basal ganglia and cerebellum in this internal clock process. Animal studies, typically lesion work, have provided further evidence that the cerebellum is important in temporal processing (e.g. Breukelaar and Dalrymple-Alford 1999; Clarke et al. 1996; Perrett et al. 1998; Yeo et al. 1985a, b, c). Pharmacological studies using rodents have revealed that dopamine agonists and dopamine antagonists have opposite effects on timing behaviour and increase and decrease the speed of the internal clock, respectively (e.g. Maricq and Church 1983; Maricq et al. 1981; Meck 1986). This finding implicates the dopamine rich nigrostriatal system in timing and is echoed in the positive effect that l-dopa medication has on the timing performance of Parkinson’s disease patients (O’Boyle et al. 1996; Pastor et al. 1992a, b). More recently, functional imaging studies have confirmed that the basal ganglia (Jueptner et al. 1995; Rao et al. 1997, 2001; Schubotz et al. 2000) and cerebellum (Jueptner et al. 1995, 1996; Kawashima et al. 2000; Penhune et al. 1998; Ramnani and Passingham 2001; Schubotz et al. 2000) are activated in timing tasks. Functional imaging studies (Brunia et al. 2000; Jueptner et al. 1996; Maquet et al. 1996; Rao et al. 2001; Tracy et al. 2000) and those involving EEG recordings (Damen and Brunia 1994; Mohl and Pfurtscheller 1991; Monfort et al. 2000) have also found evidence of a right cortical timing network, particularly involving parietal areas and the dorsolateral prefrontal cortex (DLPFC).
While the above evidence suggests the basal ganglia, cerebellum and frontal and parietal areas are involved in temporal processing, their differential roles are not clear. Ivry (1996) suggested that milliseconds- and seconds-range timing involve different neural structures and proposed that the cerebellum is involved in milliseconds-range timing and that the basal ganglia is involved in seconds-range timing. In an investigation of this claim, we used positron emission tomography (PET) to compare short-interval (500 ms) and long-interval (2 s) timing and found that the right DLPFC was only active at the longer time range, although cerebellar and basal ganglia activation was present during both (Jones et al. 2000). The results of our imaging study concur with the observation that functional imaging studies showing DLPFC activation tend to use longer intervals and tasks that are more ‘cognitive’, rather than short-range, automatic timing tasks (Lewis and Miall 2003). This distinction is reflected in a clinical study that showed that patients with prefrontal lesions have difficulty with timing of long-range (4 s) but not short-range (400 ms) intervals (Mangels et al. 1998). In another study, patients with prefrontal lesions were found to be impaired on a duration discrimination task (400 ms) and frequency discrimination task when they were combined in a dual task paradigm. Cerebellar patients were only impaired on the duration discrimination task. The authors argued that inadequate attentional resources underpinned the frontal patients’ deficits (Casini and Ivry 1999), although others have cited inadequate memory processes (e.g. Mangels et al. 1998). It is evident that considerable debate remains regarding the differential roles of the structures implicated in timing, particularly as brain areas involved in a timing task may not necessarily be part of the hypothesised ‘internal clock’, but provide necessary cognitive, sensory or motor components. One way of identifying the areas that are ‘essential’ to temporal processing is to use transcranial magnetic stimulation (TMS). This technique uses a magnetic field to create a safe, temporary disruption of neural functioning in a discrete area. Thus, behavioural disruption following TMS would indicate that the targeted brain area was essential to the task (Jahanshahi and Rothwell 2000).
To date, there have been few investigations of temporal processing using TMS. Theoret and colleagues (2001) used 5 min of 1-Hz repetitive TMS (rTMS) in a ‘before and after’ paradigm to investigate the effect on repetitive tapping (tapping in time to a visual cue) with an inter-stimulus interval of 475 ms. rTMS over the medial cerebellum was found to affect variability, but not accuracy. Conversely, rTMS over the lateral cerebellum and motor cortex did not affect either dimension. Koch et al. (2003) tested subjects on a time reproduction task (estimating and then reproducing a period of time) before and after 10 min of 1-Hz rTMS over the right DLPFC and left DLPFC. Stimulation over the right DLPFC resulted in an underestimation of intervals of 5- and 15-s duration, whereas stimulation over the left DLPFC did not alter timing behaviour. The authors concluded that the right DLPFC plays a specific role in seconds-range timing and speculate that its function is related to memory or decision processes. However, the researchers instructed the subjects to read a random sequence of numbers aloud (presented on a computer screen) whilst they were completing the task. This additional instruction was proposed to prevent subvocal counting and to therefore provide a more realistic representation of interval timing. However, the addition of the counting task creates a dual-task paradigm, which is known to affect temporal performance (e.g. Fortin et al. 1993; Sergent et al. 1993) and is likely to place additional demands on frontal areas such as the DLPFC. Furthermore, in using long intervals only, the possibility of the DLPFC being essential during millisecond estimation was not investigated. A PET study has also used the temporal reproduction paradigm to investigate seconds-range interval timing. In agreement with Koch and colleagues, Macar et al. (2002) discovered a right hemisphere network, including the right DLPFC. However, they also found evidence of supplementary motor area (SMA) activity. The SMA is the main projection site of the straito-frontal motor loop (Alexander et al. 1990) and is believed to recruit timing information from the basal ganglia. This led the authors to suggest that the SMA forms a key role in the timing process. Previous functional imaging work, including our own investigation of long and short interval estimation (e.g. Brunia et al. 2000; Jones et al. 2000; Kawashima et al. 2000; Ramnani and Passingham 2001; Schubotz et al. 2000), has also found that the SMA is activated during temporal processing and the projections it receives from the basal ganglia clearly make this assumption attractive.
Further investigation with rTMS is necessary to establish the role of the right DLPFC and the SMA in a time reproduction task. To date, rTMS has not been used to investigate whether the SMA is essential to temporal processing. In contrast to the study of Koch and colleagues, we tested millisecond and second intervals to determine if the short/long dichotomy supported by our functional imaging results is a key issue in the differential roles of the SMA and the right DLPFC in temporal processing. Additionally, as a time reproduction task involves two distinct phases, an Estimation Phase and a Reproduction Phase, we stimulated the brain at both phases such that the influence of the SMA and right DLPFC on the component timing processes occurring in each phase was investigated. A potential problem with rTMS is that the auditory and sensory component of the stimulation can disrupt timing behaviour and that this can be difficult to disentangle from real, neural effects. For example, listening to a train of clicks during timing is known to increase arousal and distort time estimation (e.g. Penton-Voak 1996). Therefore, a control site, the leg motor area, was also included.
Materials and methods
Subjects
Nine right-handed, university-educated subjects (mean age 30.6 years; SD 6.19; range 24–41) participated in the study. Three were female and six were male. All of the subjects were healthy and without a history of neurological or psychiatric disease or head injury. Written, informed consent was obtained from all subjects prior to the experiment and the study had the approval of the Joint Medical Ethics Committee of the National Hospital for Neurology and Neurosurgery and the Institute of Neurology.
Design
The study used a repeated measures 3 (Site) × 2 (Duration) × 2 (Phase) design. Each subject performed a time estimation and reproduction task at both SHORT and LONG interval lengths. For each interval length, there were three rTMS sites tested (SMA, right DLPFC and leg motor area), with rTMS delivered at one of two time points: Estimation Phase and Reproduction Phase. The order of conditions was counterbalanced using a Latin Square design.
Procedure
Subjects were seated opposite a computer screen with a response button placed at a comfortable distance in front of them. The task was first described to the subjects and they then attempted five practice trials (no rTMS) to ensure that they fully understood it. The task involved reproducing an interval of time that was visually presented to the subjects. A light blue circle (Circle 1) was flashed in the centre of a grey screen for 100 ms, and after a specified period a dark blue circle (Circle 2) appeared for 100 ms. The subjects were instructed to estimate the period between the appearances of the two circles (Estimation Phase). As soon as the dark blue circle disappeared, the subjects were asked to start reproducing the interval that they had just estimated (Reproduction Phase). When they considered that the same amount of time had elapsed, then they were to press the response button. Their response initiated the presentation of a black circle (Circle 3), which also appeared for 100 ms. No feedback was given. All subjects used their right index finger to respond.
For each rTMS site, a complete run consisted of 50 trials (split into two 25 trial blocks) in which the subjects estimated SHORT intervals and 50 trials (split into two 25 trial blocks) in which the subjects estimated LONG intervals. SHORT trials had a standard interval of 400, 450, 500, 550 or 600 ms (average 500 ms). LONG trials had a standard interval of 1,600, 1,800, 2,000, 2,200 or 2,400 ms (average 2,000 ms). The computer programme selected interval lengths pseudo-randomly, such that each subject received five presentations of each interval length within a 25 trial block. The inter-trial intervals were one of five randomly selected lengths (2,000, 2,500, 3,000, 3,500 or 4,000 ms). The different interval lengths were used to prevent learning. A baseline condition was also included in which subjects completed two 25 trial bocks (one SHORT, one LONG) without any rTMS occurring.
rTMS
The rTMS was delivered at one of two time points during the task; at the beginning of the Estimation Phase (i.e. at the onset of Circle 1) and at the beginning of the Reproduction Phase (i.e. at the onset of Circle 2). In the SHORT and LONG conditions, one block of 25 trials consisted of stimulation during the Estimation Phase and the other block of 25 trials consisted of stimulation during the Reproduction Phase.
rTMS was delivered with a flat figure-of-eight coil (90 mm outer winding diameter) connected to a Magstim rapid stimulator (Magstim, Whitland, Dyfed, UK). Each time four stimuli were given at a rate of 20 Hz. The three sites for the rTMS were the SMA, the right DLPFC and the leg motor area. The leg motor area was determined as the spot in which maximum muscle activity was observed in the legs when held out in front of the subject with ankles dorsiflexed (all areas were established using single stimulus pulses). To localize the SMA site, the coil was moved 4 cm forward from the leg motor site (approx. FCz). The DLPFC is a broad area; we used a site similar to that used by other research groups using TMS (e.g. Epstein et al. 2002; Zheng 2000). The coil was placed 5 cm anterior from the hand motor area on the right hemisphere and held parallel to the midsaggital line. The hand motor area was located by finding the lowest threshold spot for activating the contralateral first dorsal interosseous (FDI) muscle. For both the leg motor area and right DLPFC, rTMS was applied at an intensity equal to the resting hand motor threshold. The latter was established visually by finding the threshold at which a motor twitch was observed approximately 50% of the time, whilst the hand was in a resting state. To ensure that the rTMS penetrated deep enough at the SMA site, 90% of the active leg motor threshold was used. This was determined by finding the threshold at which 50% of pulses induced a twitch in the legs when held in the position described above (i.e. when leg muscles were active). For all three sites the coil handle was pointing backwards. The study used rTMS parameters within established guidelines (Wassermann 1998).
Results
Although the main focus of our experiments was to compare the effects of rTMS at different scalp sites, we also included a baseline condition in which no TMS was applied. As expected (Vierordt’s Law), subjects tended to overestimate the duration of the SHORT interval (mean 595 ms rather than 500 ms), whereas they tended to underestimate the LONG interval (mean 1,860 ms rather than 2,000 ms). When rTMS was applied over the leg motor area, all estimates were longer than the no stimulation condition (see Fig. 2). Since the leg motor area is not known to play any role in time estimation, we interpret this overestimation to factors such as the noise of the stimulus and the scalp sensation produced by rTMS interfering with performance of the task. As a result, further analysis was confined to comparison of rTMS over the leg motor area with rTMS over DLPFC or SMA.
Site-specific effects of rTMS
A three-factor ANOVA on the data (see Methods) revealed, as expected, a main effect of Duration (F (1,8)=386.15, p=0.001), and also a significant effect of Site of stimulation (F (1,8)=3.82, p=0.04). There was no significant main effect of Phase. The analysis also showed that there was a significant three-way interaction (Site × Duration × Phase: F (1,8)=3.55, p=0.05), none of the other interactions were significant.
The main effect of Site is explored in Fig. 1, where data has been collapsed over both phases and durations of the task. A priori tests showed that the main effect was due to rTMS over the right DLPFC causing subjects to underestimate time intervals compared with rTMS over the leg motor area (F (1,8)=15.18, p=0.001).

Mean differences in time reproductions of the subjects collapsed across Phase and Duration. *Significant effect of difference between rTMS over the right DLPFC and rTMS over the leg motor area
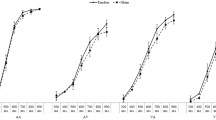
The three-way interaction was explored by separate two-factor ANOVAs for SHORT and LONG intervals (Fig. 2a, b). The ANOVA for the SHORT interval was not significant for the main effects of Site and Phase, or for the interaction of Site × Phase. To ensure that no effects in the SHORT condition could be contributing to the significant three-way interaction, a paired samples t-test was used to compare the time reproduction values for rTMS over the right DLPFC compared with rTMS over the leg motor area in the Estimation Phase. This test was not significant and as rTMS over these two areas showed the greatest difference within a Phase, we are confident that no data from the SHORT condition could be explaining the three-way interaction. In contrast, the ANOVA for the LONG interval approached significance for the effect of Site (F (1,8)=3.17, p=0.07) and for the Site × Phase interaction (F (1,8)=2.75, p=0.09). As the Site and Phase effects in the LONG condition appeared to be the likely source of the significant three-way interaction, post hoc paired samples t-tests were used to explore the significant interaction. rTMS over the right DLPFC was significantly different from rTMS over the leg motor area during the Reproduction Phase for LONG intervals (t (8)=−3.21, p=0.01). There were no significant effects for the Estimation Phase. We conclude that rTMS over the right DLPFC caused subjects to underestimate LONG time intervals when it was applied in the Reproduction phase of the task.

a Mean differences in time reproductions of the subjects SHORT condition. b Mean differences in time reproductions of the subjects LONG condition
Discussion
The present experiment explores the effect of disrupting function in the right DLPFC and the SMA with rTMS during a time reproduction task. The results were compared with the effect of rTMS over the leg motor cortex since this is unlikely to be involved in time reproduction and could therefore control for the effects of the noise and scalp sensation produced by rTMS. Indeed, comparison with a condition where no rTMS was given showed that these effects caused a general overestimation of interval estimation, perhaps due to changes in the arousal levels of the subjects. The data analysis was therefore confined to site-specific comparisons of rTMS. These showed that subjects underestimated the duration of LONG (average 2 s) intervals if rTMS was given to the right DLPFC during the Reproduction Phase of the task. There were no effects of right DLPFC stimulation in the SHORT (average 500 ms) interval estimation and there were no significant effects of SMA stimulation.
It is also worth noting that rTMS over the SMA and the right DLPFC resulted in a decrease in the time reproduction values when compared with rTMS over the leg motor area. This implies that the natural bias towards underestimating long intervals (Vierordt’s law; see Woodrow 1951) is increased when rTMS is used at these sites. The significantly increased effect on a pre-existing response tendency with rTMS over the right DLPFC in the Reproduction Phase (when compared with rTMS over the leg motor area) implies that this modulation of a pre-existing response bias is particularly related to the right DLPFC. Modulation of an existing response bias using rTMS has also been found in a study using rTMS to investigate random number generation; in this study rTMS over the left DLPFC altered the direction of the subject’s response bias (Jahanshahi et al. 1998).
Right dorsolateral prefrontal cortex
The data suggest that in long interval timing, the right DLPFC performs a function at the beginning of the Reproduction Phase that is essential to temporal reproduction. This pattern of results complement our functional imaging study in which subjects reproduced previously learned intervals of 500 ms and 2 s (Jones et al. 2000). Right DLPFC activation was only observed in the long interval condition, which led us to conclude that it was involved in the additional cognitive processes that seconds-range timing requires. Our functional imaging study also found right SMA activation in the long interval condition, although evidence to suggest that the SMA is essential to temporal processing is not clear in the present study. Additionally, the findings partially concur with the PET study of Macar et al. (2002) who found SMA and DLPFC activation in a similar temporal reproduction paradigm. However, the intervals used were, on average, 2.7 and 11 s, which are much longer than those used here.
The results also confirm the findings of Koch et al. (2003) who found underestimation in a seconds-range temporal reproduction task with rTMS over the right, but not left, DLPFC. Our study extends this conclusion in showing that rTMS during the Reproduction Phase, but not the Estimation Phase, has a significant effect on temporal processes. Koch et al. (2003) suggested that the underestimation could reflect memory or decision making processes. The results presented here argue against the second hypothesis as the effect of rTMS was only significant when it occurred at the onset of Circle 2, which is unlikely to significantly impact upon the decision to respond. The onset of Circle 2 is also the point at which the temporal reproduction occurs, i.e. ‘clock’ processes are initiated to reproduce a period of time. However, we do not believe that these clock processes are being disrupted, as clock processes are also initiated at the onset of Circle 1. We propose that the disruption produced by rTMS over the right DLPFC at this time point reflects interference with memory processes, since at the onset of Circle 2 subjects would be consolidating the time interval presented during the Estimation Phase (marked by Circles 1 and 2) in memory. This reflects the pharmacological work of Meck and colleagues (Meck 1983; Meck and Church 1987a, b) as well as a rat lesion study (Olton 1989), both of which suggest that the frontal cortex is involved in the transfer of temporal intervals to memory.
The lack of effect of rTMS on estimation of SHORT intervals suggests that the right DLPFC plays a differential role in milliseconds- and seconds-range timing. This concurs with the assertion that, unlike milliseconds-range timing, seconds-range time intervals are calculated using cognitive processes and recruit cortical areas such as the DLPFC and parietal cortex (Lewis and Miall 2003). In corroboration of this, Michon (1985) has proposed that information processing below 500 ms is highly perceptual and not accessible to cognitive control. Rammsayer (1999) found that duration discrimination of long intervals (1,000 ms) was affected by midazolam, which is known to affect working memory functions, whereas short interval discrimination (50 ms) was not. Indeed, a concurrent short-term memory task causes a lengthening of the reproduced interval in a time reproduction task when it occurs in the Reproduction Phase. Whilst, when the concurrent task occurs during the Estimation Phase, temporal reproductions decrease (Fortin and Rousseau 1998). This suggests that timing tasks share working memory resources with non-temporal tasks, particularly as concurrent tasks that don’t have a short-term memory component do not affect timing (e.g. Fortin and Breton 1995; Fortin et al. 1993). Overall, this implies that longer intervals are more vulnerable than short intervals to task-oriented memory processes subserved by prefrontal areas.
The key question that remains is whether the working memory components are storing the temporal information or providing timing calculations themselves? Fletcher and Henson (2001) suggest that the DLPFC is involved in selecting, manipulating and monitoring the items held in working memory. Certainly, many theorists dismiss the working memory aspects of the timing process as being non-specific. For example patients with frontal lesions are unable to execute a temporal (duration discrimination) or non-temporal (frequency discrimination) task when the intervals are too long and the memory load too demanding (e.g. Mangels et al. 1998). However, other research suggests that memory may be the key to timing. The Multiple Time Scale model of Staddon and Higa (1999) proposes that temporal judgements are based on memories of different ‘strengths’, i.e. a memory decays as time passes and this change is quantified in a systematic, predictable way by the organism. Indeed, inhibitory cell pairs have been identified in the DLPFC that appear to show a delay in activity between them of 200–1,400 ms, which has been presented as evidence of timing-like behaviour in the prefrontal cortex (Constantinidis et al. 2002). Lewis (2002) goes as far as proposing that this evidence suggests that the internal clock may be located within the prefrontal cortex, arguing that patients with Parkinson’s disease who display temporal deficits tend to be in an advanced stage of illness and thus have a deterioration in the dopaminergic projections to the prefrontal cortex. It is also worth noting that the original conceptions of working memory, derived from animal work with the delayed response task, considered working memory as holding information ‘on line’ over a period of time (e.g. Goldman-Rakic 1996). Regardless of the exact nature of the contribution of the prefrontal cortex to timing processes, it is undisputable that rTMS over the right DLPFC has a differential effect on the timing of SHORT and LONG intervals, and that this difference is in some way underpinned by the cognitive nature of estimating and reproducing long intervals. This leads us to conclude that the right DLPFC is essential to memory transfer and storage in seconds-range time reproduction.
Supplementary motor area
The results showed that rTMS over SMA had no significant effect compared with rTMS over the leg area on interval estimation in any of the tasks. At first sight this might lead to the conclusion that the SMA is not essential for time estimation. However, there is one limitation in the present experimental design that prevents us from interpreting any negative results. Although we gave rTMS over the approximate area of the SMA, we have no independent measure at the site and stimulus intensities we used that we were actually successful in disrupting activity in the SMA. Unlike the motor cortex, where effective stimulation can be verified by the presence of muscle twitches in contralateral body muscles, there is no test for effective stimulation of SMA. In fact, considerable evidence suggests that the SMA plays a non-motor role in timing; for example, SMA activation was found throughout the various stages of a duration discrimination task (Rao et al. 2001) and Macar et al. (1999) found EEG changes in the SMA during both duration discrimination and time reproduction tasks. Additionally, this study had a rhythmic presentation across trials whilst previous research has shown that lesions to the SMA result in impairments in reproducing rhythms from memory (Halsband et al. 1993) and SMA activation has been identified in an fMRI study of auditory and visual monitoring of rhythms (Schubotz et al. 2000). Clearly further work is needed to test these hypotheses with rTMS.
Summary
In conclusion, the different pattern of results in the SHORT and LONG conditions supports the hypothesis of previous researchers that short and long interval timing involves different neural structures (Ivry 1996; Lewis and Miall 2003). This study provides evidence that the right DLPFC is essential to the accurate reproduction of intervals in the 2-s range and that this is likely due to its role in the consolidation and transfer of temporal memory. This corroborates previous functional imaging and clinical work, which has suggested that the right hemisphere, including the right DLPFC, is involved in the timing of long (seconds) durations (e.g. Harrington et al. 1998; Jones et al. 2000; Lewis and Miall 2003).
References
Alexander GE, Crutcher MD, DeLong MR (1990) Basal ganglia-thalamocortical circuits: parallel substrates for motor, oculomotor, “prefrontal” and “limbic” functions. Prog Brain Res 85:119–146
Breukelaar JW, Dalrymple-Alford JC (1999) Effects of lesions to the cerebellar vermis and hemispheres on timing and counting in rats. Behav Neurosci 113:78–90
Brunia CH, de Jong BM, van den Berg-Lenssen MMC, Paans AM (2000) Visual feedback about time estimation is related to a right hemisphere activation measured by PET. Exp Brain Res 130:328–337
Casini L, Ivry RB (1999) Effects of divided attention on temporal processing in patients with lesions of the cerebellum or frontal lobe. Neuropsychology 13:10–21
Clarke S, Ivry RB, Grinband J, Roberts S, Shimizu N (1996) Exploring the domain of the cerebellar timing system. In: Pastor MA, Artieda J (eds) Time, internal clocks, and movement. Elsevier, New York, pp 257–280
Constantinidis C, Williams GV, Goldman-Rakic PS (2002) A role for inhibition in shaping the temporal flow of information in prefrontal cortex. Nat Neurosci 5:175–180
Damen EJ, Brunia CH (1994) Is a stimulus conveying task-relevant information a sufficient condition to elicit a stimulus-preceding negativity? Psychophysiology 31:129–139
Epstein CM, Sekino M, Yamaguchi K, Kamiya S, Ueno S (2002) Asymmetries of prefrontal cortex in human episodic memory: effects of transcranial magnetic stimulation on learning abstract patterns. Neurosci Lett 320:5–8
Fletcher PC, Henson RN (2001) Frontal lobes and human memory: insights from functional neuroimaging. Brain 124:849–881
Fortin C, Breton R (1995) Temporal interval production and processing in working memory. Percept Psychophys 57:203–215
Fortin C, Rousseau R (1998) Interference from short-term memory processing on encoding and reproducing brief durations. Psychol Res 61:269–276
Fortin C, Rousseau R, Bourque P, Kirouac E (1993) Time estimation and concurrent nontemporal processing: specific interference from short-term memory demands. Percept Psychophys 53:536–548
Gibbon J, Church RM, Meck WH (1984) Scalar timing in memory. Annals of the New York Academy of Sciences Vol 423:52–77
Goldman-Rakic PS (1996) Regional and cellular fractionation of working memory. Proc Natl Acad Sci U S A 93:13473–13480
Halsband U, Ito N, Tanji J, Freund HJ (1993) The role of premotor cortex and the supplementary motor area in the temporal control of movement in man. Brain 116:243–266
Harrington DL, Haaland KY, Hermanowicz N (1998) Temporal processing in the basal ganglia. Neuropsychology 12:3–12
Ivry RB (1996) The representation of temporal information in perception and motor control. Curr Opin Neurobiol 6:851–857
Ivry RB, Keele SW, Diener HC (1988) Dissociation of the lateral and medial cerebellum in movement timing and movement execution. Exp Brain Res 73:167–180
Jahanshahi M, Rothwell J (2000) Transcranial magnetic stimulation studies of cognition: an emerging field. Exp Brain Res 131:1–9
Jahanshahi M, Profice P, Brown RG, Ridding MC, Dirnberger G, Rothwell JC (1998) The effects of transcranial magnetic stimulation over the dorsolateral prefrontal cortex on suppression of habitual counting during random number generation. Brain 121:1533–4544
Jones C, Jahanshahi M, Dirnberger G, and Frith CD (2000) Estimation of long vs. short intervals: the functional anatomy of time estimation studied with PET. Cognitive Neuroscience Society Annual Meeting 2000:126–127 (abstract)
Jueptner M, Rijntjes M, Weiller C, Faiss JH, Timmann D, Mueller SP, Diener HC (1995) Localization of a cerebellar timing process using PET. Neurology 45:1540–1545
Jueptner M, Flerich L, Weiller C, Mueller SP, Diener HC (1996) The human cerebellum and temporal information processing—results from a PET experiment. NeuroReport 7:2761–2765
Kawashima R, Okuda J, Umetsu A, Sugiura M, Inoue K, Suzuki K, Tabuchi M, Tsukiura T, Narayan SL, Nagasaka T, Yanagawa I, Fujii T, Takahashi S, Fukuda H, Yamadori A (2000) Human cerebellum plays an important role in memory-timed finger movement: an fMRI study. J Neurophysiol 83:1079–1087
Koch G, Olivieri M, Torriero S, Caltagirone C (2003) Underestimation of time perception after repetitive transcranial magnetic stimulation. Neurology 60:1844–1846
Lewis PA (2002) Finding the timer. Trends in Cognitive Sciences 6:195–196
Lewis PA, Miall RC (2003) Distinct systems for automatic and cognitively controlled time measurement: evidence from neuroimaging. Curr Opin Neurobiol 13:250–255
Macar F, Vidal F, Casini L (1999) The supplementary motor area in motor and sensory timing: evidence from slow brain potential changes. Exp Brain Res 125:271–280
Macar F, Lejeune H, Bonnet M, Ferrara A, Pouthas V, Vidal F, Maquet P (2002) Activation of the supplementary motor area and of attentional networks during temporal processing. Exp Brain Res 142:475–485
Mangels JA, Ivry RB, Shimizu N (1998) Dissociable contributions of the prefrontal and neocerebellar cortex to time perception. Cognitive Brain Research 7:15–39
Maquet P, Lejeune H, Pouthas V, Bonnet M, Casini L, Macar F, Timsit BM, Vidal F, Ferrara A, Degueldre C, Quaglia L, Delfiore G, Luxen A, Woods R, Mazziotta JC, Comar D (1996) Brain activation induced by estimation of duration: a PET study. NeuroImage 3:119–126
Maricq AV, Church RM (1983) The differential effects of haloperidol and methamphetamine on time estimation in the rat. Psychopharmacology Berl 79:10–15
Maricq AV, Roberts S, Church RM (1981) Methamphetamine and time estimation. J Exp Psychol Anim Behav Process 7:18–30
Meck WH (1983) Selective adjustment of the speed of internal clock and memory processes. J Exp Psychol Anim Behav Process 9:171–201
Meck WH (1986) Affinity for the dopamine D2 receptor predicts neuroleptic potency in decreasing the speed of an internal clock. Pharmacol Biochem Behav 25:1185–1189
Meck WH, Church RM (1987a) Cholinergic modulation of the content of temporal memory. Behav Neurosci 101:457–464
Meck WH, Church RM (1987b) Nutrients that modify the speed of internal clock and memory storage processes. Behav Neurosci 10:465–475
Michon JA (1985) The compleat time experiencer. In: Michon JA, Jackson JL (eds) Time, mind and behaviour. Springer, Berlin Heidelberg New York, pp 21–52
Mohl W, Pfurtscheller G (1991) The role of the right parietal region in a movement time estimation task. NeuroReport 2:309–312
Monfort V, Pouthas V, Ragot R (2000) Role of frontal cortex in memory for duration: an event-related potential study in humans. Neurosci Lett 286:91–94
O’Boyle DJ, Freeman JS, Cody FWJ (1996) The accuracy and precision of timing of self-paced, repetitive movements in subjects with Parkinson’s disease. Brain 119:51–70
Olton DS (1989) Frontal cortex, timing and memory. Neuropsychologia 27:121–130
Pastor MA, Artieda J, Jahanshahi M, Obeso JA (1992a) Time estimation and reproduction is abnormal in Parkinson’s disease. Brain 115:211–225
Pastor MA, Jahanshahi M, Artieda J, Obeso JA (1992b) Performance of repetitive wrist movements in Parkinson’s disease. Brain 115:875–891
Penhune VB, Zattore RJ, Evans AC (1998) Cerebellar contributions to motor timing: a PET study of auditory and visual rhythm reproduction. J Cognit Neurosci 10:752–765
Penton-Voak IS, Edwards H, Percival A, Wearden JH (1996) Speeding up an internal clock in humans? Effects of click trains on subjective duration. J Exp Psychol Anim Behav Process 22:307–320
Perrett SP (1998) Temporal discrimination in the cerebellar cortex during conditioned eyelid responses. Exp Brain Res 121:115–124
Rammsayer TH (1999) Neuropharmacological evidence for different timing mechanisms in humans. Q J Exp Psychol B 52:273–286
Ramnani N, Passingham RE (2001) Changes in the human brain during rhythm learning. J Cognit Neurosci 13:952–966
Rao SM, Harrington DL, Haaland KY, Bobholz JA, Cox RW, Binder JR (1997) Distributed neural systems underlying the timing of movements. J Neurosci 17:5528–5535
Rao SM, Mayer AR, Harrington DL (2001) The evolution of brain activation during temporal processing. Nat Neurosci. 4:317–323
Schubotz RI, Friederici AD, Von CD (2000) Time perception and motor timing: a common cortical and subcortical basis revealed by fMRI. NeuroImage 11:1–12
Sergent V, Hellige JB, Cherry B (1993) Effects of responding hand and concurrent verbal processing on time-keeping and motor-implementation processes. Brain Cogn 23:243–262
Staddon JER, Higa JJ (1999) Time and memory: towards a pacemaker-free theory of interval timing. J Exp Anal Behavior 71:215–251
Theoret H, Haque J, Pascual-Leone A (2001) Increased variability of paced finger tapping accuracy following repetitive magnetic stimulation of the cerebellum in humans. Neurosci Lett 306:29–32
Tracy JI, Faro SH, Mohamed FB, Pinsk M, Pinus A (2000) Functional localization of a “Time Keeper” function separate from attentional resources and task strategy. NeuroImage 11:228–242
Treisman M (1963) Temporal discrimination and the indifference interval: implications for a model of the ‘internal clock’. Psychol Monographs 77:1–31
Wassermann EM (1998) Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5–7, 1996. Electroencephalogr Clin Neurophysiol 108:1–16
Woodrow H (1951) Time Perception. In: Stevens S (ed) Handbook of experimental psychology. Wiley, New York, pp 1224–1236
Yeo CH, Hardiman MJ, Glickstein M (1985a) Classical conditioning of the nictitating membrane response of the rabbit. I. Lesions of the cerebellar nuclei. Exp Brain Res 60:87–98
Yeo CH, Hardiman MJ, Glickstein M (1985b) Classical conditioning of the nictitating membrane response of the rabbit. II. Lesions of the cerebellar cortex. Exp Brain Res 60:99–113
Yeo CH, Hardiman MJ, Glickstein M (1985c) Classical conditioning of the nictitating membrane response of the rabbit. III. Connections of cerebellar lobule HVI. Exp Brain Res 60:114–126
Zheng XM (2000) Regional cerebral blood flow changes in drug-resistant depressed patients following treatment with transcranial magnetic stimulation: a statistical parametric mapping analysis. Psychiatry Research 100:75–80
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jones, C.R.G., Rosenkranz, K., Rothwell, J.C. et al. The right dorsolateral prefrontal cortex is essential in time reproduction: an investigation with repetitive transcranial magnetic stimulation. Exp Brain Res 158, 366–372 (2004). https://doi.org/10.1007/s00221-004-1912-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-004-1912-3