
Abstract
Glucose can modify proteins in human blood, forming early glycation products (e.g., Amadori compounds), which can slowly degrade to advanced glycation endproducts (AGEs). AGEs contribute significantly to complications of diabetes mellitus and, thus, represent markers of advanced disease stages. They are, however, currently unsuitable for early diagnosis and therapeutic monitoring. Here, we report sensitive strategies to identify and relatively quantify protein glycation sites in human plasma samples obtained from type 2 diabetes mellitus (T2DM) patients and age-matched nondiabetic individuals using a bottom-up approach. Specifically, Amadori peptides were enriched from tryptic digests by boronic acid affinity chromatography, separated by reversed-phase chromatography, and analyzed on-line by high-resolution mass spectrometry. Among the 52 Amadori peptides studied here were 20 peptides resembling 19 glycation sites in six human proteins detected at statistically significantly higher levels in T2DM than in the normoglycemic controls. Four positions appeared to be unique for T2DM within the detection limit. All 19 glycation sites represent promising new biomarker candidates for early diagnosis of T2DM and adequate therapeutic control, as they may indicate early metabolic changes preceding T2DM.

ᅟ
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glycation (or nonenzymatic glycosylation) is a ubiquitous post-translational protein modification formed in all organisms by the reaction of reducing sugars (e.g., glucose) with amino groups in proteins (Fig. 1) [1]. The resulting aldimines (also known as Amadori compounds, or early glycation products) can be oxidatively degraded to advanced glycation end products (AGEs) [2, 3]. This highly heterogeneous class of compounds has been recognized as marker of heart failure, uremia, atherosclerosis, neurodegenerative disorders, and diabetes mellitus [4–8]. In patients with diabetes, AGEs accumulate slowly and appear typically after several years of hyperglycemia, when the medical symptoms are clearly manifested [9]. In contrast, Amadori products accumulate already after a few weeks of diabetes-associated hyperglycemia [10], providing a unique opportunity to recognize early disease stages. Moreover, Amadori products are present at larger quantities in plasma proteins than individual AGEs and should thus be easier and more reliable to analyze [11].

Glucose-dependent reaction pathways yielding early glycation products and AGEs
To some degree, clinical diagnosis of diabetes already takes advantage of Amadori products. N-terminal glycation of the hemoglobin β-chain (HbA1c), for example, provides a good parameter for a patient’s blood glucose level during the preceding 3 mo [12]. The World Health Organization (WHO) and American Diabetic Association (ADA) guidelines consider HbA1c levels exceeding 6.5 % of the total erythrocyte hemoglobin as a clear indication of diabetes [13]. This long-term parameter, however, is not sensitive to short-term fluctuations of blood glucose levels, which may precede the development of persisting hyperglycemia [14]. Thus, further glycation sites to monitor the glucose levels at short (days) and intermediate (weeks) time intervals should provide improved diagnostics and better therapeutic controls [15].
Human serum albumin (HSA, 58 lysine residues) with a half-life time of around 20 d appears to be ideal for monitoring medium-term protein glycation levels in plasma. Although it is currently not possible to quantify single glycation sites in HSA, the total glycation degree can be determined in colorimetric assays [16]. These assays are easy to perform and allow high throughput but lack selectivity. More specific are the ketoamine oxidase assay and high performance liquid chromatography (HPLC)-based quantification of furosine in HSA hydrolyzates [17, 18]. Clinically relevant techniques rely typically on the specific interaction between Amadori compounds (cis-diol groups in the sugar moiety) and boronates, such as enzyme-linked boronate immunoassay (ELBIA) and boronic acid affinity chromatography (BAC) [19, 20]. All established techniques, however, characterize only global glycation degrees and do not allow quantification of individual glycation sites.
Recently established mass spectrometry techniques can reliably characterize protein glycation sites even in complex samples [21–23]. Zhang et al. identified 7749 unique glycated peptides corresponding to 3742 unique glycated proteins in pooled type 2 diabetes mellitus (T2DM) plasma samples [21]. While the dominant glycation sites of HSA, the most abundant protein in human plasma, at lysine residues 199, 281, 489, and especially 525 are well known [22], this recent study identified a total of 37 glycation sites in HSA. As glycation in addition affects the structure and function of proteins, a quantitative analysis of individual glycation sites in HSA may indicate both small or temporary alterations of glucose concentrations in blood and their influence on albumin binding and transport capacity [23].
In a previous report, we described the presence of Amadori peptides in tryptic digests of plasma samples obtained from individual T2DM patients by a mass spectrometry protocol that avoids the need of labeling the samples [24]. To move one step further towards potential clinical use of the technology, here we extend this study providing first evidence that relative quantification can distinguish the glycation patterns of individual T2DM patients from age-matched nondiabetic controls.
Materials and methods
Unless stated otherwise, materials were obtained from the following manufacturers:
Applichem (Darmstadt, Germany): iodoacetamide (≥98 %); Biosolve V.B. (Valkenswaard, The Netherlands): acetonitrile (LC/MS grade); Carl Roth GmbH & Co. (Karlsruhe, Germany): tris-(2-carboxyethyl)-phosphine hydrochloride (TCEP, ≥98 %), dithiothreitol (DTT, ≥99 %), and methanol (≥99.9 %); New Objective (Berlin, Germany): PicoTip on-line nano-ESI emitter (standard coating; outer diameter (o.d.) 360/20 μm and tip internal diameter (i.d.) 10 μm); QIAGEN GmbH (Hilden, Germany): 1 mL polypropylene column; Sartorius Stedim Biotech GmbH (Göttingen, Germany): Vivaspin filter devices (5000 Mw cut-off); SERVA Electrophoresis GmbH (Heidelberg, Germany): porcine trypsin (NB premium grade); Sigma-Aldrich Chemie GmbH (Taufkirchen, Germany): m-aminophenyl boronic acid agarose (mAPBA, suspension); Thermo Fisher Scientific (Dreieich, Germany): C18 gel loader StageTips; Waters GmbH (Eschborn, Germany): nanoAcquity UPLC BEH130 column (C18, ID 0.1 mm, length 10 cm, particle diameter 1.7 μm) and nanoAcquity UPLC Symmetry trap column (C18, i.d. 0.18 mm, length 2 cm, particle diameter 5 μm). Water was purified in-house (resistance 18 mΩ) on a PureLab Ultra Analytic System (ELGA Lab Water, Celle, Germany).
Plasma samples
Blood was obtained from five T2DM patients characterized by poor glycemic control (HbA1c ≥ 6.5 % of hemoglobin) and from four nondiabetic individuals matched for sex, age, and body mass index (BMI), see Electronic Supplementary Material (ESM), Table S-1. All blood samples were collected between 8 am and 9 am after a 12-h fast and stored at –80 °C.
Tryptic digestion
Plasma samples (100 μL) were depleted of lipids by centrifugation (9168 g, 30 min, 4 °C, Allegra centrifuge 21R; Beckman Coulter, Krefeld, Germany). Lipid-depleted plasma (20 μL) was diluted 10-fold with ammonium hydrogen carbonate (0.1 mol/L, pH 8.0) and desalted using Vivaspin filter devices (5 kDa cut-off) by concentrating (25 min, 9660 rpm) and diluting (0.5 mL) the samples three times. Protein concentrations were determined by a Bradford assay [25]. Briefly, acidic Coomassie Brilliant Blue G-250 solution (250 μL, 0.1 g/L in 10 % H3PO4 in 5 % aq. ethanol) was mixed with the protein sample (5 μL) in a 96-well microtiter plate, and the absorption at 595 nm was recorded in duplicates. Quantification relied on a 2-fold dilution series of bovine serum albumin (BSA; 1.0 mg/L to 62.5 μg/L). Aliquots corresponding to a protein content of 25 μg were complemented with SDS (10 % in water, w:v, 2 μL) and TCEP (50 mmol/L in water, 2 μL), diluted with aqueous ammonium hydrogen carbonate solution (50 mmol/L) to obtain a final volume of 20 μL, and incubated at 60 °C for 15 min. The samples were cooled to room temperature (RT), alkylated with iodoacetamide (0.1 mol/L, 2.2 μL) in the darkness (15 min, RT), and digested with trypsin (25 mg/L in 50 mmol/L ammonium hydrogen carbonate, 50 μL, 37 °C, overnight). Next morning the digest was frozen and stored at –80 °C. An aliquot (2 μg protein) of the sample was diluted with sample buffer (0.05 % bromophenol blue, 62.5 mmol/L Tris-HCl, pH 6.8, 20 % glycerol, 2 % SDS, 5 % β-mercaptoethanol) at least 2-fold and heated to 95 °C for 5 min. The proteins were separated by sodium dodecylsulfate polyacrylamide gel electrophoresis (SDS-PAGE, T = 12 %, C = 2.65 %) and stained with colloidal Coomassie Brilliant Blue G 250. The digestion step was considered complete (>99 %) when the original HSA band was not detectable.
Boronic acid affinity chromatography (BAC) [24]
Aliquots of tryptic plasma digests (20 μg) were diluted on ice with cold binding buffer (4 °C, 50 mmol/L magnesium acetate, 250 mmol/L ammonium acetate, pH 8.1) to a final volume of 300 μL. The sample was loaded on a polypropylene column (1 mL) filled with mAPBA (1 mL bed volume) and washed with cold binding buffer (14 mL). Amadori peptides were eluted in two steps with acetic acid (0.1 mol/L, 7 mL and then 0.2 mol/L, 1 mL) at 37 °C. Eluates were lyophilized, mixed with aqueous acetonitrile (20 %, v/v; 2× 0.5 mL), transferred to polypropylene tubes, lyophilized, and stored at –20 °C.
Solid phase extraction (SPE)
Lyophilized samples were dissolved in a mixture of aqueous acetonitrile (20 %, v/v; 12.5 μL) and formic acid (0.1 %, v/v; 87.5 μL) and loaded on C18-gel loader StageTips pre-equilibrated with aqueous acetonitrile (2.5 %) containing formic acid (0.1 %; eluent A). The column was washed with eluent A (150 μL) before the peptides were eluted with aqueous acetonitrile (60 %) containing formic acid (0.1 %; eluent B). The fractions were dried under vacuum and stored at –20 °C.
nanoUPLC-ESI-LTQ-Orbitrap-MS
Samples were dissolved in aqueous acetonitrile (3 %, v/v; 50 μL). Aliquots (10 μL) were loaded on a nanoAcquity UPLC Symmetry trap column (5 μL/min, 5 min) and separated on a nanoAcquity UPLC BEH130 column (30 °C) using a nanoAcquity UPLC System equipped with an Acquity sample manager (10 μL injection volume, full loop injection) and a nanoAcquity UPLC binary solvent manager (Waters GmbH). Eluents A and B were water and acetonitrile, respectively, both containing 0.1 % formic acid (v/v). The analytes were eluted with linear gradients from 3 % to 50 % (45 min duration) and 50 % to 85 % eluent B (2 min) at a flow rate of 0.4 μL/min. The column was connected to a PicoTip on-line nano-ESI emitter interfaced to the nanoESI source of an LTQ Orbitrap XL ETD mass spectrometer operated in positive ion mode and controlled by Xcalibur 2.0.7 software (Thermo Fisher Scientific, Bremen, Germany). Mass spectra were acquired in the Orbitrap at a resolution of 60.000. Tandem mass spectra (MS/MS) were recorded for the six most intense signals (z ≥ 2) of an Orbitrap survey scan by data-dependent acquisition (DDA) in the linear ion trap (LIT). Tandem mass spectra were analyzed with Sequest against the SwissProt database using Proteome Discoverer 1.1.0.263 (Thermo Fisher Scientific). Amadori peptides were manually confirmed [26] and annotated by their retention times (tR), m/z values, and sequences. Relative label-free quantification relied on integration of extracted ion chromatograms (XICs) (m/z ± 0.02) at the expected retention times. The specific settings of the ion source, mass analyzer, DDA, and database search are presented in ESM Table S-1.
Results
Analytical strategy
The analysis of glycation sites that are of low abundance in human plasma requires large plasma amounts that are not easily available for routine diagnostics [27]. Thus, we optimized and downscaled our analytical strategy first to identify and quantify individual Amadori peptides in tryptic digests. This protocol relies basically on enrichment by boronic affinity chromatography and nanoRPC-ESI-MS/MS (Fig. 2) [24].

Scheme of the optimized analytical strategy for relative quantification of Amadori peptides in trypsin-digested plasma samples obtained from T2DM patients and normoglycemic individuals
The effective tryptic digestion of plasma samples as a major prerequisite for sensitive analyses was evaluated by the intensity of the HSA band in SDS-PAGE. As plasma samples were not sufficiently digested after reduction and alkylation (data no shown), we tested existing denaturation strategies that use urea or SDS and reduction with DTT or TCEP [28–30]. Urea did provide quantitative digestion independent of the reducing agent, enzyme-substrate ratio, addition of CaCl2, or repetitive addition of fresh trypsin solutions, though TCEP provided better results than DTT (see ESM, Figures S-1A and S-1B). Although the HSA band was not detected in the digest (5 h, 37 °C) after treating the plasma sample with SDS and TCEP [30] (see ESM, Figure S-1C), undigested HSA was still visible when the sample was reduced with DTT (see ESM, Figure S-1D). Considering the sensitivity of the gel stain in the low ng-range (see ESM, Figure S-2) [31] and the absence of the HSA band (~1 μg in the sample), the digestion efficiency after reduction with TCEP was better than 99 %.
RPC conditions were optimized with a pooled nondiabetic plasma sample that was predigested (20 ng loaded) for peak capacities and peak heights of three intense HSA peptides eluting at early, medium, and late retention times. Expectedly, fast slopes (3 % and 1.5 %/min) provided maximal peak heights and, thus, high sensitivities (see ESM, Figure S-3A), whereas shallower gradients achieved better separations (see ESM, Figure S-3B). As an optimal condition, a linear 45-min gradient from 3 % to 50 % aqueous acetonitrile was used for further experiments.
Identification of glycation sites
Glycated peptides were identified in digested plasma samples obtained from five T2DM patients and four nondiabetic individuals by a survey Orbitrap-MS scan followed by acquisition of DDA-based tandem mass spectra. The number of identified peptides was increased by gas phase fractionation (GPF) [32] using mass ranges m/z 400 to 600, m/z 600 to 800, and m/z 800 to 1500. Data confidence could be further increased by analyzing each sample for a second time excluding all m/z-values of previously identified peptides, e.g., peptides nonspecifically retarded by BAC [33] (exclusion list in ESM, Table S-2). Glycated peptides were identified first by the characteristic neutral loss pattern of the sugar moiety (Fig. 3) [26], i.e., strong losses of two and three water molecules, corresponding to oxonium and pyrylium ions, respectively (see ESM, Figure S-4). Signals corresponding to furylium ions (loss of 3× H2O and HCHO) were typically weak. Sequences were retrieved from usually abundant b- and y-fragment ion series, which were often accompanied by the same neutral losses as described for the precursor ion, confirming the glycation status and allowing a reliable identification of the modified residue (Fig. 3B). These neutral losses, however, increased the number of m/z signals significantly, reducing the confidence scores of automatic peptide identification. Thus, all peptides and glycation sites were manually confirmed from the tandem mass spectra. In total, we could identify 52 glycated peptides in T2DM plasma representing 47 glycated lysine residues in 12 proteins (see ESM, Table S-3). All Amadori peptides were annotated by their retention times on nanoRP-UPLC (tR) and exact masses (mass accuracy ≤5 ppm) (Fig. 3).

Total ion current (TIC) chromatogram (A) and tandem mass spectrum (B) of peptide VFDEFKAmPLVEEPQNLIK recorded on a nanoRP-UPLC-ESI-Orbitrap-MS with the DDA triggered for signal m/z 736.4 (z = 3). The inset shows the XIC of m/z 736.39 ± 0.02. Pyrylium ions of b-and y-series are marked with asterisks
Relative quantification of Amadori peptides
For quantification of the 52 Amadori peptides, it was sufficient to digest only 25 μg plasma proteins and enrich them by BAC. Owing to the high salt content and large fraction volumes of the BAC, it was advantageous to desalt and enrich the samples first by solid-phase extraction before analyzing them by nanoUPLC-ESI-Orbitrap-MS. As the maximal sample transfer from the first (BAC) to the second dimension (RPC) is limited by the linear range of the most intense signal to be quantified, we analyzed equal volumes of a serially diluted enriched plasma digest (20 μg) immediately after BAC. The upper limit of the linear range was reached first for peptide KAmQTALVELVK (HSA-K525) when 10-fold diluted, i.e., injecting an aliquot corresponding to an original plasma protein amount of 2 μg. All following analyses relied on tryptic digests of 20 μg plasma proteins and transferring 10 % of the SPE eluate to the second dimension for relative quantification of glycated peptides using the peak areas at specified retention times in the XICs (Fig. 2). Indeed, all analyses were within the linear dynamic range, as indicated by the peak areas of six Amadori peptides using a sample dilution series (see ESM, Table S-4). Thus, XICs (m/z ±0.02) of all identified Amadori peptides (Fig. 3A) were integrated by Xcalibur (for the improvement of resolution after mass extraction, see Fig. 3).
Intra- and interday precisions of nanoRPC-ESI-MS analyses were determined with a tryptic HSA digest by integrating the peak areas of peptide signals m/z 773.90, 409.54, and 829.40 eluting in the most populated part of the RPC around 17 to 30 min (Fig. 3A) on three nonconsecutive days. The intraday precisions (expressed as relative standard deviation, RSD%) were 11 % to 27 % for the peak areas and 0.2 % for the retention times (see ESM, Table S-5). In spite of the fluctuation in interday precision, the data provided a meaningful and reproducible estimate of Amadori peptides in human plasma. Similarly, intra- and interday precisions were determined for three plasma peptides of different signal intensities eluting in the middle of the gradient (pooled plasma of four healthy individuals) indicating that possible matrix effects were reproducible and did not interfere with the analytes, i.e., no suppression or enhancement effects due to co-elution of multiple peptides (see ESM, Table S-5).
The tryptic digestion was highly reproducible within 1 d, as its intraday precision on 3 nonconsecutive days was similar to the precision of the nanoUPLC-ESI-MS, but the interday precision was significantly worse (see ESM, Table S-5). The precision of the complete analytical strategy consisting of sequential tryptic digestion, BAC enrichment, and nanoUPLC-ESI-Orbitrap-MS was determined for the same pooled plasma sample on 3 nonconsecutive days considering three glycated HSA peptides: LAKAmTYETTLEK (residues K351, m/z 486.92 ± 0.02), KAmQTALVELVK (K525, 645.88 ± 0.02), and KAmVPQVSTPTLVEVSR (K414, 601.34 ± 0.02). The intra- and interday precisions of the peptide quantities were 43 % to 66 % and 60 % to 76 %, respectively (see ESM, Table S-5), which were not influenced by using different chromatography columns for BAC (RSD% = 62 %, see ESM, Tables S-5 and S-2).
Relative quantification of Amadori peptides in plasma
The above validated quantitative approach was applied to analyze protein glycation profiles in plasma samples obtained from five T2DM patients (HbA1c content >6.5 %) and four nondiabetic controls (HbA1c content ≤6.5 %) matched for age, gender, and BMI. To achieve a high precision, all samples were prepared in parallel and analyzed in one batch. The peak areas of all 52 Amadori peptides were calculated from the corresponding XICs (see ESM, Table S-3) and divided by a Mann-Whitney U-test in three groups (Table 1): (1) five peptides detected only in T2DM plasma, (2) 15 peptides present in T2DM plasma at significantly higher levels than in control plasma samples, and (3) 32 peptides detected in T2DM and control plasma samples at similar intensities. The first two groups represented 19 glycation sites (two peptides corresponded to one glycation site) in six proteins, which appear to be diagnostically interesting. Approximately half of these glycated lysine residues were assigned to HSA. The peak areas of all 47 peptide signals of groups 2 and 3 were within the linear range in T2DM plasma (see ESM, Table S-4). In the control samples, however, nine peptides of group 2 were below their limits of quantification (LOQs). Thus, minimal increase factors ranging from 4 to 45 were calculated for these nine peptides using the ratio between the signals in the T2DM samples and LOQ determined for each peptide in the control samples.
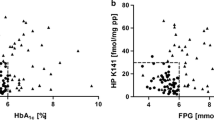
Among the 32 glycated peptides of group 3 (30 glycation sites in eight proteins, see ESM, Table S-6) present in T2DM and control samples at similar levels were 19 peptides present at similar quantities in all analyzed samples independent of the disease (Fig. 4C and ESM Figure S-5 and Table S-6). Interestingly, 13 glycated peptides (12 glycation sites in seven proteins, see ESM, Table S-6) were present at higher quantities in some T2DM plasma digests than in the controls and the other T2DM samples (Fig. 4B and ESM Figure S-5).

Peak areas obtained for HSA peptides VFDEFKAmPLVEEPQNLIK (A), KAmLVAASQAALGL (B), and KAmYLYEIAR (C) in digested plasma samples obtained from T2DM patients and nondiabetic individuals. Statistical differences were determined by the Mann-Whitney U test and p-values below 0.05 were considered as significant
Discussion
HbA1c is a well-established marker to monitor a patient’s glucose blood level over a 3-mo period. Considering the incidence of diabetes mellitus and the medical need to improve its diagnosis and prognosis, it appears surprising that glycation sites in other plasma proteins have only been suggested as potential biomarkers but not yet investigated in detail for their quantitative changes. This is probably due to the analytical challenges caused by the supposedly high number of expected glycation sites (i.e., theoretically all accessible lysine residues) and the relatively low degree of glycation. More importantly, it is generally assumed that the glycation degrees of different sites depend on the body glucose level and, thus, will change equally with a patient’s clinical parameters. If this were true, all glycation sites would be of similar diagnostic and prognostic value. Recent reports from us and other laboratories, however, indicate that glycation levels at different sites might not solely depend on the glucose sugar level but also the individual glycation site [21, 24]. A recent study aiming for the identification of glycation sites in plasma proteins revealed 2205 fructosamine-modified peptides representing 1095 glycated proteins in enzymatic digests of pooled plasma samples from diabetic patients and nondiabetic controls [21]. This was achieved by enriching glycated peptides by BAC, separating them by ion exchange chromatography (IEC), and then analyzing them by RPC-ESI-MS/MS. Interestingly, several glycation sites were detected solely or at higher levels in the pooled diabetic plasma sample [21, 34], which clearly indicates that glycation sites might be diagnostically informative in addition to HbA1c levels The clinical utility of the technology remains to be validated because only one pooled plasma sample instead of samples from several individual subjects were analyzed. Furthermore, the accuracy of label-free quantification by spectral counting is still controversially debated [27]. Our study relied on a chromatographic analysis to address two important issues: (1) Do blood glucose levels influence the glycation pattern of all proteins at similar degrees as HbA1c or is it site specific, and (2) do individuals within a T2DM cohort possess different glycation patterns?
Considering the potential diagnostic value, the current study focused on ‘dominant’ glycation sites of abundant plasma proteins directly by well-established diagnostic strategies such as mass spectrometry or immunoassays. Consequently, 52 tryptic Amadori peptides were relatively quantified in small cohorts of T2DM patients and normoglycemic individuals matched for gender, age, and BMI (Fig. 2). This selection allowed a simplified analytical strategy without the need for a third chromatographic separation, such as IEC, as applied in an earlier study on glycation sites in human plasma [21]. Eliminating IEC should improve the precision of the analysis, which is already relatively low for label-free quantification [6, 27]. Another critical step is tryptic digestion, which is challenging in complex sample matrices, such as plasma, which vary much among individuals [28]. In our hands, denaturation with chaotropic agents (e.g., urea) [29, 30] was less efficient than with SDS [31, 32] because SDS is mostly removed by BAC and, thus, does not disturb the ensuing LC-MS. Longer alkyl-chain contaminations often present in SDS, which irreversibly bind to C18-phases, would be efficiently removed by SPE, thus preventing contamination of the LC-column.
To our knowledge, only position K574 present in the C-terminal peptide KAmLVAASQAALGL of HSA was new, whereas the other 23 HSA glycation sites have been reported [24, 34]. Among the glycation sites detected in other plasma proteins were 20 described before [21, 34], whereas K98 in Ig λ chain C region, K508 in serotransferrin, and K1325 in complement C3 appear to be new.
Moreover, the data clearly show that diabetic conditions have different effects on different glycation sites: 19 sites in six proteins were glycated at significantly higher levels (p < 0.05) in T2DM than in the normoglycemic samples (including five unique positions, Table 1), whereas all other glycation sites were not affected by diabetic conditions. Hence, the glycation degrees of less than 40 % of the studied glycation sites were increased in T2DM. Remarkably, nine of the 11 differentially glycated HSA peptides were previously detected at similar abundances in different diabetic subjects [24].
Among the 20 peptides detected at higher signal intensities in digests of T2DM plasma samples than in age-matched control samples, only three have been reported (sequences 16, 18, and 25, Table 1) [34]. The increased number of peptides indicating increased glycation levels in T2DM plasma might be related to the analysis of individual samples instead of pooled samples in the previous study. Additionally, our relative quantification did not rely on spectral counting, which is considered less reliable [27]. The overall assay precision achieved here (see ESM, Table S-5) provided a confident statistical significance for peptide quantities changed at least 2-fold (i.e., 3× RSD), which was true for all peptides shown in Table 1. These Amadori peptides can be considered as prospective biomarkers of diabetes mellitus with the HSA peptides being specifically interesting for middle-term glycemic control because of the half-life time of HSA (~20 d) compared with hemoglobin present in red blood cells with a life span of around 3 mo. The sensitivity of these potential markers needs to be compared with conventional assays for glycated HSA [16–18, 35].
From the remaining glycation sites with no significant differences between disease and control groups, a set of peptides displayed highly intense signals for most T2DM patients and low intensities in the majority of controls (Fig. 4B, and ESM Figure S-5 and Table S-6). The biological background and clinical relevance of such alterations need to be further investigated using more plasma samples from larger cohorts. Additionally, the precision of the analysis needs to be increased. As BAC is the major source of abundance dispersion, plasma digests should be spiked with synthetic Amadori peptides as internal standards. Additionally, the sensitivity and the precision can be increased by switching to LC-MS/MS-based techniques, such as multiple reaction monitoring (MRM).
Concluding remarks
As current protein glycation markers are not sensitive enough to short-term fluctuations of the blood glucose levels, we have studied 52 Amadori peptides representing 12 abundant plasma proteins in patients with T2DM and normoglycemic individuals. Glycation levels of more than 60 % of the glycation sites were only slightly affected by the disease, and the rest of the sites were glycated at higher levels in T2DM patients. Based on these differences, the glycation sites can be classified in four groups: (1) five peptides detected only in T2DM and representing a reliable basis of clinical diagnostics of T2DM, (2) 15 peptides detected in T2DM at more than 2-fold higher intensities confirming the results obtained in group (1), (3) 13 peptides present at higher levels in most T2DM samples but at the control level for others, and (4) 19 peptides detected at similar or slightly elevated levels in the diabetic samples. The first two groups represented by 20 Amadori peptides are clearly promising biomarkers and confirm the justification of further validation of the technology. Furthermore, the 13 peptides listed in the third group appear interesting, as they might allow subdividing diabetes patients for better dietary control or therapy.
References
Ulrich P, Cerami A (2001) Protein glycation, diabetes, and aging. Recent Prog Horm Res 56:1–21
Hodge JE (1955) The Amadori rearrangement. Adv Carbohydr Chem 10:169–205
Grillo MA, Colombatto S (2007) Advanced glycation end-products (AGEs): involvement in aging and in neurodegenerative diseases. Amino Acids 35:29–36
Ahmed N, Thornalley PJ (2007) Advanced glycation endproducts: what is their relevance to diabetic complications? Diabetes Obes Metab 9:233–245
Hartog JW, Voors AA, Bakker SJ, Smit AJ, van Veldhuisen DJ (2007) Advanced glycation end-products (AGEs) and heart failure: pathophysiology and clinical implications. Eur J Heart Fail 9:1146–1155
Li J, Liu D, Sun L, Lu Y, Zhang Z (2012) Advanced glycation end products and neurodegenerative diseases: mechanisms and perspective. J Neurol Sci 317:1–5
Price CL, Knight SC (2007) Advanced glycation: a novel outlook on atherosclerosis. Curr Pharm Des 13:3681–3687
Thornalley PJ, Rabbani N (2009) Highlights and hotspots of protein glycation in end-stage renal disease. Semin Dial 22:400–404
Giacco F, Brownlee M (2010) Oxidative stress and diabetic complications. Circ Res 107:1058–1070
Schleicher ED, Vogt BW (1990) Standardization of serum fructosamine assays. Clin Chem 36:136–139
Karachalias N, Babaei-Jadidi R, Ahmed N, Thornalley PJ (2003) Accumulation of fructosyl-lysine and advanced glycation end products in the kidney, retina, and peripheral nerve of streptozotocin-induced diabetic rats. Biochem Soc Trans 31:1423–1425
Gabbay KH, Hasty K, Breslow JL, Ellison RC, Bunn HF, Gallop PM (1977) Glycosylated hemoglobins and long-term blood glucose control in diabetes mellitus. J Clin Endocrinol Metab 44:859–864
Furusyo N, Koga T, Ai M, Otokozawa S, Kohzuma T, Ikezaki H, Schaefer EJ, Hayashi J (2011) Utility of glycated albumin for the diagnosis of diabetes mellitus in a Japanese population study: results from the Kyushu and Okinawa Population Study (KOPS). Diabetologia 54:3028–3036
Ionescu-Tirgoviste C, Guja C, Ioacara S, Dumitrescu D, Tomescu I (2004) Continuous glucose monitoring: physiologic and pathophysiologic significance. Rom J Intern Med 42:381–393
Koga M, Murai J, Saito H, Kasayama S (2010) Glycated albumin and glycated hemoglobin are influenced differently by endogenous insulin secretion in patients with type 2 diabetes. Diabetes Care 33:270–272
Baker JR, Metcalf PA, Johnson RN, Newman D, Rietz P (1985) Use of protein-based standards in automated colorimetric determinations of fructosamine in serum. Clin Chem 31:1550–1554
Kouzuma T, Usami T, Yamakoshi M, Takahashi M, Imamura S (2002) An enzymatic method for the measurement of glycated albumin in biological samples. Clin Chim Acta 324:61–71
Schleicher E, Wieland OH (1981) Specific quantitation by HPLC of protein (lysine) bound glucose in human serum albumin and other glycosylated proteins. J Clin Chem Clin Biochem 19:81–87
Ikeda K, Sakamoto Y, Kawasaki Y, Miyake T, Tanaka K, Urata T, Katayama Y, Ueda S, Horiuchi S (1998) Determination of glycated albumin by enzyme-linked boronate immunoassay (ELBIA). Clin Chem 44:256–263
Shima K, Ito N, Abe F, Hirota M, Yano M, Yamamoto Y, Uchida T, Noguchi K (1988) High-performance liquid chromatographic assay of serum glycated albumin. Diabetologia 31:627–631
Zhang Q, Monroe ME, Schepmoes AA, Clauss TR, Gritsenko MA, Meng D, Petyuk VA, Smith RD, Metz TO (2011) Comprehensive identification of glycated peptides and their glycation motifs in plasma and erythrocytes of control and diabetic subjects. J Proteome Res 10:3076–3088
Rondeau P, Bourdon E (2011) The glycation of albumin: structural and functional impacts. Biochimie 93:645–658
Barnaby OS, Cerny RL, Clarke W, Hage DS (2011) Comparison of modification sites formed on human serum albumin at various stages of glycation. Clin Chim Acta 412:277–285
Frolov A, Hoffmann R (2010) Identification and relative quantification of specific glycation sites in human serum albumin. Anal Bioanal Chem 397:2349–2356
Bradford MM (1976) A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem 72:248–254
Frolov A, Hoffmann P, Hoffmann R (2006) Fragmentation behavior of glycated peptides derived from D-glucose, D-fructose and D-ribose in tandem mass spectrometry. J Mass Spectrom 41:1459–1469
Bantscheff M, Schirle M, Sweetman G, Rick J, Kuster B (2007) Quantitative mass spectrometry in proteomics: a critical review. Anal Bioanal Chem 389:1017–1031
Strader MB, Tabb DL, Hervey WJ, Pan C, Hurst GB (2006) Efficient and specific trypsin digestion of microgram to nanogram quantities of proteins in organic-aqueous solvent systems. Anal Chem 78:125–134
Bollineni RC, Hoffmann R, Fedorova M (2011) Identification of protein carbonylation sites by two-dimensional liquid chromatography in combination with M. J Proteom 74:2338–2350
Zhang Q, Schepmoes AA, Brock JW, Wu S, Moore RJ, Purvine SO, Baynes JW, Smith RD, Metz TO (2008) Improved methods for the enrichment and analysis of glycated peptides. Anal Chem 80:9822–9829
Anderson L, Hunter CL (2006) Quantitative mass spectrometric multiple reaction monitoring assays for major plasma proteins. Mol Cell Proteom 5:573–588
Zhang N, Li L (2004) Effects of common surfactants on protein digestion and matrix-assisted laser desorption/ionization mass spectrometric analysis of the digested peptides using two-layer sample preparation. Rapid Commun Mass Spectrom 18:889–896
Frolov A, Hoffmann R (2008) Analysis of Amadori peptides enriched by boronic acid affinity chromatography. Ann NY Acad Sci 1126:253–256
Zhang Q, Tang N, Schepmoes AA, Phillips LS, Smith RD, Metz TO (2008) Proteomic profiling of nonenzymatically glycated proteins in human plasma and erythrocyte membranes. J Proteome Res 7:2025–2032
Acharya AS, Manning JM (1980) Amadori rearrangement of glyceraldehyde-hemoglobin Schiff base adducts. A new procedure for the determination of ketoamine adducts in proteins. J Biol Chem 255:7218–7224
Acknowledgments
Financial support from Deutsche Forschungsgemeinschaft (HO-2222/9-1) is gratefully acknowledged.
Conflict of interest statement
The authors have declared no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 2.20 mb)
Rights and permissions
About this article

Cite this article
Frolov, A., Blüher, M. & Hoffmann, R. Glycation sites of human plasma proteins are affected to different extents by hyperglycemic conditions in type 2 diabetes mellitus. Anal Bioanal Chem 406, 5755–5763 (2014). https://doi.org/10.1007/s00216-014-8018-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-014-8018-y