
Abstract
Human biomonitoring (HBM) is a scientific technique that allows us to assess whether and to what extent environmental pollutants enter humans. We review here the current HBM efforts for organophosphate esters, emerging flame retardants, perfluoroalkyl substances, and phthalate esters. Use of some of these chemicals has already been banned or restricted; they are regularly detected in the environment, wildlife, and human matrices. Traditionally, blood and urine collection have been widely used as sampling methods. New non-invasive approaches (e.g., saliva, hair, nails) are emerging as valid alternatives since they offer advantages with respect to sampling, handling, and ethical aspects, while ensuring similar reliability and sensitivity. Nevertheless, the identification of biomarkers of exposure is often difficult because chemicals may be metabolized in the human body. For many of the above-mentioned compounds, the mechanisms of the favorable metabolization pathways have not been unraveled, but research on important metabolites that could be used as biomarkers of exposure is growing. This review summarizes the state of the art regarding human exposure to, (non-invasive) HBM of, and metabolism of major organophosphate esters, emerging flame retardants, perfluoroalkyl substances, and phthalate esters currently detected in the environment.

Human biomonitoring of emerging contaminants-non-invasive versus invasive matrices
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The presence of a wide array of man-made chemicals in consumer goods and health care products has attracted the attention for the inherent health risks to humans resulting from long-term exposure to these products. According to a World Health Organization report from 2009, 10 % of deaths and disease burdens are due to environmental factors (e.g., smoking) [1]. However, in a recent review, the estimate was significantly higher (about 40 % of human deaths in the world, amounting to around 62 million per year) and was attributed mainly to exposure to several hazardous pollutants [2]. In 2001, the Stockholm Convention was enacted to urgently find alternatives to control and reduce exposure [3], and thus its main aim was to protect humans and the environment against exposure to hazardous chemicals by reducing and/or eliminating their production and/or introduction on the market. A list of the most hazardous persistent organic pollutants was compiled, and has been amended several times [4, 5]. The last actualization in 2011 comprised 22 chemicals [5]. However, some of the most dangerous chemicals are the so-called endocrine-disrupting chemicals, such as the phthalate esters (PEs), organophosphate esters (OPEs), perfluoroalkyl substances (PFASs), and flame retardants (FRs); most of them are not (yet) on the Stockholm Convention list. These compounds are potentially harmful, being able to interfere with the synthesis, metabolism, and action of endogenous hormones and thus leading to various adverse biological effects, including endocrine-disrupting activity, and promotion of carcinogenicity, neurotoxicity, reproductive toxicity, hepatoxicity, and teratogenicity [6–11].
With the introduction of a new regulation dealing with the registration, evaluation, authorization and restriction of chemicals (REACH) in Europe in 2006, certain dangerous substances and preparations (including azo dyes, N,N-dimethylformamide, polycyclic aromatic hydrocarbons, and PEs) which are present on the EU market had their use restricted [12]. To replace those banned chemicals, a range of substitutes were introduced; yet the exposure sources, occurrence, and metabolism are still largely unknown [13–15].
Human biomonitoring (HBM) is a tool to map exposure patterns to environmental xenobiotics throughout the population over time. HBM also allows modeling of compound behavior and assessment of the potential toxicological impact (pharmacokinetic processes), which is crucial for characterizing exposure, assessing risk, and informing policy makers [16–20] (Fig. 1). Hence, health authorities can establish rules and regulations to avoid and/or reduce the risk of exposure to hazardous substances, specifically in groups at a high level of risk (e.g., pregnant women, mothers during the lactation period, infants, children, seniors, workers in industrial environments) [21]. HBM studies are based on the analysis of environmental contaminants and/or biomarkers of exposure in human tissues or biological fluids. Interpretation is often a complex undertaking once these chemicals are detected at low levels or quickly biotransformed into different kinds of metabolites. Further, not only the levels but also the half-lives and the metabolism of contaminants (metabolic pathways, type and amount of metabolites generated) are important factors to consider when assessing human exposure. Through identification of biomarkers of human exposure, it is possible to indicate susceptibilities or predict the incidence of outcome lesions [16, 19]. Nevertheless, biomarkers of effect and biomarkers of susceptibility are also important to assess the impact of the exposure [22]. In the last two decades, the increased number of HBM studies has generated more understanding about the bioaccumulation, metabolism, excretion, and toxic effects of pollutants and their metabolites in humans [16]. Similarly to limits for food and environmental matrices [3, 23], risk-assessment-based biomarker screening values, including biomonitoring equivalents [24] and HBM values from the German Human Biomonitoring Commission [25], are available for more than 130 analytes, including some PEs, perfluorooctanoic acid (PFOA), and perfluorooctane sulfonic acid (PFOS).

Continuous exposure effect for environmental chemicals [16]
The indroduction of non-invasive matrices brought new trends in HBM, and here we review the newest aspects for OPEs, PEs, PFASs, and emerging FRs (EFRs). The relevance of HBM approaches for each class is discussed, including a brief description of the physicochemical properties and major metabolites (Table 1). Additionally, we aimed at (1) highlighting the main exposure sources, (2) summarizing previous HBM studies of OPEs, PEs, PFASs, and EFRs and their metabolites using non-invasive versus invasive matrices, (3) indicating the main in vitro metabolites and the analogies between in vitro and in vivo metabolic pathways, (4) discussing the analytical methods used to analyze each group of pollutants, and (5) identifying research gaps and suggesting future developments for HBM focusing on non-invasive methods.
Chemicals in need of biomonitoring
Organophosphate esters
OPEs are used as additive FRs, as plasticizers in some polymers, and also in pesticide formulations, paints, varnishes, lubricants, and textile coatings among other applications [8, 29, 52, 53]. These chemicals consist of a phosphate group that links several aliphatic and/or organic substituents. More recently, polybrominated diphenyl ethers (PBDEs) commonly used as FRs were replaced by OPEs, which are usually less persistent in the environment. However, this does not mean that OPEs are less toxic or have low bioaccumulation in the environment. Most OPEs have high log K ow, but are less lipophilic than the brominated FRs (BFRs) [53]. Table 1 lists the physicochemical properties for five OPEs and their respective metabolites. Following human metabolism, OPEs are mainly excreted in urine after transformation to more hydrophilic metabolites [54–56]. There are several studies on OPEs and/or metabolites in environmental samples (air, dust, water) and humans [54, 57–60].
OPEs have structures similar to those of the organophosphorus insecticides; members of the latter group inhibit the enzyme acetylcholinesterase [61, 62], thus causing acute neurotoxic effects such as convulsions, asphyxia, and even death [63, 64].
Phthalate esters
PEs are synthetic chemicals produced and used worldwide since the 1920s [65] as plasticizers and additives in household and textile products, toys, personal-care products, furniture upholstery, blood storage bags, and medical devices [20]. Their use depends on their alkyl chain length, which can range from three to ten carbon atoms [9, 66–68]. According to the chemical structure, PEs are classified in two groups:
-
1.
High molecular weight (long chain, more than seven carbons atoms): including diisononyl phthalate, diisodecyl phthalate, di-n-octyl phthalate, and di-2-ethylhexyl phthalate (DEHP).
-
2.
Low molecular weight (short chain with three to six carbon atoms): including dibutyl phthalate (DBP), diethyl phthalate (DEP), dimethyl phthalate, butyl benzyl phthalate (BBzP), di-n-butyl phthalate (DnBP), and diisobutyl phthalate (DiBP).
In general, the long-chain PEs are less toxic to humans than are the short-chain compounds, which are classified as very dangerous substances in the REACH regulation [69, 70]. However, application limitations groups were established for both, indicating that these chemicals “shall not be used as substances or as constituents of preparations, at concentrations higher than 0.1 % by mass of the plasticized material, in toys and childcare articles” [69]. Both DEHP and DBP are considered reproductive toxicants [69]. It is planned that after August 2015, low molecular weight PEs will only be produced and sold under a specific REACH authorization (Annex XIV of 21 November 2012) [70]. Various toxic effects in humans and animals, including reproductive toxicity, carcinogenicity, and endocrine disruption, have been reported [8, 9]. PEs are ubiquitous in indoor and outdoor environments, and are the most difficult factor to control, representing a large contribution to human exposure to PEs [67]. On the other hand, exposure through personal-care products or food, which may have also a large contribution to human intake, can be controlled. Most studies have reported the levels of PEs in human matrices as metabolites (especially in urine or human milk) because of their fast hydrolysis and subsequent oxidation [36, 71, 72]. The main physicochemical properties of PEs and their known metabolites are presented in Table 1.
Perfluoroalkyl substances
PFASs are chemicals with an alkyl chain partly (poly) or fully (per) fluorinated substituted with different functional groups. This group comprises perfluoroalkyl carboxylic acids, perfluoroalkyl sulfonic acids, perfluoroalkyl sulfonamides, perfluoroalkyl sulfonamidoethanols, and fluorotelomer alcohols, which are polyfluorinated compounds [73, 74].
The chemical and temperature stability as well as good surface-tension-lowering properties and the ability to create stable foams led to the widespread use of PFASs in numerous products, such as stain repellents, insecticides, cosmetics, paints, coatings, aqueous film-forming foams, polishes, electronic devices, food packaging, and adhesives [15, 74–76]. Moreover, the perfluoroalkyl chains in PFASs are considerably more hydrophobic than alkyl chains and are substantially hydrophilic as well; these properties can change depending on the number of fluorine substituents in the carbon backbone [77, 78], which makes them ideal for surface treatments (e.g., use of polytetrafluoroethylene in many nonstick coatings for cookware and even in paper coatings) [76]. Following their widespread use, a wide range of PFASs have been detected in the environment, wildlife, food, and humans [76, 79–86], suggesting that they leak from their application products and are stable/persistent in the environment.
Since 2009, the use of PFOS, its salts, and perfluorooctane sulfonyl fluoride for the production of consumer goods has been regulated by the Stockholm Convention [4]; however, there is no restriction on the incorporation of other PFASs in consumer goods. Still, restriction of their use for specific purposes was set out in the Stockholm Convention, for instance, for the manufacture of textiles and upholstery, paper and packaging, coatings and coating additives, rubber, and plastics [87]. Directive 2006/112/EC [88] placed restrictions on the marketing and use of PFOS, and although it was also stated that PFOA and its salts are suspected of having a risk profile similar to that of PFOS, no restrictions have been imposed on their use. HBM of long-chain PFASs has been extensively explored in recent years, since there is a higher bioaccumulative effect than for short-chain analogues [2, 86, 89–93]. Therefore, in this review, the discussion will focus on HBM studies of perfluoroalkyl sulfonates and perfluoroalkyl carboxylic acids (Table 1) owing to their greater relevance for human exposure and health risk assessment [94].
Flame retardants
FRs are generally divided into halogenated organic (brominated or chlorinated), phosphorus-containing, nitrogen-containing, and inorganic FRs [6]. The halogenated FRs, especially BFRs, are the most popularly used owing to their low cost and better performance compared with other FRs [6, 7]. However, concerns about persistency, bioaccumulation, and toxicity have led to the addition of some FRs to the Stockholm Convention list, for example, PBDEs and hexabromocyclododecane (HBCD) [3, 7]. These chemicals are additives or reactive components in polymers that were used as raw materials for consumer products (computers, electronics and electrical equipment, textiles, foams, furniture, etc.) [6, 7, 10]. EFRs such as decabromodiphenyl ethane (DBDPE), 1,2-bis(2,4,6-tribromophenoxy)ethane (BTBPE), 2-ethylhexyl-2,3,4,5-tetrabromobenzoate (TBB), bis(2-ethylhexyl)-3,4,5,6-tetrabromophthalate (TBPH), tetrabromobisphenol A bis(2,3-dibromopropyl ether), Dechlorane Plus (DP), and their congeners (Dechlorane 602, Dechlorane 603, and Dechlorane 604) were introduced to the market to replace some of the restricted FRs [13, 48] (Table 1).
Low biodegradability of some FRs leads to persistent accumulation in the environment and the food-chain [10, 48] and therefore in humans and wildlife. Several studies have reported their presence in air, soil, sediments, dust, and biota [13, 48, 95, 96], but only a few have described their presence in humans [97, 98]. Since these EFRs can undergo biotransformation reactions, metabolites can be excreted in urine. Native compounds are lipophilic and have bioaccumulative potential, as shown in several studies [99]. Among the toxic effects of BFRs already described are immunotoxicity, cytotoxicity, neurotoxicity, and endocrine disruptive activity [6, 7].
Human exposure
Human exposure is “an event that occurs when there is contact between humans and the environment with a contaminant of a specific concentration for an interval of time” [100]. External exposure is the concentration of a substance of concern in a pollution source or pathway to human exposure. Internal exposure is the total concentration of this substance and its metabolites within the human body, which indicates the total human burden of the exposure [101].
Ingestion, inhalation, and dermal absorption are the most contributive pathways of human exposure to chemicals, depending on their properties and commercial applications. The diet and dust are considered significant sources for human exposure. Although it is difficult to prevent and control human exposure to various chemicals, it is possible to estimate the dominant exposure routes for each class.
Humans are exposed to PEs via the diet and skin contact, as they are the main additives used in plastic containers, wrapping films, and personal-care products [67, 102]; food and drinking water are suggested to be the dominant exposure pathway for PFASs [103, 104]. FRs are commonly used in electronic items, textiles, and building materials, so there is a higher detection frequency in indoor air and dust than in food and/or drinks [13, 53, 105]. For OPEs two sources of human exposure are suggested: ingestion (e.g., food) and inhalation (e.g., air and dust) [8, 106].
Diet
Environmental pollution can lead to human dietary exposure through drinking water and food. PEs, OPEs, FRs, and PFASs were detected in surface water, most probably through inappropriate wastewater treatment or direct industrial discharges [58, 107–109]. The water pollution may eventually lead to human dietary exposure, for instance, some OPEs were detected in finished drinking water in the USA [110], and some secondary water treatment processes failed to efficiently remove chlorinated OPEs [111]. In the Faroe Islands, PFASs were found in both surface and drinking water [103]. Moreover, the pollution of surface water and seawater resulted in the bioaccumulation of pollutants in aquatic biota, for example, fish and seafood, which are part of the human diet [103, 112–116]. Also, contamination of the agricultural environment, such as water and soil, may lead to the transport of contaminants to food products (including meat, vegetables, oil, and egg), which will ultimately contaminate consumers [114].
Migration of pollutants during food processing, storage, and handling is another pathway that contributes to dietary exposure. PEs are plasticizers used in packaging products, and may migrate to foods and drinks during processing and storage [102, 117]. Another source of PE contamination is the use of PVC gloves for food preparation. Tsumura at al. [118] reported PVC gloves contained up to 41 % DEHP, 75 % diisononyl phthalate, and 28 % BBzP, which suggestively link to the contamination in final food products. Wormuth et al. [119] suggested that food ingestion is the dominant pathway of exposure to DEHP, DnBP, and DiBP. Because of the intensive use of and consequent exposure to PEs, some studies reported by the European Food Safety Authority revealed high human exposure through the diet, for example, for BBP the intake is between 0.008 and 0.02 mg per person per day; thus, the committee decided to set a tolerable daily intake of 0.1 mg kg−1 body weight for this compound [120].
Recently, several studies [15, 76, 103] confirmed that dietary intake (food and drinking water) may be the most important source of exposure to PFASs and particularly PFOS and PFOA; however, some authors are of the opinion that environmental sources (indoor air, dust) also have an important contribution to human exposure [82, 121]. Moreover, low quantities of PFASs were found in some food-contact products, such as nonstick cookware and oil-resisting coating paper [76]. Thus, to better understand whether food and drink intake are the main sources of human exposure, a study of the correlation between dietary intake and the levels of perfluorinated chemicals in human matrices and in nonhousehold sources (dust, air) should be performed.
Dust
Dust was proven to be suitable indicator of microenvironment contamination by several environmental pollutants, including BFRs, OPEs, PFASs, and PEs [13, 57, 121–125]. Significantly higher levels of PEs were observed in indoor dust samples (5–2,220 μg g−1) than in outdoor dust samples (2–870 μg g−1) [126]. Other studies showed that PFASs, emerging BFRs, and OPEs are present at microgram per gram levels in indoor dust [57, 123, 124, 127–129]. Ingestion is the main pathway of dust intake for toddlers, who tend to have more hand-mouth contact and close-to-floor activities [130, 131]. Dust intake was estimated to be, on average, around 20 and 50 mg per day for adults and toddlers, respectively, with maximum estimates for toddles as high as 200 mg per day [131]. Taking into account the time spent indoors suggests that dust intake might be a significant route of exposure to FRs and OPEs in humans. The levels of tris(1,3-dichloro-2-propyl) phosphate (TDCPP) and triphenyl phosphate (TPP) in dust correlated with those of TDCPP metabolites in urine, suggesting that higher dust levels of OPEs relate to higher internal exposure in humans. For TPP, the levels in dust and urine did not correlate [54].
Cornelis et al. [104] estimated that in the Flemish population, the PFOS and PFOA intake via dust ingestion was below 0.02 and 0.01 ng kg−1 body weight per day, respectively, and showed that dust intake of PFOS and PFOA was negligible compared with dietary intake (over 24 and 6 ng kg−1 body weight per day, respectively). Estimated exposure was further compared with the reference dose to assess the levels of safe exposure [131].
The size of dust particles may affect the magnitude of the exposure; therefore, more attention should be paid to dust with a fine particle size (less than 100 μm) [132], since it can be suspended in air or attach to skin. Not only does ultrafine dust (less than 63 μm) have higher bioaccessibility and cytotoxicity than coarse dust, but humans are also more easily exposed to it than to coarse dust (0.3–2 mm) [126]. Cao et al. [133] observed an ascendant trend of BFR concentration in dust with decreasing of particle size within the range 0.05–2 mm. The concentrations of BTBPE and PBDEs increased with a decrease in size, showing a drop at 40 μm, and reaching a peak at 20 μm. In comparison with indoor dust (100 ± 150 μm), hand dust has smaller particle size (30 ± 30 μm) and a narrower size distribution [133]. A similar size distribution (40 ± 30 μm) of dust was found on children’s hands in a Japanese study [134]. Humans seem to be at less risk from exposure to large dust particles, so more attention should be paid to fine dust exposure. Moreover, the selection of the particle size fraction of dust may also affect the accuracy and precision of assessing human exposure and the impact thereof [132].
Hand–mouth contact
Owing to frequent contact with the ambient environment, hands not only contribute to the dermal absorption of pollutants (see the next section), but also act as a transporter during hand-to-mouth contact. Any behavior that increase the frequency and extent of hand–mouth contact, such as nail biting, smoking, and eating food with the fingers may increase the risk of exposure to pollutants [135]. Stapleton et al. [135] differentiated BFR levels between adults and children by analyzing hand wipes. Other studies correlated the hand–mouth contact with FRs between hand wipes, indoor dust, and serum [135–137], and found that wipes are good biomarkers for FRs, especially PBDEs. The authors of the studies suggested that PBDEs can be either ingested or absorbed, or both [135, 137]. However, few articles have studied exposure to OPEs, PEs, emerging BFRs, and PFASs from hand–mouth contact.
Skin
The use of personal-care products plays an important role in dermal exposure to PEs, especially short-chain PEs, such as DEP and DBP, which can be found in beauty products, such as nail polishes and perfumes [138]. Consequently, women have a significantly higher risk of exposure to short-chain PEs than do men owing to more frequent use of personal-care products [67]. High urinary levels of monoethyl phthalate (MEP), a metabolite of DEP, were associated with the use of eye shadow, cologne, and skin-care products [68]. Some PFASs are also added to some cosmetics [139], but few studies have focused on the assessment of their dermal exposure.
Inhalation
Air and suspended dust are other important exposure pathways, especially for volatile compounds. Since FRs and PEs are physically mixed rather than chemically bonded with polymers, they tend to be slowly released from the polymeric matrix through evaporation or abrasion. Salthammer et al. [140] studied the transfer processes of TDCPP and tris(1-chloro-2-propyl) phosphate (TCPP) degradation products from different foams to air through determination of the area-specific emission rates by means of sealed emission-test chambers, and concluded that degradation products are indeed released from polymer-containing products to the air. The semivolatile organic contaminants tend to accumulate on the surface of aerosols and settled dust [141].
Inhalation of organic pollutants seems to be one of the major nondietary sources of human intake, for instance, for PEs which are more abundant in both indoor air and outdoor air [121] and for which inhalation exposure can account for 60–90 % of nondietary human exposure of more volatile PEs [126]. On the other hand, ingestion (about 36 %) of less volatile PEs via dust seems to be the preferential way for human uptake. Bergh et al. [14, 142] found high levels of PEs and OPEs in indoor air. Other studies have reported high levels of DP compounds, BFRs, and PFASs in environmental air samples, suggesting that inhalation can be an important source of intake of volatile and semivolatile compounds into the human body [125, 143–145].
Biomonitoring methods
Invasive methods
Blood is one of the most popular matrices used to determine biomarkers such as drugs, metals, and organic contaminants (e.g., PEs, pesticides, and polycyclic aromatic hydrocarbons) in the human body [17, 146–149]. Depending on the type of biomarker, measurements can be performed in whole blood, serum, plasma, or specific cell types (e.g., lymphocytes). The invasive nature of blood sampling has some important drawbacks: it negatively affects the participation rate of study participants, the amount of sample is often limited, and sampling in young children or infants has practical and ethical downsides. However, from a scientific point of view, blood has been the preferred matrix for many contaminants such as BFRs, polychlorinated biphenyls (PCBs), and pesticides [22] as it is a universal link between all tissues of the organism. Nevertheless, increasing efforts are being undertaken to find alternative (i.e., non-invasive) sampling methods to substitute for blood sampling [150, 151].
The concentrations of PFASs can be measured in serum/plasma, but quantifications in whole blood have also been reported [80, 152, 153]. Validation studies have shown that serum/plasma samples yield comparable results, whereas serum or plasma to whole blood ratios, regardless of the anticoagulant used, approximated 2:1 [154], suggesting that the PFASs are not found intracellularly or attached to red blood cells [154].
PFASs can cross the placenta, and therefore can be measured in umbilical cord blood [92]. In matching samples of maternal and umbilical cord blood, the levels of PFASs were found to be lower in umbilical cord blood, with fairly consistent ratios [155]. For PFOA, the mean levels in umbilical cord blood were approximately 60–70 % of those in maternal blood, with a umbilical cord blood to maternal blood ratio ranging between 0.55 and 0.81 in most studies [156]. For PFOS, the umbilical cord blood to maternal blood ratio ranged between 0.29 and 0.45. As an alternative to umbilical cord blood, some authors have suggested measuring the perinatal exposure to PFOS and PFOA in dried blood spots; that is, a sample of the baby’s blood that is obtained by a heel prick within 48 h after birth [81, 157]. These methods may allow temporal trends of PFOS and PFOA exposure to be studied by using historical samples of dried blood spots [158].
The levels of PFASs in human serum declined between 1976 and 2007, both in men and in women [63]. However, our understanding of PFAS bioaccumulation mechanisms (especially for long-chain compounds, more than six carbon atoms) is still limited. Yet, it is well established that these compounds typically accumulate in blood owing to their association with proteins [76, 159, 160].
The vast majority of studies assessing human exposure to PEs have been conducted in urine because the concentrations of PE metabolites are at least ten times higher in urine than in serum [161–163]. For example, the levels of MEP and monoisobutyl phthalate, primary metabolites of DEP and DiBP, and mono(2-ethyl-5-carboxypentyl) phthalate (5-carboxy-MEPP), a secondary carboxylated metabolite of DEHP, were highly correlated in matching urine and serum samples [161]. Therefore, urine seems to be a matrix where PE metabolites are present in quite high concentrations, but it is a representative medium for the circulating levels of only some metabolites. Because hydrolytic metabolites have limited half-lives (approximately 70 % of the oral dose is excreted after 24 h mainly by renal excretion), oxidative products exhibited greater bioaccumulation rates (2–7 % of the excretion rate), so are considered better biomarkers before elimination [9, 71, 164–167].
Koch et al. [166] suggested the use of the term “pseudo-persistent” chemicals for PEs because of the continuous exposure to which we are subjected. Indeed, when PEs are measured in humans, they are consistently present in almost all participants of HBM studies [168, 169]. The matrix of choice is also dependent on the aim of the monitoring. Urine, serum, and saliva are not good for proxy measurements of breast milk levels. In particular, high urinary metabolite levels do not predict PE levels in human milk [170]. This shows that matrix selection should be well thought about and should be driven by the research rationale behind the HBM study.
LaKind et al. [171] pointed out the importance of adding an esterase inhibitor (e.g., 1–1.2 M phosphoric acid) during collection of breast milk, (umbilical cord) blood, saliva, or semen, which is not needed for urine. It is used to prevent immediate breakdown of the parent diester compound to the monoester metabolites [171].
Furthermore, samples are prone to contamination by environmental PE sources during or immediately after sampling. In 2001, the US Food and Drug Administration reported [172] that during sample collection (plasma, blood), DEHP can be released from a Foley catheter to the bag; afterwards, mono-2-ethylhexyl phthalate (MEHP) is formed exogenously during storage by lipases that are present in the bag) [166]. For this reason, oxidative metabolites are to be preferred over hydrolytic ones whenever possible, because they are less likely to be formed exogenously. Some authors did not report the levels of monoesters in breast milk, serum, or even saliva for that reason [34, 170]. In the case of serum, contamination can occur during blood collection via Vacutainer® systems.
As far as we know, no HBM studies have been reported for OPEs. However, there are some HBM studies for assessment of BFRs in selected populations; the NHANES survey dating from 2003–2004, showed the presence of PBDEs in more than 60 % of the US population [173], with higher levels than those reported for Japan [174], Sweden [175], and Flanders [176]. Measurements of EFRs in blood samples are to date only available from China. In 128 samples collected in 2006 from the general Chinese population, hexabromobenzene (HBB) was identified in 26 samples, with a median concentration of 0.27 ng g−1 lipid (range 0.11–1.50 ng g−1 lipid); BTBPE, DBDPE, and pentabromoethylbenzene were not detected in any of these samples [177]. In pooled serum samples from residents of a bay area near a plant producing halogenated FRs, the average concentration of DP was 3.6 ng g−1 lipid; TBPH was detected in the pooled sample of 30–39-year-old women, thus demonstrating the need for further follow-up [178]. Relatively high levels of DP were detected in whole blood (up to 2,958 ng g−1 lipid) from occupationally exposed workers at a DP manufacturing plant [179] and in serum and breast milk from women living at electronic-waste recycling sites [180].
Non-invasive methods (urine, hair, nails, saliva, hand wipes)
Besides the inherent advantage of blood being in contact with different organs and tissues, its collection has some disadvantages: (minor) some complications (hematomas, pain) are possible, and sampling is more difficult for people of different ages and/or groups (children, the elderly, or chronically ill people). On the other hand, non-invasive approaches have the advantage that most matrices can be stored for a longer time without loss of properties and at low cost [181]. At some stage, the non-invasive matrices are in contact with blood, which can render them good proxies and an alternative to blood for monitoring contaminant exposure. Moreover, hair or nails can provide information about short-term to long-term exposure (months or even years), which is not always possible for blood, plasma, or urine analysis [150, 182]. Still, the use of non-invasive matrices in HBM studies is a challenge for analysts because low concentrations of pollutants are to be detected, which hampers the real human assessment of body burdens. There have been few HBM studies including the most accessible non-invasive matrices, such as hair, saliva, nails, and hand wipes, as biomarkers of human exposure to PEs, OPEs, PFASs, and EFRs. Table 2 provides an overview of extraction and analytical methods as well as analytical thresholds for non-invasive HBM studies. Matrices such as umbilical cord blood, placenta, meconium, and breast milk were not included as these matrices are not available from the general population, and are only available during a specific (and short) period and their use is of a rather semi-invasive nature. Use of exhaled breath condensate is an emerging technique; however, according to our knowledge, it was not applied to any of the pollutants in the scope of this review.
Urine
Urine is one of the most frequently used matrices in HBM, especially for water-soluble compounds. The main advantage is that analysis is non-invasive and urine is easy to collect by spot or 24-h samples. Although spot samples are easier to collect, the varying volume and the consequent dilution of the target compounds are the major disadvantages [188, 189].
As far as we know, urinary compounds can be related to account for many routes of exposure, and measuring urine is considered one of the best approaches for measuring metabolites of body burdens in HBM. However, some authors argue that urine is probably not a good matrix to assess exposure to persistent organic compounds (e.g., PFASs), because less than 50 % of the PFASs studied can be detected in urine [183] (Table 2). Others are of the opinion that there is a strong correlation between the concentrations of PFASs (such as PFOS, PFOA, perfluorononanoic acid, perfluorodecanoic acid, and perfluorohexane sulfonate) in paired blood and urine [190]. PFOS and PFOA were analyzed in human hair, nails, urine, and serum samples; the PFOS and PFOA levels were variable between samples (5–57 ng L−1 and less than 7 ng L−1 to 160 ng L−1, respectively) [85] (Table 2). However, a similar gender effect was seen between urine and serum, with higher levels of PFOS and PFOA in male samples. Nevertheless, low concentrations of the compounds investigated limit use of urine as an indicator for exposure to perfluoroalkyl acids, especially PFOA. Another study [183] demonstrated that eight PFASs (among the total of 21 analyzed) were detected in urine samples (mean levels between 0.74 and 480 pg L−1) and in hair (detectable levels above the method limit of quantification ranged between 0.1 and 46 ng g−1). In both samples, PFOA was detected, but the frequency of detection was completely different; that is, for urine, 17 of 30 samples revealed positive values, whereas in hair only eight of 24 samples had measurable values.
There is no record of the analysis of EFRs or their metabolites in urine. Some studies have assessed human exposure to PEs by measuring their urinary excreted metabolites [191]. Suzuki et al. [192] evaluated whether single spot urine is suitable for longer-term PE exposure assessment by the measurement of metabolites in urine of pregnant Japanese women. On the basis of the urinary concentrations of PE metabolites, daily intakes of seven PEs were estimated, and none of those levels exceeded the tolerable daily intake for DEHP, DnBP, and BBzP. By the analysis of interindividual and intraindividual variance of urinary excretion of metabolites, Suzuki et al. concluded that spot urine can be used for longer-term (up to months) exposure assessment. The same conclusion was reached by other authors [193–195].
Hines et al. [170] compared the concentrations of oxidative PE metabolites in several matrices, including milk, serum, saliva, and urine, using high-performance liquid chromatography (LC) coupled with tandem mass spectrometry (MS/MS) (Table 2). PE metabolites were most frequently detected in urine of lactating women (seven of the ten urinary metabolites were detectable in more than 85 % of samples) and were less often detected in serum, milk, and saliva. The urinary PE concentration might reflect maternal exposure and does not represent the concentration of oxidative metabolites in other body fluids (especially for milk). Also, the levels of urinary DEHP metabolites were well correlated with each other, with the oxidative metabolites having stronger correlation among themselves than with the monoester MEHP. The urinary PE concentrations in this study were in agreement with those detected in urine of pregnant women in the US and elsewhere [196, 197] with an MEP concentration ten times higher than other monoesters.
The exposure to OPEs is being assessed similarly to exposure to PEs by the measurement of OPE metabolites in urine as a biomarker of exposure. Current studies related to TDCPP and TPP have mainly focused on analysis of their metabolites bis(1,3-dichloro-2-propyl) phosphate (BDCPP) and diphenyl phosphate (DPP). In general, the analysis of OPE metabolites is complex, mainly owing to matrix effects. Methods of analysis of urinary monoalkyl and dialkyl phosphates are mainly based on analysis of concentrated urine [106] using a TurboVap evaporator, solid-phase extraction (SPE) with either a noncommercial molecularly imprinted polymer [198], or a commercially available cartridge containing a reversed-phase polymer with polar functionality [55]. Meeker et al. [54] detected BDCPP and DPP in 91 % and 96 %, respectively, of analyzed human urine samples collected from the US male population. These results were confirmed by Cooper et al. [199], who found detectable levels of BDCPP and DPP ranging from 46 to 1,662 pg mL−1 and from 287 to 7,443 pg mL−1, respectively.
Hair
Hair is an appendage of the skin that grows out of the hair follicle; it extends from its roots or bulb embedded in the follicle, continues into a shaft, and terminates at a tip end. Because each hair follicle is surrounded by a system of capillary blood vessels at the root [200], the chemicals present in serum can theoretically also be found in the hair, making it a suitable matrix to assess internal exposure.
On the other hand, the external exposure is correlated with gaseous compounds solubilized on the sebaceous gland excretions, covering the hair shaft [201]. Among many publications on HBM studies, the sampling procedures are not harmonized or sufficient information on the applied sampling procedure is lacking [202]. In a recent report, a harmonized approach was suggested to cut hair near the scalp at the occipital region of the head [203]. This area has less variability in the hair growth rate, less influence from sex or age, and a large and constant blood irrigation, thus better translating an internal exposure [204–206].
Owing to its relatively high lipid content (1–4 %), hair is suitable for monitoring lipophilic compounds. It has been widely used for human exposure to metals, pharmaceuticals, or drugs of abuse [207–211], but relatively little is currently known about analysis of persistent organic pollutants in human hair. Most of these analyses were performed for dioxins [151], PCBs [212–214], and pesticides [212, 214]. Much less has been reported for BFRs (e.g., PBDEs [215–217] and HBCD [218]). Still, the choice of sampling hair for routine HBM of body burdens is not convenient for people with short hair, baldness, or other kinds of dysfunction. Some cultural and racial factors, such as type of hair (blond, brown, or red) can also have an influence on the sampled amount, because hair grows at different rates depending on the hair type [206]. Other limitations to the use of hair in HBM are the differentiation of external and internal deposition of chemicals and their levels, where several factors have an influence on their incorporation (sex, age, smoking, artificial color) [205].
For the analysis of FRs, there are only two publications where DP was investigated in human hair as well as in dust or blood samples, respectively [105, 179]. In the first study [105] the total concentration of DP (sum of the syn-DP and anti-DP isomers) in hair samples ranged between 0.02 and 58 ng g−1 hair. Strong positive correlations were found for both concentrations of syn-DP and anti-DP between human hair and dust samples, suggesting that hair analysis could be a valid screening tool for assessing human exposure to DP. In the second study [179] the total DP levels were higher (between 4 and 2,159 ng g−1 dry weight), and correlation profiles similar to those obtained with blood were identified for the three study groups (group A, workers involved in direct exposure to DP in a manufacturing process; group B, workers from the same industry but without direct involvement in manufacturing activities; group C, people that do not work in the DP industry but who are resident about 3 km from the manufacturing plant). Moreover, these authors suggested good correlation between the levels in dust and hair of a population exposed to an electronic-waste recycling area. Zheng et al. [219] reported the levels of PBDEs and EFRs such as HBB, BTBPE, and DBDPE in hair collected from people exposed to different environments. Also, high levels of correlation between hair and dust samples collected from the same region were especially described for DBDPE (r = 0.97, p = 0.03) and BTBPE (r = 0.96, p = 0.04).
To the best of our knowledge, there is one recent report on the analysis of OPEs in human hair [220], and there is one study [186] in which five DEHP metabolites were investigated as compounds that truly reflect the level of DEHP exposure in hair. The main metabolite was MEHP (mean 45 ng g−1), whereas the levels of the other metabolites—mono(2-ethyl-5-oxyhexyl) phthalate (5oxo-MEHP), mono(2-ethyl-5-hydroxyhexyl) phthalate (5-OH-MEHP), 5-carboxy-MEPP, and mono[2-(carboxymethyl)hexyl] phthalate—were below 9 ng g−1.
Francisca Perez et al. [183] developed and validated an analytical method for analysis of 21 PFASs in human hair and urine for HBM, where several pretreatment approaches were tested. The best recoveries were obtained for simple extraction in 5 mL acetonitrile (extraction and sonication for 15 min). The use of turbulent-flow LC coupled with MS/MS has eliminated time-consuming sample cleanup and has increased productivity, with good sensitivity. In total, 75 % of the samples showed positive levels of at least one of the target PFASs. PFOA and PFOS were the main compounds detected, with their levels ranging between 0.1 and 6 ng g−1 and between 3.7 and 7 ng g−1, respectively. Nevertheless, PFOS was found in both matrices (human hair and urine), indicating its bioaccumulation in human hair.
The occurrence of correlations between the levels of PFOS and PFOA in different matrices might suggest they are distributed similarly between hair, nails, and serum [85]. The correlations between the levels of both analytes in hair and serum were less pronounced than the correlations in nails and serum. Moreover, a similar gender effect and statistical relationship between hair and serum samples was observed only for PFOA. The difference in the proportion of PFOS and PFOA in hair and nails might be caused by different mechanisms of incorporation of these compounds.
Nails
Historically, nails have been used in forensic science mainly for determining arsenic, antimony, lead, or mercury poisoning [221–224] and to lesser extent to biomonitor other inorganic chemicals (e.g., Cd, Cu, Mn, Zn, Fe) [225]. Yet, there is still lack of information regarding fingernails and toenails as biomarkers of internal human exposure for organic pollutants and consequently there are no studies on PEs, OPEs or EFRs in nails. For PFASs two recent studies [85, 184] reported correlations of the levels among nails, hair, and urine.
Li et al. [85] showed moderate agreement between serum and nails for PFOS but not for PFOA [r = 0.786 (p < 0.001) and r = 0.299 (p = 0.05), respectively] and poor agreement between serum and hair for PFOA [r = 0.545 (p < 0.001) for PFOS; not significant for PFOA] as well as between serum and urine [r = 0.302 (p < 0.05) and not significant, respectively]. Even in this study, the difference in the detectable concentrations between genders was minimal for fingernails, indicating that women and men are equally exposed to PFASs.
Another study involved the determination of eight PFASs [184], including perfluoroalkyl carboxylic acids and perfluoroalkyl sulfonic acids in both nails and hair. Different extraction methods (accelerated solvent extraction, acid and alkaline digestion following liquid–liquid extraction) and extraction solvents (methanol, 2 % v/v formic acid in methanol, and acetonitrile) were tested using a common cleanup procedure (SPE Oasis WAX) for both matrices. For the extraction of PFASs from nails, the use of alkaline digestion following extraction with methanol provided the best results (0.11–0.50 ng g−1), with six compounds being detected at lower limits of detections (between 0.023 and 0.094 ng g−1). The limits of quantification in nails ranged between 0.073 and 0.299 ng g−1, and more PFASs were detected in nails than in hair from the same population, suggesting that nails are better biomarkers of PFASs.
Some authors suggested that toenails usually contain high concentration of metals, which consequently makes toenails a good matrix for assessment of exposure to inorganic chemicals [221, 222]. However, there are no comparative HBM studies for fingernails and toenails, except for PFASs. Use of toenails has been suggested because of their lower external exposure during most of the day [85, 184].
Most studies note that nails should be washed prior to extraction to allow differentiation between endogenous and exogenous exposure. The choice of the best decontamination solvent/solution must be carefully considered; that is, in general, the criteria for the choice respect the chemical polarity of the target compounds since some solvents can destroy the matrix or eliminate the target compounds. Acetone [222, 225] and a nonionic detergent (Triton X-100) [83, 225] seem to be good cleaning solvents for use prior to mineral analysis as well as for determination of PFASs [184]. Methanol and acidic solutions (dilute solutions of nitric acid and formic acid) seem to be a bad choice for cleaning nails because of their hydrophilic character and because they remove analytes. Grinding the samples provides homogeneity, in addition to better solubility and extraction of the target analytes [85, 226]. There are possible disadvantages in translating this exposure owing to an uncertainty associated with the time of exposure; that is, it is only possible to sample the distal edge of the nail plate, which does not represent the immediate exposure, therefore representing an interindividual variability. Besides the low concentrations of organic contaminants found and because of some inherent limitations of sampling, nails can provide information about longer-term exposure (months), unlike blood.
Saliva
Saliva is a secretion produced by three types of specialized salivary glands (parotid, submandibular, and sublingual glands) which have protective, defense, and digestive functions for the mouth. Saliva contains a large proportion of water (around 99 %) together with minor components (electrolytes, proteins, polypeptides, enzymes, glycoproteins) which are critical for maintaining oral health [187, 227–229]. Saliva is easy to collect by wiping the oral cavity with a swab or by using specific devices either with or without previous stimulation [187, 189]. The three types of oral fluid collectors available on the market are the Salivette®, OraSure®, and QuantisalTM. The Salivette® is mostly recommended for cortisol analysis and has advantages over traditional blood collection methods such as collection of a large amount (1.5 mL saliva) in a short time. However, the dental cotton roll used to adsorb saliva may interfere with several organic compounds and has low extraction recoveries for lipophilic compounds [230]. The OraSure® has different devices to track drugs, alcohol, and hepatitis C virus antibodies. The main disadvantage is that it collects only around 1 mL of sample and uses a cotton swab to collect a mixture of saliva and gingival crevicular fluid usually removed from the cheeks and gums and under the tongue [230]. Finally, the QuantisalTM is the most recent and simplest device to collect oral fluids for forensic drug testing. Large volumes of saliva (1–10 mL) can be stored in a buffer stabilizer solution, which avoids degradation of the matrix, allowing long-term storage [231]. This device is successfully used for illicit drug analysis [231, 232].
The use of these devices necessitates the stimulation of saliva production to the detriment of possible changes in important parameters such as saliva composition and oral pH [189].
Saliva is often in close contact with contaminants, whether this be directly through external sources of contamination, such as food, or through permanent contact with high blood flow by direct proximity to oral tissues. Thereafter, chemicals and their metabolites can pass from blood to saliva by different ways of excretion [187]. Nevertheless, the low protein content and high water content are not beneficial for protein-bound molecules, and salivary levels of hydrophobic/lipophilic compounds are usually extremely low. Saliva has been mainly used to study the metabolism and excretion of drugs [231–233], pesticides [234], PCBs, dioxins [235], and metals [226].
Saliva has not been routinely used in HBM, probably because of the various confounding factors. However, there is some literature available on its applications, namely, for PEs [170, 187] and PFASs [236]. Low levels of PE metabolites have been detected in saliva (below the limit of detection to 58 ng mL−1) [187]. The high number of enzymes present in saliva requires a postcollection treatment in order to promote their denaturation (e.g., phosphoric acid), followed by deconjugation using β-glucuronidase [187]; no cleanup method is used prior to instrumental analysis. Although the levels in saliva are lower than in those in urine or serum [161, 237], these findings suggest that saliva could be a possible biomarker for human exposure to various PEs.
Hand wipes
Since hands are in constant contact with many objects either by routine or by specific activities, the assessment of external exposure can be easily performed by cleaning the hands in wipes soaked in 2-propanol or methanol [135, 185, 238–240]. The most suitable methods used to extract organic pollutants from wipes are pressurized liquid extraction [185], Soxhlet extraction [241], and solid–liquid extraction [135, 238], where the polarity of the extraction solvents must be chosen according to the target analytes, for example, dichloromethane and hexane–dichloromethane (1:1, v/v) for PBDEs [135] and acetone for pesticides [241]. Different SPE sorbents can be used for cleanup (e.g., 6 % deactivated alumina [135] or acidified silica [185] in the case of analyses of BFRs).
Although hand wipes are not real biological specimens, they have shown good results in HBM studies of volatile organic pollutants [241], polycyclic aromatic hydrocarbons, PCBs, pesticides, and phenols [239]. There have been no studies on monitoring of PEs, PFASs, and OPEs in hand wipes. Stapleton et al. [135] investigated how hand wipes can be used to translate exposure to PBDEs by mouth-to-hand contact and dust ingestion. Several PBDEs were detected in individual wipes, with a detection frequency of 67–100 %. The results suggest better correlations for the levels of pentabromodiphenyl ethers between serum and hand wipes than for hand wipes and house dust. The palm and back of the hand levels were compared for adults (male and female) and children, and it was found that the palm has higher levels than the back of the hand and that children are subject to greater exposure to PBDEs. Watkins et al. [238] measured and compared the levels of PBDEs between hand wipes and serum collected from 31 individuals. The correlation between dust (from living areas and bedrooms) was the strongest predictor for serum; however, the association between hand wipes and serum showed that hand wipes can be good predictors of exposure especially in bedrooms and offices. Nevertheless, the correlation with dust found in offices suggests that the levels in hand wipes reflect recent exposure to the surrounding environment, and therefore more research is needed.
More recently, Allen et al. [185] demonstrated exposure to several FRs (including TDCPP, TBPH, HBCD, DP, and TBB) by comparing the concentrations in hand wipes and dust collected from people exposed in commercial airplanes and indoor environments such as homes and offices. In fact, most of these compounds were detected in 100 % of dust samples, sometimes at extremely high levels (below 29,000 ng g−1); also in hand wipes (palm and back of hand) the levels of PBDEs were quite high (390 ng per hand wipe for DBDPE). Especially, the palm revealed higher values than the back of the hand and the levels were correlated with those in dust.
Although the levels in wipes were generally lower than those in other media, several studies have demonstrated that they are good predictors of surrounding pollution.
Overview of HBM studies in non-invasive matrices
Most of the non-invasive HBM studies involve an average of 62 participants per study (except the study of Silva et al. [187], which considered more than 2,000 urine samples), which is a relatively small sample size in terms of representativeness of an HBM study (Table 3). Among the non-invasive matrices studied/considered, urine is the biological matrix in which the highest number of the pollutants of interest have been detected most often (mean value of 75 %) and in which the highest number of pollutants of interest have been detected (e.g., PFASs and PE metabolites were detected in more than 90 % of the samples analyzed) [170, 183].
Hair has also been explored in HMB for FRs, OPEs, PEs, and PFASs [85, 105, 179, 183, 186, 220]. In hair, the levels of DP compounds ranged between 0.9 and 130 ng g−1 (greater than 88 % detection frequency), those of OPEs ranged between 27 and 461 ng g−1 (89 % detection frequency), those of PE metabolites ranged between 5.7 and 44.9 ng g−1 (60 % detection frequency), and those of PFASs ranged between 0.6 and 6.5 ng g−1 (42 % detection frequency). The two non-invasive matrices used least frequently are saliva and nails. The detection of PE metabolites in saliva seems to be challenging (levels between 1.2 and 57.9 ng g−1 ) and their detection frequency is quite low (below 45 % of the samples analyzed) [170, 187]. PFASs showed good detection frequency in nails (above 70 %), although at low concentrations (0.2 and 5.1 ng g−1) [184].
Instrumental analysis
The analysis of biological non-invasive matrices such as hair and nails requires additional pretreatment compared with analysis of invasive matrices. These matrices might require decontamination/washing (removal of externally deposited contaminants), drying, cutting, and/or homogenization, on which hydrolysis might be needed before the samples can be actually extracted [83, 205]. All these manipulations can lead to unintended loss of target analytes if no proper measures are taken.
Further, the residue levels can be significantly lower in certain non-invasive matrices than in serum. The performance of the analytical instrumentation is therefore an essential parameter to make possible selective and sensitive detection of organic contaminants at desirable thresholds. Powerful techniques such as MS/MS are usually applied for instrumental analysis because of their high accuracy and selectivity for volatile or semivolatile organic contaminants [242].
The analysis of OPEs is usually performed by gas chromatography (GC) with a nitrogen–phosphorus detector or GC coupled with mass spectrometry (MS) [52, 56, 59], both of which are less susceptible to matrix effects compared with LC techniques. However LC–MS/MS is required to analyze more polar dialkyl or monoalkyl OPE metabolites [243]. Van den Eede et al. [243] developed a method for a wider group of OPE metabolites and recommended LC–negative electrospray ionization–MS/MS for analysis of DPP and GC–MS/MS for analysis of chlorinated metabolites, such as BDCPP, bis(1-chloro-2-propyl) phosphate, and bis(2-chloroethyl) phosphate. Schindler et al. [55] used GC–MS/MS for analysis of OPE metabolites [bis(2-chloroethyl) phosphate, DPP] after a lengthy sample preparation which included SPE and chemical derivatization with pentafluorobenzyl bromide.
For BFRs, the most popular instrumental techniques are GC in combination with electron capture negative ion MS or GC with electron ionization MS owing to the low polarity and high volatility of the compounds [105, 135, 185, 214, 238, 240]. Nonpolar stationary phases (e.g., DB-5HT, HT-8ms) are the most used for peak separation of FRs (DP compounds and PBDEs) [105, 135].
Although PEs and their metabolites, OPE metabolites, and PFASs are best analyzed using LC–MS, their separation is ideally performed on different stationary phases. For the best separation of PEs and their metabolites end-capped reversed-phase columns such as a Betasil phenyl high-performance LC column (100 mm × 2.1 mm, 3 μm) [167] or a Luna C18 column (50 mm × 2.0 mm, 3 μm) [186] were suggested. More polar and acidic compounds such as OPE metabolites are best chromatographed using medium-polarity stationary phases such as a phenyl–hexyl (150 mm × 3 mm, 3 μm) column or an XBC18 column (100 mm × 2.1 mm, 2.6 μm) [106, 199], which are operated in combination with strong polar elution solvents (mostly water component) or strong volatile ion pairing reagents (e.g., tributylamine) [106]. The best chromatographic separation for PFASs is achieved at low pH using a BEH C18 column (50 mm × 2.1 mm, 1.7 μm) [85, 184].
For the above-mentioned compounds, electrospray ionization or atmospheric pressure chemical ionization is mostly performed in negative mode combined with multiple-reaction monitoring, resulting in characteristic fragmentation patterns according to the chemical structure of precursor and product ions [85, 167, 186, 187, 198].
Electrospray ionization is the most popular method because of its ability to analyze large and nonvolatile molecules, but it is also sensitive to matrix effects. The use of adequate (labeled) internal standards, the addition of ion pairing reagents or buffers to the mobile phase, and the use sample cleanup before analysis are ways to reduce matrix effects [242].
Critical issues
Because most of the afore-mentioned compounds are ubiquitous environmental chemicals, precautions have to be taken to avoid or minimize (cross-)contamination or errors introduced through handling, storage, and analysis. Therefore, glassware (including SPE cartridges) is preferred over plastics, and it should be baked overnight at 450 °C. If use of plastics cannot be avoided, they should be first washed using a concentrated acidic solution (10 % HNO3) followed by ultrapure water, dried at room temperature, and finally rinsed with an appropriate solvent [244]. Nevertheless, owing to the high absorption of some organic contaminants, for example, PFASs, polypropylene is preferred over glass [245].
The use of polytetrafluoroethylene in vials, septa, and plastic bags for storing samples is to be avoided as chemicals can leach from the recipient to the biological samples, leading to erroneous results; solid samples should be wrapped in aluminum foil to safeguard the overall integrity, and liquid samples should be stored in decontaminated glass containers or appropriated collection devices (in the case of saliva) [204, 206].
Some authors state that care should be taken in sample decontamination prior to extraction, namely, for hair and nails, where it is advised to use a washing medium to remove external contamination such as dust particles [85, 246]. Most often, solutions of surfactants in water (e.g., 1 % solution of Triton X-100, 0.3 % polyoxyethylene lauryl ether), hydrophobic organic solvents, and hydrophilic organic solvents (methanol, acetone, dichloromethane) can be used to clean the samples without damaging or changing the chemical structure and sample integrity [26, 65, 79, 126, 147]. Recent research [247] has shown, however, that selective removal of externally deposited chemical contamination is not achieved by any of the solvents commonly used, and that hair should be used as such as a marker of external exposure. Althugh nails that have undergone surface treatment such as polishing were used in the past for metal analysis [210], it is highly unlikely that such samples can be successfully applied to assess organic contaminants.
Among the many publications on HBM studies, the sampling procedures are not harmonized or sufficient information on the sampling procedure applied is lacking [202]. In a recent report, a harmonized approach was suggested to cut hair near the scalp at the occipital region of the head [203]. This area has less variability in the hair growth rate, less influence from sex or age, and a large and constant blood irrigation, thus better translating an internal exposure [204–206].
A pending issue in non-invasive HBM is the differentiation between endogenous and exogenous contamination. When endogenous metabolites can be measured, for example, for OPEs, this differentiation is possible. Nonetheless, for assessment of chemicals that do not undergo metabolism such as PFASs [83, 85, 184], the discrimination is more difficult or even impossible. In such cases, exogenous contamination could not only be deposited onto surface, but could also be incorporated within the sample matrix, suggesting that measured levels reflect an integral level of both exogenous and endogenous contamination [213].
Human metabolism of emerging pollutants
In vitro metabolite formation and the enzymes responsible
Information on in vitro metabolism of the emerging pollutants of interest is presently very limited. In the few studies available, no steady-state conditions were applied, authentic standards were rarely used to identify the metabolites formed, rates of metabolite formation were not quantified, and little attention was paid to investigating the formation of phase II metabolites. Therefore, the summary of the literature reported below is to be considered strictly qualitative and based on first-insight metabolism studies only.
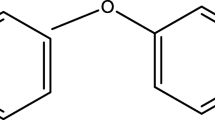
A general pathway of phase I metabolism of OPEs in vitro involves cleavage of the ether bond (producing the corresponding diester and an aldehyde or a ketone), oxidation of unsubstituted carbon atoms, and oxidative dehalogenation of the terminal (ω) carbon atom. All these reactions result in the formation of hydroxylated metabolites, some of which can be substrates of alcohol and aldehyde dehydrogenases, ultimately forming carboxylic acids. The main identified metabolites of tris(1-chloro-2-propyl) phosphate, tris(2-chloroethyl) phosphate (TCEP), TDCPP, tris(2-butoxyethyl) phosphate, and TPP are candidate markers of human exposure to these OPEs (Fig. 2).

Chemical structures of the major identified metabolites of selected organophosphate ester flame retardants formed by human liver microsomes or liver S9 fraction
A general in vitro metabolic pathway has also been elucidated for a limited number of PEs. The first step involves cleavage of one ester moiety, producing the corresponding monoester and aldehyde metabolites. The monoester primary metabolite can be further metabolized to secondary metabolites by oxidation of a carbon atom and cleavage of the second ester moiety (producing phthalic acid and an aldehyde metabolite), or it can be conjugated with sulfate or glucuronic acid (phase II metabolites). Hydroxylation of the terminal (ω) carbon atom of the alkyl chain produces an alcohol that can be further transformed into a ketone and ultimately into a carboxylic acid by the alcohol and aldehyde dehydrogenases, respectively. The major identified metabolites of DnBP, DEHP, and BBzP are presented in Fig. 3. To the best of our knowledge, there is presently no information about in vitro metabolism of DEP and DiBP in humans.

Chemical structures of the major identified metabolites of selected phthalate esters formed by human liver microsomes or liver S9 fraction
Hardly any information on metabolism of PFASs is available in the literature. However, there is one study showing that PFOS is formed by preferential metabolism of a few isomers composing the N-ethylperfluorooctane sulfonamide commercial mixture by cytochrome P450 (CYP) enzymes [248]. Because the carbon atoms are fully substituted with fluorine, it is unlikely than CYP or other phase I enzymes are able to metabolize PFOA at an appreciable rate. Thus, PFOA could be a substrate of phase II enzymes. However, no phase II metabolite was detected when PFOA was incubated with human and rat liver, kidney, and intestine microsomes [249].
The pathways of metabolism of EFRs have not been elucidated. The major identified metabolites of TBB and TBPH are reported in Fig. 4. To the best of our knowledge, there is no information on human metabolism of BTBPE, DBDPE, HBB, pentabromotoluene, hexacholocyclopentadienyl-dibromocyclooctane and DP. Few phase I metabolites were detected on incubating TBB or TBPH with human liver microsomes and liver S9 fraction. Only a minority of them were structurally identified. Therefore, more comprehensive in vitro metabolism studies are needed to identify at least the major metabolites of the EFRs of interest using authentic standards. Even less is known about the enzyme(s) involved in the formation of metabolites of EFRs.

Chemical structures of the major identified metabolites of emerging flame retardants formed by human liver microsomes or liver S9 fraction
In general, formation of metabolites produced by cleavage of the ester moiety of the OPEs and PEs of interest involves microsomal esterases and CYP enzymes [42, 250, 251]. Only in the studies characterizing the in vitro metabolism of DEHP were the individual enzymes responsible for the metabolites formed identified [42, 250].
Identification of the in vivo metabolites of emerging pollutants
Limited information is presently available about human in vivo formation and excretion of phase I and phase II metabolites of OPEs, PEs, and EFRs. For OPEs, only biomonitoring studies focusing on TDCPP and TPP metabolite formation are available [54, 199, 252]. BDCPP and DPP were the only in vitro metabolites of TDCPP and TPP, respectively, that could be measured in human urine samples [54, 199, 253], suggesting that they could be used as biomarkers of exposure for TDCPP and TPP (Table 4). However, no phase I hydroxylated (i.e., monohydroxylated and dihydroxylated metabolites, ketone and carboxylic acid) metabolites or phase II metabolites (i.e., glucuronic and sulfate conjugates) were monitored. Investigation of the presence of several phase I and phase II metabolites of TDCPP and other PFRs in human serum, urine, and feces is needed to better determine the best biomarker(s) of their exposure.
In vivo metabolism of PEs in humans has received more attention. The major in vivo PE metabolites detected in human matrices are reported in Table 4. The monoester primary metabolites of DnBP, DiBP, and BBzP were detected in the vast majority of the urine samples analyzed, suggesting that the monoester metabolites are readily formed in vivo [34, 161, 163, 252, 254]. This result is consistent with monoesters being the major DnBP, DiBP, and BBzP metabolites in vitro [251, 255], suggesting that monoester metabolites of DnBP, DiBP, and BBzP, namely, mono-n-butyl phthalate, monoisobutyl phthalate, and monobenzyl phthalate, respectively, can be used as markers of exposure. However, for DEHP, the secondary in vitro metabolites, that is, 5-OH-MEHP, 5-oxo-MEHP, 5-carboxy-MEPP, and 2-cx-MMHP, were the most prominent metabolites detected in human urine and serum samples [161, 162, 256]. Also, 5-carboxy-MEPP and MCMHP were more often detected than MEHP in serum samples [161]. All these findings suggest that the secondary metabolites of DEHP are more suitable markers of exposure than are the primary metabolites (i.e., MEHP). However, the reliability of secondary metabolites as the best markers for exposure to PEs remains to be confirmed for PEs other than DEHP.
The profile of DEHP secondary metabolites in urine changes with time after exposure and with human life stage. 5-OH-MEHP and 5-oxo-MEHP are the major urinary metabolites of DEHP during the first 12 h after exposure, whereas 5-carboxy-MEPP and MCMHP are the major urinary metabolites of DEHP after 12 h after exposure [166]. In urine samples of neonates, 5-OH-MEHP and MECPH represented 0.6 % and 65 %, respectively, of the measured DEHP metabolites, whereas these two metabolites amount to 66 % and 32 %, respectively, of the total metabolites measured in adults [256]. Therefore, selection of the appropriate DEHP metabolite to monitor largely depends on the time elapsed since the last DEHP exposure and on the human life stage.
Presently, no information is available about human in vivo metabolism of PFASs and EFRs of interest.
Biomonitoring of emerging pollutant metabolites: choices of the matrices to monitor in humans
Combining the findings of all the HBM studies mentioned so far indicates urine is the most promising matrix to monitor the presence of PE metabolites as markers of human exposure. Since most of the in vivo metabolites of DEHP (and other PEs) are formed sequentially, the urinary profile of DEHP metabolites varies with the time elapsed from DEHP exposure [162, 166]. Therefore, the urine sampling strategy can be of importance in detecting DEHP and, in general, other metabolites. In a recent study [257], significant correlations were determined between the concentrations of all phthalate metabolites detected in a 24-h pool, a first-morning urine sample, and a spot urine sample (second void of the day), all obtained within the same 24-h period. This result might support the validity of using first-morning and spot urine samples in population studies for these compounds. However, there is growing agreement that a single urine sample (either spot urine or 24-h urine) gives a high degree of misclassification. Therefore, collection of multiple spot samples taken on different days (which may be pooled) is being prosposed more and more as the preferred sampling strategy for phthalates [257, 258]. Also, first-morning urine analysis likely helps to reduce the diurnal intraindividual variability of PE exposure due to the accumulation of PE metabolites in the urine overnight. Therefore, use of a first-morning urine sample could be the sampling strategy maximizing the possibilities to detect the PE metabolites used as markers of human exposure. Lastly, monitoring PE metabolites rather than the parent compounds avoids contamination problems during sample preparation and storage due to the widespread presence of PEs in the environment.
To the best of our knowledge, there is currently no biomonitoring study investigating the presence of OPE, PFAS, and EFR metabolites in humans; hence, there is no information about the most appropriate matrices for monitoring studies. In rats treated with radiolabeled TCEP or TDCPP, 60–75 % of the radioactivity administered was measured in the excreta, mainly in urine [259–261]. However, there is no information about the apportionment of the radioactivity between parent compounds and metabolites. Therefore, urine is a promising matrix to monitor the presence of OPE metabolites, although it is not clear if feces are a reliable matrix too. The reliability of urine and feces as matrices for TCEP and TDCPP biomonitoring in humans needs to be investigated.
Research gaps and future perspectives
The compounds covered in this review were limited by the availability of non-invasive HBM focusing on these target contaminants. Other emerging contaminants are also present in our environment and will probably be included in future HBM studies. Monitoring their presence in humans will be relevant, as they belong to the same chemical class of potential harmful pollutants as the compounds covered by this review.
The new FRs such tetrabromobisphenol A bis(2,3-dibromopropyl ether), pentabromoethylbenzene, octabromo-1,3,3-trimethyl-1-phenylindan, 2,2′,4,4,5,5′-hexabromobiphenyl, and Chlordene Plus, which have already been detected in the environment and wildlife [48, 262], are potential relevant target compounds on which future HBM can focus.
There are other interesting emerging compounds which can be explored in biological samples, for example, for OPEs, 2-ethylhexyl diphenyl phosphate, and for PEs and their metabolites, there are several new pentyl/isopentyl and hexyl phthalate derivatives (e.g., n-pentyl benzyl phthalate, n-butyl isopentyl phthalate, n-butyl n-pentyl phthalate, 2-ethylhexyl n-octyl phthalate, hexyl 2-ethylhexyl phthalate) which were included as candidate substances of very high concern for authorization by the European Chemicals Agency [263]. Within the fluorochemicals class, more compounds regarding PFASs and polyfluoroalkyl substances can also be studied, for instance, the fluorotelomer alcohols (and acids), as well as the polyfluorinated monoalkyl phosphates and dialkyl phosphates which are relevant because of their degradation to perfluoroalkyl carboxylic acids under atmospheric conditions [160, 264, 265]. From our knowledge, none of these newly emerging contaminants have been studied in non-invasive matrices.
As currently no standardized methods exist for the emerging contaminants covered by this review, most of the available studies are based on customized in-house developed methods that sometimes are substantially different. As research progresses, methods will likely converge and more harmonized approaches will be available, as happened for the biomonitoring of PCBs, PBDEs, etc. However, the current lack of standardized methods of analysis might result in high uncertainty and variability of the results obtained in different laboratories. The reliability of the results generated might be affetected by the lack of appropriate quality assurance tools to establish a common basis for accurate measurements of the compounds of interest in non-invasive matrices, such as standardized methods of analysis and certified reference materials (CRMs). These tools would greatly enhance data quality and consistency. The development of standard methods and related CRMs is mainly driven by legislative requirements. As such legislation is not yet in place for these compounds in non-invasive matrices, standardized methods and CRMs are currently not available.
However, some efforts have already been made towards standardization of non-invasive methods. Through the Society of Hair Testing and the Society of Toxicological and Forensic Chemistry, there are already some approved guidelines for hair sampling and analysis in relation to drug and alcohol testing [266] and guidelines for toxicologists [267], but no validation guidelines (or CRMs) have been established for assessing environmental pollutants.
CRMs for serum and hair matrices exist, but these materials are not certified for any of the emerging compounds covered by this review. For some materials indicative values (which are not certified) are mentioned for, for example, perfluorinated chemicals in serum (SRM 1957), and such materials can be successfully used for quality control to a certain extent for the determination of PFASs, as was done by Keller et al. [268] and Salihovic et al. [269]. To our knowledge, there are currently no CRMs available for non-invasive matrices such as hair, nails, or saliva that are certified for any of the emerging compounds covered by this review.
However, even if CRMs are not certified for the target analytes, they can have an added value for quality control. Mainly the homogeneity and assumed stability of the material are important here, as is the presence of the compound of interest, albeit at an unknown (uncertified) mass fraction. For example, a reference material for trace elements in human hair (BCR 397) was used in a small interlaboratory exercise for the determination of organic pollutants [270].
Further harmonization of methods and increasing use of reference materials (which can be recertified for new emerging compounds) will result in higher quality of results and better comparability between studies.
Reviewing the literature for HBM based on non-invasive methods suggests that urine is the matrix most widely used to monitor human exposure to OPEs, PEs, and FRs and/or their hydrolytic/oxidative metabolites. However, it has not been fully clarified how much of the parent compounds are excreted in urine and what is their correlation with an invasive sample from the same population. Most of the available studies identified the native compounds or the metabolites for the groups that undergo quick metabolism (e.g., PE and OPEs), but they did not analyze their relative proportion in urine and whether native compounds can be detected.
Hair has been used for a long time to assess drug consumption and heavy metal exposure, whereas for organic pollutants only a few studies have been conducted. The high association between contaminant levels found in hair and other matrices (e.g., serum) suggests that this non-invasive matrix can be reliably used to estimate human exposure to organic pollutants. Even less information is available about nails as a biomonitoring matrix for human exposure to environmental pollutants. In particular, the ability of nails to accumulate environmental pollutants has still to be investigated.
For saliva and hand wipes, the available information on HBM is scarce, and we suggest that more research is needed for more groups of compounds (e.g., polar and lipophilic compounds). Matrices should be compared with serum/urine from a representative subpopulation. Very little information is presently available on saliva as a non-invasive matrix to monitor the presence of environmental pollutants. In our view, the levels of environmental pollutants and their metabolites detected in saliva samples should be validated with those detected in serum and urine samples from the same individuals (matching samples). Such an approach will provide evidence of the representativeness and reliability of saliva as a biomonitoring matrix in humans.
Monitoring pollutants and their metabolites in human matrices is currently complicated by several aspects, and confounding factors can hamper correct interpretation of results. Future harmonization of HBM will greatly improve comparability of different studies. Different aspects have to be optimized to yield maximum results from HBM studies by means of non-invasive matrices.
First, the selection of the most suitable non-invasive matrix is the first hurdle to overcome. As highlighted also in Table 3, not all matrices are equally suitable for every compound in HBM studies. The amount of (available) samples and the timing of sampling are also crucial. In the ideal non-invasive HBM approach, being able to properly assess human exposure to the chemicals of interest using a small sample size is a great advantage, especially when working with babies, elderly people, etc. Too low sample intakes can also lead to elevated limits of quantification, which could be incompatible with the levels to be measured. The timing and frequency of sampling are also of importance since they can affect the levels of the contaminants present in the sample and their detection frequency, as suggested by the large differences observed between spot and 24-h combined samples for the detection of PEs [192–194]. Other factors such as sweating, thirst, and hunger can influence the measured levels of contaminants in saliva [229, 271].
Second, the selection of relevant analytes and/or their metabolites is crucial, which is in many cases closely linked to the sampling time. The measured levels can be very low owing to complex metabolic pathways leading to many different metabolites, high elimination rates, compound accumulation, etc.
Third, metabolism can be a major determinant of the elimination of xenobiotics from the human body. Therefore, focusing only on the detection of the native compound(s) that humans are exposed to can be misleading in estimating human exposure to environmental pollutants. As a consequence, knowledge of the major metabolites produced from the environmental pollutants of interest can be an alternative but key approach in properly estimating human exposure to environmental pollutants. In particular, in vitro metabolism studies are powerful and rapid screening tools to identify the major metabolites formed from each environmental pollutant and to estimate the rate of metabolite formation, providing useful insights of in vivo metabolism. The major (phase I and phase II) metabolites formed in vitro are valuable candidate markers of exposure to their parent compound and may offer a valid analytical alternative to their parent compounds to monitor human exposure. This approach is very promising for conducting HBM studies of emerging pollutants for which limited (metabolism) information is available (e.g., TDCPP, TPP, DnBP, DiBP, BBzP, and DEHP).
Fourth, the metabolites formed and the rates of their formation are often unknown, and analytical reference standards for the parent compounds and their metabolites, which are essential for their identification and quantification, are unavailable in the vast majority of cases. The availability of reference materials (both standards and matrix-matched CRMs) of both native compounds and their major metabolites would greatly advance HBM research.
Finally, quantitative extraction of xenobiotics from biological matrices is often challenging because of their different and complex compositions. Moreover, the (extraction and instrumental) sensitivity is also relevant to detect these contaminants at extremely low detection levels (below nanograms per gram or nanograms per milliliter). Nevertheless, the selection of the matrix and the analytical sensitivity are somehow interlinked, which demonstrates that the inefficacy of extraction/instrumental methods and the lack of sensitivity, reproducibility, and accuracy are determinant factors for selecting the most suitable matrix. The miniaturization of sample preparation procedures (dispersive liquid–liquid microextraction, stir bar sorptive extraction, ultrasound-assisted dispersive liquid–liquid microextraction, ultrasound-assisted emulsification microextraction, vortex-assisted liquid–liquid microextraction, etc.) can enhance the potential of HBM regarding the detection of these (and many other) organic contaminants. The harmonization of methods and the use of CRMs, as mentioned before, are also at the forefront of future HBM research.
Collectively, these remarks suggest that the sampling strategy (which matrices to sample, the number of matrices available, and the timing of sampling), efficient sample preparation, and sensitive analytical methods developed using appropriate reference standards are key elements for successfully biomonitoring of xenobiotic levels in humans and properly estimating human exposure to such compounds.
References
World Health Organization (2009) Global health risks: mortality and burden of disease attributable to selected major risks. World Health Organization, Geneva
Wan HT, Leung PY, Zhao YG, Wei X, Wong MH, Wong CKC (2013) J Hazard Mater 261:763–769
(2006) Stockholm Convention on Persistent Organic Pollutants
United Nations (2009) Stockholm Convention on Persistent Organic Pollutants. Stockholm 22 May 2001. Adoption amendments to Annexes A, B and C. https://treaties.un.org/doc/Publication/CN/2009/CN.524.2009-Eng.pdf
United Nations (2011) Stockholm Convention on Persistent Organic Pollutants. Stockholm 22 May 2001. Adoption of an amendment to Annex A. https://treaties.un.org/doc/Publication/CN/2011/CN.703.2011-Eng.pdf
Segev O, Kushmaro A, Brenner A (2009) Int J Res Public Health 6:478–491
Birnbaum LS, Staskal DF (2004) Environ Health Perspect 112:9–17
Carlsson H, Nilsson U, Becker G, Östman C (1997) Environ Sci Technol 31:2931–2936
Wittassek M, Angerer J (2008) Int J Androl 31:131–138
Casas M, Chevrier C, Den Hond E, Fernandez MF, Pierik F, Philippat C, Slama R, Toft G, Vandentorren S, Wilhelm M, Vrijheid M (2013) Int J Hyg Environ Health 216:230–242
Jamal G, Hansen S, Julu POO (2002) Toxicology 181–182:23–33
European Commission (2009) Commission Regulation (EC) No 552/2009 amending Regulation (EC) No 1907/2006 of the European Parliament and of the Council on the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH) as regards Annex XVII
Ali N, Harrad S, Goosey E, Neels H, Covaci A (2011) Chemosphere 83:1360–1365
Bergh C, Magnus Åberg K, Svartengren M, Emenius G, Östman C (2011) J Environ Monit 13:2001–2009
Kantiani L, Llorca M, Sanchís J, Farré M, Barceló D (2010) Anal Bioanal Chem 398:2413–2427
Angerer J, Bird MG, Burke TA, Doerrer NG, Needham L, Robison SH, Sheldon L, Zenick H (2006) Toxicol Sci 93:3–10
Angerer J, Ewers U, Wilhelm M (2007) Int J Hyg Environ Health 210:201–228
Calafat AM, Needham LL (2009) Environ Health Perspect 117:1481–1485
Needham LL, Calafat AM, Barr DB (2007) Int J Hyg Environ Health 210:229–238
Koch HM, Calafat AM (2009) Philos Trans R Soc B 364:2063–2078
Król S, Zabiegała B, Namieśnik J (2013) Trends Anal Chem 47:84–98
Paustenbach D, Galbraith D (2006) Regul Toxicol Pharmacol 44:249–261
Schwesig D, Borchers U, Chancerelle L, Dulio V, Eriksson U, Farré M, Goksoyr A, Lamoree M, Leonards P, Wegener J-W, Lepom P, Leverett D, O’Neill A, Robinson R, Silharova K, Tolgyessy P, Slobodnik J, Tutundjian R, Westwood D (2011) Trends Anal Chem 30:1233–1242
Aylward LL, Kirman CR, Schoeny R, Portier CJ, Hays SM (2013) Environ Health Perspect 121:287–294
Schulz C, Wilhelm M, Heudorf U, Kolossa-Gehring M (2012) Int J Hyg Environ Health 215:150–158
World Health Organization (2004) Environmental health criteria 209. Flame retardants: tris(Chloropropyl) phosphate and tris(2-chloroethyl)phosphate. World Health Organization, Geneva
Budavari S (2001) The Merck index - an encyclopedia of chemicals, drugs, and biologicals, 13th edn. Merck, Whitehouse Station
Hansch C, Leo A, Hoekman D (1995) Exploring QSAR: hydrophobic, electronic, and steric constants. American Chemical Society, Washington
World Health Organization (2000) Environmental health criteria 218. Flame retardants: tris(2-butoxyethyl)phosphate, tris(2-ethylhexyl)phosphate and tetrakis(hydroxymethyl) phosphorium salts. World Health Organization, Geneva
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans (1989) Some flame retardants and textile chemicals and exposures in the textile manufacturing industry. IARC monographs vol 48. International Agency for Research on Cancer, Lyon
Koch HM, Lorber M, Christensen KLY, Pälmke C, Koslitz S, Brüning T (2013) Int J Hyg Environ Health 216:672–681
US National Institutes of Health (2006) Supporting nomination for toxicological evaluation by the National Toxicology Program: chemical information profile for diethyl phthalate. Integrated Laboratory Systems, Research Triangle Park
Environmental Protection Agency (2006) Toxicological review of dibutyl phthalate (di-n-butyl phthalate). Environmental Protection Agency, Washington
Koch HM, Christensen KLY, Harth V, Lorber M, Brüning T (2012) Arch Toxicol 86:1829–1839
International Programme on Chemical Safety (2001) ICSC 0829 - diisobutyl phthalate. http://www.inchem.org/documents/icsc/icsc/eics0829.htm
Koch HM, Müller J, Angerer J (2007) J Chromatogr B 847:114–125
Saravanabhavan G, Murray J (2012) J Environ Public Health 2012:810501
GreenFacts (2001–2013) GreenFacts - facts on health and the environment. http://www.greenfacts.org
Bolgar M, Hubball J, Groeger J, Meronek S (2008) Handbook for the chemical analysis of plastic and polymer additives. CRC, Boca Raton
ChemicalBook (2008) ChemicalBook—chemical search engine. http://www.chemicalbook.com/
Agency for Toxic Substances & Disease Registry (2002) ATSDR - toxicological profile: di(2-ethylhexyl)phthalate (DEHP). http://www.atsdr.cdc.gov/toxprofiles/tp.asp?id=684&tid=65
Choi K, Joo H, Campbell JL, Clewell R, Andersen ME, Clewell HJ (2012) Toxicol In vitro 26:315–322
European Food Safety Authority (2008) EFSA J 653:1–131
(2003) Safety (MSDS) data for perfluorononanoic acid. .http://www.chemexper.net/PE/perfluorononanoic_acid.html
US Environmental Protection Agency (2009) Long-chain perfluorinated chemicals (PFCs) action plan. US Environmental Protection Agency, Washington
ChemSpider (2014) Royal Society of Chemistry, Cambridge. http://www.chemspider.com/
Roberts SC, Macaulay LJ, Stapleton HM (2012) Chem Res Toxicol 25:1435–1441
Covaci A, Harrad S, Abdallah MA, Ali N, Law RJ, Herzke D, de Wit C (2011) Environ Int 37:532–556
Hakk H, Letcher RJ (2003) Environ Int 29:801–828
Yamaguchi Y, Kawano M, Tatsukawa R (1998) Arch Environ Contam Toxicol 17:807–812
Feo ML, Barón E, Eljarrat E, Barceló D (2012) Anal Bioanal Chem 404:2625–2637
Dirtu AC, Van den Eede N, Malarvannan G, Ionas AC, Covaci A (2012) Anal Bioanal Chem 404:2555–2581
Van der Veen I, de Boer J (2012) Chemosphere 88:1119–1153
Meeker JD, Cooper EM, Stapleton HM, Hauser R (2013) Environ Health Perspect 121:580–585
Schindler BK, Förster K, Angerer J (2009) Anal Bioanal Chem 395:1167–1171
Schindler BK, Förster K, Angerer J (2009) J Chromatogr B 877:375–381
Bergh C, Torgrip R, Emenius G, Ostman C (2011) Indoor Air 21:67–76
Regnery J, Püttmann W (2010) Water Res 44:4097–4104
Staaf T, Ostman C (2005) J Environ Monit 7:883–887
Fries E, Puttmann W (2001) J Environ Monit 3:621–626
Abou-Donia MB (2005) J Occup Health Saf 21:408–432
Ray D (1998) Organophosphorus esters: an evaluation of chronic neurotoxic effects. MRC Institute for Environment and Health, pp 1–62
Singh G, Khurana D (2009) Neurol India 57:119–125
Gearhart JM, Jepson GW, Clewell HJ, Andersen ME, Conolly RB (1994) Environ Health Perspect 102:51–60
GEMACO Marketing (2010) Phthalate free | history. http://www.phthalate-free.de/history.htm
Calafat AM, Wong L-Y, Silva MJ, Samandar E, Preau JL, Jia LT, Needham LL (2011) Environ Health Perspect 119:50–55
Wittassek M, Koch HM, Angerer J, Brüning T (2011) Mol Nutr Food Res 55:7–31
Romero-Franco M, Hernández-Ramírez RU, Calafat AM, Cebrián ME, Needham LL, Teitelbaum S, Wolff MS, López-Carrillo L (2011) Environ Int 37:867–871
European Parliament and Council (2007) Regulation (EC) No 1907/2006 of the European Parliament and of the Council of 18 December 2006 concerning the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH), establishing a European Chemicals Agency, amending Directive 1999/45/EC and repealing Council Regulation (EEC) No 793/93 and Commission Regulation (EC) No 1488/94 as well as Council Directive 76/769/EEC and Commission Directives 91/155/EEC, 93/67/EEC, 93/105/EC and 2000/21/EC
Ventrice P, Ventrice D, Russo E, Sarro GD (2013) Environ Toxicol Pharmacol 36:88–96
Koch HM, Angerer J (2007) Int J Hyg Environ Health 210:9–19
Calafat AM, Slakman AR, Silva MJ, Herbert AR, Needham LL (2004) J Chromatogr B 805:49–56
Lau C, Anitole K, Hodes C, Lai D, Pfahles-Hutchens A, Seed J (2007) Toxicol Sci 99:366–394
Buck RC, Franklin J, Berger U, Conder JM, Cousins IT, De Voogt P, Jensen AA, Kannan K, Mabury SA, Van Leeuwen SPJ (2011) Integr Environ Asses Manag 7:513–541
Kissa E (2001) Fluorinated surfactants and repellents. Dekker, New York, p 640
Domingo JL (2012) Environ Int 40:187–195
Krafft MP, Riess JG (2009) Chem Rev 109:1714–1792
Buck RC, Murphy PM, Pabon M (2012) In: Knepper TP, Lange FT (eds) Polyfluorinated chemicals and transformation products. Handbook of environmental chemistry, vol 17. Springer, Berlin, pp 1–6
Tao L, Kannan K, Aldous KM, Mauer MP, Eadon GA (2008) Environ Sci Technol 42:3472–3478
Zhang T, Sun H, Lin Y, Wang L, Zhang X, Liu Y, Geng X, Zhao L, Li F, Kannan K (2011) J Agric Food Chem 59:11168–11176
Ma W, Kannan K, Wu Q, Bell EM, Druschel CM, Caggana M, Aldous KM (2013) Anal Bioanal Chem 405:4127–4138
Haug LS, Huber S, Becher G, Thomsen C (2011) Environ Int 37:687–693
Liu W, Xu L, Li X, Jin YH, Sasaki K, Saito N, Sato I, Tsuda S (2011) Environ Sci Technol 45:8144–8150
Guy WS, Taves DR, Brey WS Jr (1976) In: Filler R (ed) Biochemistry involving carbon-fluorine bonds. ACS symposium series, vol 28. American Chemical Society, Washington, pp 117–134
Li J, Guo F, Wang Y, Zhang J, Zhong Y, Zhao Y, Wu Y (2013) Environ Int 53:47–52
Inoue K, Okada F, Ito R, Kato S, Sasaki S, Nakajima S, Uno A, Saijo Y, Sata F, Yoshimura Y, Kishi R, Nakazawa H (2004) Environ Health Perspect 112:1204–1207
Xu W, Wang X, Cai Z (2013) Anal Chim Acta 790:1–13
European Council and Parliament (2006) Directive 2006/122/EC of the European Parliament and of the Council of 12 December 2006 amending for the 30th time Council Directive 76/769/EEC on the approximation of the laws, regulations and administrative provisions of the Member States relating to restrictions on the marketing and use of certain dangerous substances and preparations (perfluorooctane sulfonates)
Olsen GW, Chang S-C, Noker PE, Gorman GS, Ehresman DJ, Lieder PH, Butenhoff JL (2009) Toxicology 256:65–74
Haug LS, Thomsen C, Becher G (2009) Environ Sci Technol 43:2131–2136
Calafat AM, Wong L-Y, Kuklenyik Z, Reidy J, Needham LL (2007) Environ Health Perspect 115:1596–1602
Glynn A, Berger U, Bignert A, Ullah S, Aune M, Lignell S, Darnerud PO (2012) Environ Sci Technol 46:9071–9079
Yeung LWY, Miyake Y, Taniyasu S, Wang Y, Yu H, So MK, Jiang G, Wu Y, Li J, Giesy JP, Yamashita N, Lam PKS (2008) Environ Sci Technol 42:8140–8145
European Food Safety Authority (2012) EFSA J 10:2743–2747
Harju M, Heimstad ES, Herzke D, Sandanger T, Posner S, Wania F (2009) Current state of knowledge and monitoring requirements: emerging “new” brominated flame retardants in flame retarded products and the environment. Norwegian Pollution Control Authority, Oslo
Verreault J, Gebbink W, Gauthier LT, Gabrielsen GW, Letcher RJ (2007) Environ Sci Technol 41:4925–4931
Karlsson M, Julander A, van Bavel B, Hardell L (2007) Environ Int 33:62–69
Karlsson M (2006) Levels of brominated flame retardants in humans and their environment: occupational and home exposure. PhD thesis, Örebro University
Hakk H, Larsen G, Bowers J (2004) Chemosphere 54:1367–1374
Committee on Advances in Assessing Human Exposure to Airborne Pollutants, National Research Council (1991) Human exposure assessment for airborne pollutants: advances and opportunities. National Academies Press, Washington
Niesink R, de Vries J, Hollinger M (1996) Toxicology: principles and applications. CRC, Boca Raton, pp 17–38
Koch HM, Rossbach B, Drexler H, Angerer J (2003) Environ Res 93:177–185
Eriksson U, Kärrman A, Rotander A, Mikkelsen B, Dam M (2013) Environ Sci Pollut Res Int 20:7940–7948
Cornelis C, D’Hollander W, Roosens L, Covaci A, Smolders R, Van Den Heuvel R, Govarts E, Van Campenhout K, Reynders H, Bervoets L (2012) Chemosphere 86:308–314
Zheng J, Wang J, Luo X-J, Tian M, He L-Y, Yuan J-G, Mai B-X, Yang Z-Y (2010) Environ Sci Technol 44:9298–9303
Reemtsma T, Lingott J, Roegler S (2011) Sci Total Environ 409:1990–1993
Möller A, Xie Z, Caba A, Sturm R, Ebinghaus R (2012) Atmos Environ 46:346–353
Zeng F, Wen J, Cui K, Wu L, Liu M, Li Y, Lin Y, Zhu F, Ma Z, Zeng Z (2009) J Hazard Mater 169:719–725
Möller A, Ahrens L, Surm R, Westerveld J, Van Der Wielen F, Ebinghaus R, De Voogt P (2010) Environ Pollut 158:3243–3250
Stackelberg PE, Furlong ET, Meyer MT, Zaugg SD, Henderson AK, Reissman DB (2004) Sci Total Environ 329:99–113
Andresen J, Bester K (2006) Water Res 40:621–629
Ma Y, Cui K, Zeng F, Wen J, Liu H, Zhu F, Ouyang G, Luan T, Zeng Z (2013) Anal Chim Acta 786:47–53
Kim J-W, Isobe T, Chang K-H, Amano A, Maneja RH, Zamora PB, Siringan FP, Tanabe S (2011) Environ Pollut 159:3653–3659
Wang D-G, Alaee M, Byer JD, Brimble S, Pacepavicius G (2013) Sci Total Environ 445–446:329–336
Cheng Z, Nie X-P, Wang H-S, Wong M-H (2013) Environ Int 57–58:75–80
Tomy GT, Pleskach K, Ismail N, Whittle DM, Helm PA, Sverko E, Zaruk D, Marvin CH (2007) Environ Sci Technol 41:2249–2254
Frederiksen H, Skakkebaek NE, Andersson A-M (2007) Mol Nutr Food Res 51:899–911
Tsumura Y, Ishimitsu S, Kaihara A, Yoshii K, Nakamura Y, Tonogai Y (2001) Food Addit Contam 18:569–579
Wormuth M, Scheringer M, Vollenweider M, Hungerbühler K (2006) Risk Anal 26:803–824
European Food Safety Authority (2005) Opinion of the Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food (AFC) on a request from the Commission related to butylbenzylphthalate (BBP) for the use in food contact materials. Available via http://www.efsa.europa.eu/en/efsajournal/pub/241.htm
Harrad S, de Wit CA, Abdallah MA-E, Bergh C, Björklund J, Covaci A, Darnerud PO, de Boer J, Diamond M, Huber S, Leonards P, Mandalakis M, Ostman C, Haug LS, Thomsen C, Webster TF (2010) Environ Sci Technol 44:3221–3231
Ionas AC, Covaci A (2013) Int J Environ Anal Chem 93:1074–1083
Zhu J, Hou Y, Feng Y-L, Shoeib M, Harner T (2008) Environ Sci Technol 42:386–391
Beesoon S, Genuis SJ, Benskin JP, Martin JW (2012) Environ Sci Technol 46:12960–12967
Shoeib M, Harner T, M Webster G, Lee SC (2011) Environ Sci Technol 45:7999–8005
Wang W, Wu F-Y, Huang M-J, Kang Y, Cheung KC, Wong MH (2013) J Hazard Mater 261:753–762
Stapleton HM, Allen JG, Kelly SM, Konstantinov A, Klosterhaus S, Watkins D, McClean MD, Webster TF (2008) Environ Sci Technol 42:6910–6916
Zhu J, Feng Y-L, Shoeib M (2007) Environ Sci Technol 41:7694–768
Dirtu AC, Ali N, Van den Eede N, Neels H, Covaci A (2012) Environ Int 49:1–8
Harrad S, Goosey E, Desborough J, Abdallah MA-E, Roosens L, Covaci A (2010) Environ Sci Technol 44:4198–4202
Van Den Eede N, Dirtu AC, Neels H, Covaci A (2011) Environ Int 37:454–461
Cao Z-G, Yu G, Chen Y-S, Cao Q-M, Fiedler H, Deng S-B, Huang J, Wang B (2012) Environ Int 49:24–30
Cao Z, Yu G, Chen Y, Liu C, Liu K, Zhang T, Wang B, Deng S, Huang J (2013) J Hazard Mater 252–253:11–18
Yamamoto N, Takahashi Y, Yoshinaga J, Tanaka A, Shibata Y (2006) Arch Environ Contam Toxicol 51:157–163
Stapleton HM, Kelly SM, Allen JG, Mcclean MD, Webster TF (2008) Environ Sci Technol 42:3329–3334
Stapleton HM, Eagle S, Sjödin A, Webster TF (2012) Environ Health Perspect 120:1049–1054
Watkins DJ, McClean MD, Fraser AJ, Weinberg J, Stapleton HM, Sjödin A, Webster TF (2011) Environ Health Perspect 119:1247–1252
Koo HJ, Lee BM (2004) J Toxicol Environ Health A 67:1901–1914
Lien G-W, Huang C-C, Wu K-Y, Chen M-H, Lin C-Y, Chen C-Y, Hsieh W-S, Chen P-C (2013) Chemosphere 92:843–850
Salthammer T, Fuhrmann F, Uhde E (2003) Indoor Air 13:49–52
Salthammer T, Bahadir M (2009) Clean Soil Air Water 37:417–435
Bergh C, Luongo G, Wise S, Ostman C (2012) Anal Bioanal Chem 402:51–59
Wang D-G, Yang M, Qi H, Sverko E, Ma W-L, Li Y-F, Alaee M, Reiner EJ, Shen L (2010) Environ Sci Technol 44:6608–6613
Shi T, Chen S-J, Luo X-J, Zhang X-L, Tang C-M, Luo Y, Ma Y-J, Wu J-P, Peng X-Z, Mai B-X (2009) Chemosphere 74:910–916
Saito I, Onuki A, Seto H (2007) Indoor Air 17:28–36
Fogelholm M (1995) Int J Sport Nutr 5:267–284
Lillsunde P, Michelson L, Forsstriim T, Korte T, Schultz E, Ariniemi K, Portman M, Sihvonenb M, Seppälä T (1996) Forensic Sci Int 77:191–210
Sjödin A, Hagmar L, Klasson-Wehler E, Kronholm-Diab K, Jakobsson E, Bergman A (1999) Environ Health Perspect 107:643–648
Luque N, Ballesteros-Gómez A, van Leeuwen S, Rubio S (2012) J Chromatogr A 1235:84–91
Schramm K-W, Kuettner T, Weber SLK (1992) Chemosphere 24:351–358
Nakao T, Aozasa O, Ohta S, Miyata H (2005) Arch Environ Contam Toxicol 49:124–130
Halldorsson TI, Fei C, Olsen J, Lipworth L, McLaughlin JK, Olsen SF (2008) Environ Sci Technol 42:8971–8977
Toms L-ML, Calafat AM, Kato K, Thompson J, Harden F, Hobson P, Sjödin A, Mueller JF (2009) Environ Sci Technol 43:4194–4199
Ehresman DJ, Froehlich JW, Olsen GW, Chang S-C, Butenhoff JL (2007) Environ Res 103:176–184
Beesoon S, Webster GM, Shoeib M, Harner T, Benskin JP, Martin JW (2011) Environ Health Persp 119:1659–1664
Midasch O, Drexler H, Hart N, Beckmann MW, Angerer J (2007) Int Arch Occup Environ Health 80:643–648
Kato K, Wanigatunga AA, Needham LL, Calafat AM (2009) Anal Chim Acta 656:51–55
Spliethoff HM, Tao L, Shaver SM, Aldous KM, Pass KA, Kannan K, Eadon GA (2008) Environ Sci Technol 42:5361–5367
Post GB, Cohn PD, Cooper KR (2012) Environ Res 116:93–117
Parsons JR, Sáez M, Dolfing J, de Voogt P (2008) In: Whitacre DM (ed) Reviews of environmental contamination and toxicology, vol 196. Springer, New York, pp 53–71
Frederiksen H, Jørgensen N, Andersson A-M (2010) J Anal Toxicol 34:400–410
Koch HM, Bolt HM, Angerer J (2004) Arch Toxicol 78:123–130
Silva MJ, Barr DB, Reidy JA, Malek NA, Hodge CC, Caudill SP, Brock JW, Needham LL, Calafat AM (2013) Environ Health Perspect 112:331–338
Preuss R, Koch HM, Angerer J (2005) J Chromatogr B 816:269–280
Kato K, Silva MJ, Wolf C, Gray LE, Needham LL, Calafat AM (2007) Toxicology 236:114–122
Koch HM, Bolt HM, Preuss R, Angerer J (2005) Arch Toxicol 79:367–376
Silva MJ, Reidy J, Preau JL, Needham LL, Calafat AM (2006) Environ Health Perspect 114:1158–1161
Buttke DE, Sircar K, Martin C (2012) Environ Health Perspect 120:1613–1618
Hoppin JA, Jaramillo R, London SJ, Bertelsen RJ, Salo PM, Sandler DP, Zeldin DC (2013) Environ Health Perspect 121:1129–1134
Hines EP, Calafat AM, Silva MJ, Mendola P, Fenton SE (2009) Environ Health Perspect 117:86–92
LaKind JS (2012) Environ Int 35:994–995
US Food Drug Administration (2011) Safety assessment of di-(2-ethylhexyl) phthalate (DEHP) released from PVC medical devices. US Food and Drug Administration, Rockville
Centers for Disease Control and Prevention (2013) Fourth national report on human exposure to environmental chemicals. Department of Health and Human Services, Centers for Disease Control, Atlanta
Koizumi A, Yoshinaga T, Harada K, Inoue K, Morikawa A, Muroi J, Inoue S, Eslami B, Fujii S, Fujimine Y, Hachiya N, Koda S, Kusaka Y, Murata K, Nakatsuka H, Omae K, Saito N, Shimbo S, Takenaka K, Takeshita T, Todoriki H, Wada Y, Watanabe T, Ikeda M (2005) Environ Res 99:31–39
Thuresson K, Höglund P, Hagmar L, Sjödin A, Bergman Å, Jakobsson K (2006) Environ Health Perspect 114:176–181
Schoeters G, Colles A, Den Hond E, Croes K, Vrijens J, Baeyens W, Nelen V, Van De Mieroop E, Covaci A, Bruckers L, Van Larebeke N, Sioen I, Morrens B, Loots I (2012) In: Knudsen L, Merlo DF (eds) Biomarkers and human biomonitoring. Royal Society of Chemistry, pp 135–165
Zhu L, Ma B, Hites R (2009) Environ Sci Technol 43:6963–6968
He S, Li M, Jin J, Wang Y, Bu Y, Xu M, Yang X, Liu A (2013) Environ Toxicol Chem 32:1242–1247
Zhang H, Wang P, Li Y, Shang H, Wang Y, Wang T, Zhang Q, Jiang G (2013) Environ Sci Technol 47:10567–10573
Ben Y-J, Li X-H, Yang Y-L, Li L, Di J-P, Wang W-Y, Zhou R-F, Xiao K, Zheng M-Y, Tian Y, Xu X-B (2013) Environ Pollut 173:176–181
Smolders R, Schramm K-W, Nickmilder M, Schoeters G (2009) Environ Health 8:1–10
Cooper G, Kronstrand R, Kintz P (2012) Forensic Sci Int 218:20–24
Perez F, Llorca M, Farré M, Barceló D (2012) Anal Bioanal Chem 402:2369–2378
Li J, Guo F, Wang Y, Liu J, Cai Z, Zhang J, Zhao Y, Wu Y (2012) J Chromatogr A 1219:54–60
Allen JG, Stapleton HM, Vallarino J, Mcneely E, Mcclean MD, Harrad SJ, Rauert CB, Spengler JD (2013) Environ Health 12:17
Chang Y-J, Lin K-L, Chang Y-Z (2013) Clin Chim Acta 420:155–159
Silva MJ, Reidy JA, Samandar E, Herbert AR, Needham LL, Calafat AM (2005) Arch Toxicol 79:647–652
Barr DB, Wang RY, Needham LL (2005) Environ Health Perspect 113:1083–1091
Esteban M, Castaño A (2009) Environ Int 35:438–449
Zhang Y, Beesoon S, Zhu L, Martin JW (2013) Environ Sci Technol 47:10619–10627
Blount BC, Silva MJ, Caudill SP, Needham LL, Pirkle JL, Sampson EJ, Lucier GW, Jackson RJ, Brock JW (2000) Environ Health Perspect 108:979–982
Suzuki Y, Niwa M, Yoshinaga J, Watanabe C, Mizumoto Y, Serizawa S, Shiraishi H (2009) Environ Health Prev Med 14:180–187
Hoppin J, Brock JW, Davis BJ, Baird DD (2002) Environ Health Perspect 110:515–518
Hauser R, Meeker JD, Park S, Silva MJ, Calafat AM (2004) Environ Health Perspect 112:1734–1740
Teitelbaum SL, Britton J, Calafat A, Ye X, Silva MJ, Reidy J, Galvez MP, Brenner BL, Wolff MS (2008) Environ Res 106:257–269
Adibi JJ, Perera FP, Jedrychowski W, Camann DE, Barr D, Jacek R, Whyatt RM (2003) Environ Health Perspect 111:1719–1722
Swan SH, Main KM, Liu F, Stewart SL, Kruse RL, Calafat AM, Mao CS, Redmon JB, Ternand CL, Sullivan S, Teague JL (2005) Environ Health Perspect 113:1056–1061
Möller K, Crescenzi C, Nilsson U (2004) Anal Bioanal Chem 378:197–204
Cooper EM, Covaci A, van Nuijs ALN, Webster TF, Stapleton HM (2011) Anal Bioanal Chem 401:2123–2132
Spearman RIC (1977) In: Jarrett A (ed) The hair folicule. The physiology and pathophysiology of the skin, vol 4. Academic, New York, pp 1255–1292
Covaci A, Tutudaki M, Tsatsakis AM, Schepens P (2002) Chemosphere 46:413–418
D’Havé H, Covaci A, Scheirs J, Schepens P, Verhagen R, De Coen W (2005) Environ Sci Technol 39:6016–6020
Esteban M, Schindler E, Jimenez J, Holger K, Angerer J, Castaño A (2011) DEMOCOPHES – train the trainers, training module 1: fieldwork preanalytical phase 2. Berlin
Wennig R (2000) Forensic Sci Int 107:5–12
Schramm K-W (2008) Chemosphere 72:1103–1011
Kintz P, Villain M (2005) In: Tobin DJ (ed) Hair in toxicology: an important biomonitor. Royal Society of Chemistry, Cambridge, pp 89–95
Pragst F, Balikova M (2006) Clin Chim Acta 370:17–49
Wang T, Fu J, Wang Y, Liao C, Tao Y, Jiang G (2009) Environ Pollut 157:2445–2451
Tsatsakis AM, Psillakis TK, Tzatzarakis M, Kourtopoulos H, Paritsis N (1997) Clin Chim Acta 263:187–195
Nakahara Y (1999) J Chromatogr B 733:161–180
Kintz P, Ginet M, Marques N, Cirimele V (2007) Forensic Sci Int 170:204–206
Altshul L, Covaci A, Hauser R (2004) Environ Health Perspect 112:1193–1199
Zhang H, Chai Z, Sun H (2007) Environ Int 33:685–693
Zhao G, Wang Z, Dong MH, Rao K, Luo J, Wang D, Zha J, Huang S, Xu Y, Ma M (2008) Sci Total Environ 397:46–57
Leung AOW, Chan JKY, Xing GH, Xu Y, Wu SC, Wong CKC, Leung CKM, Wong MH (2010) Environ Sci Pollut Res 17:1300–1313
Tadeo JL, Sánchez-Brunete C, Miguel E (2009) Talanta 78:138–143
Aleksa K, Carnevale A, Goodyer C, Koren G (2012) Forensic Sci Int 218:37–43
Malarvannan G, Isobe T, Covaci A, Prudente M, Tanabe S (2013) Sci Total Environ 442:366–379
Zheng J, Xiao-Jun L, Jian-Gang Y, Jing W, Yu-Tao W, Shen-Jun C, Bi-Xian M, Zhong-Yi Y (2011) Envion Pollut 159:3706–3713
Kucharscha A, Covaci A, Voorspoels S (2013) In: Conference proceedings of “The 33rd international symposium on halogenated persistent organic pollutants and POPs (dioxin)”, Daegu, South Korea
Barbosa F, Tanus-Santos JE, Gerlach RF, Parsons PJ (2005) Environ Health Perspect 113:1669–1674
Button M, Jenkin GRT, Harrington CF, Watts MJ (2009) J Environ Monit 11:610–617
Suzuki T, Watanabe S, Matsuo N (1989) J Ind Health 31:235–238
Katayama Y, Ishida N (1987) Radioisotopes 36:103–107
Mehra R, Juneja M (2005) J Sci Ind Res India 64:119–124
Luque N, Ballesteros-Gómez A, van Leeuwen S, Rubio S (2010) J Chromatogr A 1217:3774–3782
Schenkels LCPM, Veerman ECI, Nieuw Amerongen AV (1995) Crit Rev Oral Biol Med 6:161–175
Neyraud E, Palicki O, Schwartz C, Nicklaus S, Feron G (2012) Arch Oral Biol 57:556–566
Aps JKM, Martens LC (2005) Forensic Sci Int 150:119–131
Höld KM, de Boer D, Zuidema J, Maes R (1995) J Chromatogr B 663:103–110
Moore C (2011) Drug Test Anal 3:166–168
Quintela O, Crouch DJ, Andrenyak DM (2006) J Anal Toxicol 30:614–616
Schramm W, Smith RH, Craig PA, Kidwell DA (1992) J Anal Toxicol 16:1–9
Bulgaroni V, Rovedatti MG, Sabino G, Magnarelli G (2012) Environ Monit Assess 184:3307–3314
Ogawa T, Asai Y, Yamashita M, Takasuga T (2003) J Dent Res 82:849–853
Tao L (2011) Biomonitoring of perfluorochemicals in human blood. PhD thesis, State Univeristy of New York at Albany
Silva MJ, Samandar E, Preau JL, Reidy JA, Needham LL, Calafat A (2005) J Anal Toxicol 29:819–824
Watkins DJ, McClean MD, Fraser AJ, Weinberg J, Stapleton HM, Sjödin A, Webster TF (2012) Environ Sci Technol 46:1192–200
Wilson NK, Chuang JC, Lyu C, Menton R, Morgan MK (2003) J Expo Anal Environ Epidemiol 13:187–202
Watkins DJ, McClean MD, Fraser AJ, Weinberg J, Stapleton HM, Webster TF (2013) Environ Int 59C:124–132
Gordon SM, Callahan PJ, Nishioka MG, Brinkman MC, O’Rourke MK, Lebowitz MD, Moschandreas DJ (1999) J Expo Anal Environ Epidemiol 9:456–470
Amini N, Crescenzi C (2003) J Chromatogr B 795:245–256
Van Den Eede N, Neels H, Jorens PG, Covaci A (2013) J Chromatogr A 1303:48–53
DEMOCOPHES — COPHES. http://www.eu-hbm.info/democophes
Martin J, Kannan K, Berger U, de Voogt P, Field J, Franklin J, Giesy J, Harner T, Muir D, Scott B, Kaiser M, Jarnberg U, Jones K, Mabury S, Schroeder H, Simcik M, Sottani C, Bavel B, Karrman A, Lindström G, Van Leeuwen S (2004) Environ Sci Technol 38(13):248A–255A
Muto M, Isobe T, Ramu K, Tue NM, Viet PH, Takahashi S, Tanabe S (2012) In: Kawaguchi M, Misaki K, Sato H, Yokokawa T, Itai T, Nguyen TM, Ono J (eds) Interdisciplinary studies on environmental chemistry-environmental pollution and ecotoxicology. Terrapub, Tokyo, pp 229–237
Kucharscha A, Covaci A, Voorspoels S (2013). In: Conference proceedings of “The 33rd international symposium on halogenated persistent organic pollutants and POPs (dioxin)”, Daegu, South Korea
Benskin JP, Holt A, Martin JW (2009) Environ Sci Technol 43:8566–8572
Kemper R, Nabb DL (2005) Drug Chem Toxicol 28:281–287
Choi K, Joo H, Campbell JL, Andersen ME, Clewell HJ (2013) Toxicol In Vitro 27:1451–1457
Hanioka N, Takahara Y, Takahara Y, Tanaka-Kagawa T, Jinno H, Narimatsu S (2012) Chemosphere 89:1112–1117
Janjua NR, Frederiksen H, Skakkebaek NE, Wulf HC, Andersson A-M (2008) Int J Androl 31:118–130
Carignan CC, McClean MD, Cooper EM, Watkins DJ, Fraser AJ, Heiger-Bernays W, Stapleton HM, Webster TF (2013) Environ Int 55:56–61
Silva MJ, Samandar E, Reidy J, Hauser R, Needham LL, Calafat AM (2007) Environ Sci Technol 41:7576–7580
Picard K, Lhuguenot JC, Lavier-Canivenc MC, Chagnon MC (2001) Toxicol Appl Pharmacol 172:108–118
Silva MJ, Reidy J, Preau JL, Samandar E, Needham LL, Calafat AM (2006) Biomarkers 11:1–13
Frederiksen H, Kranich SK, Jørgensen N, Taboureau O, Petersen JH, Andersson A-M (2013) Environ Sci Technol 47:958–967
Preau JL, Wong L-Y, Silva MJ, Needham LL, Calafat AM (2010) Environ Health Perspect 118:1748–1754
Burka LT, Sanders JM, Herr DW, Matthews HB (1990) Drug Metab Dispos 19:443–447
Lynn RK, Wong K, Galvie-Gould C, Kennish JM (1981) Drug Metab Dispos 9:434–441
Nomeir AA, Kato S, Matthews HB (1981) Toxicol Appl Pharmacol 57:401–413
Houde M, Berryman D, De la Lafontaine Y, Verreault J (2014) Sci Total Environ 479–480:48–56
European Chemicals Agency (2014) Homepage - ECHA. http://echa.europa.eu/
Lehmler HJ (2005) Chemosphere 58:1471–1496
Jackson DA, Mabury SA (2012) Environ Toxicol Chem 31:1966–1971
European Workplace Drug Testing Society (2013) Home -ewdts. http://www.ewdts.org
Society of Toxicological and Forensic Chemistry (2008–2014) GTFCh homepage. http://www.gtfch.org
Keller JM, Calafat AM, Kato K, Ellefson ME, Reagen WK, Strynar M, O’Connell S, Butt CM, Mabury SA, Small J, Muir DCG, Leigh SD, Schantz MM (2010) Anal Bioanal Chem 397:439–451
Salihovic S, Kärrman A, Lindström G, Lind PM, Lind L (2013) J Chromatogr A 1305:164–170
Gill U, Covaci A, Ryan JJ, Emond A (2004) Anal Bioanal Chem 380:924–929
Palicki O, Schwartz C, Nicklaus S, Feron G (2012) Arch Oral Biol 57:556–566
Acknowledgments
The authors acknowledge the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement no. 316665 (project A-TEAM) and grant agreement no. 264600 (project INFLAME) for the funding of PhD grants (Marie Curie Actions funding program) for A.A., A.K., and F.X. and for a postdoctoral grant for C.E.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Alves, A., Kucharska, A., Erratico, C. et al. Human biomonitoring of emerging pollutants through non-invasive matrices: state of the art and future potential. Anal Bioanal Chem 406, 4063–4088 (2014). https://doi.org/10.1007/s00216-014-7748-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-014-7748-1