
Abstract
Trialkyl esters of phosphoric acid are widely used as flame retardants. The corresponding dialkylphosphates are formed as the main metabolites in animal experiments. We extended a previously published method for the determination of four organophosphorus flame retardant metabolites [bis(2-chloroethyl) phosphate, diphenyl phosphate, di-m-cresyl phosphate and di-p-cresyl phosphate] to be able to determine di-n-butyl phosphate (DBP) and bis(2-chloropropyl) phosphate (BCPP) in human urine samples additionally in one run. After solid-phase extraction, derivatization with pentafluorobenzyl bromide and further solid-phase cleanup, the extracts were analysed by gas chromatography–tandem mass spectrometry. The limits of detection were 0.25 µg/l for both analytes. Interday imprecisions were 2–6%. To show the applicability of the method, the internal burden of 25 persons of the population was determined. Twelve percent of the urine samples analysed tested positive for BCPP at concentrations from below the limit of detection to 0.85 µg/l; one sample contained 0.26 µg/l DBP.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several studies proved the ubiquitousness of organophosphorus flame retardants (OPFRs), phosphoric acid triesters, in several environmental matrices, such as soil, water and air [1–9]. Two OPFRs, tri-n-butyl phosphate (TBP) and tris(2-chloropropyl) phosphate (TCPP), are of interest for this study because of high production volumes and considerable toxicological relevance. TBP had a worldwide production volume of up to 5,000 tonnes in 2001 [10]. It is used in aircraft hydraulic fluids and as an additive in coatings and floor finishers to provide plasticizing and flame-retarding properties. Furthermore, it is used as a solvent for extraction of rare-earth elements. TCPP is used as a flame retardant in rigid and flexible polyurethane foams and had a production volume of more than 40,000 tonnes worldwide in 1997 [11]. In recent years, TCPP has been predominantly used as a substitute for tris(2-chloroethyl) phosphate. TBP is known from animal experiments to be a carcinogen and fetotoxic toxicant [12–15]. TCPP is suspected to be carcinogenic [16].
TBP and TCPP are rapidly resorbed and distributed throughout the whole body in animal experiments [17, 18]. In blood and urine of animals the OPFRs are hydrolysed spontaneously or enzymatically by α-esterases and phosphorylphosphatases to form the corresponding dialkyl phosphates as the main metabolites [10, 17, 19, 20]. Owing to the toxicity and the broad applicability of TBP and TCPP, it is necessary to determine if and to what extent the general population is burdened by the use of those OPFRs.
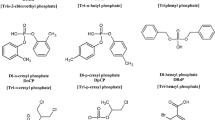
Therefore, a sensitive and selective method was developed to determine di-n-butyl phosphate (DBP) and bis(2-chloropropyl) phosphate (BCPP) (Fig. 1), the main metabolites of TBP and TCPP in human urine samples.

Structures of the flame retardants, the metabolites analysed and the corresponding internal standards
We recently published the first method for human biomonitoring of four OPFRs [21]. The present method is an enhancement of that previously published method. The applicability is shown by analysis of the internal burden of 25 persons of the general population of southern Germany.
Experimental
Chemicals and reagents
Deionized water was prepared by a Milli-Q Plus system (Millipore, Eschborn, Germany).
Acetonitrile (lichrosolv, seccosolv), acetone, hexane, toluene, hydrochloric acid (37%) and potassium carbonate were purchased from Merck (Darmstadt, Germany). 2,3,4,5,6-Pentafluorobenzyl bromide was purchased from Aldrich Chemical (Steinheim, Germany).
Five grams of 2,3,4,5,6-pentafluorobenzyl bromide was diluted in 6 ml of acetonitrile (seccosolv) and used as the reagent for derivatization. Isolute ENV+ cartridges were obtained from Biotage (Uppsala, Sweden). Bond Elut PSA (500 mg, 3 ml) and Bond Elut FL (500 mg, 3 ml) cartridges were obtained from Varian (Middelburg, The Netherlands).
DBP (purity 97%) was purchased from Fluka (Deisenhofen, Germany). BCPP (purity greater than 91%) and the labelled standards DBP-d 18 (purity greater than 96%) and BCPP-d 2 (purity greater than 98%) were custom-synthesized by Kadem Custom Chem (Göttingen, Germany).
Instrumentation
The gas chromatography–tandem mass spectrometry (GC-MS/MS) system consists of a gas chromatograph (CP-3800, Varian, Darmstadt, Germany) and an autosampler (CP-8400, Varian, Darmstadt, Germany) coupled to a triple-quadrupole mass spectrometer (1200 L, Varian, Darmstadt, Germany). A Varian VF-35 ms (35% phenyl-methylpolysiloxane) capillary column (60 m, 0.25-mm inner diameter, 0.25 µm; Varian, Darmstadt, Germany) was used. The Varian Workstation 6.41 software program was used for analysis.
Standard preparation
Stock solutions (1 g/l) in acetonitrile were prepared for DBP and BCPP. The stock solutions (1 g/l) were diluted to a mixed standard working solution with water to a concentration of 10 mg/l. Five calibration standards in concentrations between 5 and 50 µg/l were prepared in pooled urine. The calibration standards were aliquoted in 5-ml portions.
Stock solutions of the two deuterium-labelled standards (DBP-d 18, BCPP-d 2; Fig. 1), both 1 g/l, were prepared in acetonitrile and diluted to a mixed internal standard working solution with acetonitrile (both 10 mg/l). All solutions and calibration standards were stored at -18°C in the dark.
Sample preparation and solid-phase extraction
The sample preparation was performed as published elsewhere [21]. In short, the urine samples are acidified, spiked with 20 µl internal standard solution and enriched by means of solid-phase extraction using ENV+ cartridges. For derivatization, 2,3,4,5,6-pentafluorobenzyl bromide is added to the acetonitrile extracts. In a second solid-phase extraction, further cleanup is performed and excessive derivatization agent is removed. After concentration, the measurement is accomplished by GC-MS/MS.
Instrumental analysis
Analysis was performed by injecting 1 µl of each sample splitlessly onto a capillary column. Helium was used as the carrier gas at a flow rate of 1.5 ml/min. The injector was set to 260°C and the transfer line to 280°C. The temperature of the source was 200°C. The column temperature was 80°C initially for 0.5 min. At a rate of 25°C/min it was raised to 110°C and held for 1 min. Then it was raised to 270°C at a rate of 25°C/min and to 290°C at a rate of 20°C/min, held for 2 min and raised to a final temperature of 300°C, where it was held for 8 min. The two analytes were eluted in less than 14 min. The analyte peaks were identified by quantitation and confirmation ions for each pentafluorobenzyl OPFR metabolite as shown in Table 1.
Study subject and sample collection
To show the applicability of the validated method, 25 spot urine samples, randomly selected from a south-German population, were analysed. None of the study subjects was occupationally exposed to OPFRs. The demographic characteristics are as follows: 12 females and 13 males, aged between 24 and 57 years, with a median of 41 years. All but one were nonsmokers. Creatinine levels ranged from 0.26 to 1.45 g/l, with a median of 0.72 g/l. The samples were stored without any pretreatment in polyethylene containers until analysis.
Daily operation and quality-control procedure
Pooled urine samples of multiple donors, spiked with standard solution to two concentrations, 10 and 30 µg/l, served as quality-control material. The two control materials, one blank water sample and a full calibration sample, were extracted and analysed in each run along with the samples. Calibration was performed by plotting the ratio of the peak area of the standard to the internal standard versus the concentration using the Varian Workstation 6.41 software program with a regression weighting of 1/x.
Method validation
A signal-to-noise ratio of 3 for the quantifier ion trace was defined as the limit of detection (LOD). We assessed the imprecision of the method by intraday and interday reproducibility. The reproducibility was studied by eightfold analysis of urine samples spiked in two concentrations, 10 µg/l (Q low) and 30 µg/l (Q high). Relative recoveries were ascertained by analysis of eight different urine samples with creatinine levels of 0.23–3.27 g/l which were spiked with standard solution to two concentrations, 20 µg/l (c low) and 40 µg/l (c high). The ratios of the peak area of the analyte and the internal standard were compared with the calibration graph to obtain the relative recovery. Confirmation ions were used to confirm a detected peak as the target analyte. The ratio of the quantitation ion to the confirmation ion had to be consistent with the ratio determined from standards. Variations of less than 20% of the ratio of the quantitation ion to the confirmation ion were accepted. The exact differences in the retention time of standards and internal standards are given in Table 1.
Results and discussion
We extended our previously published method [21] for the determination of metabolites of OPFRs in human urine samples. DBP and BCPP could be analysed together with four other OPFR metabolites in one run. Figure 2 shows a GC-MS/MS chromatogram of a native urine sample containing 0.26 µg/l DBP and 0.85 µg/l BCPP as well as bis(2-chloroethyl) phosphate and diphenyl phosphate. Di-m-cresyl phosphate and di-p-cresyl phosphate could only be detected in spiked urine samples.

Gas chromatography–tandem mass spectrometry chromatogram of a native urine sample containing 0.26 µg/l di-n-butyl phosphate (DBP) and 0.85 µg/l bis(2-chloropropyl) phosphate (BCPP). BCEP bis(2-chloroethyl) phosphate, DPP diphenyl phosphate, DmCP di-m-cresyl phosphate, DpCP di-p-cresyl phosphate
During the validation process the method proved to be robust and reliable. Deuterium-labelled internal standards for each analyte are indispensable to achieve the demonstrated validation data, summarized in Table 2.
The LODs were 0.25 µg/l for DBP and BCPP. The high sensitivity and selectivity of the method is obvious. The calibration curves were linear for the whole measuring range, with Pearson coefficients of correlation greater than 0.999.
Eight different urine samples, spiked to two different concentrations, were analysed to determine the relative recoveries and to reflect the absence of matrix effects. The mean relative recoveries (range) were 97.2% (94–101%) and 97.5% (95–102%) for 20 and 40 µg/l DBP, respectively, and 100.6% (91–111%) and 100.8% (94–108%) for the two concentrations of BCPP. Considering those values, the method showed good accuracy and high robustness for extremely varying urine matrices. The native concentrations of the eight urine samples were found to be less than the LOD (DBP) and less than the LOD to 2.5 µg/l BCPP.
Intraday imprecisions were 3.5% (DBP) and 5.0% (BCPP) for Q low and 2.9% (DBP) and 3.5% (BCPP) for Q high. The interday imprecisions determined on eight different days were 5.2% (DBP) and 5.5% (BCPP) for Q low and 3.7% (DBP) and 1.8% (BCPP) for Q high. Those values for the imprecision point out that the present method produces highly reproducible results.
None of the blank water samples contained any traces of the analytes; therefore, blank-related problems and artefacts from the labelled internal standards can be excluded.
The validated method was applied to examine 25 native urine samples from the general population. DBP could be determined in one urine sample at a concentration of 0.26 µg/l. BCPP was determined in 12% of the urine samples analysed in concentrations between less than the LOD and 0.85 µg/l. We were able to demonstrate that this method is sensitive enough to detect background levels in the general population as well as higher concentrations as expected for occupationally exposed workers. Our results indicate that parts of the general population are exposed to OPFRs. In particular, bis(2-chloroethyl) phosphate (50%), diphenyl phosphate (30%) and BCPP (12%) could be determined in urine samples of the general population. Representative studies are necessary to confirm those results.
Conclusions
Our previously published method could be extended for the determination of two additional metabolites of OPFRs. After solid-phase extraction, derivatization and a second solid-phase extraction step, trace-level concentrations of six OPFR metabolites could be determined in one run. High reproducibility, reliability, robustness, sensitivity and selectivity characterize this method. As a result of the excellent sample cleanup, minimal system maintenance is required. Owing to the high sensitivity of the method, it is possible to determine native concentrations of OPFR metabolites in human urine samples for the first time. Background levels in the general population of Germany can now be ascertained. With the detection of DBP and BCPP, it has been proven that those metabolites are formed and excreted via urine. This provides a first glance at the human metabolism of OPFRs.
References
Andresen J, Bester K (2006) Water Res 40:621–629
Andresen JA, Grundmann A, Bester K (2004) Sci Total Environ 332:155–166
Fries E, Püttmann W (2001) J Environ Monit 3:621–626
Fries E, Püttmann W (2003) J Environ Monit 5:346–352
Ingerowski G, Friedle A, Thumulla J, Sagunski H (1997) Umweltmed Forsch Prax 2:233–235
Kersten W, Reich T (2003) Gefahrstof Reinhalt Luft 63:85–91
Martinez-Carballo E, Gonzalez-Barreiro C, Sitka A, Scharf S, Gans O (2007) Sci Total Environ 388:290–299
Nagorka R, Ullrich D (2003) Gefahrstof Reinhalt Luft 63:79–84
Reemtsma T, García-López M, Rodríguez I, Quintana JB, Rodil R (2008) Trends Anal Chem 27:727–737
OECD (2001) Tributylphosphate. SIDS initial assessment report, unep publications. http://www.inchem.org/documents/sids/sids/126-73-8.pdf
National Research Council (2000) Toxicological risks of selected flame-retardant chemicals. National Academies Press, Washington
Forschungsgemeinschaft D (2008) MAK- und BAT-Werte Liste 2008. Wiley-VCH, Weinheim
National Institute for Occupational Safety and Health (2005) Tributyl phosphate. International chemical safety cards. http://www.cdc.gov/niosh/ipcsneng/neng0584.html
National Institute for Occupational Safety and Health (2005) Tributyl phosphate. NIOSH pocket guide to chemical hazards. http://www.cdc.gov/niosh/npg/npgd0625.html
SOCMA (1991) (Synthetic Organic Chemical Manufacturer Association Inc) A development toxicity study in rats with tributyl phosphate. Tributyl Phosphate Task Force, Biodynamics Inc. 89-3535
Bayrisches Landesamt für Umwelt (2006) Chemikalien in der Umwelt—Vorkommen, Belastungspfade, Regelungen. Bayer. Landesamt für Umwelt, Augsburg
IPCS (1991) Tri-n-butyl phosphate. Environmental health criteria 112. World Health Organization, Geneva
Minegishi K-I, Kurebayashi H, Nambaru S, Morimoto K, Takahashi T, Yamaha T (1988) Eisei Kagaku 34:102–114
IPCS (1998) Flame retardants: tris(chloropropyl) phosphate and tris(2-chloroethyl) phosphate. Environmental health criteria 209. World Health Organization, Geneva
Marquardt H, Schäfer S (2004) Lehrbuch der Toxikologie. Wissenschaftliche Verlagsgesellschaft, Stuttgart
Schindler BK, Förster K, Angerer J (2009) J Chromatogr B 877:375–381
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schindler, B.K., Förster, K. & Angerer, J. Quantification of two urinary metabolites of organophosphorus flame retardants by solid-phase extraction and gas chromatography–tandem mass spectrometry. Anal Bioanal Chem 395, 1167–1171 (2009). https://doi.org/10.1007/s00216-009-3064-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-009-3064-6