
Abstract
Rationale
Accumulating evidence indicates that the mixed serotonin and dopamine receptor agonist lysergic acid diethylamide (LSD) induces an altered state of consciousness that resembles dreaming.
Objectives
This study aimed to test the hypotheses that LSD produces dreamlike waking imagery and that this imagery depends on 5-HT2A receptor activation and is related to subjective drug effects.
Methods
Twenty-five healthy subjects performed an audiorecorded guided mental imagery task 7 h after drug administration during three drug conditions: placebo, LSD (100 mcg orally) and LSD together with the 5-HT2A receptor antagonist ketanserin (40 mg orally). Cognitive bizarreness of guided mental imagery reports was quantified as a standardised formal measure of dream mentation. State of consciousness was evaluated using the Altered State of Consciousness (5D-ASC) questionnaire.
Results
LSD, compared with placebo, significantly increased cognitive bizarreness (p < 0.001). The LSD-induced increase in cognitive bizarreness was positively correlated with the LSD-induced loss of self-boundaries and cognitive control (p < 0.05). Both LSD-induced increases in cognitive bizarreness and changes in state of consciousness were fully blocked by ketanserin.
Conclusions
LSD produced mental imagery similar to dreaming, primarily via activation of the 5-HT2A receptor and in relation to loss of self-boundaries and cognitive control. Future psychopharmacological studies should assess the differential contribution of the D2/D1 and 5-HT1A receptors to cognitive bizarreness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The effects of serotonergic or classic psychedelics such as the semisynthetic lysergic acid diethylamide (LSD) share distinct phenomenological similarities with night sleep dreaming, such as vivid sensorimotor imagery, alterations in thought processes, disinhibition of basic emotions and needs and changes in the feeling and control of the self (Hobson 2001; Fischman 1983; Jacobs 1978; Savage 1955).
The notion that psychedelics produce a dreamlike state in humans is supported by phenomenological, neurophysiological and pharmacological evidence. Early research with LSD showed that the drug increased saccadic eye movements and early rapid eye movement (REM) dream phases when administered during sleep or shortly before sleep onset (Green 1969; Torda 1968; Muzio et al. 1966). Patients undergoing LSD-/psilocybin-assisted psychotherapy (Leuner 1981; Chandler and Hartman 1960) and healthy subjects that were administered LSD or psilocybin in an experimental setting (Carhart-Harris et al. 2016; Schmid et al. 2015; Studerus et al. 2011; Abramson et al. 1955) rated the overall quality of the psychedelic-induced subjective experience as a dreamlike state that included the experience of facilitated access to memories of the past and fantasies about the future. Neuroimaging studies showed that, in psychedelic states (Lebedev et al. 2015; Tagliazucchi et al. 2014; Carhart-Harris and Nutt 2014) and REM dreams (Solms 2000; Braun 1997; Maquet et al. 1996), and following direct electrical stimulation of the temporal lobe (Mégevand et al. 2014; Halgren et al. 1978), dreamlike experiences, such as visual hallucinations and psychotic-like alterations in the sense of self, correlated with increases in neuronal activation of temporal lobe regions. However, the highly variable phenomenological content of psychedelic imagery has so far undermined endeavours to show a stringent link between the psychedelic-induced state of consciousness and dreaming.
Dreaming is defined as mental activity characterised by vivid, predominantly visual, imagery that follows a narrative structure and occurs during sleep (Nir and Tononi 2010). Extensive studies on the basic phenomenological structure of dreaming showed that cognitive bizarreness is a common feature of the formal organisation of dream mentation and can be operationalised and validly assessed as an index of dream state (Hobson 2009). Cognitive bizarreness is the strange, irrational and fanciful quality of REM sleep dream mentation, which is characterised by the presence of improbable or impossible imaginary events, characters, objects, thoughts or feelings (Hobson 2009). The principal aim of this study was to use cognitive bizarreness as a measure of dreamlike imagery to test the hypothesis that LSD produces dreamlike waking imagery. Moreover, given that both LSD and dreaming induce changes in a range of subjective experiences, including perception, mood, cognition and sense of self, we further aimed to assess the relation between the effects of LSD on each of these domains and on cognitive bizarreness.
There is evidence that hallucinatory effects of psychedelics are mediated by serotonin 2A (5-HT2A) receptor stimulation in the brain (Nichols 2004; Vollenweider et al. 1998). However, LSD has high affinity and agonist activity at 5-HT2A/C, 5-HT1A/B, 5-HT6, 5-HT7 and dopamine D2 and D1 receptors (de Gregorio et al. 2016; Halberstadt and Geyer 2011; Passie et al. 2008; Marona-Lewicka and Nichols 2007; Thisted and Nichols 2005; Nichols 2004; Giacomelli et al. 1998), and no previous study has investigated the specific receptor contributions to the cognitive effects of LSD in humans. Therefore, a third aim of this study was to investigate whether stimulation of the 5-HT2A receptor mediates the effects of LSD on cognitive bizarreness. To this end, we combined pharmacological manipulation (LSD) and the selective 5-HT2A receptor antagonist ketanserin (Leysen et al. 1982). Pre-treatment with ketanserin reverses symptoms induced by the LSD-like psychedelic psilocybin in healthy subjects (Kometer et al. 2013; Quednow et al. 2012; Vollenweider et al. 1998). Using a double-blind, within-subjects study design, we systematically compared the post-peak effects of LSD, placebo and LSD after pre-treatment with ketanserin on cognitive bizarreness during a guided mental imagery task and in relation to the effects on subjective experience.
Method
Participants
Twenty-five healthy subjects were recruited through an advertisement placed on the web platform of the University of Zurich. The Mini-International Neuropsychiatric Interview (Sheehan et al. 1998), the DSM-IV self-rating questionnaire for Axis II personality disorders (Wittchen and Fydrich 1997) and the Hopkins Symptom Checklist (Franke and Derogatis 1995) were used to exclude individuals with present or previous psychiatric disorders or a history of major psychiatric disorders in first-degree relatives. Verbal intelligence quotient was assessed using the multiple-choice vocabulary intelligence test (MWT-B) (Merz et al. 1975). Subjects were healthy according to medical history, physical examination, routine blood analysis, electrocardiography and urine tests for drug use and pregnancy. Demographic characteristics of the study sample and lifetime use of illicit drugs are shown in Tables 1 and 2, respectively. Of the 25 subjects, 9 (36%) reported prior experience with classic psychedelics. Cannabis had the highest prevalence of lifetime drug use, and the prevalence in our study sample (76%) was higher than the lifetime prevalence in a comparable population of Swiss students (59%) (Dammann et al. 2014). Subjects were required to abstain from the use of any prescription or illicit drug for a minimum of 2 weeks prior to the first test day and for the duration of the entire study and to abstain from drinking alcohol for at least 24 h prior to each test day. Six subjects were light cigarette smokers (<5 cigarettes/day) and were told to maintain their usual smoking habits but not to smoke cigarettes during the sessions. Urine tests and self-report questionnaires were used to verify the absence of drug and alcohol use and pregnancy on the screening visit and each experimental visit before drug administration. Urine tests of all subjects included in the study were negative. No alcohol test was performed.
Study design
Subjects participated in a double-blind, placebo-controlled, within-subjects, crossover design that involved three experimental sessions performed in a balanced order. The between-session interval was at least 2 weeks. The test sessions began at 7:45 AM. At 8:00 AM, subjects received pre-treatment and at 9:00 AM they received treatment. The pre-treatment/treatment combinations were as follows: placebo (179 mg of mannitol and 1 mg of aerosil orally) + LSD (100 mcg orally), ketanserin (40 mg orally) + LSD (100 mcg orally) and placebo + placebo. These are referred to as LSD, Ket+LSD and Pla conditions, respectively.
Plasma concentration of LSD peaks 1.5 h (range, 0.5–4 h) after administration and has a half-life of 3.6 h, slower elimination after 12 h and a terminal half-life of 8.9 h (Dolder et al. 2015). After a single oral dose of 40 mg ketanserin, plasma concentration peaks after 1.1 h and has a relatively long elimination half-life of 29.2 h (Persson et al. 1987). The time delay between pre-treatment and treatment was 1 h, to ensure maximal 5-HT2A receptor occupancy (Ettrup et al. 2014). A single 40-mg dose of ketanserin taken orally represents a regular therapeutic dose and completely blocks 5-HT2A receptor-induced alterations in states of consciousness of healthy subjects (Kometer et al. 2013; Quednow et al. 2012; Vollenweider et al. 1998).
A standardised lunch was served at 1:00 PM. The mental imagery task was performed at 4:00 PM, 7 h after drug treatment. This is during the descending phase of the acute effects of LSD (Dolder et al. 2015). This had the disadvantage that the effects of LSD were not evaluated during drug peak but had the advantage that subjects could engage in a verbal dialogue, which was a requirement for the imagery task and which would have been very difficult during drug peak, where people often show reduced vigilance, impoverished speech and reluctance to engage in verbal communication despite having intense inner experiences (Johnson et al. 2008). The current study was a small part of a larger neuroimaging study (Preller et al. 2017), and the design of the larger study dictated that the mental imagery task be performed at 4:00 PM.
A standardised dinner was served at 6:00 PM. At approximately 9:00 PM, about 12 h after treatment and therefore after the acute effects of LSD had subsided (Dolder et al. 2015), subjects were discharged into the custody of a family member or close friend.
All subjects provided written informed consent prior to their inclusion in the study and were paid for their participation. The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and International Conference on Harmonization Guidelines in Good Clinical Practice and was approved by the Ethics Committee of the Canton of Zurich, Switzerland and the Swiss Agency for Therapeutic Products (Swissmedic). The administration of LSD to healthy subjects was authorised by the Swiss Federal Office for Public Health, Bern, Switzerland.
Study drugs
Gelatine capsules that contained 100 mcg of LSD (d-LSD hydrate; Lipomed AG, Arlesheim, Switzerland) with a high purity (>99%, high-performance liquid chromatography) (Dolder et al. 2015) and identical capsules that contained ketanserin (40 mg of Sufrexal®; Janssen-Cilag, Zug, Switzerland) or placebo (179 mg of mannitol and 1 mg of aerosil; Hospital Pharmacy, Canton Hospital, Lucerne, Switzerland) were administered in single oral doses.
Guided mental imagery task
The guided mental imagery task followed the standardised guided affective imagery procedure, a systematic imagery method for analytically oriented psychotherapy described by Leuner (1969). The task was performed in a quiet, slightly dimmed room. Subjects lay on a couch in a comfortable position with their eyes closed and were instructed to focus their attention on their inner experience. After a brief instruction to relax, subjects were asked to imagine a motif (scene), for example, a meadow, any meadow that came to their mind. No further instructions were given; everything was left as open and as unstructured as possible so that the subjects could develop their own images and actions, projected onto the initial motif.
Throughout the task, the guide remained in a loose form of dialogue with the subjects to keep himself informed of the development of the subjects’ imagery and enabling him to slow down the process and have the subjects delve more deeply into their imagery experience.Footnote 1 To minimise the influence of the guide on the descriptions given by the subjects, open-ended, standardised questions were asked throughout. Present tense was used to focus the imagery experience on the here-and-now. Questions were only used to keep the imagery process going and to explore the imaginary world with all senses (e.g. “What are you doing?”, “What do you see/hear/smell/taste/feel?”, “Is there anything you are tempted to do right now?”, “How do you feel now?”, “Please describe”). Whenever possible, explicit verbal input from the guide was kept to a minimum and replaced by confirming fillers (e.g. “mhm”) or encouraging words (“keep going”). During the imagery task, no interpretations or comments on the imagery content were given. The guide was trained by the Swiss Association for Guided Affective Imagery, Berne (www.sagkb.ch).
The motif used to begin the imagery task was a meadow in session 1, a creek in session 2 and a house in session 3. These were selected from the five basic motifs recommended by Leuner (1969) for imagery novices.
The guided mental imagery task lasted 30 min. Verbal imagery reports from the subjects were audiorecorded and later transcribed, yielding a total data set of 75 imagery reports. Most study subjects were naïve to mental imagery, and all subjects were familiarised with the task beforehand in a separate pre-investigation visit using a flower as the motif. All subjects could spontaneously engage in mental imagery.
Outcome measures
State of consciousness
Subjective state of consciousness was evaluated using the five-dimensional Altered State of Consciousness (5D-ASC) questionnaire (Dittrich 1996). The 5D-ASC uses a visual analogue scale (VAS) to evaluate aetiology-independent alterations in consciousness, including changes in perception, mood, cognition and experience of self and environment. Subjective state of consciousness was quantified using five lower-order scales: elementary imagery (visual hallucinations of regular patterns, colours or light flashes), complex imagery (visual hallucinations of scenes and pictures), euphoric mood (positive affect and mania-like experiences), loss of self-boundaries and cognitive control (alterations in the experience of the self and body such as diminished subject-object and inner-outer dualities and impaired control of thinking and volition) and changed meaning of percepts (increased attribution of personal meaning to environmental stimuli).
Subjects completed a 45-item short version of the 5D-ASC at several time points (T1 = 180 min, T2 = 270 min and T3 = 390 min after drug treatment). At T4 (720 min after drug treatment), after acute drug effects had receded, participants completed the 94-item full version of the 5D-ASC and were instructed to retrospectively rate the overall peak of their subjective experiences across the session. The mental imagery task was performed close to T3, at 420 min after drug treatment; therefore, the 5D-ASC short version completed at T3 was used to quantify subjective state of consciousness. The 5D-ASC full version completed at T4 was not used as this retrospectively measured the state of consciousness during the drug peak, and the mental imagery task was performed during the descending phase of the subjective LSD effects (Dolder et al. 2015).
Intensity of drug effects
The intensity of drug effects was evaluated using the global 5D-ASC (G-ASC) score. This is the average score of all 45 items in the short version of the 5D-ASC. The G-ASC for the full version of the 5D-ASC was calculated as the average score of the 45 items that appear in the short version. The G-ASC score at time points T1, T2, T3 and T4 was used to indicate the time course of drug effects across the session. The G-ASC score at time point T3 was used to indicate the intensity of drug effects at the time of the mental imagery task. In the LSD condition, the G-ASC score at time point T3 was also expressed as a percentage of the 5D-ASC score at time point T4, to indicate the intensity of LSD effects at the time of the mental imagery task relative to the retrospectively rated peak drug effects.
Mental imagery experience
After completion of the mental imagery task, subjects retrospectively rated their mental imagery experience on VASs for visual vividness, emotional arousal, positive emotions, negative emotions, insight and relaxation. Each VAS was presented as a 100-mm horizontal line marked with “not at all” on the left and “extremely” on the right.
Cognitive bizarreness of mental imagery reports
Cognitive bizarreness of mental imagery reports was evaluated using an adapted version of Hobson’s two-stage scoring system for measuring cognitive bizarreness (Hobson 2009). This is a reliable and validated set of criteria that was used in previous studies of REM dream reports (Scarone et al. 2008; Williams et al. 1992). The scoring system is described in Table 3. Each identified bizarre item was assigned a single main category (plot, cognition or feeling state) and a combination of subcategories (e.g. discontinuity and incongruity). For plot and cognition, the uncertainty subcategory (A3 and B3, respectively) was combined into a single subcategory (A3/B3) because judges could not determine from the transcribed imagery reports whether the uncertainty arose as the subject reported his or her experience or was an inherent property of an imagined scenario.
Imagery reports were scored by two external judges who were blind to drug condition. The judges independently scored the same 15 imagery reports (three reports per subject from a random sample of five subjects). Inter-rater reliability was quantified using intra-class correlation coefficient and was 0.95. Each judge then randomly selected one-half of the remaining 60 imagery reports and independently scored these 30 imagery reports.
For each subject and each drug condition, bizarreness density (BD) was quantified for each category (plot, cognition and feeling state) and subcategory, respectively, by dividing the number of bizarre items in the report in that category and subcategory, respectively, by the word count of the report. This was carried out to correct for differences in length of reports. Total BD was calculated by dividing the total number of bizarre items in the report (i.e. number of bizarre items in all categories) by the word count of the report. The mean (SD) number of words in the reports was 4353 (793), 3979 (851) and 4112 (893) for LSD, Ket + LSD and Pla conditions, respectively.
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics 23 software (IBM, Chicago, IL, USA).
State of consciousness
The 45-item 5D-ASC score at time point T3 was analysed using a repeated-measures analysis of variance (ANOVA) with drug (LSD, Ket + LSD and Pla) and scale (elementary imagery, complex imagery, euphoric mood, loss of self-boundaries and cognitive control and changed meaning of percepts) as the within-subjects factors. Significant main effects or interactions in the ANOVA were followed by Bonferroni-corrected post hoc pairwise comparisons with a significance level of p < 0.05 (two-tailed test).
Intensity of drug effects
The G-ASC score was analysed using a repeated-measures ANOVA with drug (LSD, Ket + LSD and Pla) and time point (T1, T2, T3 and T4) as the within-subjects factors.
Mental imagery experience
VAS scores for mental imagery experience were analysed using a repeated-measures ANOVA with drug (LSD, Ket + LSD and Pla) and scale (visual vividness, emotional arousal, positive emotions, negative emotions, insight and relaxation) as the within-subjects factors.
Cognitive bizarreness of mental imagery reports
BD was analysed using a repeated-measures ANOVA with drug (LSD, Ket + LSD and Pla) and bizarreness category (plot, cognition and feeling state) as the within-subjects factors, and a separate repeated-measures ANOVA with drug (LSD, Ket + LSD and Pla) and bizarreness subcategory (plot discontinuity, plot incongruity, plot/cognition uncertainty, cognition discontinuity, cognition incongruity, feeling state discontinuity, feeling state incongruity and feeling state uncertainty) as the within-subjects factors.
Relations between cognitive bizarreness, state of consciousness and mental imagery experience
The LSD-induced change in cognitive bizarreness, state of consciousness and mental imagery experience was quantified using the change in total BD, 5D-ASC scale scores and mental imagery experience VAS scores between the LSD and Pla drug conditions (ΔBD, Δ5D-ASC and ΔVAS, respectively). Pearson multiple correlation was used to quantify the relations between these variables.
A multiple linear regression analysis with removal with ΔBD as the dependent variable and Δ5D-ASC as predictor variables was used to further examine whether the LSD-induced change in total BD was associated with the LSD-induced change in state of consciousness. Collinearity tests, residual tests and diagnostic plots were used to detect outliers and to ascertain that regression modelling assumptions were met.
Results
State of consciousness
At the time of the mental imagery task, LSD still produced marked alterations in state of consciousness, as indicated by a significant main effect of drug (F(1.00, 24.03) = 27.86, p < 0.001, partial η 2 = 0.54) in a repeated-measures (drug × scale) ANOVA on 5D-ASC score at T3. There was also a significant main effect of scale (F(4.00, 63.70) = 8.40, p < 0.001, partial η 2 = 0.26) and a significant drug × scale interaction (F(8.00, 68.44) = 7.54, p < 0.001, partial η 2 = 0.24). Bonferroni-corrected post hoc pairwise comparisons revealed a greater score on all five 5D-ASC scales in the LSD condition than in the Pla and Ket + LSD conditions (all p < 0.05). Scores did not differ between the Pla and Ket + LSD conditions for any 5D-ASC scale (all p = n.s.), indicating that ketanserin pre-treatment completely blocked all LSD-induced effects (Fig. 1a).

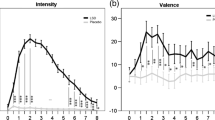
Subjective state of consciousness and mental imagery experience. a State of consciousness at the time of the mental imagery task. The graph shows the score on each 5D-ASC scale at time point T3 in each drug condition. LSD increased the score on all five 5D-ASC scales. Ketanserin pre-treatment completely blocked all LSD-induced effects (all p = n.s.). b Intensity of drug effects across the experimental session. The graph shows G-ASC score at each time point in each drug condition. At T1-T3, G-ASC score represents the intensity of drug effects at those time points, whereas, at T4, the 5D-ASC was retrospectively rated and G-ASC score represents the drug peak effects. T3 was immediately prior to the mental imagery task. LSD increased the G-ASC at all time points, and G-ASC showed a typical nonlinear decline over time, as previously shown (Dolder et al. 2015; Schmid et al. 2015; Passie et al. 2008). Ketanserin pre-treatment completely blocked all LSD-induced effects (all p = n.s.). c Mental imagery experience. The graph shows the VAS score for each aspect of mental imagery experience in each drug condition. LSD increased VAS score for visual vividness and emotional arousal. Ketanserin pre-treatment completely blocked all LSD-induced effects (all p = n.s.). Data are expressed as mean plus standard error in N = 25 subjects. Asterisks indicate significant differences between LSD and placebo conditions (*p < 0.05; **p < 0.001, Bonferroni-corrected). 5D-ASC, Altered States of Consciousness; G-ASC, global 5D-ASC; VAS, visual analogue scale; Pla, placebo; Ket, ketanserin; LSD, lysergic acid diethylamide; T1 = 180 min, T2 = 270 min, T3 = 390 min, T4 = 720 min after drug treatment
Intensity of drug effects
Effects of LSD were apparent at each time point during the session, as indicated by a significant main effect of drug (F(1.00, 24.12) = 61.52, p < 0.001, partial η 2 = 0.72), in a repeated-measures (drug × time) ANOVA of G-ASC score. There was also a significant main effect of time (F(1.93, 46.39) = 34.80, p < 0.001, partial η 2 = 0.59) and a significant drug × time interaction (F(2.07, 49.56) = 27.59, p < 0.001, partial η 2 = 0.54). Bonferroni-corrected post hoc pairwise comparisons revealed greater G-ASC score at all four time points in the LSD condition than in the Pla and Ket + LSD conditions (all p < 0.001). G-ASC score did not differ between the Pla and Ket + LSD conditions for any 5D-ASC scale (all p = n.s.), indicating that ketanserin pre-treatment completely blocked all LSD-induced effects (Fig. 1b).
In the LSD condition, the mean (SD) G-ASC score at the time of the mental imagery task and during drug peak was 23.78% (24.25) and 37.95% (21.89), respectively. At the time of the mental imagery task, the relative intensity of LSD effects was 62.6% of the peak.
Mental imagery experience
LSD significantly modulated subjective mental imagery experience, as indicated by a significant main effect of drug (F(2, 48) = 8.57, p < 0.001, partial η 2 = 0.26), in a repeated-measures (drug × scale) ANOVA of the retrospectively administered VAS for mental imagery experience. The ANOVA further revealed a significant main effect of scale (F(2.86, 68.71) = 55.23, p < 0.001, partial η 2 = 0.70) and a significant drug × scale interaction (F(5.58, 133.86) = 3.21, p = 0.007, partial η 2 = 0.12). Bonferroni-corrected post hoc pairwise comparisons revealed greater VAS score on the vividness and arousal scales in the LSD condition than in the Pla condition and on the vividness scale in the LSD condition than in the Ket + LSD condition (all p < 0.05). VAS score did not differ between the Pla and Ket + LSD conditions for any VAS scale (all p = n.s.), indicating that ketanserin pre-treatment completely blocked all LSD-induced effects (Fig. 1c).
Cognitive bizarreness of mental imagery reports
LSD significantly increased cognitive bizarreness of mental imagery reports, as indicated by a significant main effect of drug (F(1.070, 25.60) = 33.57, p < 0.001, partial η 2 = 0.58), in a repeated-measures (drug × category) ANOVA of BD. Bonferroni-corrected post hoc comparisons on this main effect revealed significantly greater BD in the LSD condition than in the Pla and Ket + LSD conditions (all p < 0.001). BD did not differ between the Pla and Ket + LSD conditions (all p = n.s.), indicating that ketanserin pre-treatment completely blocked the effect of LSD (Fig. 2a). The ANOVA further revealed a significant main effect of category (F(1.15, 27.65) = 24.31, p < 0.001, partial η 2 = 0.50) and a significant interaction of drug × category (F(1.24, 29.71) = 223.14, p < 0.001, partial η 2 = 0.41). Bonferroni-corrected post hoc pairwise comparisons on this interaction revealed greater BD for two of the three categories in the LSD condition than in the Pla and Ket + LSD conditions (all p < 0.05). BD for the feeling state category did not differ across drug conditions (all p = n.s.). BD did not differ between the Pla and Ket + LSD conditions for any category (all p = n.s.), indicating that ketanserin pre-treatment completely blocked all LSD-induced effects (Fig. 2a).

Bizarreness density (BD) of guided mental imagery reports. a Total BD and BD in each main category. The graph shows total BD and BD in each main category in each drug condition. LSD increased BD for the plot and cognition categories (both p < 0.001) but not BD for the feeling state category (p = n.s.). Ketanserin pre-treatment completely blocked all LSD-induced effects (all p = n.s.). b BD in each subcategory. The graph shows BD in each subcategory in each drug condition. LSD increased BD for plot discontinuity, plot incongruity, plot/cognition uncertainty and cognition incongruity subcategories (all p < 0.05). Ketanserin pre-treatment completely blocked all LSD-induced effects (all p = n.s.). Data are expressed as mean plus standard error in N = 25 subjects. Asterisks indicate significant differences between LSD and placebo conditions (*p < 0.05; **p < 0.001, Bonferroni-corrected). A1, plot discontinuity; A2, plot incongruity; A3/B3, plot/cognition uncertainty; B1, cognition discontinuity; B2, cognition incongruity; C1, feeling state discontinuity; C2, feeling state incongruity; C3, feeling state uncertainty; Pla, placebo; Ket, ketanserin; LSD, lysergic acid diethylamide
A separate repeated-measures (drug × subcategory) ANOVA of BD revealed a significant main effect of drug (F(1.06, 25.46) = 37.00, p < 0.001, partial η 2 = 0.61). The ANOVA further revealed a significant main effect of subcategory (F(1.74, 41.67) = 19.19, p < 0.001, partial η 2 = 0.44) and a significant drug × subcategory interaction (F(2.14, 51.31) = 18.87, p < 0.001, partial η 2 = 0.44). Bonferroni-corrected post hoc pairwise comparisons revealed greater BD on four of the eight subcategories in the LSD condition than in the Pla and Ket + LSD conditions (all p < 0.05). BD did not differ between the Pla and Ket + LSD conditions for any subcategory (all p = n.s.), indicating that ketanserin pre-treatment completely blocked all LSD-induced effects (Fig. 2b).
Relations between cognitive bizarreness, state of consciousness and mental imagery experience
There was a significant positive correlation between LSD-induced increase in total BD and LSD-induced increase in 5D-ASC score for the loss of self-boundaries and cognitive control scale (r = 0.44, N = 25, p < 0.05, uncorrected) (Table 4 and Fig. 3). There was also a trend-level correlation between LSD-induced increase in total BD and LSD-induced increase in 5D-ASC score for the euphoric mood scale (p = 0.05, uncorrected) and emotional arousal VAS score (p = 0.08, uncorrected). A multiple linear regression analysis was used to develop a model to predict LSD-induced increase in total BD from LSD-induced increase in 5D-ASC scale scores. The loss of self-boundaries and cognitive control 5D-ASC scale was the only predictor that had a significant (p < 0.05) partial effect in the full model. The model accounted for 19% of the variance in LSD-induced increase in total BD (F(1, 23) = 5.50, p = 0.03, adjusted R 2 = 0.19).

Change in loss of self-boundaries and cognitive control was related to change in cognitive bizarreness of guided mental imagery reports. The scatter plot shows the relation between the LSD-induced increase in score on the loss of self-boundaries and cognitive control scale of the 5D-ASC (difference between LSD and placebo drug conditions, x-axis) and the LSD-induced increase in total bizarreness density (BD) of mental imagery reports (difference between LSD and placebo drug conditions, y-axis) (r = 0.44, N = 25, p < 0.05, uncorrected)
Discussion
In this psychopharmacological study, we provide quantitative evidence that LSD produces dreamlike imagery in healthy humans when awake. Specifically, we conclusively show that LSD, in comparison with placebo, increased cognitive bizarreness, a formal measure of REM dream mentation (Hobson 2009) (Fig. 2). Furthermore, we show that the dreamlike effect of LSD was mediated by brain 5-HT2A receptor stimulation (Fig. 2) and was related to LSD-induced subjective loss of self-boundaries and cognitive control (Fig. 3 and Table 4). The findings of this study confirm the long-held view that psychedelics induce dreamlike states of consciousness (Schmid et al. 2015; Carhart-Harris and Nutt 2014; Tagliazucchi et al. 2014; Studerus et al. 2011; Hobson 2001; Fischman 1983; Jacobs 1978) and provide a deeper understanding of the link between the psychedelic state of consciousness and dreaming.
Cognitive bizarreness and sense of self
Several effects of LSD could increase cognitive bizarreness. One is LSD-induced disturbance of the basic sense of self, also known as depersonalisation. Similar to what happens during dreaming (Kahn 2013), this alters fundamental structures of consciousness, i.e. mental framework and perspectives on space, time, causality and selfhood. Our results show that the LSD-induced increase in the cognitive bizarreness of mental imagery reports was related to the LSD-induced loss of self-boundaries and cognitive control (Fig. 3 and Table 4). This finding is in accordance with a recent functional magnetic resonance imaging study (Preller et al. 2017) that used a music paradigm to investigate the effects of LSD on the processing of personal meaning. Preller et al. reported that LSD increased behavioural measures of meaning attribution as well as activity in cortical midline regions and the ventrolateral prefrontal cortex in response to previously meaningless music stimuli. They concluded that LSD alters meaning attribution by increasing the activity of brain areas that are typically involved in self-processing.
Our finding is also in line with studies that used the LSD-like 5-HT2A/1A receptor agonist psilocybin and showed that psilocybin-induced cognitive symptoms such as disorganised thinking were secondary to psilocybin-induced self-disturbance (Vollenweider and Geyer 2001; Vollenweider et al. 1997). A recent study (Lebedev et al. 2015) found that individual variability of psilocybin-induced psychedelic symptoms was best explained by a common factor that included vivid dreamlike imagery, loss of self-boundaries and fear of losing control over thought processes. Moreover, there is evidence that bizarreness in REM dreams of normal subjects (Fosse et al. 2004) and in waking thoughts and dreams of schizophrenic patients (Rasmussen and Parnas 2015; Sass and Byrom 2015; Scarone et al. 2008; Limosani et al. 2011) is closely related to disturbed sense of self, and there is qualitative evidence that many bizarre features of both psychedelic imagery and dreams can be traced back to loss of self-boundaries and cognitive control (Pines 1976; Leuner 1968; Savage 1955; Abramson et al. 1955). For example, one subject in the present study described loss of self-boundaries and cognitive control and how closely this was related to bizarre imagery in the LSD condition as follows: “I merged with the environment. I became one with all. It made me float around, and I no longer had a will to decide where I should go next. I felt that everything was happening without my volition. At one moment, everything wound around me, like a plant. And then I went into the core of the plant, and suddenly, I somehow emerged within an air bubble that was spat out of a volcano. I was me, but somehow also not me. And then, I was flowing down the volcano as a lava stream”.
Cognitive bizarreness and basic visual processing
A second effect of LSD that could increase cognitive bizarreness is changes in basic visual processes. This is supported by a recent neuroimaging study (Carhart-Harris et al. 2016), which showed that LSD-induced simple and complex hallucinations were closely related to LSD-induced activation of the primary visual cortex. This is further supported by mathematical modelling (Bressloff et al. 2002; Ermentrout and Cowan 1979) and behavioural (Baggott et al. 2010) and neuroimaging (Roseman et al. 2016; de Araujo et al. 2012) studies showing that psychedelic-induced excitation of the primary visual cortex may facilitate spontaneous formation of retinotopically organised geometric hallucinations, which in turn could progress to more complex scenic hallucinations by spreading up the visual hierarchy.
However, our results clearly support the conclusion of other authors (Family et al. 2016; Fischer and Landon 1972; Weintraub et al. 1959; Savage 1955) that it is not the interaction of LSD with basic visual processing but rather LSD-induced higher-level alterations of self and cognition that increase cognitive bizarreness. First, the LSD-induced increase in cognitive bizarreness was not related to a change in the elementary and complex imagery scale of the 5D-ASC, nor to VAS score of the visual vividness of mental imagery (Table 4). Second, the effects of LSD on cognitive bizarreness were not evenly distributed across the bizarreness subcategories (Fig. 2), as would be expected from a purely bottom-up account of cognitive bizarreness based on random visual noise. Rather, they were loaded heavily on the plot category and much less on the cognition and feeling state categories. This indicates that, despite unrealistic content in terms of plot, character, objects or actions, mental imagery reports in the LSD condition still contained a narrative structure and a relatively coherent unfolding of imaginary events over time. This narrative-thematic constancy is also characteristic of dreaming, where it is known as single mindedness (Rechtschaffen 1978). During LSD imagery, for example, one study subject saw a mouldered shipwreck on the seashore. He unlocked and entered a dungeon inside the ship’s hull. There, he found the bones of a dead pirate, scattered on the wooden floor. Next to the pirate, there was a bottle of rum, gold and jewellery. The subject then realised, for the first time and with a certain degree of emotional involvement, that he had been pursuing ambitious life goals such as career-building and money-making but with consequences of social neglect and chronic feelings of loneliness.
Cognitive bizarreness and creative thinking
A third effect of LSD that could increase cognitive bizarreness is an increase in creative or divergent, nonlinear thinking, which is defined as a thought process where many responses to a single question or problem are generated and where the responses are often novel or lead to a broader perspective than in normal thought (Guilford 1967). Although we did not directly investigate the effects of LSD on creative thinking, during the LSD condition, subjects consistently reported that they experienced their imagery as “very dynamic, rapidly changing, fugitive, enormously varied”, “less inhibited by logical constraints and necessity to make sense” and “spontaneously, effortlessly, evolving more naturally”. Importantly, many subjects retrospectively reported that imaginary objects and scenes were like a condensation and recombination of multiple memory fragments, allowing them to see things under novel perspectives and relations. This latter notion is supported by the result that discontinuous, incongruent imaginary content in terms of plot, character, objects or actions accounted for the largest component of cognitive bizarreness during LSD (Fig. 2). Furthermore, this is supported by a growing body of literature (Sweat et al. 2016; Baggott 2015; Sessa 2008; Leuner 1973) indicating that psychedelics induce a state of broadened consciousness that is associated with a different cognitive style, including facilitated access to remote semantic associations (Family et al. 2016; Spitzer et al. 1996; Rittenhouse et al. 1994); cross-modal fusion between sensory modalities (synaesthesia), perception and feeling (physiognomic perception) and imagery and perception (eidetic imagery) (Terhune et al. 2016; Sinke et al. 2012; Glicksohn 1992); thinking in metaphors and symbols (Lakoff 1993; Martindale and Fischer 1977; Landon and Fischer 1970); enhanced problem-solving capabilities (Sio et al. 2013; Frecska et al. 2012; Wagner et al. 2004); and increased topographically long-range neuronal connectivity in the brain (Achermann et al. 2016; Petri et al. 2014; Massimini et al. 2010). Taken together, these findings suggest that creative thinking may be an important mechanism behind cognitive bizarreness, where there is increased binding of logically incompatible, but associatively remotely connected, features into new phenomenological Gestalts (Rittenhouse et al. 1994). This hypothesis should be tested in future studies by concurrently assessing LSD-induced changes in cognitive bizarreness and measures of creative thinking in the same subjects.
Cognitive bizarreness and the 5-HT2A receptor
LSD-induced effects on cognitive bizarreness could be related to several LSD-induced effects, including loss of self-boundaries and cognitive control, and enhancement of creative thinking. However, our results showed that all LSD-induced effects, including effects on subjective reports of state of consciousness (5D-ASC score) and mental imagery experience (VAS scores; Fig. 1) and on the cognitive bizarreness of mental imagery (Fig. 2), were fully blocked by the 5-HT2A receptor antagonist ketanserin. This shows that stimulation of the 5-HT2A receptor is a key mechanism of action mediating both the LSD-induced changes in subjective experience and the dreamlike effects of LSD.
This finding is in line with previous animal (Halberstadt and Geyer 2010; González-Maeso et al. 2007) and human (Valle et al. 2016; Kometer et al. 2013; Quednow et al. 2012; Carter et al. 2005) studies showing that psychedelic effects can be reversed by 5-HT2A inverse agonists or antagonists and that 5-HT2A receptor antagonism is key to the antipsychotic properties of multi-receptor acting atypical antipsychotic drugs such as clozapine (Meltzer et al. 2009; Meltzer et al. 2003). This finding is also in line with previous human studies that highlighted the importance of 5-HT receptor involvement in the generation of complex visual hallucinations in Parkinson’s disease (Ballanger et al. 2010) and in the sporadic dream-enhancing effects of selective serotonin reuptake inhibitors (Pace-Schott 2008; Pace-Schott et al. 2001).
However, the current result that dreamlike effects of LSD were blocked by ketanserin is somewhat surprising given that LSD also stimulates dopamine D2 and D1 receptors (de Gregorio et al. 2016; Halberstadt and Geyer 2011; Passie et al. 2008; Marona-Lewicka and Nichols 2007; Thisted and Nichols 2005; Nichols 2004; Giacomelli et al. 1998), that activation of dopamine receptors in mesolimbic and mesocortical systems is a crucial receptor mechanism in the generation of dream imagery (Solms 2000) and the visual hallucinations of schizophrenic patients (Gottesmann 2006) and that dopaminergic agonists such as levodopa can induce vivid dreaming (Thompson and Pierce 1999). Furthermore, animal studies (Halberstadt 2015; Celada et al. 2004; Amargós-Bosch et al. 2004; Krebs-Thomson and Geyer 1998; Schreiber et al. 1995; Araneda and Andrade 1991) suggest that 5-HT1A receptor stimulation produces the opposite behaviours to the 5-HT2A receptor-mediated behaviours induced by psychedelics. In humans, the non-hallucinogenic and selective 5-HT1A receptor agonist buspirone reduced psilocybin-induced simple and complex hallucinations (Pokorny et al. 2016), and pre-treatment with the 5-HT1A antagonist pindolol enhanced the psychedelic effects of N,N-dimethyltryptamine (Strassman 1995). Moreover, 5-HT1A receptor stimulation may suppress REM sleep (Driver et al. 1995; Gillin et al. 1994).
Therefore, although the present results strongly indicate that the subjective and dreamlike effects of LSD are predominantly mediated by 5-HT2A receptor stimulation, future studies should specifically assess the differential contributions of D2/D1 and 5-HT1A receptors, e.g. by using selective receptor antagonists such as haloperidol (Vollenweider et al. 1998) or pindolol (Nichols 2004) or by using non-hallucinogenic 5-HT2A receptor agonists such as lisuride (González-Maeso et al. 2007) or 2,5-dimethoxy-4-ethylamphetamine (DOET) (Snyder et al. 1969). Investigating the effects of the non-hallucinogenic 5-HT2A receptor agonist DOET on cognitive bizarreness would be a particularly intriguing approach because, in human studies, DOET did not produce visual hallucinations but increased associative thinking and induced an altered sense of self (Snyder et al. 1971; Weingartner et al. 1970).
Limitations
Most of the study subjects were naïve to LSD. This might have impaired their ability to exercise cognitive control over the imagery experience in the LSD condition. In future studies, it might be interesting to assess individual predisposition to navigate through psychedelic imagery or to increase these cognitive capabilities via, for example, mindfulness training (Stumbrys et al. 2015). A further limitation is that the effects of LSD on imagery could have been due, at least partially, to changes in language production (Family et al. 2016) or attention (Passie et al. 2008), which would have influenced directly the narrative description of imagery content rather than imagery mentation itself. Although the effects of LSD on imagery were not evenly distributed across the bizarreness subcategories—as would be expected from general effects on language production or attention—we cannot rule out this potential confound completely. Therefore, it would be informative to include a control task (such as a description of a video) in future studies to differentiate between narrative descriptions of mental imagery and narrative descriptions of visual imagery in relation to cognitive bizarreness. Finally, animal studies (Marona-Lewicka and Nichols 2007; Thisted and Nichols 2005) have shown that the behavioural effects of LSD occur in two temporal phases, with later effects being substantially mediated by D2 receptor stimulation. Therefore, the lateness of the imagery task is a further limitation, because we cannot assume that late effects are merely a lesser version of early effects.
Potential clinical implications
Although psychedelic-induced visual hallucinations have been related to broadband decreases in electrophysiological oscillations, there are reports that oscillations in the gamma range are intact or even slightly increased during psychedelic states (Kometer et al. 2015; Muthukumaraswamy et al. 2013). Given that gamma range oscillations have been related to dream cognition (Llinás and Ribary 1993) and enhanced dream lucidity (Voss et al. 2014), which is the awareness during dreaming that one is dreaming and the capacity to wilfully influence some aspects of the dream actions, one might speculate that psychedelic dream states differ from normal night dreams in the degree of lucidity and gamma range oscillatory activity in frontotemporal regions of the brain. In fact, unlike during sleep, psychedelic states are not characterised by drowsiness and loss of awareness but rather by an enhanced clarity and richness of consciousness (Leuner 1981). One might even speculate that the psychedelic-specific combination of lucid consciousness with loss of self-boundaries and cognitive control might relax rigid thinking and let previously unrecognised, self-relevant images rise into consciousness (LaBerge and Rheingold 1991). This might be an important mechanism to facilitate psychological insight, a notion that is supported by early clinical studies in the 50s of the last century (Sandison and Whitelaw 1957; Frederking 1955; Savage 1955; Sandison 1954; Sandison et al. 1954; Busch and Johnson 1950), when LSD was used as an aid in psychotherapeutic treatment of chronic psychiatric conditions.
Conclusions
Using a standardised, formal measure of dreaming cognition in healthy subjects, we found that LSD produced mental imagery comparable to that reported in dreams, primarily via activation of the 5-HT2A receptor. Dreamlike effects of LSD were related to loss of self-boundaries and cognitive control but not to visual hallucinations. Future studies should further assess the contribution of specific subtypes of 5-HT and dopamine receptors to cognitive bizarreness.
Notes
As this meditative state progresses, subjects experience a “quasi-reality” with its concomitant feelings and associated affects, which was termed “catathymic imagery” by Leuner (1969).
References
Abramson HA, Jarvik ME, Kaufman MR, Kornetsky C, Levine A, Wagner M (1955) Lysergic acid diethylamide (LSD-25): I. Physiological and perceptual responses. The Journal of Psychology 39(1):3–60. doi:10.1080/00223980.1955.9916156
Achermann P, Rusterholz T, Dürr R, König T, Tarokh L (2016) Global field synchronization reveals rapid eye movement sleep as most synchronized brain state in the human EEG. Royal Society Open Science 3(10):160201. doi:10.1098/rsos.160201
Amargós-Bosch M, Bortolozzi A, Puig MV, Serrats J, Adell A, Celada P, Mengod G, Artigas F, Toth M (2004) Co-expression and in vivo interaction of serotonin 1A and serotonin 2A receptors in pyramidal neurons of prefrontal cortex. Cereb Cortex 14(3):281–299. doi:10.1093/cercor/bhg128
Araneda R, Andrade R (1991) 5-Hydroxytryptamine 2 and 5-hydroxytryptamine 1A receptors mediate opposing responses on membrane excitability in rat association cortex. Neuroscience 40(2):399–412. doi:10.1016/0306-4522(91)90128-B
de Araujo DB, Ribeiro S, Cecchi GA, Carvalho FM, Sanchez TA, Pinto JP, de Martinis BS, Crippa JA, Hallak JEC, Santos AC (2012) Seeing with the eyes shut: neural basis of enhanced imagery following ayahuasca ingestion. Hum Brain Mapp 33(11):2550–2560. doi:10.1002/hbm.21381
Baggott MJ (2015) Psychedelics and creativity: a review of the quantitative literature. PeerJ PrePrints 3:e1202v1. doi:10.7287/peerj.preprints.1202v1
Baggott MJ, Siegrist JD, Galloway GP, Robertson LC, Coyle JR, Mendelson JE (2010) Investigating the mechanisms of hallucinogen-induced visions using 3,4-methylenedioxyamphetamine (MDA): a randomized controlled trial in humans. PLoS One 5(12):e14074. doi:10.1371/journal.pone.0014074
Ballanger B, Strafella AP, van Eimeren T, Zurowski M, Rusjan PM, Houle S, Fox SH (2010) Serotonin 2A receptors and visual hallucinations in Parkinson disease. Arch Neurol 67(4):416–421. doi:10.1001/archneurol.2010.35
Braun A (1997) Regional cerebral blood flow throughout the sleep-wake cycle. An H2(15)O PET study. Brain 120(7):1173–1197. doi:10.1093/brain/120.7.1173
Bressloff PC, Cowan JD, Golubitsky M, Thomas PJ, Wiener MC (2002) What geometric visual hallucinations tell us about the visual cortex. Neural Comput 14(3):473–491. doi:10.1162/089976602317250861
Busch AK, Johnson WC (1950) LSD 25 as an aid in psychotherapy; preliminary report of a new drug. Diseases of the nervous system 11(8):241–243
Carhart-Harris R, Nutt D (2014) Was it a vision or a waking dream? Front Psychol 5:255. doi:10.3389/fpsyg.2014.00255
Carhart-Harris RL, Muthukumaraswamy S, Roseman L, Kaelen M, Droog W, Murphy K, Tagliazucchi E, Schenberg EE, Nest T, Orban C, Leech R, Williams LT, Williams TM, Bolstridge M, Sessa B, McGonigle J, Sereno MI, Nichols D, Hellyer PJ, Hobden P, Evans J, Singh KD, Wise RG, Curran HV, Feilding A, Nutt DJ (2016) Neural correlates of the LSD experience revealed by multimodal neuroimaging. Proc Natl Acad Sci U S A 113(17):4853–4858. doi:10.1073/pnas.1518377113
Carter OL, Burr DC, Pettigrew JD, Wallis GM, Hasler F, Vollenweider FX (2005) Using psilocybin to investigate the relationship between attention, working memory, and the serotonin 1A and 2A receptors. J Cogn Neurosci 17(10):1497–1508. doi:10.1162/089892905774597191
Celada P, Puig MV, Amargós-Bosch M, Adell A, Artigas F (2004) The therapeutic role of 5-HT1A and 5-HT2A receptors in depression. J Psychiatry Neurosci 29(4):252–265
Chandler AL, Hartman MA (1960) Lysergic acid diethylamide (LSD-25) as a facilitating agent in psychotherapy. Arch Gen Psychiatry 2(3):286–299. doi:10.1001/archpsyc.1960.03590090042008
Dammann G, Dürsteler-Macfarland KM, Strasser H, Skipper GE, Wiesbeck GA, Wurst FM (2014) Cannabis use among a sample of 16 to 18 year old students in Switzerland. Psychiatr Danub 26(1):56–65
Dittrich A (1996) Aetiologie-unabhängige Strukturen veränderter Wachbewusstseinszustände: Ergebnisse empirischer Untersuchungen über Halluzinogene I. Und II. Ordnung, sensorische Deprivation, hypnagoge Zustände, hypnotische Verfahren sowie Reizüberflutung. VWB, Berlin
Dolder PC, Schmid Y, Haschke M, Rentsch KM, Liechti ME (2015) Pharmacokinetics and concentration-effect relationship of oral LSD in humans. Int J Neuropsychopharmacol 19(1):1–7. doi:10.1093/ijnp/pyv072
Driver H, Flanigan M, Bentley A, Mitchell D, Luus H, Shapiro C (1995) The influence of ipsapirone, a 5-HT1A agonist, on sleep patterns of healthy subjects. Psychopharmacology 117(2):186–192. doi:10.1007/BF02245186
Ermentrout G, Cowan J (1979) A mathematical theory of visual hallucination patterns. Biol Cybernetics 34(3):137–150. doi:10.1007/BF00336965
Ettrup A, Cunha-Bang SD, Mcmahon B, Lehel S, Dyssegaard A, Skibsted AW, Jørgensen LM, Hansen M, Baandrup AO, Bache S, Svarer C, Kristensen JL, Gillings N, Madsen J, Knudsen GM (2014) Serotonin 2A receptor agonist binding in the human brain with [11C] Cimbi-36. J Cereb Blood Flow Metab 34(7):1188–1196. doi:10.1038/jcbfm.2014.68
Family N, Vinson D, Vigliocco G, Kaelen M, Bolstridge M, Nutt DJ, Carhart-Harris RL (2016) Semantic activation in LSD: evidence from picture naming. Language, Cognition and Neuroscience 31(10):1320–1327. doi:10.1080/23273798.2016.1217030
Fischer R, Landon GM (1972) On the arousal state-dependent recall of 'subconscious' experience: stateboundness. Br J Psychiatry 120(555):159–172. doi:10.1192/bjp.120.555.159
Fischman LG (1983) Dreams, hallucinogenic drug states, and schizophrenia: a psychological and biological comparison. Schizophr Bull 9(1):73–94. doi:10.1093/schbul/9.1.73
Fosse R, Stickgold R, Hobson JA (2004) Thinking and hallucinating: reciprocal changes in sleep. Psychophysiology 41(2):298–305. doi:10.1111/j.1469-8986.2003.00146.x
Franke GH, Derogatis LR (1995) Die Symptom-Checkliste von Derogatis SCL-90-R; deutsche Version; Manual. Beltz-Test-GmbH, Göttingen
Frecska E, Móré CE, Vargha A, Luna LE (2012) Enhancement of creative expression and entoptic phenomena as after-effects of repeated ayahuasca ceremonies. J Psychoactive Drugs 44(3):191–199. doi:10.1080/02791072.2012.703099
Frederking W (1955) Intoxicant drugs (mescaline and lysergic acid diethylamide) in psychotherapy. J Nerv Ment Dis 121(3):262–266
Giacomelli S, Palmery M, Romanelli L, Cheng C, Silvestrini B (1998) Lysergic acid diethylamide (LSD) is a partial agonist of D2 dopaminergic receptors and it potentiates dopamine-mediated prolactin secretion in lactotrophs in vitro. Life Sci 63(3):215–222. doi:10.1016/S0024-3205(98)00262-8
Gillin J, Jernajczyk W, Valladares-Neto D, Golshan S, Lardon M, Stahl S (1994) Inhibition of REM sleep by ipsapirone, a 5HT1A agonist, in normal volunteers. Psychopharmacology 116(4):433–436. doi:10.1007/BF02247474
Glicksohn J (1992) An exploratory study of syncretic experience: eidetics, synaesthesia and absorption. Perception 21(5):637–642. doi:10.1068/p210637
González-Maeso J, Weisstaub NV, Zhou M, Chan P, Ivic L, Ang R, Lira A, Bradley-Moore M, Ge Y, Zhou Q, Sealfon SC, Gingrich JA (2007) Hallucinogens recruit specific cortical 5-HT2A receptor-mediated signaling pathways to affect behavior. Neuron 53(3):439–452. doi:10.1016/j.neuron.2007.01.008
Gottesmann C (2006) The dreaming sleep stage: a new neurobiological model of schizophrenia? Neuroscience 140(4):1105–1115. doi:10.1016/j.neuroscience.2006.02.082
Green WJ (1969) LSD and the sleep-dream cycle. Experimental medicine and surgery 27(1–2):138–144
de Gregorio D, Posa L, Ochoa-Sanchez R, Mclaughlin R, Maione S, Comai S, Gobbi G (2016) The hallucinogen d-lysergic diethylamide (LSD) decreases dopamine firing activity through 5-HT1A, D2 and TAAR1 receptors. Pharmacol Res 113:81–91. doi:10.1016/j.phrs.2016.08.022
Guilford JP (1967) The nature of human intelligence. McGraw-Hill, New York
Halberstadt AL (2015) Recent advances in the neuropsychopharmacology of serotonergic hallucinogens. Behav Brain Res 277:99–120. doi:10.1016/j.bbr.2014.07.016
Halberstadt A, Geyer M (2010) LSD but not lisuride disrupts prepulse inhibition in rats by activating the 5-HT2A receptor. Psychopharmacology 208(2):179–189. doi:10.1007/s00213-009-1718-x
Halberstadt AL, Geyer MA (2011) Multiple receptors contribute to the behavioral effects of indoleamine hallucinogens. Neuropharmacology 61(3):364–381. doi:10.1016/j.neuropharm.2011.01.017
Halgren E, Walter RD, Cherlow DG, Crandall PH (1978) Mental phenomena evoked by electrical stimulation of the human hippocampal formation and amygdala. Brain 101(1):83–115. doi:10.1093/brain/101.1.83
Hobson JA (2001) The dream drugstore: chemically altered states of consciousness. MIT Press, Cambridge
Hobson JA (2009) REM sleep and dreaming: towards a theory of protoconsciousness. Nature Reviews Neuroscience 10(11):803–813. doi:10.1038/nrn2716
Jacobs B (1978) Dreams and hallucinations: a common neurochemical mechanism mediating their phenomenological similarities. Neurosci Biobehav Rev 2(1):59–69. doi:10.1016/0149-7634(78)90007-6
Johnson MW, Richards W, Griffiths R (2008) Human hallucinogen research: guidelines for safety. J Psychopharmacol 22(6):603–620. doi:10.1177/0269881108093587
Kahn D (2013) Brain basis of self: self-organization and lessons from dreaming. Front Psychol 4(1):408. doi:10.3389/fpsyg.2013.00408
Kometer M, Schmidt A, Jäncke L, Vollenweider FX (2013) Activation of serotonin 2A receptors underlies the psilocybin-induced effects on α oscillations, N170 visual-evoked potentials, and visual hallucinations. J Neurosci 33(25):10544–10551. doi:10.1523/JNEUROSCI.3007-12.2013
Kometer M, Pokorny T, Seifritz E, Vollenweider FX (2015) Psilocybin-induced spiritual experiences and insightfulness are associated with synchronization of neuronal oscillations. Psychopharmacology 232(19):3663–3676. doi:10.1007/s00213-015-4026-7
Krebs-Thomson K, Geyer MA (1998) Evidence for a functional interaction between 5-HT1A and 5-HT2 receptors in rats. Psychopharmacology 140(1):69–74. doi:10.1007/s002130050740
LaBerge S, Rheingold H (1991) Exploring the world of lucid dreaming. Ballantine Books, New York
Lakoff G (1993) How metaphor structures dreams. Dreaming 3(2):77–98. doi:10.1037/h0094373
Landon M, Fischer R (1970) On similar linguistic structures in creative performance and psilocybin-induced experience. Confinia psychiatrica 13(2):115–138
Lebedev AV, Lövdén M, Rosenthal G, Feilding A, Nutt DJ, Carhart-Harris RL (2015) Finding the self by losing the self: neural correlates of ego-dissolution under psilocybin. Hum Brain Mapp 36(8):3137–3153. doi:10.1002/hbm.22833
Leuner H (1968) Basic functions involved in the psychotherapeutic effect of psychotomimetics. In: Shlien JM (ed) Research in psychotherapy. American Psychological Association, Washington, pp 466–470
Leuner H (1969) Guided affective imagery (GAI). A method of intensive psychotherapy. Am J Psychother 23(1):4–21
Leuner H (1973) Creativity and modification of consciousness. Confinia psychiatrica 16(3):141–158
Leuner H (1981) Halluzinogene. Hans Huber, Bern
Leysen JE, Niemegeers CJ, van Nueten JM, Laduron PM (1982) [3H]Ketanserin (R 41 468), a selective 3H-ligand for serotonin2 receptor binding sites. Binding properties, brain distribution, and functional role. Mol Pharmacol 21(2):301–314
Limosani I, D'Agostino A, Manzone ML, Scarone S (2011) Bizarreness in dream reports and waking fantasies of psychotic schizophrenic and manic patients: empirical evidences and theoretical consequences. Psychiatry Res 189(2):195–199. doi:10.1016/j.psychres.2011.02.023
Llinás R, Ribary U (1993) Coherent 40-Hz oscillation characterizes dream state in humans. Proc Natl Acad Sci U S A 90(5):2078–2081. doi:10.1073/pnas.90.5.2078
Maquet P, Péters J, Aerts J, Delfiore G, Degueldre C, Luxen A, Franck G (1996) Functional neuroanatomy of human rapid-eye-movement sleep and dreaming. Nature 383(6596):163–166. doi:10.1038/383163a0
Marona-Lewicka D, Nichols DE (2007) Further evidence that the delayed temporal dopaminergic effects of LSD are mediated by a mechanism different than the first temporal phase of action. Pharmacol Biochem Behav 87(4):453–461. doi:10.1016/j.pbb.2007.06.001
Marona-Lewicka D, Thisted RA, Nichols DE (2005) Distinct temporal phases in the behavioral pharmacology of LSD: dopamine D2 receptor-mediated effects in the rat and implications for psychosis. Psychopharmacology 180(3):427–435. doi:10.1007/s00213-005-2183-9
Martindale C, Fischer R (1977) The effects of psilocybin on primary process content in language. Confinia psychiatrica 20(4):195–202
Massimini M, Ferrarelli F, Murphy M, Huber R, Riedner B, Casarotto S, Tononi G (2010) Cortical reactivity and effective connectivity during REM sleep in humans. Cognitive neuroscience 1(3):176–183. doi:10.1080/17588921003731578
Mégevand P, Groppe DM, Goldfinger MS, Hwang ST, Kingsley PB, Davidesco I, Mehta AD (2014) Seeing scenes: topographic visual hallucinations evoked by direct electrical stimulation of the parahippocampal place area. J Neurosci 34(16):5399–5405. doi:10.1523/JNEUROSCI.5202-13.2014
Meltzer HY, Li Z, Kaneda Y, Ichikawa J (2003) Serotonin receptors: their key role in drugs to treat schizophrenia. Prog Neuro-Psychopharmacol Biol Psychiatry 27(7):1159–1172. doi:10.1016/j.pnpbp.2003.09.010
Meltzer HY, Mills R, Revell S, Williams H, Johnson A, Bahr D, Friedman JH (2009) Pimavanserin, a serotonin2A receptor inverse agonist, for the treatment of Parkinson’s disease psychosis. Neuropsychopharmacology 35(4):881–892. doi:10.1038/npp.2009.176
Merz J, Lehrl S, Galster V, Erzigkeit H (1975) MWT-B: ein Intelligenzkurztest. Psychiatrie Neurologie und Medizinische Psychologie 27(7):423–428
Muthukumaraswamy SD, Carhart-Harris RL, Moran RJ, Brookes MJ, Williams TM, Erritzoe D, Sessa B, Papadopoulos A, Bolstridge M, Singh KD, Feilding A, Friston KJ, Nutt DJ (2013) Broadband cortical desynchronization underlies the human psychedelic state. J Neurosci 33(38):15171–15183. doi:10.1523/JNEUROSCI.2063-13.2013
Muzio JN, Roffwarg HP, Kaufman E (1966) Alterations in the nocturnal sleep cycle resulting from LSD. Electroencephalogr Clin Neurophysiol 21(4):313–324. doi:10.1016/0013-4694(66)90037-X
Nichols DE (2004) Hallucinogens. Pharmacol Ther 101(2):131–181. doi:10.1016/j.pharmthera.2003.11.002
Nir Y, Tononi G (2010) Dreaming and the brain: from phenomenology to neurophysiology. Trends Cogn Sci 14(2):88–100. doi:10.1016/j.tics.2009.12.001
Pace-Schott EF (2008) Serotonin and dreaming. In: Monti JM, Pandi-Perumal SR, Jacobs BL, Nutt DJ (eds) Serotonin and sleep: molecular, functional and clinical aspects. Birkhäuser Verlag, Basel, pp 307–324
Pace-Schott EF, Gersh T, Silvestri R, Stickgold R, Salzman C, Hobson JA (2001) SSRI treatment suppresses dream recall frequency but increases subjective dream intensity in normal subjects. J Sleep Res 10(2):129–142. doi:10.1046/j.1365-2869.2001.00249.x
Passie T, Halpern JH, Stichtenoth DO, Emrich HM, Hintzen A (2008) The pharmacology of lysergic acid diethylamide: a review. CNS neuroscience & therapeutics 14(4):295–314. doi:10.1111/j.1755-5949.2008.00059.x
Persson B, Pettersson A, Hedner T (1987) Pharmacokinetics of ketanserin in patients with essential hypertension. Eur J Clin Pharmacol 32(3):259–265. doi:10.1007/BF00607573
Petri G, Expert P, Turkheimer F, Carhart-Harris R, Nutt D, Hellyer PJ, Vaccarino F (2014) Homological scaffolds of brain functional networks. J R Soc Interface 11(101):20140873. doi:10.1098/rsif.2014.0873
Pines M (1976) A psychoanalytic view of sleep. Postgrad Med J 52(603):26–31. doi:10.1136/pgmj.52.603.26
Pokorny T, Preller KH, Kraehenmann R, Vollenweider FX (2016) Modulatory effect of the 5-HT1A agonist buspirone and the mixed non-hallucinogenic 5-HT1A/2A agonist ergotamine on psilocybin-induced psychedelic experience. Eur Neuropsychopharmacol 26(4):756–766. doi:10.1016/j.euroneuro.2016.01.005
Preller KH, Herdener M, Pokorny T, Planzer A, Kraehenmann R, Stämpfli P, Liechti ME, Seifritz E, Vollenweider FX (2017) The fabric of meaning and subjective effects in LSD-induced states depend on serotonin 2A receptor activation. Curr Biol 27(3):451–457. doi:10.1016/j.cub.2016.12.030
Quednow BB, Kometer M, Geyer MA, Vollenweider FX (2012) Psilocybin-induced deficits in automatic and controlled inhibition are attenuated by ketanserin in healthy human volunteers. Neuropsychopharmacology 37(3):630–640. doi:10.1038/npp.2011.228
Rasmussen AR, Parnas J (2015) Anomalies of imagination and disordered self in schizophrenia spectrum disorders. Psychopathology 48(5):317–323. doi:10.1159/000431291
Rechtschaffen A (1978) The single-mindedness and isolation of dreams. Sleep 1(1):97–109. doi:10.1093/sleep/1.1.97
Rittenhouse CD, Stickgold R, Hobson JA (1994) Constraint on the transformation of characters, objects, and settings in dream reports. Conscious Cogn 3(1):100–113. doi:10.1006/ccog.1994.1007
Roseman L, Sereno MI, Leech R, Kaelen M, Orban C, McGonigle J, Feilding A, Nutt DJ, Carhart-Harris RL (2016) LSD alters eyes-closed functional connectivity within the early visual cortex in a retinotopic fashion. Hum Brain Mapp 37(8):3031–3040. doi:10.1002/hbm.23224
Sandison RA (1954) Psychological aspects of the LSD treatment of the neuroses. J Ment Sci 100(419):508–515. doi:10.1192/bjp.100.419.508
Sandison RA, Whitelaw JD (1957) Further studies in the therapeutic value of lysergic acid diethylamide in mental illness. J Ment Sci 103(431):332–343. doi:10.1192/bjp.103.431.332
Sandison RA, Spencer AM, Whitelaw JD (1954) The therapeutic value of lysergic acid diethylamide in mental illness. J Ment Sci 100(419):491–507. doi:10.1192/bjp.100.419.491
Sass LA, Byrom G (2015) Self-disturbance and the bizarre: on incomprehensibility in schizophrenic delusions. Psychopathology 48(5):293–300. doi:10.1159/000437210
Savage C (1955) Variations in ego feeling induced by d-lysergic acid diethylamide (LSD-25). Psychoanal Rev 42(1):1–16
Scarone S, Manzone ML, Gambini O, Kantzas I, Limosani I, D'Agostino A, Hobson JA (2008) The dream as a model for psychosis: an experimental approach using bizarreness as a cognitive marker. Schizophr Bull 34(3):515–522. doi:10.1093/schbul/sbm116
Schmid Y, Enzler F, Gasser P, Grouzmann E, Preller KH, Vollenweider FX, Brenneisen R, Müller F, Borgwardt S, Liechti ME (2015) Acute effects of lysergic acid diethylamide in healthy subjects. Biol Psychiatry 78(8):544–553. doi:10.1016/j.biopsych.2014.11.015
Schreiber R, Brocco M, Audinot V, Gobert A, Veiga S, Millan MJ (1995) (1-(2,5-Dimethoxy-4 iodophenyl)-2-aminopropane)-induced head-twitches in the rat are mediated by 5-hydroxytryptamine (5-HT)2A receptors: modulation by novel 5-HT2A/2C antagonists, D1 antagonists and 5-HT1A agonists. J Pharmacol Exp Ther 273(1):101–112
Sessa B (2008) Is it time to revisit the role of psychedelic drugs in enhancing human creativity? J Psychopharmacol 22(8):821–827. doi:10.1177/0269881108091597
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC (1998) The mini-International neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 59(Suppl. 20):22–33
Sinke C, Halpern JH, Zedler M, Neufeld J, Emrich HM, Passie T (2012) Genuine and drug-induced synesthesia: a comparison. Conscious Cogn 21(3):1419–1434. doi:10.1016/j.concog.2012.03.009
Sio U, Monaghan P, Ormerod T (2013) Sleep on it, but only if it is difficult: effects of sleep on problem solving. Mem Cogn 41(2):159–166. doi:10.3758/s13421-012-0256-7
Snyder SH, Faillace LA, Weingartner H (1969) A new psychotropic agent. Psychological and physiological effects of 2,5-dimethoxy-4-ethyl amphetamine (DOET) in man. Arch Gen Psychiatry 21(1):95–101. doi:10.1001/archpsyc.1969.01740190097014
Snyder SH, Weingartner H, Faillace LA (1971) DOET (2,5-dimethoxy-4-ethylamphetamine), a new psychotropic drug: effects of varying doses in man. Arch Gen Psychiatry 24(1):50–55. doi:10.1001/archpsyc.1971.01750070052006
Solms M (2000) Dreaming and REM sleep are controlled by different brain mechanisms. The Behavioral and brain sciences 23(6):843–850. doi:10.1017/S0140525X00003988
Spitzer M, Thimm M, Hermle L, Holzmann P, Kovar K-A, Heimann H, Gouzoulis-Mayfrank E, Kischka U, Schneider F (1996) Increased activation of indirect semantic associations under psilocybin. Biol Psychiatry 39(12):1055–1057. doi:10.1016/0006-3223(95)00418-1
Strassman RJ (1995) Human psychopharmacology of N,N-dimethyltryptamine. Behav Brain Res 73(1):121–124. doi:10.1016/0166-4328(96)00081-2
Studerus E, Kometer M, Hasler F, Vollenweider FX (2011) Acute, subacute and long-term subjective effects of psilocybin in healthy humans: a pooled analysis of experimental studies. J Psychopharmacol 25(11):1434–1452. doi:10.1177/0269881110382466
Stumbrys T, Erlacher D, Malinowski P (2015) Meta-awareness during day and night. Imagination, Cognition and Personality 34(4):415–433. doi:10.1177/0276236615572594
Sweat N, Bates L, Hendricks PS (2016) The associations of naturalistic classic psychedelic use, mystical experience, and creative problem solving. J Psychoactive Drugs 48(5):344–350. doi:10.1080/02791072.2016.1234090
Tagliazucchi E, Carhart-Harris R, Leech R, Nutt D, Chialvo DR (2014) Enhanced repertoire of brain dynamical states during the psychedelic experience. Hum Brain Mapp 35(11):5442–5456. doi:10.1002/hbm.22562
Terhune DB, Luke DP, Kaelen M, Bolstridge M, Feilding A, Nutt D, Carhart-Harris R, Ward J (2016) A placebo-controlled investigation of synaesthesia-like experiences under LSD. Neuropsychologia 88:28–34. doi:10.1016/j.neuropsychologia.2016.04.005
Thompson DF, Pierce DR (1999) Drug-induced nightmares. Ann Pharmacother 33(1):93–98. doi:10.1345/aph.18150
Torda C (1968) Contribution to serotonin theory of dreaming (LSD infusion). New York state journal of medicine 68(9):1135–1138
Valle M, Maqueda AE, Rabella M, Rodríguez-Pujadas A, Antonijoan RM, Romero S, Alonso JF, Mañanas MÀ, Barker S, Friedlander P, Feilding A, Riba J (2016) Inhibition of alpha oscillations through serotonin-2A receptor activation underlies the visual effects of ayahuasca in humans. Eur Neuropsychopharmacol 26(7):1161–1175. doi:10.1016/j.euroneuro.2016.03.012
Vollenweider FX, Geyer MA (2001) A systems model of altered consciousness: integrating natural and drug-induced psychoses. Brain Res Bull 56(5):495–507. doi:10.1016/S0361-9230(01)00646-3
Vollenweider FX, Leenders KL, Scharfetter C, Maguire P, Stadelmann O, Angst J (1997) Positron emission tomography and fluorodeoxyglucose studies of metabolic hyperfrontality and psychopathology in the psilocybin model of psychosis. Neuropsychopharmacology 16(5):357–372. doi:10.1016/S0893-133X(96)00246-1
Vollenweider FX, Vollenweider-Scherpenhuyzen MF, Bäbler A, Vogel H, Hell D (1998) Psilocybin induces schizophrenia-like psychosis in humans via a serotonin-2 agonist action. Neuroreport 9(17):3897–3902
Voss U, Holzmann R, Hobson A, Paulus W, Koppehele-Gossel J, Klimke A, Nitsche MA (2014) Induction of self awareness in dreams through frontal low current stimulation of gamma activity. Nat Neurosci 17(6):810–812. doi:10.1038/nn.3719
Wagner U, Gais S, Haider H, Verleger R, Born J (2004) Sleep inspires insight. Nature 427(6972):352–355. doi:10.1038/nature02223
Weingartner H, Snyder SH, Faillace LA, Markley H (1970) Altered free associations: some cognitive effects of DOET (2,5-dimethoxy-4-ethylamphetamine). Behav Sci 15(4):297–303. doi:10.1002/bs.3830150402
Weintraub W, Silverstein AB, Klee GD (1959) The effect of LSD on the associative processes. J Nerv Ment Dis 128(5):409–414
Williams J, Merritt J, Rittenhouse C, Hobson JA (1992) Bizarreness in dreams and fantasies. Conscious Cogn 1(2):172–185. doi:10.1016/1053-8100(92)90059-J
Wittchen H-U, Fydrich T (1997) Strukturiertes Klinisches Interview für DSM-IV (SKID-I und SKID-II). Hogrefe, Göttingen
Acknowledgements
This study was financially supported by grants from the Heffter Research Institute (1-190413), the Swiss Neuromatrix Foundation (2015-0103), the Usona Institute (2015-2056) and the Swiss National Science Foundation (SNSF, P2ZHP1_161626).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Kraehenmann, R., Pokorny, D., Vollenweider, L. et al. Dreamlike effects of LSD on waking imagery in humans depend on serotonin 2A receptor activation. Psychopharmacology 234, 2031–2046 (2017). https://doi.org/10.1007/s00213-017-4610-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-017-4610-0