
Abstract
Rationale
Alcohol increases the tendency for risky driving in some individuals but not others. Little is known about the factors underlying this individual difference. Studies find that those who underestimate their blood alcohol concentration (BAC) following a dose of alcohol tend to be more impulsive and report greater willingness to drive after drinking than those who estimate their BACs to be greater than their actual BAC. BAC underestimation could contribute to risky driving behavior following alcohol as such drivers might perceive little impairment in their driving ability and thus no need for caution.
Objectives
This study was designed to test the relationship between drivers’ BAC estimations following a dose of alcohol or a placebo and the degree of risky driving they displayed during a simulated driving test.
Methods
Forty adult drivers performed a simulated driving test and estimated their blood alcohol concentration after receiving a dose of alcohol (0.65 g/kg for men and 0.56 g/kg for women) or a placebo.
Results
Alcohol increased risk-taking and impaired driving skill. Those who estimated their BAC to be lower were the riskiest drivers following both alcohol and placebo.
Conclusions
The tendency to estimate lower BACs could support a series of high-risk decisions, regardless of one’s actual BAC. This could include the decision to drive after drinking.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In the USA, driving under the influence of alcohol (DUI) offense is determined by a per se law for which the legal blood alcohol concentration (BAC) limit is 80 mg/dL. However, many alcohol-related motor vehicle collisions (MVCs) occur below the legal limit. This is consistent with laboratory research that indicates individuals at the same BAC can differ greatly in their responses to alcohol. For example, studies have shown marked individual differences in the behavioral response to a dose of alcohol that cannot be accounted for by individual differences in the subjects’ BACs (Linnoila et al. 1986; Nicholson et al. 1992; Fillmore and Vogel-Sprott 1998). As such, subject characteristics and environmental factors might also contribute to the intensity of impairment.
One personal characteristic that has attracted research attention concerns the drinker’s self-perception of alcohol intoxication (e.g., Beirness 1987). Such self-evaluations are influenced by a host of factors, including interoceptive cues (e.g., euphoria and light headedness) and behavioral changes associated with intoxication (e.g., slurred speech and impaired gait). These cues can serve as a basis for drinkers to estimate their BAC, which can affect efficacy judgments concerning their overall functioning (Verdejo-Garcia et al. 2012). However, drinkers tend to be naive about alcohol pharmacokinetics and there is often a discrepancy between their estimated BAC after drinking and their observed BAC (Martin et al. 1991; Grant et al. 2012). Indeed, errors of overestimation and underestimation of BAC have been reported (Beirness 1984, 1987). Underestimation is thought to result from reduced sensitivity to interoceptive and behavioral cues that signal impairment. Errors of underestimation are especially dangerous if drinkers perceive they are fit to drive despite elevated BACs (Martin et al. 1991; Grant et al. 2012).
Indeed, laboratory studies find that underestimators are more willing to drive when above the legal limit relative to those who are more accurate in their estimations (Beirness 1984, 1987). There is also some evidence that such individual differences in patterns of BAC estimation and willingness to drive remain stable over time (Quinn and Fromme 2012). Underestimators also tend to generally prefer risky over safer alternatives (e.g., Proestakis et al. 2013). Those who underestimate their BAC also report more problems with alcohol (Bois and Vogel-Sprott 1974; Lansky et al. 1978; Beirness 1984, 1987; Aston and Liguori 2013; Aston et al. 2013). Collectively, the results suggest that BAC underestimation might be characteristic of impulsive individuals and could account for their increased willingness to drive after drinking.
There is convincing evidence that BAC underestimation can promote the decision to drive after drinking. However, little is known about how underestimation of BAC might affect driving behaviors. Alcohol impairs driving skills including steering and the ability to maintain vehicle position on the roadway (Moskowitz and Fiorentino 2000). Alcohol also increases driver risk-taking, such as tailgating (Fillmore et al. 2008; Laude and Fillmore 2015). Some drivers experience elevations in their risk-taking while driving skill is minimally impaired, whereas others show little change in risk-taking following alcohol but display considerable impairment in their skill (Laude and Fillmore 2015).
BAC underestimation could account for individual differences in risky driving under alcohol. Those who believe they are below their actual BAC might perceive fewer negative consequences from their behavior and thus increase the amount of risk they are willing to accept when driving (Fromme et al. 1997). In contrast, those who overestimate their BAC may be more cognizant of potential hazardous consequences of alcohol-related impairments and reduce the amount of risk for injury/collision they are willing to take when driving.
The present study sought to test the role of BAC estimation error on adult drivers’ risk-taking and their skill level during tests of simulated driving. Drivers were tested in two different simulated driving scenarios. One scenario was a “skill-relevant” situation that emphasized drivers’ visual motor skill. The other drive presented a “risk-relevant” situation that instigated risk-taking behavior (i.e., tailgating) by placing participants in a high-traffic situation. Drinkers’ self-estimation of their BAC was obtained using a Likert-type rating scale. Tests were completed under an active dose of alcohol and a placebo. The active dose of alcohol was expected to impair driving skill and increase risky driving. We also predicted that drivers who estimated lower BACs would display the greatest risk-taking under the drug.
Method
Participants
Forty adult drivers (21 women and 19 men) between the ages of 21 and 34 years participated in the study. Online postings and fliers advertised for volunteers for studies on the effects of alcohol on behavioral performance. Interested individuals called the laboratory to schedule an appointment for screening. All volunteers had to hold a valid driver’s license for the past 3 years. Individuals reporting any psychiatric disorder, CNS injury, or head trauma were excluded from participation. Volunteers consisted of drinkers who self-reported consuming alcohol at least twice per month, with at least two drinks per occasion, over the past 90 days. Individuals were excluded if their current alcohol use met dependence/withdrawal criteria as determined by the substance use disorder module of the Structured Clinical Interview for DSM-IV (SCID-IV). No participant reported the use of any psychoactive prescription medication. Urine samples were obtained to test for metabolites of amphetamines (including methylphenidate), barbiturates, benzodiazepines, cocaine, opiates, and tetrahydrocannabinol (THC; ICUP drug screen by Instant Technologies). Any volunteer who tested positive for the presence of any of these drugs during any test session was excluded from the study. However, participants who tested positive for THC were retained, provided that they did not self-report past day use. No female volunteers who were pregnant or breast-feeding participated in the research, as determined by self-report and urine human chorionic gonadotrophin levels (Icon25 Hcg urine test by Beckman Coulter). All sessions were conducted in the Human Behavioral Pharmacology Laboratory of the Department of Psychology. Volunteers were required to abstain from alcohol and any other psychoactive substances for 24 h and to fast for 4 h prior to each test session. At the beginning of each session, a zero breath alcohol concentration (BrAC) was verified by the Intoxilyzer (model 400, CMI Inc.).
Apparatus and materials
A computerized driving simulator was used to measure driving behaviors (STISIM Drive, Systems Technology Inc., Hawthorne, CA). The simulations placed the participant in the driver seat of the vehicle, which was controlled by steering wheel movements and manipulations of the accelerator and brake pedals. Crashes, either into another vehicle or off of the road, resulted in the presentation and sound of a shattered windshield. The program then reset the driver in the center of the right lane.
Driver risk-taking test
This 5–10-min drive (depending on the speed of the participant) examined risky driving behavior. Participants drove 21,100 ft on a busy street with four lanes in a metropolitan setting. Each direction of traffic comprised two lanes. The driver was free to navigate among other vehicles within the driver’s two lanes of traffic. Other vehicles traveled at various speeds in both lanes, which forced the driver to change lanes to overtake vehicles traveling at slower speeds. There was no posted speed limit. To instigate the potential for risk-taking, drivers could earn monetary reinforcement for quickly completing the drive; $5 for completion under 5 min, $4 for 5–6 min, $3 for 6–7 min, $2 for 7–8 min, $1 for 9–10 min, and $0.50 for over 10 min. There was a penalty for crashing (loss of $0.25/crash), which conflicted with the incentive to speed during the trip. Tests using this type of response conflict have been used in other research to examine acute effects of alcohol on risky driving behavior (Fillmore et al. 2008).
Driver skill test
This drive measured ability to control the lane position of the vehicle. This 15-min driving course consisted of 80,000 ft of a winding two-lane highway through a rural setting with overcast skies, buildings, and trees. Drivers were instructed to maintain a constant speed of 55 mph while remaining in the center of the right lane. The drive scenario included both straight and winding sections, requiring vigilance on the part of the driver in order to maintain the vehicle in the center of the lane. This drive has been used in prior work to test the impairing effects of alcohol on driving skill (e.g., Harrison et al. 2007).
BAC estimation
Participants estimated their BAC on a Likert-type rating scale ranging from 0 to 160 mg/dL with graduated demarcations each 5 mg/dL. The current legal driving limit for intoxication in the USA (80 mg/dL) was indicated by the words “legal limit” as the center point on the scale. Drivers were to estimate their BAC relative to the legal limit by putting a slash through the corresponding point on the scale. The legal limit was included as a reference point for subjects because it is a common, lay definition that could be used to make decisions about driving after drinking. This measure has been used in other alcohol studies (e.g., Harrison et al. 2007).
Subjective intoxication
Participants evaluated their level of intoxication on 100-mm visual analogue scale with anchors of 0 “not at all” to 100 “very much.” This scale has been used in other alcohol studies (e.g., Harrison et al. 2007).
Driving History and Experience Questionnaire
This self-report questionnaire gathered information on length of time holding a driver’s license and number of days driven/week.
Drinking habits
The timeline follow-back calendar (TLFB; Sobell and Sobell 1992) measured the number of days subjects drank alcohol over the past 90 days and the total number of drinks consumed over that period. The Personal Drinking Habits Questionnaire (PDHQ) measured the subject’s customary number of standard drinks and weekly frequency of drinking (Vogel-Sprott 1992).
Procedure
Familiarization session
The purpose of this session was to familiarize participants with laboratory procedures and obtain information on driving history, drug use, drinking patterns, general health status, and demographic characteristics. Participants also practiced the risk- and skill-relevant drives.
Test sessions
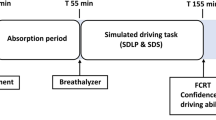
Each dose was administered on a separate test session, and all participants received each dose. Dose administration was blind and dose order was counterbalanced across participants. At the beginning of each session, participants received either an active dose of alcohol or a placebo. The active dose was administered as 95 % alcohol containing one part alcohol and three parts carbonated mix. Men received a 0.65 g/kg dose of alcohol. Because women can achieve higher BACs than men for a given dose, they received 86 % of the 0.65 g/kg dose (i.e., 0.56 g/kg alcohol; Fillmore 2001). The dose typically produces an average peak BrAC of 80 mg/dL, approximately 60–70 min after drinking. The dose was chosen based on prior research that has shown that it reliably affects driving behavior in driving simulations (Harrison and Fillmore 2005; Weafer and Fillmore 2012). The placebo consisted of a volume of carbonated mix that matched the total volume of the alcohol drink. A small amount (3 mL) of alcohol was floated on the surface of the beverage. Glasses were sprayed with an alcohol mist that resembled condensation and provided a strong alcoholic scent. Each dose was consumed within 6 min.
Subjects performed the task battery: (1) driver skill test, (2) driver risk-taking test, (3) subjective intoxication self-report, and (4) BAC estimation self-report. Drive tests were presented in a fixed order to avoid generalization of incentivizing behavior from the test of driver risk to the test of driver skill. The test battery began 40 min post-drinking and ended at 70 min. All testing occurred during the ascending period of the BAC curve. BrACs were measured at 40 and 70 min (Intoxilyzer model 400, CMI Inc.). Breath samples were also taken following placebo ostensibly to measure BrAC. After a test session concluded, participants relaxed in a waiting room. They received a meal and were released when their BrAC fell below 20 mg/dL. Transportation home was provided. Upon completing the final session, participants were paid and debriefed.
Criterion measures
Driver risk-taking: measured by time to collision
Time to collision (TTC) is a time-related safety margin measure (Taieb-Maimon and Shinar 2001), determined by the bumper-to-bumper distance between two vehicles divided by the closing speed of the vehicles (Zhang and Kaber 2013). TTC is operationally defined as the time that remains until collision occurs if the lead and the driven vehicle were to continue on the same course (Zhang and Kaber 2013). A TTC value was calculated for each traffic situation encountered by the driven car. The TTC score for a given subject was then defined as the minimum TTC value in the distribution of traffic encounters. This encounter represents the riskiest instance or the point the driver came closest to an accident across the drive. Riskier driving was indicated by smaller TTC values (seconds). Average drive speed (mph) and accident frequency were also recorded.
Driver skill: measured by lane position standard deviation
Lane position standard deviation (LPSD) indicates the degree of adjustment a driver implements to maintain position within the center of the driven lane. Within-lane position of the vehicle was obtained by averaging the deviation measures sampled at each foot. LPSD was taken as the standard deviation of the average within-lane position. Greater within-lane deviation indicates poorer driving skill. The measure has been used in other alcohol studies (e.g., Weafer and Fillmore 2012). Average drive speed (mph) and accident frequency were also recorded.
Results
Demographics, drug and alcohol use, and driving history
Table 1 lists demographic and other background characteristics of participants. The racial makeup of the sample was as follows: Caucasian (n = 28), African-American (n = 7), Asian (n = 4), and one participant who reported belonging to a category not listed. The sample was comprised of experienced drivers who regularly operated a motor vehicle. On average, participants drank on one third of the last 90 days, three drinks per occasion (Table 1). Regarding past 30-day drug use, the sample reported tobacco (n = 13), THC (n = 15), and stimulant drug use (n = 2). No daily use of any drug except for caffeine was reported. Ten participants tested positive for THC but reported they had not used within 24 h prior to each session.
Observed and estimated blood alcohol concentrations
BACs following the active dose were comparable across time in both male and female drivers. A 2 (sex) × 2 time (40 vs. 70 min) mixed-model analysis of variance (ANOVA) obtained no significant main effects or interactions, ps > 0.06. Based on the entire sample, the mean BrAC was 62.7 mg/dL (SD = 14.0) at 40 min and 71.4 mg/dL (SD = 13.1) at 70 min. No BAC was detected following placebo.
Drivers’ estimations of their BAC were higher following alcohol than placebo (alcohol M = 84.6 mg/dL, SD = 31.6; placebo M = 36.9 mg/dL, SD = 27.2), and this was confirmed by a significant one-way ANOVA of dose condition, F (1, 39) = 80.47, p < 0.01, η 2 = 0.67.
Estimation error was quantified by taking individuals’ estimated BAC minus their observed BAC at that time (70 min post-drinking). Drivers’ mean estimated BAC was significantly greater than their mean observed BAC, t (39) = 2.49, p = 0.02. The average degree of overestimation was 13.2 mg/dL (SD = 33.6)
Driver risk-taking (TTC)
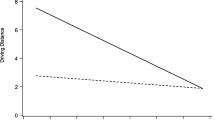
Alcohol reduced drivers’ TTC with other vehicles (i.e., riskier drivers). This was indicated by a one-way ANOVA of dose (placebo vs. alcohol), F (1, 39) = 5.96, p = 0.02, η 2 = 0.13. Figure 1 (left panel) shows that drivers’ TTC scores decreased under alcohol compared with placebo.

The figure plots the criterion measures for the test of driver risk-taking and driver skill. The left panel depicts the mean time to collision values (TTCs) from the test of driver risk-taking under placebo and alcohol. The right panel shows the mean deviation of lane position (LPSD) from the test of driver skill under placebo and alcohol. Capped vertical lines indicate the standard error of the mean
Although accidents were rare with less than a single accident per drive, they were statistically more frequent under alcohol, M = 0.83, SD = 0.90, compared with placebo, M = 0.40, SD = 0.74, F (1, 39) = 5.24, p = 0.03, η 2 = 0.12. Drivers traveled at comparable speeds following placebo, M = 48.03 mph, SD = 9.81, and alcohol, M = 48.91 mph, SD = 9.92, F (1, 39) = 0.47, p = 0.50.
Relation of drivers’ BAC estimation error to their risk-taking
Hierarchical regression analyses tested the degree to which BAC underestimation was associated with risky driving under alcohol independent of drivers’ observed BrAC. Drivers’ observed BrAC (step 1) and their error in BAC estimation (step 2) served as predictors in the model and were regressed onto the drivers’ TTC scores. The tolerance test indicated low multicollinearity between the predictors (tolerance = 0.88). Drivers’ BAC estimation errors, but not their observed BrACs, accounted for a significant amount (30 %) of the variance in drivers’ TTC scores, t (37) = 4.08, p < 0.01. The regression statistics are presented in Table 2. The positive slope relating BAC estimation error to TTC indicates that lower estimated BACs were associated with lower TTC scores (i.e., riskier driving).
Driving skill (LPSD)
Alcohol reduced driver’s ability to maintain their vehicle in the center of the lane, as indicated by a significant increase in LPSD under alcohol versus placebo, F (1, 39) = 20.30, p < 0.01, η 2 = 0.34 (Fig. 1, right panel).
More accidents were observed following alcohol, M = 1.95, SD = 4.18, compared with placebo, M = 0.48, SD = 1.04, F (1, 39) = 6.79, p = 0.01, η 2 = 0.15. Drivers’ speed did not significantly differ across dose conditions, F (1, 39) = 0.88, p = 0.36. Per instructions, drivers maintained an average speed of 54.67 mph (SD = 3.09).
Relation of drivers’ BAC estimation error to their skill
Neither BAC estimation errors nor observed BrACs significantly contributed to driving skill under alcohol. A hierarchical regression of BrAC (step 1) and error in BAC estimation (step 2) onto drivers’ LPSD obtained no significant effects ps > 0.11 (Table 2).
Relation of drivers’ BAC estimation to their subjective intoxication and drinking habits
Individuals perceived greater intoxication following alcohol (M = 61.79, SD = 22.5) than placebo (M = 11.57, SD = 14.98), and this difference was confirmed by a one-way ANOVA of dose, F (1, 39) = 140.19, p < 0.01, η 2 = 0.81. Pearson’s correlations showed that drivers’ BAC estimations under alcohol were not related to their level of subjective intoxication, p = 0.23, or to their drinking habits as measured by the TLFB and PDHQ, ps > 0.36.
BAC estimation and driving in the placebo condition
Individuals who estimated higher BACs following alcohol also tended to estimate higher BACs following placebo, as was indicated by a significant correlation of BAC estimations between the two dose conditions, r (39) = 0.34, p = 0.03.
Pearson’s correlations showed that drivers who estimated lower BACs after drinking the placebo also tended to be riskier drivers during the placebo session, r (39) = 0.44, p < 0.01, but their BAC estimates had no relationship to their driving skill (LPSD; r (39) = −0.16, p < 0.32).
Discussion
The present study provides new information on a potential determinant of driver risk-taking under alcohol. Those who displayed the greatest alcohol-induced increases in risky driving were also those who tended to estimate lower BACs. Reasons for the relationship are not known but could involve a failure to actively inhibit impulses to take risks under the drug. Laboratory measures show that alcohol impairs drivers’ ability to inhibit behavioral impulses and that more disinhibited drivers display greater risk-taking in simulated driving scenarios (Fillmore et al. 2008; Laude and Fillmore 2015). However, drinkers can also compensate for the disinhibiting effects of alcohol, effectively reducing the tendency for impulsive action, when they are aware of the potential for impairment (Fillmore et al. 1999; Marczinski and Fillmore 2005). It is possible that drivers in the current study who estimated higher BACs were more cognizant of the impairing effects of alcohol on their driving and as such, actively sought to resist risky driving by maintaining sufficient safety margins. By contrast, those who estimated lower BACs might have perceived little potential for impairment and thus failed to actively compensate for the disinhibiting effects of the drug on their risk-taking.
The study showed that alcohol impaired driving skill (LPSD) compared with placebo. However, drivers’ BAC estimation errors showed no relation to individual differences in their driving skill under the drug. Non-decision-based aspects of driving, such as the precision at maintaining one’s lane position, are considered largely automatic operations requiring little conscious awareness from the driver (Michon 1985; Salvucci 2006). As such, driving skill might not be influenced by the driver’s perceived BAC. By contrast, more volitional aspects of driving, such as risk-taking in which drivers make conscious decisions about whether or not to execute certain risky driving maneuvers, might be more apt to be influenced by the driver’s perceived level of impairment and estimated BAC. The finding that drivers’ beliefs about their BAC could specifically influence decision-based aspects of driving behavior is also consistent with evidence that BAC underestimation can contribute to the decision to drive after drinking (Beirness 1987). Indeed, the tendency to estimate lower BACs could support a series of high-risk decisions, regardless of one’s actual BAC.
Consistent with prior research (Beirness 1984, 1987), drinkers in the present study made errors when estimating their BAC. There is some evidence that BAC estimation is a product of interoceptive cues and behavioral changes associated with intoxication (Bois and Vogel-Sprott 1974; Lansky et al. 1978; Beirness 1984, 1987; Aston and Liguori 2013; Aston et al. 2013). The development of tolerance to subjective effects, often seen in heavy drinkers, could contribute to lower estimates of BAC. However, we found that BAC estimation errors bore no relation to drivers’ levels of subjective intoxication following alcohol nor were such errors related to individuals’ drinking habits. One possibility is that non-pharmacological factors contribute to self-estimations of BACs. Our study showed that subjects who estimated higher BACs following alcohol also tended to estimate higher BACs even after a placebo was administered. Basing one’s BAC estimations on the physical properties of the drinks could explain the consistency in subjects’ estimates across dose conditions. Participants might have been influenced by the taste and smell of the drinks and used that information to estimate their BACs, along with the number of glasses and volume of the beverage (all properties that were consistent across the alcohol and placebo sessions). It is also conceivable that the rating scale used to measure estimations of BACs contributed to this correlation. Individual differences in BAC estimations could also be due in part to different response styles of the subjects to such rating scales and thus represent a systematic source of method variance. Collectively, these findings suggest that the tendency to overestimate or underestimate one’s BAC might be determined by factors other than interoceptive cues of intoxication, drinking habits, and other pharmacological-based factors.
It is also noteworthy that drivers who estimated lower BACs following placebo tended to be riskier drivers in the placebo session. This suggests that the mere expectation of receiving alcohol could elicit risk-taking in certain drivers, which is a notion that has been raised by others (e.g., McMillen and Wells-Parker 1987; Burian et al. 2003). However, the current study was not designed to fully examine this account. Tests of the role of expectancies require manipulating the expectation of alcohol independent of its administration and an assessment of the specific types of effects drivers expect from alcohol on a variety of driving behaviors, including risk-taking.
It is also worthwhile to address some potential experimental factors that could have influenced the results. Evidence that drivers’ BAC estimations predicted our measure of driving risk but not driving skill could be due entirely to monetary incentives which were present in the risk drive but not in the skill drive. The skill drive tested lateral precision at a constant speed over the sustained driving period; we wanted to avoid any potential factors that could affect the drivers’ motivation. By contrast, the risk drive emphasized completing the course in the least time needed. Such a demand necessitates motivation by external rewards and in this case, the use of monetary incentives for quick completion of the drive. Further, incentives were included to model conditions under which risky driving is likely to occur. Outside of the laboratory, drivers engage in risk-taking because they are motivated to do so by some incentive or punisher (e.g., speed to avoid being late). Indeed, without any incentives present, simulated driving can be argued to be essentially risk-free as even vehicle crashes in the simulator present no risk of injury or harm to a subject. As such, models of risk-taking must incorporate some external reinforcers that can be acquired or lost based on driving behavior.
Task feedback during the drives could also influence drivers’ BAC estimations. For example, drivers who experienced a crash during a drive might view themselves as more intoxicated and thus estimate higher BACs. However, supplemental analyses tested the relationships between accidents in the simulator and drivers’ BAC estimations and did not yield support for the hypothesis that crashes might be associated with higher BAC estimations.
In conclusion, the findings of the present study demonstrate that drivers’ estimates of their BAC could serve as a useful predictive marker of who is likely to take risks behind the wheel while drinking and who is not. Although factors thought to contribute to DUI-related MVCs have been identified (Zador et al. 2000; Ryb et al. 2006; Hubicka et al. 2010), the distinct cognitive-behavioral mechanisms that function to increase risk-taking or impair skill are not well understood (but see Laude and Fillmore 2015), including those relevant to BAC estimation error. Future research should aim to identify mechanisms underlying these broader constructs while maintaining the fundamental distinction between drivers’ risk-taking and their skill level.
References
Aston ER, Liguori A (2013) Self-estimation of blood alcohol concentration: a review. Addict Behav 38:1944–1951
Aston ER, Neiberg RH, Liguori A (2013) Breath alcohol estimation training: behavioral effects and predictors of success. Alcohol Alcohol 48:396–401
Beirness DJ (1984) Self-estimates of blood alcohol concentration. Alcohol Drugs Driving 15:3–9
Beirness DJ (1987) Self-estimates of blood alcohol concentration in drinking-driving context. Drug Alcohol Depend 19:79–90
Bois C, Vogel-Sprott M (1974) Discrimination of low blood alcohol levels and self-titration skills in social drinkers. Q J Stud Alcohol 35(1 pt A):86–97
Burian SE, Hensberry R, Liguori A (2003) Differential effects of alcohol and alcohol expectancy on risk-taking during simulated driving. Hum Psychopharmacol Clin Exp 18:175–184
Fillmore MT (2001) Cognitive preoccupation with alcohol and binge drinking in college students: alcohol-induced priming of the motivation to drink. Psychol Addict Behav 15:325
Fillmore MT, Vogel-Sprott M (1998) Behavioral impairment under alcohol: cognitive and pharmacokinetic factors. Alcohol Clin Exp Res 22:1476–1482
Fillmore MT, Vogel-Sprott M, Gavrilescu D (1999) Alcohol effects on intentional behavior: dissociating controlled and automatic influences. Exp clin psychopharm 7:372–378
Fillmore MT, Blackburn JS, Harrison EL (2008) Acute disinhibiting effects of alcohol as a factor in risky driving behavior. Drug Alcohol Depend 95:97–106
Fromme K, Katz E, D’Amico E (1997) Effects of alcohol intoxication on the perceived consequences of risk taking. Exp Clin Psychopharmacol 5:14
Grant S, LaBrie JW, Hummer JF, Lac A (2012) How drunk am I? Misperceiving one’s level of intoxication in the college drinking environment. Psychol Addict Behav 26:51
Harrison EL, Fillmore MT (2005) Are bad drivers more impaired by alcohol?: sober driving precision predicts impairment from alcohol in a simulated driving task. Accid Anal Prev 37:882–889
Harrison EL, Marczinski CA, Fillmore MT (2007) Driver training conditions affect sensitivity to the impairing effects of alcohol on a simulated driving test to the impairing effects of alcohol on a simulated driving test. Exp Clin Psychopharmacol 15:588
Hubicka B, Källmén H, Hiltunen A, Bergman H (2010) Personality traits and mental health of severe drunk drivers in Sweden. Soc Psychiatry Psychiatr Epidemiol 45:723–731
Lansky D, Nathan PE, Lawson DM (1978) Blood alcohol level discrimination by alcoholics: the role of internal and external cues. J Consult Clin Psychol 46:953
Laude JR, Fillmore MT (2015) Simulated driving performance under alcohol: effects on driver-risk versus driver-skill. Drug Alcohol Depend 154:271–277
Linnoila M, Stapleton J, Lister R, Guthrie S, Eckardt M (1986) Effects of alcohol on accident risk. Pathologist 40:36–41
Marczinski CA, Fillmore MT (2005) Compensating for alcohol-induced impairment of control: effects on inhibition and activation of behavior. Psychopharmacology 181:337–346
Martin CS, Rose RJ, Obremski KM (1991) Estimation of blood alcohol concentrations in young male drinkers. Alcohol Clin Exp Res 15:494–499
McMillen D, Wells-Parker E (1987) The effect of alcohol consumption on risk-taking while driving. Addict Behav 12:241–247
Michon JA (1985) A critical view of driver behavior models: what do we know, what should we do? In: Evans L, Schwing RC (eds) Hum Beh Traffic Saf. Plenum Press, New York, pp 485–520
Moskowitz H, Fiorentino D (2000) A review of the literature on the effects of low doses of alcohol on driving-related skills. No. HS-809 028. U.S. Department of Transportation, National Highway Traffic Safety Administration, Washington, D.C
Nicholson ME, Wang M, Airhihenbuwa CO, Mahoney BS, Maney DW (1992) Predicting alcohol impairment: perceived intoxication versus BAC. Alcohol Clin Exp Res 16:747–750
Proestakis A, Espín AM, Exadaktylos F, Cortés Aguilar A, Oyediran OA, Palacio LA (2013) The separate effects of self-estimated and actual alcohol intoxication on risk taking: a field experiment. J Neurosci Psychol Econ 6:115
Quinn PD, Fromme K (2012) Event-level associations between objective and subjective alcohol intoxication and driving after drinking across the college years. Psychol Addict Behav 26:384
Ryb GE, Dischinger PC, Kufera JA, Read KM (2006) Risk perception and impulsivity: association with risky behaviors and substance abuse disorders. Accid Anal Prev 38:567–573
Salvucci DD (2006) Modeling driver behavior in a cognitive architecture. Hum Factors 48:362–380
Sobell LC, Sobell MBM (1992) Timeline followback: a technique for assessing self-reported alcohol consumption. In: Litten RZ, Allen J (eds) Measuring alcohol consumption: psychosocial and biological methods. Humana Press, New Jersey
Taieb-Maimon M, Shinar D (2001) Minimum and comfortable driving headways: reality versus perception. Hum Factors: J Hum Factors Ergon Soc 43:159–172
Verdejo-Garcia A, Clark L, Dunn BD (2012) The role of interoception in addiction: a critical review. Neurosci Biobehav Rev 36:1857–1869
Vogel-Sprott M (1992) Alcohol tolerance and social drinking: learning the consequences. Guilford Press, New York
Weafer J, Fillmore MT (2012) Acute tolerance to alcohol impairment of behavioral and cognitive mechanisms related to driving: drinking and driving on the descending limb. Psychopharmacology 220:697–706
Zador PL, Krawchuk SA, Voas RB (2000) Alcohol-related relative risk of driver fatalities and driver involvement in fatal crashes in relation to driver age and gender: an update using 1996 data. J Stud Alcohol 61:387–395
Zhang Y, Kaber DB (2013) An empirical assessment of driver motivation and emotional states in perceived safety margins under varied driving conditions. Ergonomics 56:256–267
Acknowledgments
This research was funded by NIAAA grants R01 AA021722 and F31 AA023694.The NIAAA had no further role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA or the National Institutes of Health. The experiment complies with the current laws of the USA in which they were performed.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The University of Kentucky Medical Institutional Review Board approved the study. All study volunteers provided informed consent and received $110 (plus money earned in the driver risk-taking test) for their participation.
Conflict of interest
All authors declare that they have no conflicts of interest. Authors have full control of all primary data and agree to allow the journal to review the data if requested.
Rights and permissions
About this article

Cite this article
Laude, J.R., Fillmore, M.T. Drivers who self-estimate lower blood alcohol concentrations are riskier drivers after drinking. Psychopharmacology 233, 1387–1394 (2016). https://doi.org/10.1007/s00213-016-4233-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-016-4233-x