
Abstract
Rationale
Minocycline has long been applied to various infectious diseases as a tetracycline antibiotic and recently has found new application in the treatment of brain diseases such as stroke and multiple sclerosis. In addition, minocycline has also been suggested as an effective drug for psychiatric diseases. These suggestions imply that minocycline may modulate our mental activities, while the underlying mechanism remains to be clarified.
Objective
To investigate how minocycline influences human mental activity, we experimentally examined how minocycline works on human social decision making in a double-blind randomized trial.
Methods
Forty-nine healthy volunteers were administered minocycline or placebo over four days, after which they played (1) a trust game, in which they decided how much to trust an anonymous partner, and (2) a dictator game, in which they decided how to divide resources between themselves and an anonymous partner.
Results
The minocycline group did not display increased trusting behavior or more altruistic resource allocation. In fact, the minocycline group displayed a slight reduction in trusting behavior. However, the minocycline group did show a strong positive correlation between the degree of risk taking in the trust game and in a separate evaluation of others' trustworthiness, whereas the placebo group showed no such correlation.
Conclusions
These results suggest that minocycline led to more rational decision-making strategies, possibly by increasing emotion regulation. Since minocycline is a well-known inhibitor of microglial activation, our findings may open a new optional pathway for treating mental states in which a component of rational decision making is impaired.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Minocycline is a tetracycline antibiotic and has long been applied to various infectious diseases. Recently, minocycline has been applied to brain diseases such as stroke and multiple sclerosis. In addition, minocycline has been suggested as an effective drug for psychiatric diseases (Levkovitz et al. 2009; Miyaoka 2008; Mizoguchi et al. 2008; Munzar et al. 2002). These reports imply that minocycline may modulate our social/mental activities while the underlying mechanism remains to be clarified.
Decision-making experiments have been proven to be one of the most reliable methods of measuring social/mental activities in humans. Using these decision-making experiments, recent neuro-economic research has shown that human mental activities are modulated by neurotransmitters such as oxytocin and serotonin (Crockett et al. 2008; Eisenegger et al. 2009; Kosfeld et al. 2005).
To our knowledge, only one study has investigated the effect of minocycline on social activities in healthy volunteers, which suggested that minocycline attenuates the subjective reward effects of dextroamphetamine and also speeds reaction times on a sustained attention task (Sofuoglu et al. 2011). This result may have been induced by improving distrustfulness of the participants. Therefore, this report implies that minocycline may promote prosocial behaviors such as trusting others because distrustfulness is one of the important psychiatric symptoms. As the initial step to clarify our hypothesis, we investigated the effects of minocycline on trust behaviors in a trust game among healthy adult volunteers.
Methods and materials
This double-blind randomized study was approved by the Kyushu University Ethical Committee under the administration of the UMIN clinical trial center (UMIN000003281). All participants gave written informed consent to participate after a complete description of the study. Participants were administered minocycline or placebo for four days, after which they made economic decisions in interpersonal situations. Participants also completed a general trust scale questionnaire at pre- and posttreatment.
Subjects
Participants were 49 Japanese males (mean age = 28.41 years, SD = 4.74 years) who were recruited by advertisements on campus. Inclusion criteria are as follows: healthy adult males from 20 to 39 years old who could give informed consent. Exclusion criteria are the following five items: (1) those who have ever had side effects due to antibiotics including minocycline; (2) those who have severe heart, liver, or kidney disease; (3) those who have a tendency to develop allergies; and (4) those who have ever been diagnosed with psychiatric disorders. Table S1 in the supplementary material shows the details of the participants. Their mental and physical health was confirmed by interview with psychiatrists (TAK and HH). All the participants were qualified for this study.
Drug administration
Participants received a sheet describing their detailed dosing schedule. They were then asked to write the exact time of every dosing and to submit every capsule package as the evidence of dosing. Participants started to take a capsule in the evening of the first day and then twice a day (morning and evening) for three days afterward. On the day of the game experiment (the fifth day), they were instructed to take the last capsule three-hour prior to the appointed time for the experiment so that they would play a trust game and a dictator game under the drug's effect. Each capsule contained 100 mg minocycline (in the treatment group) or 100 mg lactose (in the placebo group). This dose is within the range of the usual daily dose of minocycline used for the treatment of infections (Jonas and Cunha 1982). Participants were randomly assigned to the treatment group or to the placebo group in advance, with a double-blind procedure.
Procedure
Prior to drug administration, participants completed a set of questions including a general trust scale (Yamagishi and Yamagishi 1994). After four days of daily drug administration, participants were interviewed by physicians regarding side effects, other medications, and adherence to the drug administration protocol. They then played a trust game (Berg et al. 1995) and a dictator game (Forsythe et al. 1994). Each game was a two-person game, and each participant was ostensibly randomly paired with an anonymous male from another participant pool who had not taken the capsules. Participants' partners were actually research confederates. For each game, the participant's partner was always the same person, a Japanese male of 26 years old in the trust game and a Japanese male of 25 years old in the dictator game. Participants knew that they had a different partner for each game. In order to control the participant's impression of their partners, the partners acted and talked exactly the same way throughout all the experimental sessions. After playing the games, participants completed the same questionnaire as at pretreatment. Finally, participants were given a fixed reward for their participation, with additional rewards based on the results of the two games.
Trust and dictator games
Trust game
In this two-player game, each player was initially given 900 Japanese yen [JPY; about 10 US dollars (USD)]. The first player then decided how much of the 900 JPY to give to the second player. The second player then went to another room where the amount of money given to him by the first player was tripled. The second player then decided whether to return to the lab (and split his money equally with the first player) or not to return (and keep all of his money). Figure 1A describes the structure of the trust game. Participants were ostensibly assigned their roles as first or second players randomly.

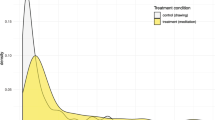
A Structure of the trust game. The first decision tree shows the extreme cases. B Amount of offer (in percent) in each game, *p = 0.051. C Correlation of general trust score and amount of offer in trust game in the control condition (left) and in the minocycline condition (right). In each graph of C, it appears 18 dots though N = 19 because there are two persons with an exactly same scores in each condition; placebo (4.67, 600) and minocycline (6.00, 900)
In the actual game, all the participants were assigned to be the first player. The first player's decision as to how much money to give to the second player depended on the first player's level of trust in his partner. The amount of money given was a behavioral measure of the first player's trustfulness. In this experiment, participants had no information about the partner except that he was male. The participants thus were likely to have made their decisions based primarily on how much they trusted others in general.
Dictator game
In this two-player game, the first player was given 1,300 JPY (about 15 USD) and unilaterally decided how to split the money between the players. The second player had no chance to take any action for or against the first player's decision. The first player's decision in this type of game is known to be a reliable indicator of altruism (Forsythe et al. 1994). Participants were ostensibly assigned their roles as first or second players randomly, but all the participants were actually assigned to be the first player. Because, again, the participants did not know anything about their partners other than their gender, the participants were likely to have made their decisions based primarily on how altruistic they were in general.
Trust scale
At pre- and posttreatment, participants completed a trust scale consisting of six questions answered on a seven-point Likert type scale. This scale measures respondents' estimation of others' human benevolence. A full description of the scale is available in (Yamagishi and Yamagishi 1994). The reliability and validity of this scale have been confirmed across many countries (Gheorghiu et al. 2009).
Results
Analysis
Prior to the analysis, we excluded the data of participants who did not meet the criteria for effective experimental manipulation. The criteria and the detailed dropout rate are shown in the Electronic supplementary material. Eleven participants were dropped out for analysis, resulting in 38 (19 for each condition) who were used for the further analysis. Since the dropout rate was 22.4%, we performed power analysis. The statistical power with given effect size d is 0.766 with our final subject sample. This is close to the commonly used efficient power of 0.8. The following analyses are shown with this sample. All of the analyses were performed with SPSS version 18 and 19.
Behavior in trust game and dictator game
We compared the mean amount of participants' monetary offers in each game by a t test. Figure 1B shows the ratio of money given in each game. In the trust game, the amount of money given by the participants was marginally lower in the minocycline group than in the placebo group (t(30) = 2.03, p = 0.051). The confidence interval (95%) was 0.13 to 378.82. In the dictator game, there was no difference in generosity between the minocycline group and the placebo group (t(36) = 0.51, ns). The confidence interval (95%) was −240.55 to 284.76. Combining the results of the two games, we concluded that minocycline did not generally promote prosocial behaviors among our participants.
General Trust Scale scores
According to the past research on the General Trust Scale, the major confounders of General Trust are culture, sex, and education level (e.g., Yamagishi and Yamagishi 1994). To eliminate these confounders' effects, we tried to recruit a homogeneous sample on sex and education level. As a result, all the participants were Japanese male and had a college/university level education so that we could test the effect of General Trust without these confounders.
We performed ANOVA with a repeated measure to examine the change of participants' trust level. Drug condition (minocycline vs. control), repeated measure of trust score (before vs. after treatment), and their interaction were the independent variables, while the General Trust Score was the dependent variable. The results showed that there is no significant difference in all the possible effects. The mean scores and statistical values in each effect is the following: drug condition (minocycline, 4.29 vs. control, 4.73; F(1, 36) = 2.16, ns), repeated measure of trust score (before, 4.43 vs. after, 4.58; F(1, 36) = 2.38, ns), and their interaction (minocycline before 4.15, minocycline after 4.42, control before 4.72, control after 4.75; F(1, 36) = 1.62, ns). According to these results, we conclude that minocycline did not increase our participants' general sense of trust in others.
Differences in decision-making style between conditions
Although minocycline itself does not appear to promote trust or altruistic behavior, minocycline may have effects on the ways participants made decisions. We performed a multiple linear regression analysis to explore this possibility with the amount of money offered in trust game as the dependent variable and with experimental condition, trust scale score, and their interaction as independent variables. For the prediction of offer amounts in the trust game, the best fitting model was the full model just described (R 2 = 0.424, F(3,34) = 8.33, p < 0.001). The main effect of condition was significant (β = −2.17, t = −3.37, p < 0.01); the main effect of the trust scale score was marginally significant (β = −0.87, t = −1.94, p < 0.10), and the interaction term was also significant (β = 2.14, t = −3.01, p < 0.01). The most prominent effect was the interaction term. We interpreted this as meaning that participants' general trust in others had differing effects on offer amounts in the trust game depending on whether the participant was administered minocycline or a placebo. None of the candidate models predicted participants' offers in the dictator game.
Since the interaction term was significant in the trust game, we also correlated the trust scale score and the amount of money offered in the trust game in each experimental condition. The results show a strong positive correlation for the minocycline group (r = 0.702, p < 0.001) and no correlation for the placebo group (r = −0.039, ns.; Fig. 1C). We should note that in Fig. 1C, 17 participants (10 for placebo group) offered the maximum amount in the trust game, and this may be ceiling effect. It is also notable that, despite the possible ceiling effect, the minocycline condition still shows a strong positive correlation while the control condition does not.
Discussion
This study reveals that (1) minocycline slightly reduces trusting behavior and (2) in the minocycline condition (but not in the placebo condition), the more participants trusted others generally, the more they displayed trusting behavior. In the trust game, with an anonymous partner, participants in the minocycline condition made their decisions based primarily on how much they trusted people in general, whereas participants in the control condition appeared not to do so. Our interpretation is that participants in the control condition attended more to their uncertainties regarding their anonymous partners and/or to their fears of being exploited in what was fundamentally a risky situation, than to their general trust for others, whereas participants in the minocycline condition took a more rational strategy, attending to the lack of information about the partner rather than to their fears about that lack of information. The results of the experiment suggest that minocycline can relatively increase participants' attention on the appropriate cues in their current social interaction resulting in that participants made decisions along with the their general trust.
How can minocycline have the above effects? Minocycline is known to work in the brain by inhibiting activation of microglia, a type of glial cell with immunological functions. Therefore, the effects of minocycline in our decision-making experiment may be explained by microglia.
When activated, microglia release cytokines, free radicals, and neurotransmitters, which contribute to homeostasis and brain pathologies such as neurodegenerative disorders and neuropathic pain (Block et al. 2007; Hanisch and Kettenmann 2007). Studies of microglial contributions to psychiatric disorders have only recently begun (Monji et al. 2009). Recent PET imaging studies report that microglial activation has appeared in the brains of acute phase patients with schizophrenia (Doorduin et al. 2009; Takano et al. 2010; van Berckel et al. 2008), methamphetamine users (Sekine et al. 2008), alcoholics (He and Crews 2008; Wu et al. 2011), and suicide patients (Steiner et al. 2006, 2008). Emotional dysregulation is often a factor in various psychiatric illnesses, including suicide (Mann et al. 2005). Schizophrenia patients and methamphetamine users have been treated with minocycline (Levkovitz et al. 2009; Miyaoka 2008; Tanibuchi et al. 2010). Furthermore, one study has investigated the effect of minocycline on social activities in healthy volunteers and has suggested that minocycline attenuates the subjective reward effects of dextroamphetamine (Sofuoglu et al. 2011). These reports suggest that minocycline improves psychiatric symptoms and promotes prosocial behaviors by modulating microglial activation. Past neuro-economics research has shown that human social decision making is modulated by neurotransmitters such as oxytocin and serotonin in the context of neuronal networks, while microglia have recently been receiving increased attention by researchers (Graeber and Streit 2010; Miller 2005; Yirmiya and Goshen 2011). Recent findings have suggested that microglia monitor microenvironmental changes including synapses in the brain (Graeber 2010; Wake et al. 2009). Previously, no PET study has reported microglial activation in healthy persons, while these findings imply that microglia may perform actively not only in the pathological brain but also in the brain of healthy persons. The interrelationship between microglia and minocycline has not been clarified from the present study; while summing up above-mentioned previous reports, we hypothesize that microglia may be activated during the process of decision making in healthy persons, and our results suggest that inhibiting microglial activation with minocycline may lead to a more rational approach to decision making and promote prosocial behaviors by modulating neurosynaptic–microglial networks.
Recent animal studies have reported that stressors such as physical pain and isolation may induce microglial activation (Frank et al. 2007; Schiavone et al. 2009; Sugama et al. 2009). Another animal study indicated that microglial activation causes anxiety, which in turn can be decreased by minocycline treatment (Neigh et al. 2009). These reports imply that the risks inherent in the trust game may have induced anxiety in the participants, which in turn may have been reduced by inhibiting microglial activation in the minocycline group.
Adding the above discussion, we should mention another possibility. Participants' perception of the games in experiment might differ between conditions. It has been argued that subjective reward in social interaction can change depending on whether the given situation is perceived as competitive or cooperative (Lee 2008). Sofuoglu et al. (2011) report that minocycline attenuates subjective rewarding. Thus, it is possible that participants in the minocycline group attenuated reward and induced a more competitive perception in the trust game, resulting in smaller offer than those in the control group. If so, participants in the minocycline group would give a smaller amount of money in the dictator game as well. However, the data of our study show no difference for the amount of money in the dictator game between the conditions. It is necessary to conduct further research to explore this possibility.
Conclusion
Given that minocycline controls microglial activation, we hypothesize that activation of microglia may modulate emotion regulation and that microglial inhibition by minocycline causes increased emotion regulation, leading to more rational decision making. The present study did not measure participants' anxiety, and we are unable to draw concrete conclusions about how anxiety may have influenced participants' decision making. These relationships should be investigated in future research.
While the results of our study led us to some intriguing conclusions, this study has a number of limitations. First, the small sample size and ceiling effect in our experiment may have affected the results we obtained. Second, this study did not examine the dose-dependent effects of minocycline since only 200 mg/day dose was used. Third, the external validity is limited to interaction between men. It should be noted that since the first player was always informed that the second player was a male, our results should be regarded in caution; the results may have been altered if one or both players were female. Further studies are needed to clarify the sex differences. Finally, we should consider another direction of minocycline effect not limited to our microglia hypothesis. Minocycline also has been reported to have other CNS effects, such as interacting with brain glutamate and dopamine neurotransmission. Furthermore, one recent in vitro study showed that minocycline potentiates the neurite outgrowth in neuronal cells (PC12), suggesting another effect of minocycline on neuronal plasticity (Hashimoto and Ishima 2010). It remains to be clarified whether not only microglial modulation but also these other CNS effects could have been involved in the trust-related behavioral effects we observed. Further research should be performed to clarify this molecular mechanism.
We put forward a novel hypothesis that microglia may interact directly with mental activities such as trust. Our experiment may shed new light on the underlying mechanism of action of microglia on mental activities. Further research is needed to clarify our preliminary findings.
References
Berg J, Dickhaut J, McCabe K (1995) Trust, reciprocity, and social history. Game Econ Behav 10:122–142
Block ML, Zecca L, Hong JS (2007) Microglia-mediated neurotoxicity: uncovering the molecular mechanisms. Nat Rev Neurosci 8:57–69
Crockett MJ, Clark L, Tabibnia G, Lieberman MD, Robbins TW (2008) Serotonin modulates behavioral reactions to unfairness. Science 320(5884):1739
Doorduin J, de Vries EF, Willemsen AT, de Groot JC, Dierckx RA, Klein HC (2009) Neuroinflammation in schizophrenia-related psychosis: a PET study. J Nucl Med 50:1801–1807
Eisenegger C, Naef M, Snozzi R, Heinrichs M, Fehr E (2009) Prejudice and truth about the effect of testosterone on human bargaining behaviour. Nature 463:356–359
Forsythe R, Horowitz J, Savin N, Sefton M (1994) Fairness in simple bargaining experiments. Game Econ Behav 6:347–369
Frank MG, Baratta MV, Sprunger DB, Watkins LR, Maier SF (2007) Microglia serve as a neuroimmune substrate for stress-induced potentiation of CNS pro-inflammatory cytokine responses. Brain Behav Immun 21:47–59
Gheorghiu MA, Vignoles VL, Smith PB (2009) Beyond the United States and Japan: testing Yamagishi's emancipation theory of trust across 31 nations. Soc Psychol Q 72:365–383
Graeber MB (2010) Changing face of microglia. Science 330:783–788
Graeber MB, Streit WJ (2010) Microglia: biology and pathology. Acta Neuropathol 119:89–105
Hanisch UK, Kettenmann H (2007) Microglia: active sensor and versatile effector cells in the normal and pathologic brain. Nat Neurosci 10:1387–1394
Hashimoto K, Ishima T (2010) A novel target of action of minocycline in NGF-induced neurite outgrowth in PC12 cells: translation initiation [corrected] factor eIF4AI. PLoS One 5:e15430
He J, Crews FT (2008) Increased MCP-1 and microglia in various regions of the human alcoholic brain. Exp Neurol 210:349–358
Jonas M, Cunha BA (1982) Minocycline. Ther Drug Monit 4:137–145
Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E (2005) Oxytocin increases trust in humans. Nature 435(7042):673–676
Lee D (2008) Game theory and neural basis of social decision making. Nat Neurosci 11:404–409
Levkovitz Y, Mendlovich S, Riwkes S, Braw Y, Levkovitch-Verbin H, Gal G, Fennig S, Treves I, Kron S (2009) A double-blind, randomized study of minocycline for the treatment of negative and cognitive symptoms in early-phase schizophrenia. J Clin Psychiatry 71(2):138–149
Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, Hegerl U, Lonnqvist J, Malone K, Marusic A, Mehlum L, Patton G, Phillips M, Rutz W, Rihmer Z, Schmidtke A, Shaffer D, Silverman M, Takahashi Y, Varnik A, Wasserman D, Yip P, Hendin H (2005) Suicide prevention strategies: a systematic review. JAMA 294:2064–2074
Miller G (2005) Neuroscience. The dark side of glia. Science 308(5723):778–781
Miyaoka T (2008) Clinical potential of minocycline for schizophrenia. CNS Neurol Disord Drug Targets 7:376–381
Mizoguchi H, Takuma K, Fukakusa A, Ito Y, Nakatani A, Ibi D, Kim HC, Yamada K (2008) Improvement by minocycline of methamphetamine-induced impairment of recognition memory in mice. Psychopharmacology 196:233–241
Monji A, Kato T, Kanba S (2009) Cytokines and schizophrenia: microglia hypothesis of schizophrenia. Psychiatry Clin Neurosci 63:257–265
Munzar P, Li H, Nicholson KL, Wiley JL, Balster RL (2002) Enhancement of the discriminative stimulus effects of phencyclidine by the tetracycline antibiotics doxycycline and minocycline in rats. Psychopharmacology 160:331–336
Neigh GN, Karelina K, Glasper ER, Bowers SL, Zhang N, Popovich PG, DeVries AC (2009) Anxiety after cardiac arrest/cardiopulmonary resuscitation: exacerbated by stress and prevented by minocycline. Stroke 40:3601–3607
Schiavone S, Sorce S, Dubois-Dauphin M, Jaquet V, Colaianna M, Zotti M, Cuomo V, Trabace L, Krause KH (2009) Involvement of NOX2 in the development of behavioral and pathologic alterations in isolated rats. Biol Psychiatry 66:384–392
Sekine Y, Ouchi Y, Sugihara G, Takei N, Yoshikawa E, Nakamura K, Iwata Y, Tsuchiya KJ, Suda S, Suzuki K, Kawai M, Takebayashi K, Yamamoto S, Matsuzaki H, Ueki T, Mori N, Gold MS, Cadet JL (2008) Methamphetamine causes microglial activation in the brains of human abusers. J Neurosci 28:5756–5761
Sofuoglu M, Mooney M, Kosten T, Waters A, Hashimoto K (2011) Minocycline attenuates subjective rewarding effects of dextroamphetamine in humans. Psychopharmacology 213:61–68
Steiner J, Mawrin C, Ziegeler A, Bielau H, Ullrich O, Bernstein HG, Bogerts B (2006) Distribution of HLA-DR-positive microglia in schizophrenia reflects impaired cerebral lateralization. Acta Neuropathol 112:305–316
Steiner J, Bielau H, Brisch R, Danos P, Ullrich O, Mawrin C, Bernstein HG, Bogerts B (2008) Immunological aspects in the neurobiology of suicide: elevated microglial density in schizophrenia and depression is associated with suicide. J Psychiatr Res 42:151–157
Sugama S, Takenouchi T, Fujita M, Conti B, Hashimoto M (2009) Differential microglial activation between acute stress and lipopolysaccharide treatment. J Neuroimmunol 207:24–31
Takano A, Arakawa R, Ito H, Tateno A, Takahashi H, Matsumoto R, Okubo Y, Suhara T (2010) Peripheral benzodiazepine receptors in patients with chronic schizophrenia: a PET study with [11C]DAA1106. Int J Neuropsychopharmacol 13:943–950
Tanibuchi Y, Shimagami M, Fukami G, Sekine Y, Iyo M, Hashimoto K (2010) A case of methamphetamine use disorder treated with the antibiotic drug minocycline. Gen Hosp Psychiatry 32(559):e1–e3
van Berckel BN, Bossong MG, Boellaard R, Kloet R, Schuitemaker A, Caspers E, Luurtsema G, Windhorst AD, Cahn W, Lammertsma AA, Kahn RS (2008) Microglia activation in recent-onset schizophrenia: a quantitative (R)-[11C]PK11195 positron emission tomography study. Biol Psychiatry 64:820–822
Wake H, Moorhouse AJ, Jinno S, Kohsaka S, Nabekura J (2009) Resting microglia directly monitor the functional state of synapses in vivo and determine the fate of ischemic terminals. J Neurosci 29:3974–3980
Wu Y, Lousberg EL, Moldenhauer LM, Hayball JD, Robertson SA, Coller JK, Watkins LR, Somogyi AA, Hutchinson MR (2011) Attenuation of microglial and IL-1 signaling protects mice from acute alcohol-induced sedation and/or motor impairment. Brain Behav Immun 25(Suppl1):S155–S164
Yamagishi T, Yamagishi M (1994) Trust and commitment in the United States and Japan. Motiv Emot 18:9–66
Yirmiya R, Goshen I (2011) Immune modulation of learning, memory, neural plasticity and neurogenesis. Brain Behav Immun 25:181–213
Acknowledgments
This work was financially supported by the Grant-in-Aid from JSPS to Motoki Watabe, Takahiro A. Kato, Akira Monji, and Shigenobu Kanba. We thank to Prof. Kazuhide Hashiya and Mr. Katsuhiko Ishikawa (Graduate School of Human-Environment Studies, Kyushu University) for their technical supports.
Conflict of interest
All authors declare that they have no financial conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Motoki Watabe and Takahiro A. Kato contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
DOC 35 kb
Rights and permissions
About this article
Cite this article
Watabe, M., Kato, T.A., Monji, A. et al. Does minocycline, an antibiotic with inhibitory effects on microglial activation, sharpen a sense of trust in social interaction?. Psychopharmacology 220, 551–557 (2012). https://doi.org/10.1007/s00213-011-2509-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-011-2509-8