
Abstract
Rationale
Caffeine typically produces positive effects on mood and performance. However, tolerance may develop following habitual use, and abrupt cessation can result in withdrawal symptoms, such as fatigue. This study investigated whether caffeine has a greater stimulant effect in a withdrawn state compared to a normal caffeinated state, among moderate daily caffeine consumers.
Materials and methods
Using a within-subjects design, 17 caffeine consumers (mean ± sd = 375 ± 101 mg/day) ingested placebo or caffeine (250 mg) following 30-h of caffeine abstention or normal dietary caffeine use on four separate days. Self-reported mood and performance on choice reaction time, selective attention, and memory tasks were measured.
Results
Caffeine had a greater effect on mood and choice reaction time in the abstained state than in the normal caffeinated state, but caffeine improved selective attention and memory in both states.
Conclusions
Although improvements in mood and reaction time may best explained as relief from withdrawal symptoms, other performance measures showed no evidence of withdrawal and were equally sensitive to an acute dose of caffeine in the normal caffeinated state.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
At normal dietary concentrations, caffeine produces a mild neurostimulant effect by antagonizing adenosine, thus disinhibiting neuronal firing throughout the brain (for review, see Nehlig 1999; Ferre 2008). Acute caffeine administration typically improves mood (e.g., self-reported alertness and energy) and visual-motor performance (i.e., simple reaction time; Fine et al. 1994; Warburton 1995; Robelin and Rogers 1998; Haskell et al. 2005; Childs and de Wit 2006). However, the effect of caffeine on more cognitively demanding tasks varies; some studies have shown improvements in vigilance, selective attention, and memory (Lieberman et al. 1987; James 1998; Heatherley et al. 2005), while other studies have found no effect (Loke and Meliska 1984; Lorist and Snel 1997; Rogers and Dernoncourt 1998).
Daily caffeine use has been shown to diminish the stimulant effects of an acute dose of caffeine; for instance, in rodents, the development of tolerance has been demonstrated to the locomotor stimulant effects of caffeine following chronic administration of doses ranging between 5 mg/kg/day to 65 mg/kg/day (Chou et al. 1985; Finn and Holtzman 1986). Analogously, tolerance has also been shown to the subjective stimulant and anxiogenic side effects (e.g., jitteriness) of caffeine after subjects were maintained on 900 mg/day (Evans and Griffiths 1992). Upregulation of adenosine receptors after chronic caffeine exposure may be the mechanism of tolerance (Johansson et al. 1997; Shi and Daly 1999; Varani et al. 1999), although sensitization and other changes have been identified as well (Green and Stiles 1986; Powell et al. 2001). Conversely, there is also evidence against the development of tolerance to increased brain energy metabolism following an acute dose of caffeine in rats chronically treated with 10 mg/kg/day of caffeine (Nehlig et al. 1986).
Caffeine has a half-life of approximately 4 to 8 h (Patwardhan et al. 1980). Withdrawal symptoms typically begin following overnight abstinence, and peak between 20 to 51 h (Juliano and Griffiths 2004). Symptoms may occur after only 3 days of use (Evans and Griffiths 1999) and from doses as low as 100 mg/day (Griffiths et al. 1990). Headaches are the most commonly reported symptom of caffeine withdrawal, followed by decreased alertness and increased fatigue (Juliano and Griffiths 2004).
Given the development of tolerance, some investigators have proposed that among daily users, caffeine primarily restores mood and performance that have been degraded by withdrawal (James 1994; James and Rogers 2005). In support of this, several studies have shown an initial, but not an accumulative, effect of caffeine on mood and performance following overnight abstinence (Robelin and Rogers 1998; Yeomans et al. 2002). Hypothetically, physiological caffeine concentrations must fall below a certain threshold before mood and performance can be affected by caffeine again (James and Rogers 2005). Alternatively, there is evidence that an acute dose of caffeine can improve mood and performance in caffeine users who were allowed caffeine ad libitum prior to the study (Frewer and Lader 1991; Warburton et al. 2001; Christopher et al. 2005; Smith et al. 2005), and some have reported a dose-dependent relationship (Frewer and Lader 1991; Smith et al. 2005). This suggests that caffeine can produce a significant amount of stimulation beyond the alleviation of withdrawal symptoms.
Previous studies that have administered an acute dose of caffeine in a normal caffeinated state have not included a withdrawn state for comparison (Frewer and Lader 1991; Warburton et al. 2001; Christopher et al. 2005; Smith et al. 2005). A comparison of these two states would answer the question that is pertinent to the majority of daily caffeine consumers: are there benefits to drinking more than one's average daily dose of caffeine? The present study investigates whether caffeine can enhance cognition and mood when administered to subjects in their normal caffeinated state, in contrast with the administration of caffeine after 30 h of caffeine abstinence. We hypothesized that a dose of caffeine given on top of normal caffeine consumption would have less of an effect than when given following a period of abstinence. In addition, we hypothesized that caffeine would be most effective on measures of mood and reaction time, than on measures of selective attention and memory.
Methods
Participants
Habitual caffeine consumers (ages 18–50) who drink between two–five cups of coffee per day were recruited from the Winston-Salem, North Carolina community by flyers and word of mouth. Potential volunteers were initially screened over the phone. Participants were prescreened to ensure they would experience symptoms of withdrawal (Hughes et al. 1993). They were asked if they would feel more tired than usual or have a headache if they went a day or two without caffeine, and had to answer affirmatively to be eligible. Potential volunteers also completed a screening visit which consisted of vital signs, a medical history, a depression and alcohol-use questionnaire, and a urinalysis of illicit drug use by enzyme multiplied immunoassay testing (Rubenstein et al. 1972). Following the screening visit, daily caffeine use was recorded prospectively across seven consecutive days using a modified caffeine consumption diary (Landrum 1992; Addicott et al. 2009). In this diary, participants documented the quantity and number of items consumed from a list of caffeinated beverages, foods, and medications into 6-h time bins. Caffeine use was quantified using standard caffeine content values (Center for Science in the Public Interest; www.cspinet.org). Healthy individuals who consumed between 200–600 mg/day and had a negative drug screen were included in the study. Exclusion criteria included abuse of alcohol or other drugs, a history of neurological disorders, visual acuity that could not be corrected to 20/40, and symptoms of depression or anxiety. The Institutional Review Board of Wake Forest University School of Medicine approved this study. Participants gave written informed consent prior to entering the study and were financially compensated for their time.
Seventeen participants completed the study (eight men); there were 14 Caucasians, one Asian, one African-American, and one Hispanic. The average (± standard deviation) age was 30 ± 8 years, weight was 74 ± 15 kg, and education level was 17 ± 3 years. The estimated caffeine intake from the 7-day diary was 375 ± 101 mg/day (5.5 ± 2.5 mg/kg/day). Three women reported using oral birth control, and two participants reported using cigarettes.
Measures
Salivary caffeine concentrations were monitored to verify compliance with the study requirements. Samples were collected with Salivette® cotton swabs (Sarstedt, Newton, NC, USA). Participants were instructed not to eat, drink, or brush their teeth for 15 min before the saliva sample was obtained. After rinsing their mouths with water, participants chewed on the cotton swab for 45 sec. Samples were centrifuged and frozen at −70˚C until assayed using high-performance liquid chromatography (Deroche et al. 1990; Holland et al. 1998; Global Lifescience Solutions, LLC, Ann Arbor, MI, USA). The minimum detection threshold was 0.02 µg/ml and concentrations below this threshold were recorded as zero.
Mood was assessed using a self-report form. The symptoms selected for the self-report form were drawn from Juliano and Griffiths' (2004) review of caffeine withdrawal symptoms as well as from empirical studies (Warburton 1995; Rogers et al. 2003). The self-report form consisted of six positive mood symptoms (alert, able to concentrate, energetic, talkative, cheerful/happy, and friendly), six negative symptoms (tired, drowsy/sleepy, depressed, headache, lazy/sluggish, and light-headed), and four symptoms classified as side effects (jittery, anxious/nervous, tense, pounding heartbeat). The side effects have previously been reported to be associated with the ingestion of high doses of caffeine (Richardson et al. 1995; Childs and de Wit 2006). Participants rated the extent to which they were currently experiencing each mood symptom on a scale from 1 (“not at all”) to 5 (“extremely”). The main dependent variables were the average mood score consisting of both the positive and negative symptoms, and the average side effects score. Negative mood scores were inverted (scores of 1 and 2 were changed to scores of 5 and 4, and vice versa) so that increases in the average mood score indicate improvements in mood. In addition, changes in individual mood items were analyzed using the original scores.
The stimulus for the choice reaction time task consisted of a black and white checkerboard with a single red square appearing randomly in one of the four quadrants. This task was presented using visual display goggles (Resonance Technology, Inc. Los Angeles, CA, USA) and participants responded using a response box with their right hand. Participants were instructed to make a response indicating whether the red square was on the right or left half of the checkerboard (i.e., press the left button if the red square is on the left side, and the right button if it is on the right side). The checkerboard was presented 156 times with durations of 250 ms. The interstimulus interval averaged 3.7 ± 2.7 sec and ranged 1.5–11.9 sec. The dependent variables were average reaction time and accuracy (number correct/number possible).
A modified version of the Eriksen flanker task (Eriksen and Eriksen 1974; Posthuma et al. 2002) was used to assess selective attention. Five arrows were presented in each trial. In congruent trials, all arrows faced the same direction (i.e., < < < < <), and in incongruent trials, the center arrow faced the opposite direction of the flanking arrows (i.e., < < > < <). This task was also presented using visual display goggles. Participants were instructed to make a response indicating the direction of the center arrow (i.e., press the left button if the center arrow faces left, and the right button if it faces right) and to ignore the flanking arrows. There were 80 trials total, with an equal number of congruent and incongruent trials presented randomly. Each presentation had a duration of 500 msec, and the interstimulus interval averaged 2.3 ± 0.7 sec and ranged 1.0–3.9 sec. The dependent variables were average reaction time, accuracy, and the interference effect (average incongruent trial reaction time–average congruent trial reaction time).
Memory was measured with an n-back letter task. In separate tasks, capital letters appeared on a screen one at a time and participants indicated whether the letter displayed was identical or different than the letter 1-letter or 2-letters preceding it. Completion of the 1-back task always preceded the 2-back task. Participants performed the memory tasks alone in a quiet room using a laptop computer. Each task consisted of 51 trials. Letters remained displayed for 250 msec, and the average interstimulus interval was a maximum of 2.4 sec and ranged 0.6–2.4 sec. The dependent variables were accuracy, the difference in accuracy (1-back task–2-back task), and average reaction time.
Procedure
This study utilized a within-subject design; caffeine administration was double-blind and placebo-controlled. Each participant had four study visits, separated by at least 1 week. For two of the visits, participants were told to “use caffeine like they normally do” prior to arrival at the laboratory; these visits constituted the “normal” state. For the other two visits, participants were instructed to abstain from caffeine for 30 h prior to arrival at the laboratory; these visits constituted the “abstained” state. Participants were asked to abstain from caffeine for 30 h to capture potential withdrawal symptoms in their peak range (Juliano and Griffiths 2004). In each state, participants were administered a caffeine capsule (250 mg, anhydrous) and a matching placebo capsule (lactose) on separate visits. Participants were instructed that in each state (withdrawn and native caffeinated) they would participate in two drug conditions on different days, one day would be caffeine and one day would be placebo. They were explicitly told “you will be given a capsule which will contain either caffeine or placebo but you will not be told what you are taking.” Abbreviations for the state by drug conditions used in the remainder of the manuscript are: abstained caffeine (AC), abstained placebo (AP), normal caffeine (NC), and normal placebo (NP). Capsules were prepared by the Wake Forest University Baptist Hospital pharmacy. Seventeen state by drug condition sequences were chosen randomly from 24 possible sequences.
Study visits were conducted between 7 a. m. and 4 p. m. Participants kept a 3-day caffeine consumption diary which was inclusive of the study day. Upon arrival to the laboratory, a saliva sample was obtained to measure caffeine concentrations, and the 3-day caffeine diary was collected. Participants were asked if they had experienced a headache either that day or the day before. The first mood report was filled-out, and then the capsule was administered. Participants were allowed to relax for the next 45 min, and were instructed not to consume food or beverages other than water for the duration of the experiment. Then, a second saliva sample was obtained, and a second mood report was completed. Participants were familiarized with the computer tasks and had a brief practice session for each task at every study visit. The choice reaction time and selective attention tasks were conducted in a magnetic resonance scanner as part of a functional imaging study. Computer tasks were programmed with E-Prime 1.0 (Psychology Software Tools, Pittsburgh, PA, USA) and were completed within 1 h after the second saliva sample. Participants had all four visits either in the morning or in the afternoon, with four random exceptions due to scheduling conflicts.
Data Analysis
The average score and individual items of self-reported mood and salivary caffeine concentrations were analyzed with separate 2 (state) × 2 (drug) × 2 (time) repeated-measures analysis of variance (ANOVA). One mood symptom item was not reported by one subject, and the average mood was calculated without that item. Choice reaction time was analyzed with a 2 (state) × 2 (drug) repeated-measures ANOVA. The flanker and memory tasks were analyzed separately with 2 (state) × 2 (drug) × 2 (task type) repeated-measures ANOVAs. Significant main effects were further analyzed with paired samples t tests. Caffeine-use diaries and salivary-caffeine concentrations were correlated using Pearson product-moment correlations. Results were significant if p < 0.05. Data were analyzed with SPSS 16.0 (Chicago, IL, USA). Computer task results were cleaned of responses ± 3 standard deviations from each individual's mean reaction time, and reaction times less than 50 msec were recorded as nonresponses. Incorrect responses were included in the mean reaction time.
Results
The 3-day caffeine-use diaries and salivary caffeine concentrations confirmed the participants’ compliance with the study procedure. None of the participants reported using caffeine in the 30 h prior to the abstained state visits. Participants reported consuming an average of 229 ± 123 mg the day of the normal state visits. The average precapsule salivary caffeine concentration was 0.2 ± 0.2 µg/ml in the abstained state, and was 2.7 ± 2.6 µg/ml in the normal state. Caffeine administration increased concentrations by an average of 3.2 ± 1.3 µg/ml (drug × time interaction: F (1, 16) = 97.6; p < 0.001); this resulted in higher caffeine concentrations in the NC condition (6.1 ± 2.7 µg/ml) than in the AC condition (2.9 ± 2.0 µg/ml; t test: t (16) = 5.2; p < 0.001). Concentrations were similar between the AC condition (2.9 ± 2.0 µg/ml) and the NP condition (2.5 ± 2.7 µg/ml). In the normal state, the average reported caffeine consumption from the study days correlated with the average precapsule salivary caffeine concentrations (r = 0.64; p < 0.01) and also correlated with the average caffeine use reported in the 7-day diary (r = 0.75; p < 0.005).
Participants reported headaches on 26 occasions (76% of the time) during the two abstained state days, and on three occasions (9% of the time) during the normal state days (state: F (1, 16) = 63.2; p < 0.001). Only one participant denied experiencing a headache on either day in the abstained state.
Individual mood items that produced significant state, drug × time, and state × drug × time interaction effects are shown in Table 1. In summary, the average mood score was greater in the normal state than in the abstained state (state: F (1, 16) = 44.8; p < 0.001); see Fig. 1. All of the individual positive and negative mood symptoms exhibited this state effect except for talkative and depressed. Average mood decreased from the pre- to the postmeasure in the placebo conditions (drug × time: F (1, 16) = 11.2; p < 0.005; AP pre- to postmeasure: t (16) = 2.0; p = 0.058; NP pre- to postmeasure: t (16) = 3.5; p < 0.005); this drug × time effect was significant for energetic, talkative, headache, drowsy, and tired. Lastly, caffeine increased average mood only in the AC condition (state × drug × time: F (1, 16) = 5.1; p < 0.05; AC pre- to postmeasure: t (16) = 3.1; p < 0.01); this effect was significant for tiredness although there were trends for talkative and headache. Caffeine increased the average side effect score in both the normal and abstained states (drug × time: F (1, 16) = 6.1; p < 0.05), this effect was significant for pounding heartbeat and jittery. Follow-up comparisons between average pre- and postcapsule side effects were marginally significant (AC: t (16) = 1.9; p = 0.08; NC: t (16) = 1.9; p = 0.07).

Average self-reported mood scores pre- and postcapsule administration. Mood scores were higher in the normal state than in the abstained state, and caffeine increased mood in the abstained state only. Mood decreased following placebo in the normal state (paired t test pre- to postcapsule: *p < 0.01). Bars are SEM
Caffeine reduced choice reaction time in the abstained state, but not in the normal state (state × drug: F (1, 16) = 7.7; p < 0.05; t test AP to AC: t (16) = 3.2; p < 0.01); see Fig. 2. However, reaction time in the AP condition was not significantly slower than in the NP condition. Accuracy of task performance was over 98% in all four conditions, and was not affected by the state or drug conditions.

Average reaction times for the choice reaction time task after caffeine and placebo in the abstained and normal state. Caffeine decreased reaction times in the abstained state (paired t test placebo to caffeine: *p < 0.01), but not in the normal state. Bars are SEM
Congruent trials of the flanker selective attention task were performed faster than the incongruent trials (task: F (1, 16) = 92.7; p < 0.001); see Fig. 3. Caffeine reduced reaction times during the incongruent trials, but not in the congruent trials (drug × task: F (1, 16) = 9.8; p < 0.01; t test incongruent trials AP to AC: t (16) = 2.2; p < 0.05; NP to NC: t (16) = 3.1; p < 0.01). Caffeine decreased the interference effect overall (drug: F (1, 16) = 9.8; p < 0.01) and this decrease from NP to NC was significant (t (16) = 4.2; p < 0.005). Performance accuracy for congruent trials (100%) was higher than for incongruent trials (93.2%; task: F (1, 16) = 33.4; p < 0.001), although accuracy was not affected by the state or drug conditions.

Average reaction times for the congruent and incongruent task conditions in the flanker selective attention task following placebo and caffeine in the abstained (AP and AC, respectively) and normal state (NP and NC, respectively). Caffeine decreased reaction time in the incongruent task (paired t test AP to AC and NP to NC: *p < 0.05), but not in the congruent task. Bars are SEM
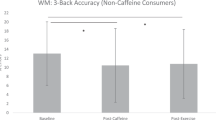
Performance accuracy for the 2-back memory task (96.6%) was lower than for the 1-back task (97.8%; task: F (1, 16) = 6.0; p < 0.05); see Fig. 4. Despite a pattern of increased accuracy after caffeine, there was only a trend towards a drug effect (F (1, 16) = 2.9; p = 0.11); this increase was significant for the 1-back task from AP to AC (t (16) = 2.4; p < 0.05). There were no main effects or interactions for the difference in accuracy between the two tasks (1-back–2-back). Reaction times for the 1-back task were faster than for the 2-back task (task: F (1, 16) = 20.7; p < 0.001). Caffeine reduced reaction times for both trial types (drug: F (1, 16) = 4.7; p < 0.05). This reduction was significant for the 1-back task from NP to NC (t (16) = 3.6; p < 0.005). Reaction times were slower in the normal state than in the abstained state for the 2-back task, but there was no difference between states for the 1-back task (state × task: F (1, 16) = 14.9; p < 0.005). Reaction times for the 2-back task decreased across sessions, and the state effect may be attributable to an imbalance in the state by drug conditions. There were no session effects for 2-back accuracy, 1-back accuracy, or 1-back reaction time.

Average accuracy (percent correct responses) for the 1-back and 2-back task conditions in the memory task following placebo and caffeine in the abstained (AP and AC, respectively) and normal state (NP and NC, respectively). Caffeine increased accuracy in the 1-back task (paired t test AP to AC: *p < 0.05), but did not significantly affect accuracy in the 2-back task. Bars are SEM
Discussion
We evaluated the effects of caffeine following normal caffeine use among moderate consumers, and compared the results to the administration of caffeine following 30 h of abstinence among the same subjects. As we hypothesized, caffeine had less of an effect on mood and choice reaction time in the normal state than in the abstained state. Abstention had a negative effect on mood and choice reaction time, but not on selective attention and memory. Caffeine improved selective attention and memory in both the abstained and normal caffeine states. These results suggest that among moderate daily caffeine users there may be some benefits to consuming more than one’s typical daily intake.
Patterns of caffeine consumption reflect the belief that caffeine has stimulant effects above and beyond relief from withdrawal symptoms. For example, students who drink a cup of coffee every morning may drink two or three cups the morning of an exam, believing that caffeine will enhance their alertness and performance above average. The literature on mood symptoms overwhelmingly attributes caffeine with improving alertness and alleviating fatigue (for reviews, see Smith 2002; Ruxton 2008). However, some argue that these effects occur in low or nonhabitual caffeine consumers, but tolerance develops during habitual use, so consuming more than the maintenance dose ought to have little or no beneficial effect (James and Rogers 2005; Rogers 2007). While this has frequently been shown for mood (Richardson et al. 1995; Phillips-Bute and Lane 1997; James 1998; Robelin and Rogers 1998; Yeomans et al. 2002), several studies have also shown positive effects in a nonwithdrawn state (Frewer and Lader 1991; Warburton 1995; Christopher et al. 2005). In our study, caffeine improved mood in the abstained state only. In the normal state, caffeine had no effect (Fig. 1). Interestingly, mood worsened after placebo in both the abstained and normal states. It is possible that the interval between mood reports resulted in boredom or fatigue, or exaggerated existing withdrawal symptoms in the placebo conditions. Alternatively, caffeine may have maintained positive mood that otherwise would have been lessened by this waiting period.
While some studies have suggested that caffeine withdrawal can impair behavioral performance by slowing reaction time or decreasing accuracy (Streufert et al. 1995; James 1998; Robelin and Rogers 1998; Yeomans et al. 2002), other studies have reported no impairments during withdrawal (Richardson et al. 1995; Phillips-Bute and Lane 1997; Haskell et al. 2005; Hewlett and Smith 2006). In this study, performance was not significantly adversely affected by withdrawal, although choice reaction time exhibited a trend to be slower in the AP than in the NP condition (Fig. 2). Caffeine significantly decreased reaction time in the abstained state but had no effect in the normal state, possibly because participants were already responding at an optimal speed.
In the selective attention task, caffeine decreased incongruent reaction times and the interference effect, suggesting that caffeine enhances selective attention regardless of state (Fig. 3). Caffeine had a smaller effect on accuracy in the memory task; only the 1-back task in the abstained state was significantly improved in follow-up comparisons, although there is a pattern of improvement after caffeine across the two tasks and states (Fig. 4). The absence of a significant effect was expected, since many studies report little or no effect of caffeine on memory (Foreman et al. 1989; Warburton 1995; Phillips-Bute and Lane 1997; Koppelstaetter et al. 2008). Unexpectedly, reaction times were slower in the 2-back task during the normal state than during the abstained state. We hypothesize that this finding is due to a practice effect combined with an imbalance in the state by drug condition orders and could have been eliminated by increasing our sample size to include all possible state by drug combinations. Alternatively, caffeine has been reported to impair memory (Mednick et al. 2008). Another consideration is that our subjects could have been exerting more effort during the abstained state to compensate for withdrawal-related fatigue. Future studies are needed to resolve this issue.
In the normal caffeinated state, caffeine did not improve mood, choice reaction time, or memory accuracy. It is possible that this is a result of tolerance, however, the increased side-effect ratings do not support the development of tolerance, and there may be other explanations for the lack of an effect. First, tolerance may have partially developed and was not overcome by the amount of caffeine administered. Second, there may be ceiling effects of the measures used; for example, if a subject rated alertness as a 5 out of 5 prior to caffeine, then his alertness level could not be shown to increase after caffeine. Third, there may be physiological boundaries; if a subject is already responding at a maximum speed then his reaction time cannot be reduced further by caffeine. None of these explanations preclude caffeine’s ability to act as a stimulant in the central nervous system of habitual consumers. Perhaps studies utilizing brain imaging techniques could provide more insights on the underlying neurobiology of the acute and chronic effects of caffeine without relying on subjective reports or behavioral limitations (e.g., Dager et al. 1999; Laurienti et al. 2002; Sigmon et al. 2009).
The methods used here differ from the majority of caffeine studies in several ways. Most notable is our use of the normal caffeinated state as a baseline. Some studies have administered caffeine in a normal caffeinated state, but did not include a withdrawn state for comparison (Frewer and Lader 1991; Christopher et al. 2005). Others have controlled for withdrawal by administering a pretreatment dose of caffeine (Warburton 1995; Yeomans et al. 2002), by comparing habitual consumers to non- or low-consumers (Rogers et al. 2003; Haskell et al. 2005; Hewlett and Smith 2007), or by comparing overnight withdrawn to long-term abstinent consumers (James 1998; Rogers et al. 2005). Several studies have controlled for both tolerance and withdrawal among habitual users in a caffeinated state by including a long-term abstinent condition (≥1 week) for comparison; these results suggest that once tolerance has developed, the daily maintenance dose of caffeine does not improve mood and performance above the long-term abstinent baseline (Evans and Griffiths 1992; James et al. 2005; Judelson et al. 2005; Sigmon et al. 2009). Inclusion of a long-term abstinent condition could have strengthened our methods, especially by ensuring that our subjects and measures were sensitive to an acute dose of caffeine prior to the development of tolerance. Also, without this condition for comparison, the positive effects on performance seen in the normal caffeinated state could be attributed to withdrawal reversal, although withdrawal typically begins after 12 h of abstinence (Griffiths and Woodson 1988; Juliano and Griffiths 2004). However, the aim of this study was to compare whether an extra dose of caffeine could improve mood and performance above the normal caffeinated state baseline, and none of the above articles describe the effects of an acute dose of caffeine beyond the maintenance dose. Arguably, the effects of caffeine in long-term abstinent subjects are not necessarily equivalent to the effects in habitual users, since caffeine has induced adaptive physiological changes following daily caffeine use. This question would be best addressed with a study comparing the stimulant effects of caffeine to placebo in all three normal-caffeinated, overnight-withdrawn, and long-term abstinent states.
We also prescreened potential participants for withdrawal symptoms. A review of caffeine self-administration reported that withdrawal symptoms occur in less than half of daily caffeine users (Hughes et al. 1993), and including subjects who do not experience withdrawal symptoms could confound or reduce the effect of withdrawal. A drawback is that prescreening selects subjects who may expect to experience withdrawal symptoms. Whether the presence or absence of these symptoms interacts with the effects of withdrawal on cognitive performance or caffeine consumption would be an interesting future direction. In addition, we requested 30 h of caffeine abstinence, since withdrawal symptoms reportedly peak between 20–51 h (Juliano and Griffiths 2004), although the majority of withdrawal studies only request overnight abstinence. Determining how the intensity of these symptoms, or the duration of abstinence, affects withdrawal-related behaviors would also be an important issue to resolve in the future.
A limitation of our study is that participants were not blind to the caffeine state they were experiencing (normal or abstained), and expectancy effects may have contributed to the mood results. Expectations can predict the perceived effects of caffeine on mood after the ingestion of a placebo believed to be caffeine (Fillmore and Vogelsprott 1992; Lotshaw et al. 1996). Other studies have blinded participants to the state they were experiencing by replacing dietary caffeine with study-supplied capsules or beverages (James 1998; Rogers et al. 2005). The drug ingested during our study session was administered double-blind to prevent expectancy effects from influencing the change in mood scores, although we did not administer a follow-up questionnaire to confirm whether or not the blinding was effective. A second limitation is that our 250-mg dose increased side effects, which could have informed some participants that they had ingested caffeine instead of placebo. This dose was selected because it has been shown to be effective in changing mood and reaction time while producing few side effects (Lieberman et al. 1987; Frewer and Lader 1991; Kaplan et al. 1997). Alternatively, smaller doses (e.g., 50% of total daily intake) have been shown to prevent withdrawal symptoms (Mitchell et al. 1995) and produce positive changes in mood and performance (Lieberman et al. 1987). Other measures, such as vigilance or rapid visual information processing performance, have been shown to be sensitive to caffeine (Fine et al. 1994; Yeomans et al. 2002; Childs and de Wit 2006), and including those measures in our study could have informed our results. Lastly, participants were asked to abstain from caffeine for 30 h prior to capsule administration, but the actual duration of caffeine abstinence depended on their normal pattern of caffeine use. Different abstinence durations could have increased variability in withdrawal symptom intensity between subjects. Similarly, the exact time of caffeine use in the normal state was not recorded in the participants’ diaries. No attempt was made to control the timing of caffeine use outside the study to preserve the naturalistic design, but variability in the interval between last caffeine use and the onset of the study across participants may have affected the results and could have been controlled for in the analyses.
In summary, we compared the effects of caffeine in an abstained and a normal caffeinated state to determine whether the stimulant effects of caffeine can mostly be attributed to alleviating withdrawal, or whether caffeine can produce stimulant effects beyond the normal baseline. Our results suggest that caffeine was most effective at improving mood and simple reaction time following 30 h of abstention among moderate users. However, caffeine also provided some performance gains on more cognitively demanding tasks when administered following normal daily caffeine consumption. This corroborates the common habit among daily caffeine users of caffeine loading before a particularly challenging mental activity.
References
Addicott MA, Yang LL, Peiffer AM, Laurienti PJ (2009) Methodological considerations for the quantification of self-reported caffeine use. Psychopharmacology 203:571–578
Childs E, de Wit H (2006) Subjective, behavioral, and physiological effects of acute caffeine in light, nondependent caffeine users. Psychopharmacology 185:514–523
Chou DT, Khan S, Forde J, Hirsh KR (1985) Caffeine tolerance: behavioral, electrophysiological and neurochemical evidence. Life Sci 36:2347–2358
Christopher G, Sutherland D, Smith A (2005) Effects of caffeine in non-withdrawn volunteers. Hum Psychopharmacol Clin Exp 20:47–53
Dager SR, Layton ME, Strauss W, Richards TL, Heide A, Friedman SD, Artru AA, Hayes CE, Posse S (1999) Human brain metabolic response to caffeine and the effects of tolerance. Am J Psychiatry 156:229–237
Deroche GM, Portz BS, Rector WG, Everson GT (1990) Simultaneous determination of caffeine and antipyrine in plasma and saliva using high-performance liquid-chromatography. J Liq Chromatogr 13:3493–3505
Eriksen BA, Eriksen CW (1974) Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept Psychophys 16:143–149
Evans SM, Griffiths RR (1992) Caffeine tolerance and choice in humans. Psychopharmacology (Berl) 108:51–59
Evans SM, Griffiths RR (1999) Caffeine withdrawal: a parametric analysis of caffeine dosing conditions. J Pharmacol Exp Ther 289:285–294
Ferre S (2008) An update on the mechanisms of the psychostimulant effects of caffeine. J Neurochem 105:1067–1079
Fillmore M, Vogelsprott M (1992) Expected effect of caffeine on motor performance predicts the type of response to placebo. Psychopharmacology 106:209–214
Fine BJ, Kobrick JL, Lieberman HR, Marlowe B, Riley RH, Tharion WJ (1994) Effects of caffeine or diphenhydramine on visual vigilance. Psychopharmacology 114:233–238
Finn IB, Holtzman SG (1986) Tolerance to caffeine-induced stimulation of locomotor activity in rats. J Pharmacol Exp Ther 238:542–546
Foreman N, Barraclough S, Moore C, Mehta A, Madon M (1989) High doses of caffeine impair performance of a numerical version of the Stroop task in men. Pharmacol Biochem Behav 32:399–403
Frewer LJ, Lader M (1991) The effects of caffeine on two computerized tests of attention and vigilance. Hum Psychopharmacol 6:119–128
Green RM, Stiles GL (1986) Chronic caffeine ingestion sensitizes the A1 adenosine receptor-adenylate cyclase system in rat cerebral cortex. J Clin Invest 77:222–227
Griffiths RR, Woodson PP (1988) Caffeine physical dependence: a review of human and laboratory animal studies. Psychopharmacology 94:437–451
Griffiths RR, Evans SM, Heishman SJ, Preston KL, Sannerud CA, Wolf B, Woodson PP (1990) Low-dose caffeine physical dependence in humans. J Pharmacol Exp Ther 255:1123–1132
Haskell CF, Kennedy DO, Wesnes KA, Scholey AB (2005) Cognitive and mood improvements of caffeine in habitual consumers and habitual non-consumers of caffeine. Psychopharmacology 179:813–825
Heatherley SV, Hayward RC, Seers HE, Rogers PJ (2005) Cognitive and psychomotor performance, mood, and pressor effects of caffeine after 4, 6 and 8 h caffeine abstinence. Psychopharmacology (Berl) 178:461–470
Hewlett P, Smith A (2006) Acute effects of caffeine in volunteers with different patterns of regular consumption. Hum Psychopharmacol 21:167–180
Hewlett P, Smith A (2007) Effects of repeated doses of caffeine on performance and alertness: new data and secondary analyses. Hum Psychopharmacol 22:339–350
Holland DT, Godfredsen KA, Page T, Conner JD (1998) Simple high-performance liquid chromatography method for the simultaneous determination of serum caffeine and paraxanthine following rapid sample preparation. J Chromatogr B Analyt Technol Biomed Life Sci 707:105–110
Hughes JR, Oliveto AH, Bickel WK, Higgins ST, Badger GJ (1993) Caffeine self-administration and withdrawal: incidence, individual differences and interrelationships. Drug Alcohol Depend 32:239–246
James JE (1994) Does caffeine enhance or merely restore degraded psychomotor performance. Neuropsychobiology 30:124–125
James JE (1998) Acute and chronic effects of caffeine on performance, mood, headache, and sleep. Neuropsychobiology 38:32–41
James JE, Rogers PJ (2005) Effects of caffeine on performance and mood: withdrawal reversal is the most plausible explanation. Psychopharmacology (Berl) 182:1–8
James JE, Gregg ME, Kane M, Harte F (2005) Dietary caffeine, performance and mood: enhancing and restorative effects after controlling for withdrawal reversal. Neuropsychobiology 52:1–10
Johansson B, Georgiev V, Lindstrom K, Fredholm BB (1997) A1 and A2A adenosine receptors and A1 mRNA in mouse brain: effect of long-term caffeine treatment. Brain Res 762:153–164
Judelson DA, Armstrong LE, Sokmen B, Roti MW, Casa DJ, Kellogg MD (2005) Effect of chronic caffeine intake on choice reaction time, mood, and visual vigilance. Physiol Behav 85:629–634
Juliano LM, Griffiths RR (2004) A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features. Psychopharmacology (Berl) 176:1–29
Kaplan GB, Greenblatt DJ, Ehrenberg BL, Goddard JE, Cotreau MM, Harmatz JS, Shader RI (1997) Dose-dependent pharmacokinetics and psychomotor effects of caffeine in humans. J Clin Pharmacol 37:693–703
Koppelstaetter F, Poeppel TD, Siedentopf CM, Ischebeck A, Verius M, Haala I (2008) Does caffeine modulate verbal working memory processes? An fMRI study. Neuroimage 39:492–499
Landrum RE (1992) College students' use of caffeine and its relationship to personality. Coll Stud J 26:151–155
Laurienti PJ, Field AS, Burdette JH, Maldjian JA, Yen YF, Moody DM (2002) Dietary caffeine consumption modulates fMRI measures. Neuroimage 17:751–757
Lieberman HR, Wurtman RJ, Emde GG, Roberts C, Coviella IL (1987) The effects of low doses of caffeine on human performance and mood. Psychopharmacology (Berl) 92:308–312
Loke WH, Meliska CJ (1984) Effects of caffeine use and ingestion on a protracted visual vigilance task. Psychopharmacology 84:54–57
Lorist MM, Snel J (1997) Caffeine effects on perceptual and motor processes. Electroencephalogr Clin Neurophysiol 102:401–413
Lotshaw SC, Bradley JR, Brooks LR (1996) Illustrating caffeine's pharmacological and expectancy effects utilizing a balanced placebo design. J Drug Educ 26:13–24
Mednick SC, Cai DJ, Kanady J, Drummond SPA (2008) Comparing the benefits of caffeine, naps and placebo on verbal, motor and perceptual memory. Behav Brain Res 193:79–86
Mitchell SH, Dewit H, Zacny JP (1995) Caffeine withdrawal symptoms and self-administration following caffeine deprivation. Pharmacol Biochem Behav 51:941–945
Nehlig A (1999) Are we dependent upon coffee and caffeine? A review on human and animal data. Neurosci Biobehav Rev 23:563–576
Nehlig A, Daval JL, Boyet S, Vert P (1986) Comparative effects of acute and chronic administration of caffeine on local cerebral glucose utilization in the conscious rat. Eur J Pharmacol 129:93–103
Patwardhan RV, Desmond PV, Johnson RF, Schenker S (1980) Impaired elimination of caffeine by oral-contraceptive steroids. J Lab Clin Med 95:603–608
Phillips-Bute BG, Lane JD (1997) Caffeine withdrawal symptoms following brief caffeine deprivation. Physiol Behav 63:35–39
Posthuma D, Mulder EJ, Boomsma DI, de Geus EJ (2002) Genetic analysis of IQ, processing speed and stimulus-response incongruency effects. Biol Psychol 61:157–182
Powell KR, Luvone PM, Holtzman SG (2001) The role of dopamine in the locomotor stimulant effects and tolerance to these effects of caffeine. Pharm Biochem Behav 69:59–70
Richardson NJ, Rogers PJ, Elliman NA, O'Dell RJ (1995) Mood and performance effects of caffeine in relation to acute and chronic caffeine deprivation. Pharmacol Biochem Behav 52:313–320
Robelin M, Rogers PJ (1998) Mood and psychomotor performance effects of the first, but not of subsequent, cup-of-coffee equivalent doses of caffeine consumed after overnight caffeine abstinence. Behav Pharmacol 9:611–618
Rogers PJ (2007) Caffeine, mood and mental performance in everyday life. Nutr Bull 32:84–89
Rogers PJ, Dernoncourt C (1998) Regular caffeine consumption: a balance of adverse and beneficial effects for mood and psychomotor performance. Pharmacol Biochem Behav 59:1039–1045
Rogers PJ, Martin J, Smith C, Heatherley SV, Smit HJ (2003) Absence of reinforcing, mood and psychomotor performance effects of caffeine in habitual non-consumers of caffeine. Psychopharmacology 167:54–62
Rogers PJ, Heatherley SV, Hayward RC, Seers HE, Hill J, Kane M (2005) Effects of caffeine and caffeine withdrawal on mood and cognitive performance degraded by sleep restriction. Psychopharmacology 179:742–752
Rubenstein KE, Schneider RS, Ullman EF (1972) Homogenous enzyme immunoassay: a new immunochemical technique. Biochem Biophys Res Commun 47:846–851
Ruxton CHS (2008) The impact of caffeine on mood, cognitive function, performance and hydration: a review of benefits and risks. Nutr Bull 33:15–25
Shi D, Daly JW (1999) Chronic effects of xanthines on levels of central receptors in mice. Cell Mol Neurobiol 19:719–732
Sigmon SC, Herning RI, Better W, Cadet JL, Griffiths RR (2009) Caffeine withdrawal, acute effects, tolerance, and absence of net beneficial effects of chronic administration: cerebral blood flow velocity, quantitative EEG, and subjective effects. Psychopharmacology. 204(4):573–85
Smith A (2002) Effects of caffeine on human behavior. Food Chem Toxicol 40:1243–1255
Smith A, Sutherland D, Christopher G (2005) Effects of repeated doses of caffeine on mood and performance of alert and fatigued volunteers. J Psychopharmacology 19:620–626
Streufert S, Pogash R, Miller J, Gingrich D, Landis R, Lonardi L, Severs W, Roache JD (1995) Effects of caffeine deprivation on complex human functioning. Psychopharmacology 118:377–384
Varani K, Portaluppi F, Merighi S, Ongini E, Belardinelli L, Borea PA (1999) Caffeine alters A2A adenosine receptors and their function in human platelets. Circulation 99:2499–2502
Warburton DM, Bersellini E, Sweeney E (2001) An evaluation of a caffeinated taurine drink on mood, memory and information processing in healthy volunteers without caffeine abstinence. Psychopharmacology 158:322–328
Warburton DM (1995) Effects of caffeine on cognition and mood without caffeine abstinence. Psychopharmacology (Berl) 119:66–70
Yeomans MR, Ripley T, Davies LH, Rusted JM, Rogers PJ (2002) Effects of caffeine on performance and mood depend on the level of caffeine abstinence. Psychopharmacology (Berl) 164:241–249
Acknowledgments
We would like to thank the General Clinical Research Center for their assistance with the collection of data.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by grants from the National Institutes of Health (National Institute of Biomedical Imaging and Bioengineering: R01 EB03880 and National Institute on Drug Abuse: F31 DA024950).
Rights and permissions
About this article
Cite this article
Addicott, M.A., Laurienti, P.J. A comparison of the effects of caffeine following abstinence and normal caffeine use. Psychopharmacology 207, 423–431 (2009). https://doi.org/10.1007/s00213-009-1668-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-009-1668-3