
Abstract
Rationale
Research has begun to examine how acute cognitive impairment from alcohol could contribute to alcohol abuse. Specifically, alcohol-induced impairment of inhibitory control could compromise the drinker’s ability to stop the self-administration of alcohol, increasing the risk of binge drinking.
Objective
The present study was designed to test this hypothesis by examining the relation between acute alcohol impairment of inhibitory control and alcohol consumption during a single drinking episode.
Materials and methods
Twenty-six healthy adults performed a cued go/no-go task that measured inhibitory control. The study tested the degree to which their inhibitory control was impaired by a moderate dose of alcohol (0.65 g/kg) versus a placebo and the extent to which individual differences in this impairment predicted levels of alcohol consumption as assessed by ad lib drinking in the laboratory.
Results
In accord with the hypothesis, greater impairment of inhibitory control from alcohol was associated with increased ad lib consumption.
Conclusion
Acute impairment of inhibitory control might be an important cognitive effect that contributes to abuse in addition to the positive rewarding effects of the drug.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Understanding why individuals repeatedly engage in excessive alcohol consumption despite its myriad negative health consequences has been a long-standing challenge for researchers. It is well-recognized that alcohol abuse is an individual difference problem in that, while most adults are exposed to alcohol, only a few individuals develop abuse-related problems. One explanation for this individual difference is that drinkers who do develop abuse problems do so because they experience abnormal responses to alcohol, such as heightened reactions to the drug. Among the many affective, behavioral, and physiological changes that occur as acute responses to alcohol, particular interest has concerned the acute rewarding or pleasurable effects of the drug. Alcohol, like other drugs of abuse, can function as a powerful reinforcer (e.g., DiChiara et al. 1996; Koob 2003; Robinson and Berridge 1993). For some drinkers, the positive rewarding effects of alcohol could be of sufficient intensity to maintain its excessive use despite the accrual of negative consequences (Koob 2003; Koob et al. 1998). In short, the acute rewarding effects simply outweigh the negative short-term and long-term consequences of excessive use.
There is considerable empirical evidence from human and animal studies to support the notion that the rewarding effects of drugs play a major role in drug abuse. For example, preclinical studies show that a priming dose of alcohol can reinstate alcohol consumption in recently detoxified laboratory animals (Katz and Higgins 2003; Shaham et al. 2003). Furthermore, studies of humans find that an initial small dose of alcohol can “prime” an individual to consume more alcohol (de Wit and Chutuape 1993; Fillmore 2001; Fillmore and Rush 2001; Ludwig et al. 1974). Alcohol priming has been demonstrated in both alcoholics and social drinkers (e.g., de Wit and Chutuape 1993; Ludwig et al. 1974). Traditionally, such effects have been attributed to alcohol’s action on brain mechanisms of reward, whereby incentive properties of a small dose reinforce the consumption of greater amounts (Koob and Le Moal 1997; Robinson and Berridge 1993; Stewart et al. 1984; Wise and Bozarth 1987).
Although there is little dispute that reward mechanisms play an important role in abuse potential, neurocognitive mechanisms have become another focus in recent years. Researchers have begun to consider how the acute effects of alcohol itself can contribute directly to its abuse potential by altering the drinker’s neurocognitive mechanisms involved in the regulation and self-control of behavior and attention (Fillmore 2003, 2007; Lyvers 2000). Alcohol is well-known for its acute “disinhibiting” effects on behavior and its chronic use is associated with sustained states of undercontrolled behavior often described as impulsivity (e.g., Bates et al. 2002; Fillmore 2003, 2007; Jentsch and Taylor 1999; Lyvers 2000). According to several theories, behavioral control is governed by two independent processes: an activational process and an inhibitory process (Fowles 1987; Gray 1976; Logan and Cowan 1984). The activational process is responsible for executing behavior, whereas the inhibitory process is responsible for inhibiting inappropriate or unwanted behavior. These two processes act in opposition, and behavior is assumed to reflect the relative strength of each process.
During the past decade, laboratory studies have provided considerable support for the notion that alcohol can actually promote impulsive actions by impairing basic inhibitory mechanisms that normally serve to suppress inappropriate behavior (Fillmore 2003, 2007). Stop-signal and cued go/no-go tasks are reaction time tasks used to model behavioral control as the ability to quickly activate a response to a go-signal and suddenly inhibit a response when a stop-signal occurs (Logan 1994; Logan and Cowan 1984; Miller et al. 1991). Studies using these tasks have found that alcohol impairs the ability to inhibit behavior (e.g., de Wit et al. 2000; Fillmore and Vogel-Sprott 2000; Marczinski and Fillmore 2003; Mulvihill et al. 1997). The findings are important because they identify a basic inhibitory mechanism that is impaired by alcohol which could contribute to the display of impulsive, aggressive, and other socially inappropriate behaviors under the drug (Fillmore 2003, 2007; Jentsch and Taylor 1999).
The impairing effect of alcohol on the drinker’s inhibitory control might also contribute to the abuse potential of the drug. The ability to inhibit or terminate instigated and ongoing behaviors is likely integral in the process of terminating a drinking episode. When inhibitory control is reduced or compromised in some fashion, as it appears to be following alcohol consumption, the drinker’s ability to stop the self-administration of alcohol could be impaired. Such a theory could explain why many heavy drinkers and alcoholics begin a drinking episode with the intention of having only one or two drinks but continue on to drink excessively to the point of gross intoxication. The initial couple of drinks could be sufficient to impair the drinker’s ability to inhibit the ongoing act of continuing alcohol consumption, resulting in the inability to stop drinking in the situation. Furthermore, this acute impairment of inhibitory control likely occurs in conjunction with the drug’s rewarding effects that serve to positively reinforce continued consumption in the situation.
The impairing effect of alcohol on behavioral inhibition demonstrated in simple laboratory tasks, such as the cued go/no-go task, could contribute importantly to our understanding of nonreward-based mechanisms by which acute alcohol intoxication could operate to promote continued and excessive alcohol consumption. In the past, cognitive factors such as this have been largely ignored as mechanisms of abuse in favor of more traditional theories based on the rewarding properties of the drug. Given that impaired inhibitory control could promote excessive drinking, it is reasonable to assume that individuals who experience greater impairments of inhibitory control from alcohol should be more likely to drink excessively. The present study was designed to examine the relation between acute alcohol impairment of inhibitory control and alcohol consumption during a single drinking episode. The study used the cued go/no-go model of inhibitory control to measure the degree to which inhibitory control was impaired by a moderate dose of alcohol (0.65 g/kg) and to determine the extent to which individual differences in this impairment predicted levels of alcohol consumption as assessed by ad lib drinking in the laboratory.
Materials and methods
Participants
Twenty-six adult drinkers (12 women and 14 men) between the ages of 21 and 26 years (mean age = 21.9, SD = 1.4) were recruited to participate in this study. Screening measures were conducted to determine medical history and current and past drug and alcohol use. Any volunteers who self-reported head trauma, psychiatric disorder, or substance abuse disorder were excluded from participation. Volunteers were asked a series of specific questions in order to determine their typical drinking habits. Those who reported infrequent drinking (i.e., less than two drinking occasions per month) or who reported a potential risk for alcohol dependence were excluded from participation. Dependence was determined by a score of 5 or higher on the Short Michigan Alcoholism Screening Test (S-MAST) (Seltzer et al. 1975). Any other high-risk indicators of dependence, including prior treatment for an alcohol use disorder and driving under the influence conviction, also precluded participation in the study. These screening measures allowed for recruitment of adults who regularly consumed alcohol, while excluding those who were dependent on alcohol. Additionally, because the study involved an ad lib beer consumption session, all volunteers were asked if they enjoyed drinking beer. Any volunteers who did not like to drink beer were ineligible for participation.
Recent use of amphetamine, barbiturates, benzodiazepines, cocaine, opiates, and tetrahydrocannabinol was assessed by means of urine analysis. Any volunteer who tested positive for the presence of any of these drugs was excluded from participation. No female volunteers who were pregnant or breast-feeding, as determined by self-report and urine human chorionic gonadotrophin levels, participated in this study. Volunteers were recruited via notices placed on community bulletin boards and by university newspaper advertisements. The University of Kentucky Medical Institutional Review Board approved the study, and participants received $120 for their participation.
Apparatus and materials
Cued go/no-go task
Inhibitory control was measured by a cued go/no-go reaction time task used in other research to measure the disinhibiting effects of alcohol (e.g., Fillmore et al. 2005; Marczinski and Fillmore 2003). Cues provide preliminary information regarding the type of imperative target stimulus (i.e., go or no-go) that is likely to follow. The cues have a high probability of signaling the correct target. Inhibitory and activational tendencies show rapid development of cue dependence as the cues come to elicit preparatory processes for the inhibition or execution of behavior (e.g., Miller et al. 1991; Posner 1980). The go cue conditions are of particular interest. Go cues generate response prepotency which speeds response time to go targets. However, participants must overcome this response prepotency in order to inhibit the response if a no-go target is subsequently displayed. Failures to inhibit responses to no-go targets are more frequent following go cues compared with no-go cues, indicating that it is more difficult to inhibit prepotent responses (Miller et al. 1991). Moreover, inhibitory control in this prepotent, go cue condition appears to be highly sensitive to the effects of alcohol and other psychoactive drugs (for review, see Fillmore 2003).
The task was operated using the E-Prime experiment generation software (Schneider et al. 2002) and was performed on a personal computer. A trial involved the following sequence of events: (a) presentation of a fixation point (+) for 800 ms; (b) a blank white screen for 500 ms; (c) a cue, displayed for one of five stimulus onset asynchronies (SOAs = 100, 200, 300, 400, and 500 ms); (d) a go or no-go target, which remained visible until a response occurred or 1,000 ms had elapsed; and (e) an intertrial interval of 700 ms.
The cue was a rectangle (7.5 × 2.5 cm) framed in a 0.8-mm black outline that was presented in the center of the computer monitor against a white background. The cue was presented in either a horizontal (2.5 cm tall × 7.5 cm wide) or vertical (7.5 cm tall × 2.5 cm wide) orientation. The go and no-go targets were colored green and blue, respectively, and they were displayed on the monitor as a solid hue that filled the interior of the rectangle cue. Participants were instructed to press the forward slash (/) key on the keyboard as soon as a go (green) target appeared and to suppress the response when a no-go (blue) target was presented. Key presses were made with the right index finger.
The orientation of the cue (horizontal or vertical) signaled the probability that a go or no-go target would be displayed. Cues that were presented vertically preceded the go target on 80% of the trials and preceded the no-go target on 20% of the trials. Cues that were presented horizontally preceded the no-go target on 80% of the trials and preceded the go target on 20% of the trials. Therefore, on the basis of cue–target pairings, vertical and horizontal cues operated as go and no-go cues, respectively. The different SOAs (100, 200, 300, 400, and 500 ms) between cues and targets encouraged participants to pay attention to the cues, and the variability and randomness of the SOAs prevented the participants from anticipating the exact onset of the targets.
A test consisted of 250 trials that presented the four possible cue–target combinations. An equal number of vertical (125) and horizontal (125) cues were presented before an equal number of go (125) and no-go (125) target stimuli. Each cue–target combination was presented at each of the five SOAs, and an equal number of SOAs separated each cue–target combination. The presentation of cue–target combinations and SOAs was random. For each trial, the computer recorded whether a response occurred and, if so, the reaction time (RT) in milliseconds was measured from the onset of the target until the key was pressed. To encourage quick and accurate responding, feedback was presented to the participant during the intertrial interval by displaying the words correct or incorrect along with the RT in milliseconds. A test required approximately 15 min to complete.
Personal drinking habits questionnaire (PDHQ; Vogel-Sprott 1992)
This questionnaire was administered in order to identify two measures of an individual’s current, typical drinking habits: typical blood alcohol concentration (BAC; typical peak BAC attained during a drinking episode) and frequency (number of drinking occasions per week). Typical BAC was calculated based on self-reported number of drinks usually consumed in a drinking episode, the type of alcohol usually consumed (beer, wine, or liquor), and the typical hourly duration of the drinking episode. This information, along with gender and weight in kilograms, was entered into an anthropometric formula to calculate peak BAC obtained during the typical drinking episode of each participant (McKim 2007). BAC is a good general indicator of functional impairment and so this measure of a drinker’s “typical BAC” provides a good indication of problem drinking behavior for the individual (NIAAA 2004).
Barratt impulsiveness scale (BIS-10; Patton et al. 1995)
This 34-item self-report questionnaire measures the personality dimension of impulsivity, thought to contribute to both behavioral disinhibition in response to alcohol and risk for alcohol abuse (Fillmore 2007; Finn et al. 1994; Sher and Trull 1994). Sample items include “I plan tasks carefully,” “I am self-controlled,” and “I act ‘on impulse’.” Participants indicate how typical each of the statements is for them on a four-point Likert scale (“rarely/never,” “occasionally,” “often,” or “almost always/always”). Scores range from 34 to 136 with higher scores indicating greater total levels of impulsiveness. In addition to a total score, six factors can be obtained from the questionnaire that assess different aspects of impulsivity, including attention (focusing on the task at hand), motor impulsiveness (acting on the spur of the moment), self-control (planning and thinking carefully), cognitive complexity (enjoying challenging mental tasks), perseverance (a consistent life style), and cognitive instability (thought insertions and racing thoughts).
Subjective intoxication
Degree of subjective intoxication was measured on a visual analog scale that has been used in previous research (e.g., Fillmore and Blackburn 2002). Participants rated their degree of subjective intoxication by placing a vertical line at the point representing the extent to which they “feel the alcohol” on a 100-mm horizontal line ranging from 0 mm “not at all” to 100 mm “very much.”
BACs
These were determined from breath samples measured by an Intoxilyzer, Model 400 (CMI, Owensboro, KY, USA).
Procedure
Screening
Interested volunteers responded to study advertisements by calling the laboratory. At that time, they were informed that the purpose of the study was to examine the effects of alcohol on computer tasks. An intake screening interview was also conducted on the telephone in order to determine eligibility for participation in the study. Any volunteer with a self-reported psychiatric disorder, learning disability, or substance abuse problem was excluded from the study. Eligible volunteers then made appointments to come in to the laboratory for four sessions: a familiarization session, two dose–challenge sessions, and an ad lib alcohol consumption session. All participants were tested individually. Sessions were scheduled at least 24 h apart and were completed within 3 weeks. Participants were instructed to fast for 4 h prior to each alcohol session, as well as to refrain from consuming alcohol or any psychoactive drugs or medications for 24 h before all sessions. Prior to each session, participants provided urine samples that were tested for the presence of drug metabolites (ON trak TesTstiks, Roche Diagnostics, Indianapolis, IN, USA) and, in women, HCG, in order to verify that they were not pregnant (Mainline Confirms HGL, Mainline Technology, Ann Arbor, MI, USA). Breath samples were also provided at the beginning of each session to verify a zero BAC.
Familiarization
All participants completed a familiarization session in order to become acquainted with laboratory procedures and the cued go/no-go task and to obtain necessary information required for participation. During this session, informed consent for participation was provided. Participants’ heights and weights were measured, and the questionnaire measures were completed. Task instructions for the cued go/no-go task were explained, and participants completed one 15-min practice trial, which is sufficient to become familiar with the task (Marczinski and Fillmore 2003).
Dose–challenge sessions
The degree to which alcohol impaired inhibitory control was examined with the cued go/no-go task. Performance was tested under an active dose (0.65 g/kg) and a placebo (0.0 g/kg). Dose order was randomized across subjects, and dose was calculated based on body weight. The alcohol beverage was served as one part alcohol and three parts carbonated mix, divided equally into two glasses. Participants had 2 min to finish each glass, and the two glasses were served 4 min apart. The placebo beverage consisted of four parts carbonated mix and was served in the same manner. Five milliliters of alcohol was floated on the top of each glass and the glasses were sprayed with an alcoholic mist which resembled condensation and provided a strong alcoholic odor. Previous research has shown that individuals report that these beverages contain alcohol (e.g., Fillmore and Blackburn 2002).
The 0.65-g/kg dose produces an average peak BAC of 80 mg/100 mL and was chosen on the basis of previous research that showed that response inhibition is reliably impaired at this BAC (e.g., Marczinski and Fillmore 2003). The peak BAC was expected to occur about 60 min after drinking (Fillmore and Vogel-Sprott 1998). Subjective effects were measured 20 min after drinking, and the cued go/no-go task was performed 30 min after drinking. Breath samples were collected at 25 and 45 min after drinking (immediately preceding and immediately following the testing period), during both the placebo and alcohol test sessions. Once the testing was finished, participants remained at leisure in the lounge area and were provided with snacks and drinks and allowed to watch movies and read magazines. Participants’ BACs were monitored at 20-min intervals and participants were allowed to leave once their BAC fell to 20 mg/100 mL or below.
Ad libitum consumption test
The final session measured the participants’ ad lib alcohol consumption. Participants completed a taste-rating task (Marlatt et al. 1973), which previous research has shown provides a reliable measure of ad lib consumption (Collins et al. 1996; Marczinski et al. 2005). Participants sampled four different beers, and using Likert scales, they rated them on various qualities (e.g., aftertaste, fullness) ostensibly to provide information on people’s beer preferences in order to aid in future research. The beers were served in four clear, frosted glasses, color-coded by a rubber band placed around the bottom of the glass. The beers sampled were Michelob Light™, Rolling Rock™, Molson Golden™, and Harp™. These were chosen because they are representative of beers commonly consumed by young adults and because they are all similar in per volume alcohol content (4.3%, 4.6%, 5.0%, and 4.55%, respectively).
Participants were told that this was a 4.5-h session and that the actual tasting portion would last for 90 min. They were told that they may drink as much of or as little of each beer as they liked, but to be sure to sample enough of each beer to give an accurate rating. The session took place in a room designed to promote a relaxing, leisurely atmosphere. Posters with slogans relating to beer and partying were hung on the walls, and participants were seated in a large recliner. Next to the recliner was a minirefrigerator in which the beers were kept when they were not being sampled. This allowed the beers to stay cold throughout the entire tasting process. A TV, DVD player, and stereo were also available to provide entertainment during the session. Ad lib sessions were held individually for each participant.
Once the 90 min had passed, participants’ BACs were measured and the four glasses were removed from the testing room. The remaining beer was measured in milliliters and subtracted from the total amount of beer presented to determine the amount of beer consumed by the participant.
Criterion measures
For the cued go/no-go task, failures of response inhibition were measured as the proportion of no-go targets in which a participant failed to inhibit a response. The measure of interest was the proportion (p) of inhibition failure score in the go cue (i.e., prepotent) condition. This proportion was calculated based on the 25 trials in which no-go targets were preceded by go cues. Greater p-inhibition failures indicate poorer inhibitory control (i.e., disinhibition). Impairment under alcohol compared to placebo was tested by a one-way repeated-measures analysis of variance (ANOVA). Speed of responding to targets in the go cue condition was measured by the participant’s average RT for a test. RT scores under alcohol compared to placebo were analyzed by a one-way repeated-measures ANOVA. Omission errors were also recorded when participants failed to respond to go targets. Omission errors were infrequent and occurred on no more than 2% of go target trials (approximately two trials per test) in either dose condition.
For the ad lib session, the principal measure of ad lib consumption was the amount of beer in milliliters consumed by the participant. Ad lib BAC was also measured by the subject’s breath sample obtained at the conclusion of the ad lib drinking period (i.e., at 90 min).
Results
Self-reported drinking habits
The mean typical BAC achieved by subjects outside of the laboratory was 97.2 mg/100 mL (SD = 71.9). Subjects’ typical BACs ranged from a minimum of 0 mg/100 mL to a maximum of 276 mg/100 mL. Mean drinking frequency for the sample was 2.2 occasions per week (SD = 0.9). Drinking frequencies ranged from a minimum of one to a maximum of five occasions per week. t tests obtained no significant gender differences in these drinking habits (ps > 0.16).
Dose–challenge sessions
No detectable BACs were observed in the placebo condition. Gender differences in BAC in the active dose condition were analyzed by a 2 (gender) × 2 (time) mixed-design ANOVA. No main effect or interaction involving gender was observed (ps > 0.37). There was a main effect of time, F(1, 24) = 36.8, p < 0.01, owing to an increase in BAC on the ascending limb of the BAC curve when testing occurred. For the entire sample, the mean BAC was 64.3 mg/100 mL (SD = 21.8) at the beginning of the test (25 min after drinking) and 84.7 mg/100 mL (SD = 20.2) at the conclusion of the test (45 min after drinking).
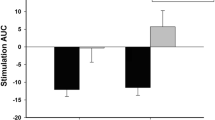
Alcohol impairment of p-inhibition failures was analyzed by a one-way repeated-measures ANOVA. A significant dose effect was found, F(1, 25) = 29.7, p < 0.01. Figure 1 (left panel) shows that alcohol impaired inhibitory control, as evident by the increase in p-failures under alcohol compared to placebo. Alcohol impairment of reaction time was analyzed by a one-way repeated-measures ANOVA. Again, a significant dose effect was found, F(1, 25) = 4.8, p = 0.04. Figure 1 (right panel) shows that alcohol significantly slowed reaction time compared to placebo. Subjective reports of intoxication were also affected by alcohol. A one-way repeated-measures ANOVA obtained a significant dose effect, F(1, 25) = 105.8, p < 0.01, demonstrating that alcohol significantly increased ratings of intoxication. The mean (SD) intoxication rating was 10.3 (12.3) under placebo and 42.8 (19.3) under alcohol.

Mean proportion of inhibitory failures under the 0.0-g/kg (placebo) and 0.65-g/kg alcohol dose conditions (left panel). Mean reaction time under the 0.0-g/kg (placebo) and 0.65-g/kg alcohol dose conditions (right panel). Capped vertical lines indicate standard errors of the mean
In order to examine individual differences, the magnitude of impaired inhibitory control for each subject was calculated as the difference in p-inhibition failures between the alcohol and placebo condition. p-inhibition failures under placebo were subtracted from those under alcohol for each subject, such that a greater difference score indicated greater alcohol impairment of inhibitory control (i.e., an increase in inhibitory failures). Mean magnitude of impairment for the entire sample was 0.08 (SD = 0.08). Scores ranged from a minimum of 0.00 (no impairment) to a maximum of 0.24. Thus, the sample displayed marked individual differences in the magnitude of alcohol impairment of inhibitory control.
Ad lib consumption
The primary measure of ad lib consumption was the amount of beer consumed (in milliliters). The entire sample consumed a mean of 696.5 mL (SD = 455.1). Individual amounts of consumption ranged from 26.0 to 1,420.0 mL. The mean ad lib BAC obtained during the session was 25.4 mg/100 mL (SD = 23.7) and ranged from 0.0 to 78.0 mg/100 mL. Thus, the sample displayed marked individual differences in measures of ad lib consumption.
In order to validate the ad lib beer consumption measure as an estimator of subjects’ typical quantity of alcohol consumption outside the laboratory, laboratory consumption measures were correlated with subjects’ self-reported drinking habits. These correlations are presented in Table 1. As expected, the laboratory measures of ad lib drinking significantly correlated with the typical quantity of alcohol consumed as indicated by subjects’ typical BAC, but not with the typical frequency of their alcohol use.
Relationship between impaired inhibitory control and ad lib consumption
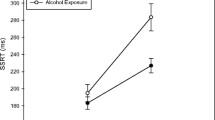
To test the hypothesis that greater impairment of inhibitory control under alcohol should predict greater levels of alcohol consumption, a bivariate regression analysis examined the relation between subjects’ ad lib drinking and their impairment of inhibitory control in response to alcohol. Ad lib consumption, assessed as the amount of beer (in milliliters) consumed, was treated as the dependent measure, and magnitude of impaired inhibitory control served as the independent (i.e., predictor) variable in the regression equation. The results of this regression are presented in Table 2. The analysis revealed a significant relationship between magnitude of impaired inhibitory control and ad lib consumption. Magnitude of impairment accounted for 20% of the variance in subjects’ ad lib consumption. Figure 2 plots this relationship and shows that those who displayed greater impairment of inhibitory control in response to alcohol also consumed more alcohol in the ad lib session. An outlier analysis revealed that no cases had undue influence or leverage based on Cook’s distance and Studentized residuals.

Relationship between participants’ magnitude of impaired inhibitory control under alcohol relative to placebo and the amount of beer consumed (in milliliters) in the ad lib consumption task. Slope is indicated by least squares regression line (solid line)
An additional bivariate regression analysis showed that magnitude of impaired inhibitory control also predicted BAC achieved during the ad lib session (Table 2). As Table 2 shows, alcohol impairment of inhibitory control accounted for a significant amount of variance in ad lib BAC. Those who displayed greater impairment of inhibitory control obtained higher BACs during the ad lib session.
It is also possible that those who drank more were simply more impaired by alcohol regardless of the behavioral measure. To address this possibility, individual differences in ad lib consumption were also examined in relation to individual differences in the degree to which alcohol impaired (i.e., slowed) drinkers’ reaction time on the cued go/no-go task. Difference scores were calculated in order to determine the degree to which reaction time was slowed under alcohol compared to placebo for each participant. A bivariate regression analysis revealed no significant relationship between alcohol impairment of reaction time and ad lib consumption (p = 0.88).
Basal levels of inhibitory control and trait impulsivity as predictors of ad lib consumption
It is also possible that greater alcohol consumption in the ad lib task could be a function of poor levels of inhibitory control in general, and not necessarily the degree to which inhibitory control was impaired by alcohol. The p-failures score in the placebo condition of the cued go/no-go task provides a measure of inhibitory control unaffected by alcohol, and so these scores were used to test this possibility. A regression analysis revealed no significant relationship between levels of inhibitory control under placebo and individual differences in ad lib consumption (p = 0.38).
Poor inhibitory control is also thought to underlie the broader trait of impulsivity, which is another potential factor that could be associated with increased ad lib consumption. This was tested by a regression analysis which revealed no significant relationship between ad lib consumption and impulsivity as measured by total BIS score (p = 0.76). The entire sample reported a total mean (SD) impulsivity score of 55.3 (7.2). Scores ranged from a minimum of 41.0 to a maximum of 71.0. Regression analyses were also conducted to test for possible relationships between ad lib consumption and each of the six BIS subscales. None of these correlations was found to be significant (ps > 0.05).
Discussion
This study examined the relationship between magnitude of alcohol impairment of inhibitory control and ad lib alcohol consumption. The predicted relationship was observed. Drinkers who exhibited greater impairment of inhibitory control in response to alcohol also consumed greater amounts of alcohol when given ad lib access. Moreover, individual differences in ad lib consumption were predicted specifically by impairment of inhibitory control and not by impairment of reaction time or baseline levels of inhibitory control or trait impulsivity. The specificity of this relationship is an important finding. This is the first study to examine alcohol consumption as a function of both acute impairment of inhibitory mechanisms and sober levels of inhibitory control. Evidence that consumption might be mediated by disinhibition in response to alcohol and not necessarily by the drinkers’ general sober levels of inhibitory control or trait impulsivity is a new finding that adds to the understanding of factors underlying individual differences in levels of alcohol consumption.
Furthermore, the findings were based on a well-validated laboratory assessment of typical drinking behaviors outside the laboratory. The ad lib consumption task provided a laboratory measure of abuse potential, and this measure has been used in the past to examine alcohol consumption behavior within a laboratory setting (Collins et al. 1996; Marczinski et al. 2005). These studies have demonstrated the validity of the ad lib consumption task as a measure of consumption patterns outside of the laboratory. The current study provided additional support for the validity of the task, in that ad lib consumption measures significantly correlated with typical BAC achieved outside the laboratory. Thus, individual differences in amounts of consumption on this task can be interpreted as possible indicators for abuse potential.
To our knowledge, this is one of few studies to provide laboratory-based evidence that acute alcohol-induced impairment of inhibitory control might be an important factor in abuse potential. Research on the role of cognitive processes in addiction has usually concerned how the individual’s cognitive state can contribute to alcohol abuse by triggering drinking episodes. For example, studies have examined how expectancies, implicit cognitions, and memories concerning alcohol effects can operate as precursors to consumption (Roehrich and Goldman 1995; Stein et al. 2000; Wiers and Stacy 2006). These cognitive events are present before the drinking episode is initiated. Similarly, studies that concern the role of disinhibition in alcohol and other drug abuse usually approach the problem from a trait perspective by considering disinhibition as an enduring stable attribute that is part of a personality construct, such as impulsivity (Sher and Trull 1994; Widiger and Smith 1994). By contrast, less research has examined how acute changes in cognitive states following alcohol consumption can also contribute to excessive use within the episode. The current study examined inhibitory control as a dynamic process that can be temporarily altered by the drug itself to increase the risk for abuse. For example, in a problem drinker, impaired inhibitory control following alcohol consumption could override the drinker’s intentions to limit alcohol intake, and therefore, increase risk for binge use. Often, drinkers report initial intentions of consuming only one or two drinks. However, they often proceed to drink to the point of gross intoxication. The current study suggests that such unintentional excessive consumption could be due to acute inability to inhibit drinking behavior once drinking has begun.
It is also important to consider the generalizability of these findings. One issue concerns the “threshold” dose at which alcohol will begin to impair the drinker’s inhibitory control. The conclusions of this study are based on the assumption that the impairment of inhibitory control observed at the BACs obtained in the active dose–challenge session (approximately 80 mg/100 mL) would be evident at the lower BACs obtained during consumption of the initial few drinks, such as in the ad lib test. Previous research has demonstrated that impairment of inhibitory control is a linear function of dose, and significant impairment has been shown at BACs as low as 50 mg/100 mL (Marczinski and Fillmore 2003). To our knowledge, alcohol impairment of inhibitory control has not been studied at BACs lower than 50 mg/100 mL, and therefore, it is not possible to state with certainty that impairment would be observed at the BACs observed in the ad lib session (mean = 25.4 mg/100 mL). However, it is reasonable to assume that some degree of impairment of inhibitory control is produced at lower BACs, which would be achieved following the initial consumption of as few as a couple of drinks.
Another issue concerns the generalizability of the findings to problem drinkers. The participants in this study were social drinkers with no history of alcohol dependence. Thus, it is unlikely that these drinkers regularly experience any severe loss of self-control concerning their alcohol consumption. However, the sample did include young drinkers who reported patterns of binge drinking. Early binge drinking is a risk factor for later alcohol abuse (Cloninger 1987), and greater sensitivity to the impairing effect of alcohol on inhibitory control could be an important factor underlying this risk.
It is also important to recognize that this is a correlational study. Impairment of inhibitory control accounts for only a small, albeit significant, proportion of the total variance in individual differences in alcohol consumption. Clearly, many other factors contribute to the individual differences in quantity of alcohol consumed during a drinking episode. Such factors include genetic predisposition for alcohol abuse (e.g., family history), other personality characteristics (e.g., sensation seeking), as well as situational factors (e.g., stress). Future research is needed to examine how impaired inhibitory control might interact with such factors to influence alcohol consumption.
In conclusion, this study provides evidence for a nonreward-based mechanism that might contribute to the abuse potential of alcohol. The majority of research examining the relationship between acute effects of alcohol and levels of consumption has centered around the rewarding effects of the drug (Koob 2003; Robinson and Berridge 1993), and there is little doubt that these rewarding effects play a substantial role in increasing levels of alcohol use. However, the current findings suggest the involvement of another factor resulting from alcohol consumption that may also play a role in determining individual differences in drinking patterns. Specifically, the impairing effect of alcohol on inhibitory control may be an additional means through which alcohol serves to promote abuse, independent of the positive rewarding effects of the drug.
References
Bates ME, Bowden SC, Barry D (2002) Neurocognitive impairment associated with alcohol use disorders: implications for treatment. Exp Clin Psychopharmacol 10:193–212
Cloninger CR (1987) A systematic method for clinical description and classification of personality variants. Arch Gen Psychiatry 44:573–588
Collins RL, Gollnisch G, Izzo C (1996) Drinking restraint and alcohol-related outcomes: exploring the contributions of beverage instructions, beverage content, and self-monitoring. J Stud Alcohol 57:563–571
de Wit H, Chutuape MA (1993) Increased ethanol choice in social drinkers following ethanol preload. Behav Pharmacol 4:29–36
de Wit H, Crean J, Richards JB (2000) Effects of d-amphetamine and ethanol on a measure of behavioral inhibition in humans. Behav Neurosci 114:830–837
DiChiara G, Acquas E, Tanda G (1996) Ethanol as a neurochemical surrogate of conventional reinforcers: the dopamine–opiod link. Alcohol 13:13–17
Fillmore MT (2001) Cognitive preoccupation with alcohol and binge drinking in college students: alcohol-induced priming of the motivation to drink. Psychol Addict Behav 15:325–332
Fillmore MT (2003) Drug abuse as a problem of impaired control: current approaches and findings. Behav Cogn Neurosci Rev 2:179–197
Fillmore MT (2007) Acute alcohol induced impairment of cognitive functions: past and present findings. International Journal of Disability and Human Development 6:115–125
Fillmore MT, Vogel-Sprott M (1998) Behavioral impairment under alcohol: cognitive and pharmacokinetic factors. Alcohol Clin Exp Res 22:1476–1482
Fillmore MT, Vogel-Sprott M (2000) Response inhibition under alcohol: effects of cognitive and motivational conflict. J Stud Alcohol 61:872–880
Fillmore MT, Rush CR (2001) Alcohol effects on inhibitory and activational response strategies in the acquisition of alcohol and other reinforcers: priming the motivation to drink. J Stud Alcohol 62:646–656
Fillmore MT, Blackburn J (2002) Compensating for alcohol-induced impairment: alcohol expectancies and behavioral disinhibition. J Stud Alcohol 63:237–246
Fillmore MT, Marczinski CA, Bowman AM (2005) Acute tolerance to alcohol effects on inhibitory and activational mechanisms of behavioral control. J Stud Alcohol 66:663–672
Finn PR, Kessler DN, Hussong AM (1994) Risk for alcoholism and classical conditioning to signals for punishment: evidence for a weak behavioral inhibition system? J Abnorm Psychol 103:293–301
Fowles DC (1987) Application of a behavioral theory of motivation to the concepts of anxiety and impulsivity. J Res Pers 21:417–435
Gray JA (1976) The behavioral inhibition system: a possible substrate for anxiety. In: Feldman MP, Broadhurst A (eds) Theoretical and experimental bases of the behavior therapies. Wiley, London, pp 3–41
Jentsch JD, Taylor JR (1999) Impulsivity resulting from frontostriatal dysfunction in drug abuse: implication for the control of behavior by reward-related stimuli. Psychopharmacology 146:373–390
Katz JL, Higgins ST (2003) The validity of the reinstatement model of craving and relapse to drug use. Psychopharmacology 168:21–30
Koob GF (2003) Neuroadaptive mechanisms of addiction: studies on the extended amygdala. Eur Neuropsychopharmacol 13:442–452
Koob GF, Le Moal M (1997) Drug abuse: hedonic homeostatic dysregulation. Science 278:52–58
Koob GF, Rocio M, Carrera A, Gold LH, Heyser CJ, Maldonado-Irizarry C et al (1998) Substance dependence as a compulsive behavior. J Psychopharmacol 12:39–48
Logan GD (1994) On the ability to inhibit thought and action: a user’s guide to the stop-signal paradigm. In: Dagenback D, Carr TH (eds) Inhibitory processes in attention, memory, and language. Academic, San Diego, pp 189–239
Logan GD, Cowan WB (1984) On the ability to inhibit thought and action: a theory of an act of control. Psychol Rev 91:295–327
Ludwig AM, Wikler A, Stark LH (1974) The first drink: psychobiological aspects of craving. Arch Gen Psychiatry 30:539–547
Lyvers M (2000) “Loss of control” in alcoholism and drug addiction: a neuroscientific interpretation. Exp Clin Psychopharmacol 8:225–249
Marczinski CA, Fillmore MT (2003) Preresponse cues reduce the impairing effects of alcohol on the execution and suppression of responses. Exp Clin Psychopharmacol 11:110–117
Marczinski CA, Bryant R, Fillmore MT (2005) The relationship between cognitive preoccupation with alcohol and alcohol use in male and female college students. Addiction Research and Theory 13:383–394
Marlatt GA, Demming B, Reid JB (1973) Loss of control drinking in alcoholics: an experimental analogue. J Abnorm Psychol 81:233–241
McKim WA (2007) Drugs and behavior: an introduction to behavioral pharmacology, 6th edn. Prentice Hall, New Jersey
Miller J, Schaffer R, Hackley SA (1991) Effects of preliminary information in a go versus no-go task. Acta Psychol 76:241–292
Mulvihill LE, Skilling TA, Vogel-Sprott M (1997) Alcohol and the ability to inhibit behavior in men and women. J Stud Alcohol 58:600–605
National Institute on Alcohol Abuse and Alcoholism (2004) NIAAA council approves definition of binge drinking. NIAAA Newsletter, No. 3, Winter 2004
Patton JH, Stanford MS, Barratt ES (1995) Factor structure of the Barratt Impulsiveness Scale. J Clin Psychol 51:768–774
Posner MI (1980) Orienting of attention. Q J Exp Psychol 32:3–25
Robinson TE, Berridge KC (1993) The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Rev 18:247–291
Roehrich L, Goldman M (1995) Implicit priming of alcohol expectancy memory processes and subsequent drinking behavior. Exp Clin Psychopharmacol 3:402–410
Schneider W, Eschman A, Zuccolotto A (2002) E-prime user’s guide. Psychology Software Tools, Pittsburgh, PA
Seltzer ML, Vinokur A, van Rooijen L (1975) A self-administered Short Michigan Alcoholism Screening Test (SMAST). J Stud Alcohol 36:117–126
Shaham Y, Shalev U, Lu L, de Wit H, Stewart J (2003) The reinstatement model of drug relapse: history, methodology, and major findings. Psychopharmacology 168:3–20
Sher KJ, Trull TJ (1994) Personality and disinhibitory psychopathology: alcoholism and antisocial personality disorder. J Abnorm Psychol 103:92–102
Stein KD, Goldman MS, Del Boca FK (2000) The influence of alcohol expectancy priming and mood manipulation on subsequent alcohol consumption. J Abnorm Psychol 109:106–115
Stewart J, de Wit H, Eikelboom R (1984) Role of unconditioned and conditioned drug effects in the self-administration of opiates and stimulants. Psychol Rev 91:251–268
Vogel-Sprott M (1992) Alcohol tolerance and social drinking: learning the consequences. Guilford, New York
Wiers RW, Stacy AW (2006) Implicit cognition and addiction: an introduction. In: Wiers RW, Stacy AW (eds) Handbook of implicit cognition and addiction. Sage, London, pp 1–8
Widiger TA, Smith GT (1994) Substance use disorder: abuse, dependence and dyscontrol. Addiction 89:267–282
Wise RA, Bozarth MA (1987) A psychomotor stimulant theory of addiction. Psychol Rev 94:469–492
Acknowledgement
This research was supported by grant R21 DA021027 from the National Institute on Drug Abuse and by grant R01 AA12895 from the National Institute on Alcohol Abuse and Alcoholism.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Weafer, J., Fillmore, M.T. Individual differences in acute alcohol impairment of inhibitory control predict ad libitum alcohol consumption. Psychopharmacology 201, 315–324 (2008). https://doi.org/10.1007/s00213-008-1284-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-008-1284-7