
Abstract
Rationale
Individual differences in responsiveness to caffeine occur even within a caffeine-consuming population, but the factors that mediate differential responsiveness remain unclear.
Objectives
To compare caffeine’s effects on performance and mood in a group of high vs moderate consumers of caffeine and to examine the potential role of subjective awareness of the effects of caffeine in mediating any differential responsiveness.
Materials and methods
Two groups of regular caffeine consumers (<200 mg/day and >200 mg/day) attended two sessions at which mood and cognitive functions were measured before and 30 min after consumption of 400-mg caffeine or placebo in a capsule. Cognitive tests included visual information processing, match-to-sample visual search (MTS) and simple and choice reaction times. Post-session questionnaires asked participants to describe any perceived effect of capsule consumption.
Results
High consumers, but not moderate consumers, demonstrated significantly faster simple and choice reaction times after caffeine relative to placebo. These effects were not attributable to obvious group differences in withdrawal or tolerance because there were no group differences in baseline mood or in reports of negative affect after caffeine. Instead, the high consumers were more likely to report experiencing positive effects of caffeine, whereas the moderate consumers were more likely to report no effect.
Conclusions
The sensitivity of caffeine consumers to the mood- and performance-enhancing effects of caffeine is related to their levels of habitual intake. High caffeine consumers are more likely than moderate consumers to perceive broadly positive effects of caffeine, and this may contribute to their levels of use.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The mood-enhancing effects of caffeine have been well documented (e.g. see Smith 2002 for review). However, there is evidence to suggest that not all habitual caffeine consumers report such effects of caffeine. Evans and Griffiths (1992) stratified a group of regular caffeine consumers into caffeine “choosers” and “non-choosers” based on a caffeine-vs-placebo choice procedure. In tests of the subjective effects elicited by caffeine, the “choosers” reported more positive effects of caffeine on mood (e.g. increased vigor, friendliness, energy) in comparison with the “non-choosers” who tended to report negative subjective effects (e.g. tension, anxiety, jitteriness). The observation that the “choosers” tended to show negative subjective effects of placebo (e.g. headache and fatigue) relative to “non-choosers” indicates that the “choosers” might have experienced greater caffeine withdrawal symptoms compared with the “non-choosers”, and this influenced their responding. This is consistent with the observation that the facilitatory effects of caffeine are often observed in deprived consumers of caffeine, but not in non-consumers (James and Rogers 2005; Rogers et al. 2003; Smit and Rogers 2002). However, it is also possible that the caffeine “choosers” had developed tolerance to the aversive, anxiety-related effects of caffeine that occur at high doses (Jacobson and Thurman-Lacey 1992), which differentiated their responses from those of “non-choosers”.
Smit and Rogers (2000) have also argued that levels of daily caffeine intake may influence the effects of caffeine on cognitive performance. They reported that positive effects of caffeine on cognitive performance were more robust in a group of high caffeine consumers (>200 mg/day) relative to a group of low consumers (<100 mg/day). However, because all participants were overnight withdrawn from caffeine, it was not possible to determine whether this was due to a greater negative impact of withdrawal in the high consumers or to differences in sensitivity to the effects of caffeine. In a similar vein, previous research from our laboratory has highlighted individual differences in the effects of caffeine on cognition and mood in a group of regular caffeine consumers: Not all participants who received a 400-mg dose of caffeine showed significant improvements in responding (Attwood 2006). Interestingly, it has also been shown that individuals consuming high levels of caffeine (>350 mg/day) demonstrate an attentional bias for caffeine-related words, whereas moderate consumers (100–250 mg/day) and non-consumers do not (Yeomans et al. 2005). Moreover, Yeomans et al. (2005) found that attentional bias in the high consumers correlated both with reported levels of habitual caffeine intake and caffeine craving.
Hence, although there is evidence to suggest that individual differences in habitual consumption of caffeine influence the response to caffeine, the factors that mediate this differential responsiveness remain unclear. The aim of the present study was, firstly, to examine the effect of habitual consumption of caffeine on both cognitive performance and conventional mood measures. It was predicted that only the high consumers would demonstrate significant improvements in cognitive performance after caffeine. Secondly, our aim was to distinguish between several possible explanations for this differential responsiveness by taking extensive measures of the effects of caffeine on mood in both moderate and high consumers and asking participants about their perceptions of any effects experienced at the end of the test.
The actual and perceived effects of a 400-mg dose of caffeine and placebo were measured in moderate- and high caffeine consumers. All participants were regular tea and/or coffee drinkers, and a cut-off consumption criterion of 200 mg/day of caffeine (Smit and Rogers 2000) was used to distinguish the moderate (<200 mg/day) from high (>200 mg/day) consumer groups. Because, in our laboratory, a dose of 400 mg of caffeine (but not 250 mg) has produced facilitatory effects on cognition and mood compared with placebo (Attwood 2006) and significant improvements in performance and arousal have previously been demonstrated after ingestion of 400 mg of caffeine (e.g. Flaten et al. 2003; Loke 1988; Jacobson and Edgley 1987), this dose was selected as being likely to produce robust effects on performance. Furthermore, because we wanted to test whether differential tolerance might underlie any differences in responding between moderate and high consumer groups, we chose a relatively high dose of caffeine that has been shown previously to induce some aversive, anxiety-related effects (Childs and de Wit 2006; Jacobson and Thurman-Lacey 1992).
The cognitive test battery used to measure performance comprised tasks that have been shown to be sensitive to the effects of caffeine. Measures of both simple reaction time (SRT) and choice reaction time (CRT) were taken; many studies have reported decreased reaction times over a wide range of caffeine doses (e.g. Brice and Smith 2002; Smit and Rogers 2000; Smith et al. 1994a,b; Lieberman et al. 1987; Roache and Griffiths 1987). In addition, a rapid visual information processing task (RVIP) and pattern detection task were chosen because caffeine has been shown to improve both speed and accuracy in these tests (Yeomans et al. 2002; Smit and Rogers 2000; Durlach 1998; Warburton 1995; Frewer and Lader 1991). Visual analogue scales (VAS) were used to measure subjective mood effects and were adapted from a questionnaire that has detected significant effects of caffeine on mood (Richardson et al. 1995).
Materials and methods
Participants
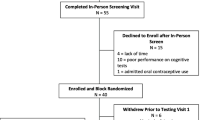
Forty-nine students and staff from the University of Birmingham, UK (18 male; mean age 23.2 years, range 18–41 years) responded to poster advertisements to take part in a study examining the cognitive effects of over-the-counter drugs in return for cash or course credits. Participants were screened by means of an e-mailed intake questionnaire to ensure that all were non-smoking, habitual caffeine consumers. Three participants were excluded due to not turning up for a scheduled session, and one participant was excluded due to being unable to swallow the capsule; thus, 45 participants were included in the analyses. The participants were separated into two groups (moderate vs high consumers) whose daily caffeine intake was less than or greater than 200 mg/day, respectively (see Table 1). To minimize expectancy effects, participants were informed that they could receive one of several possible substances (paracetamol, caffeine, ibuprofen or aspirin).
Experimental design
Each participant attended two sessions (caffeine and placebo). Inter-session intervals did not fall below 24 h or exceed 14 days. All testing took place between 1200 and 1800 h, and participants attended their sessions at approximately the same time of day. Test times were balanced between consumer groups. Capsule administration was double blind, and approximately equal groups received placebo first vs caffeine first (14 moderate and 9 high consumers had placebo first, and 10 moderate and 12 high consumers had caffeine first). Before each session, participants were asked to abstain from all psychoactive substances from 2300 h the previous night. To promote compliance, a reminder e-mail was sent the day before each session, a saliva assay (which was not analysed) was taken on arrival, and a form confirming abstinence was signed.
Capsule administration
Caffeine (400 mg; Sigma-Aldrich, Poole, UK) was administered in a gelatin capsule (Shionogi Qualicaps, size-00, Madrid, Spain) with water. The placebo capsule contained arrowroot (Supercook, Leeds, UK).
Cognitive tasks
The cognitive tasks were from the Cambridge Neuropsychological Test Automated Battery (CANTAB; Cambridge Cognition, Cambridge, UK). To keep the length of the test session to a reasonable duration, baseline testing on each session comprised the simple reaction time and choice reaction time tasks only.
Simple reaction time
The simple reaction time task comprised two experimental blocks, each of 15 trials. The stimulus was a small yellow spot, which was presented for 250 ms inside a white circle that remained centrally on screen throughout the test. Each trial began with the participants depressing the press-pad key until the yellow spot appeared, at which point they were required to touch the screen (inside the white circle) as quickly as possible. The next trial did not begin until the participants had once again depressed the press-pad key.
Choice reaction time
The choice reaction time task comprised four experimental blocks (15 trials each) in which five white circles were arranged around a central point on the screen. The white circles were fixed on screen throughout the test. For each trial, the yellow spot appeared in one of these five circles, and participants had to touch this circle as quickly as possible.
For both reaction time tests, the inter-trial interval varied randomly between 750 and 2,250 ms to reduce anticipatory responding. Decision and movement latencies were measured separately. Both tasks were preceded by an unanalysed practice block of ten trials.
Match-to-sample visual search
An abstract pattern (target) appeared centrally on the computer screen. After a 1.5-s interval, distracter patterns appeared in boxes surrounding this central pattern. Within the array of distracters, one pattern was an identical match to the central target. To initiate each trial, a press-pad key was depressed until the identical pattern was identified. At this point, the participants were required to move their hands from the press pad to touch the identical pattern on screen. If the response was incorrect (indicated by a red cross on the screen), participants were asked to continue choosing from the distracter patterns until they had chosen the correct one. There were three levels of difficulty that differed according to the number of distracters: two (level 1), four (level 2) or eight (level 3). Reaction duration, movement duration and errors were recorded. The main task was preceded by a practice block of three trials (one per level), but these data were not analysed.
Rapid visual information processing
A series of single digits appeared sequentially on the computer screen, and participants were required to respond, via a press pad, whenever they identified one of three three-digit number strings (3-5-7; 2-4-6; 4-6-8). Each digit was displayed for 600 ms before being replaced with the next. The task ran for six consecutive blocks, each comprising nine target strings, although the data from the first block were not analysed (total task time, 6 min). A practice version of 2 min also preceded each test run.
Mood measures
Participants completed a pen-and-paper mood questionnaire on arrival and also immediately before and after completion of the computer test battery (approximately 30 and 55 min post-capsule ingestion). Seventeen adjectives were rated on 100-mm VAS (adapted from Rogers et al. 1995) from 0 (not at all) to 100 mm (extremely): “Friendly”, “Headache”, “Alert”, “Cheerful”, “Drowsy”, “Anxious”, “Energetic”, “Angry”, “Muddled”, “Calm”, “Tired”, “Dejected”, “Tense”, “Clear-headed”, “Relaxed”, “Thirsty” and “Jittery”. Participants were told to consider each line as the extreme spectrum of that emotion and to transect the line appropriately to show how they were feeling at that specific moment.
Post-session questionnaires
The post-session questionnaire asked participants to report any perceived effects of the capsule. First, they were asked to tick “yes” or “no” to the question “Did you feel any effect of the capsule?” If they ticked “yes”, space was provided for participants to describe these effects. For analysis, these responses were classified as either positive, negative or no effect. The positive responses mentioned were alertness, cheerfulness, increased well-being, decreased drowsiness/tiredness and decreased headache. The negative responses mentioned were anxiety, tension, jitteriness, deflated mood, headache and nausea. “No effect” was recorded when participants ticked “no” to the first part of the question.
Procedure
On arrival, participants confirmed overnight abstinence from any psychoactive substances and provided a saliva sample. A baseline mood questionnaire and practice on the SRT and CRT (two blocks each) were completed immediately before capsule ingestion. An interval of 30 min then elapsed to allow for drug absorption, during which time the participants were asked to sit quietly (reading material, e.g. current periodicals, was provided). After this interval, the experimenter returned to administer the tests in the following order: second mood questionnaire, RVIP, MTS, SRT, CRT, third mood questionnaire. Finally, participants completed the post-session questionnaire.
Statistical analyses
Statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS; version 11.5) for Windows. For SRT and CRT movement duration data, reaction times below 100 ms or more than three standard deviations above an individual’s mean score were deemed outliers and removed. There were no differences in the mood changes observed over 30–50 min vs the changes over 0–50 min, so only the changes from baseline to 50 min (i.e. the whole test session) are presented.
Independent t-tests examined between-group differences at baseline for reaction time performance and mood. Gender and order of treatment (capsule to be consumed) were included as blocking factors in these analyses but did not influence the outcome.
Two-way analyses of variance (ANOVAs) with group (high consumer, moderate consumer) and drug (caffeine, placebo) as between- and within-subject factors, respectively, were conducted on data from the cognitive tasks. For SRT, CRT and MTS, reaction times were separated into two scores: reaction duration (i.e. time between presentation of distracters and movement from the press pad) and movement duration (time between movement from the press pad key to touching the correct pattern on screen). The number of errors was also analysed for the RVIP and MTS tasks. A priori planned comparisons were conducted to analyse the effect of capsule on mood and performance scores in the high and moderate consumer groups. Because baseline scores were found to correlate with the test measures, baseline score was included as a covariate where possible. Two participants were omitted from the analyses of the SRT and CRT experimental trials due to corrupt data.
For the mood ratings, a principle components analysis was performed using varimax rotation. Analysis of the 17 mood items revealed five factors with eigenvalues greater than 1 that accounted for 69% of the variance. Items with loadings greater than 0.5 were retained on each factor unless the same items had a loading greater than 0.4 on another factor. The five factors were: “Tense negative mood” (items loaded onto this factor were: Tense, Jittery, Angry, Dejected), “Sleepiness/hydration” (items loaded onto this factor were: Drowsy, Tired, Thirsty), “General positive mood” (items loaded onto this factor were: Energetic, Cheerful, Friendly) “Mental clarity” (items loaded onto this factor were: Alert, Clear-headed, Muddled) and “Mental repose” (items loaded onto this factor were: Calm, Relaxed). Participant’s scores for each factor were calculated by adding the scores of all the items loading onto the factor. Two ratings did not load clearly onto any factor (anxiety and headache) and were analysed separately. A two-way ANOVA was conducted on each mood factor with consumer group as a between-subjects factor. This analysis reduced the number comparisons, thus reducing the likelihood of a Type II error due to conservative corrections for multiple comparisons (Bonferroni correction).
Gender and order of capsule administration were included as blocking factors in the analyses of performance and mood; however, their inclusion did not change an outcome, so these results are not reported. Correlation analyses also showed that time since having eaten and time of day of testing did not correlate with the test measures. All post-hoc multiple comparisons employed the Bonferonni correction.
Results
Participant characteristics
Some body mass index (BMI) data were missing due to six participants choosing not to complete the personal details form in full, therefore the BMI analysis comprised data from 39 participants. The moderate and high consumer groups did not differ significantly in age (t = 0.45; df = 43; p > 0.05) or BMI (t = 0.44; df = 37; p > 0.05). There was a significant difference between the two groups in daily levels of caffeine consumption (t = −7.50; df = 43; p < 0.0001; see Table 1).
CANTAB test battery
Simple Reaction Time
At baseline, there were no significant differences between groups on SRT reaction duration or movement duration (Table 2). There were no significant main effects of caffeine or group on SRT reaction duration or movement duration. However, there were significant caffeine-by-group interactions for both SRT reaction duration [F(1, 40)=4.59; p < 0.05] and movement duration [F(1, 40)=4.57; p < 0.05]. Paired t-tests revealed that the high consumers (t = 2.80; df = 20; p < 0.05), but not the moderate consumers (t = 0.16; df = 21; p > 0.05), were significantly faster on SRT reaction duration after caffeine compared with placebo (Fig. 1a). For movement duration, the moderate consumers were significantly slower after caffeine relative to placebo (t = 2.78; df = 21; p < 0.05). In contrast, the high consumers were marginally faster after caffeine, although this difference was not significant (t = 0.74; df = 20; p > 0.05; Fig. 1a).

a Mean SRT reaction (RD) and movement (MD) durations (ms) for moderate (<200 mg) and high (>200 mg/day) consumer groups. b Mean CRT reaction (RD) and movement (MD) durations (ms) for moderate (<200 mg/day) and high (>200 mg/day) consumer groups. In all cases, error bars represent +1 SEM. Asterisk Significantly different from placebo, p < 0.05
Choice Reaction Time
For CRT, there were no significant differences at baseline between groups for either reaction duration or movement duration (Table 2). There was a significant main effect of caffeine for CRT reaction duration [F(1, 40)=8.58; p < 0.01], but no effect of group [F(1, 40)=1.56; p > 0.05] nor a significant interaction [F(1, 40)=1.12; p > 0.05]. Paired t-tests showed that only the high consumers were significantly faster after caffeine compared with placebo (t = 2.78; df = 20; p < 0.05; Fig. 1b). For CRT movement durations, there were no significant main effects of caffeine or group, nor was there a significant interaction between group and capsule (Fig. 1b).
MTS and RVIP
There were no significant main effects of capsule or group on any level of MTS reaction and movement durations (see Table 3). There was one significant interaction between group and capsule for level 3 movement duration [F(1, 43)=4.42; p < 0.05]. The group means suggested that the moderate consumers were slower after caffeine relative to placebo, with little difference for the high consumers; however, this difference did not reach significance (t = −1.84; df = 23; p > 0.05). There were no other significant interactions.
There were no errors for level 1 MTS performance; therefore, only errors for levels 2 and 3 were analysed. There were no significant main effects or significant interaction for level 2 errors. There was a significant effect of caffeine for level 3 errors [F(1, 43)=5.17; p < 0.05] due to participants making fewer errors after caffeine than placebo. There was no main effect of group and no significant interaction (see Table 3). Paired t-tests revealed that the moderate consumers made significantly fewer errors after caffeine relative to placebo (t = 2.72; df = 23; p < 0.02). After caffeine, the number of errors made by the moderate consumers at level 3 was similar to the performance shown by the higher consumers in both drug conditions.
There were no significant main effects or significant interactions for RVIP reaction time or errors. A blocked analysis was conducted by splitting the data into two equal blocks of 18 targets. For reaction time, there was a significant effect of block [F(1, 43)=4.46; p < 0.05] and a trend towards a block by capsule interaction [F(1, 43)=2.9; p = 0.097] suggesting that the deterioration in performance across blocks was most prominent in the placebo condition. Although the caffeine-by-block-by-group interaction did not reach significance [F(1, 43)=2.30; p > 0.05], inspection of the means suggests that this deterioration was counteracted by caffeine in the high but not moderate consumers.
Subjective effects
There were no significant group differences on any of the mood factors at baseline (Table 2). Caffeine, relative to placebo, significantly increased ratings of “tense negative mood” [F(1, 43)=9.30; p < 0.005] and “anxious” [F(1, 43)=4.68; p < 0.05] and decreased ratings of “mental repose” [F(1, 43)=9.31; p < 0.005] and “sleepiness” [F(1, 43)=6.88; p < 0.02]. There were no other significant main effects of caffeine. There were no significant main effects of consumer group.
There was a near significant caffeine-by-group interaction for ratings of “sleepiness” [F(1, 43)=7.25; p = 0.01]. A priori t-tests showed that the high consumers, but not the moderate consumers, reported significant reductions in “sleepiness” (t = −3.54; df = 20; p < 0.003) relative to placebo (Fig. 2).

Change (mm) in ratings of “tense negative mood”, “anxious”, “mental repose” and “sleepiness” for the caffeine and placebo sessions in the moderate and high caffeine consumer groups. Asterisk Significantly different from placebo, p < 0.01
Post-session questionnaires
There were no differences between groups in terms of the number of participants reporting negative effects of caffeine. In contrast, the high consumers were significantly more likely to report positive consequences of caffeine, and the moderate consumers were more likely to report “no effect” [χ 2 (2, N = 45) = 7.92; p < 0.05; see Table 4].
Discussion
The results indicate that high-caffeine consumers (>200 mg/day) are more likely than moderate-caffeine consumers (<200 mg/day) to respond to caffeine. We found that high, but not moderate consumers, showed significant benefits of caffeine, relative to placebo on SRT and CRT, and a reduction in rated sleepiness. Furthermore, the high consumers were more likely to perceive positive effects of caffeine, as measured by post-session written reports, suggesting that level of habitual intake may mediate variations between people in sensitivity and/or responsiveness to the positive effects of caffeine.
There are several possible explanations for the differential responsiveness of high and moderate consumers to caffeine. First, the high consumers may experience greater levels of withdrawal during abstinence, which is reversed by caffeine (James and Rogers 2005). However, analyses of baseline cognitive and mood ratings found no significant differences between high and moderate consumers that would indicate obvious differences in withdrawal symptoms. Griffiths et al. (1990) suggest that measurement of caffeine withdrawal should involve several different measures and should take place over different time points, perhaps implying that more extensive measurement of pre-session mood may have identified differences in withdrawal symptoms. Considering the sensitivity of the VAS to pick up post-caffeine mood fluctuations, there is no reason to expect sensitivity shortcomings with these measures at baseline, and evidence of a caffeine withdrawal state has previously been detected using the same items (Rogers et al. 1995).
Alternatively, the moderate consumers may have experienced aversive effects of caffeine to which the high consumers had developed tolerance (Evans and Griffiths 1992). However, the post-consumption mood measures demonstrated that all participants showed evidence of increases in tense negative mood and anxiety after caffeine and a reduction in mental repose, and analysis of the post-session questionnaire (which examined participants’ perceptions of the effects of capsule ingestion) showed that the two groups did not differ in their reports of negative effects. This suggests that the group differences were not due to stronger experiences of aversive effects among the moderate consumers. In fact, compared with the high consumers, the moderate consumers were less likely to report positive effects and more likely to report perceiving no effect of the capsule. It is possible that the stronger responses of the high consumers are due to greater sensitivity to the positive effects of caffeine, and this in turn might influence their level of caffeine consumption. It would therefore be informative to assess whether positive effects of caffeine are still perceived in the absence of tolerance, e.g. in a group of fully withdrawn high consumers.
The present data suggest that experiencing positive effects of caffeine is not necessary for the maintenance of caffeine use, as the moderate consumers still drink caffeinated beverages every day. For these moderate consumers, consumption might be maintained by other factors, such as the association of the drink with environmental reinforcers such as social interactions or breaks from work, or perhaps mere exposure to tea or coffee is sufficient to generate liking (Zajonc 1968) and, consequently, to maintain consumption. Alternatively, the moderate consumers may have expectations regarding the positive effects of caffeine that influence their choice of beverage.
We found no significant effects of caffeine on RVIP speed or accuracy. It is possible that the 6-min RVIP task used in this study was not long enough to reveal significant effects of caffeine. It may also be relevant that, in our version of the task, participants were required to identify specific strings of numbers; in other versions of the task, the target is more typically any string of odd or even numbers (Yeomans et al. 2002; Smit and Rogers 2000). Nevertheless, in the present study, RVIP scores slowed across the two time blocks in all conditions except for the high consumers after caffeine, suggesting that caffeine may have reduced task fatigue among the high consumers only. This is consistent with other reports that caffeine can offset a natural deterioration in performance in tasks requiring sustained attention (Frewer and Lader 1991).
There were significant effects of caffeine on level 3 of the MTS task in the moderate consumers: Relative to placebo, the moderate consumers made fewer errors after caffeine. In comparison, the high consumers did not show effects of caffeine on any level of the task. However, the moderate consumers were also slower after caffeine on level 3 of this task, and the number of errors made was reduced only to the level of the high consumers, suggesting that their increased accuracy on the caffeine session may have reflected a speed–accuracy trade-off. The moderate consumers also had slowed CRT movement durations after caffeine, suggesting that caffeine may have had a detrimental effect on motoric control in moderate consumers. It is possible that this reflects the increased tense/negative responses reported by all consumers after caffeine that was not offset by positive effects in the moderate compared to the high consumers.
These findings have implications for caffeine researchers who group caffeine consumers together as a single homogenous sample and may explain some of the variability in reports of the effects of caffeine. Although many studies have reported significant effects of caffeine on mood and cognitive performance, some studies have found little or no effect on these measures (e.g. Watson et al. 2000; Smith et al. 1994a,b, 1997; Bruce et al. 1986; Kuznicki and Turner 1986). Methodological issues have often been cited to explain these null effects. However, the present data suggest that not taking account of a consumer’s habitual level of caffeine consumption may reduce the likelihood of detecting caffeine effects. In addition, the present results suggest that data collected from high caffeine consumers are not necessarily representative of the effects of caffeine in moderate consumers, and vice versa.
In summary, these findings suggest that caffeine consumers differ in their psychomotor and subjective responses to caffeine. This may be, at least in part, due to a heightened responsiveness and perception of the positive effects of the drug in high consumers, which, in turn, may drive their high levels of use. Why individuals should differ in their sensitivity to the positive effects of drugs is not clear, but evidence suggests that individual variations in metabolism could be important (e.g. Grant et al. 1983). Further research is needed to ascertain whether the greater responsiveness of the high consumers is a consequence of chronic self-administration of high daily doses of caffeine or whether their high levels of consumption are driven by a heightened sensitivity to caffeine’s positive effects.
References
Attwood AS (2006) Conditioned psychomotor effects of caffeine in humans. Unpublished PhD Thesis, University of Birmingham
Brice CF, Smith AP (2002) Effects of caffeine on mood and performance: a study of realistic consumption. Psychopharmacology 164:188–192
Bruce M, Scott N, Lader M, Marks M (1986) The psychopharmacological and electrophysiological effects of single doses of caffeine in healthy human subjects. Br J Clin Pharmacol 22:81–87
Childs E, de Wit H (2006) Subjective, behavioral, and physiological effects of acute caffeine in light, nondependent caffeine users. Psychopharmacology 185:514–523
Durlach PJ (1998) The effects of a low dose of caffeine on cognitive performance. Psychopharmacology 140:116–119
Evans SM, Griffiths RR (1992) Caffeine tolerance and choice in humans. Psychopharmacology 108:51–59
Flaten MA, Aasli O, Blumenthal TD (2003) Expectations and placebo responses to caffeine-associated stimuli. Psychopharmacology 169:198–204
Frewer LJ, Lader M (1991) The effects of caffeine on two computerized tests of attention and vigilance. Hum Psychopharmacol 6:119–128
Grant DM, Tang BK, Kalow W (1983) Variability in caffeine metabolism. Clin Pharmacol Ther 33:591–602
Griffiths RR, Evans SM, Heishman SJ, Preston KL, Sannerud CA, Wolf B, Woodson PP (1990) Low-dose caffeine physical dependence in humans. J Pharmacol Exp Ther 255:1123–1131
Jacobson BH, Edgley BM (1987) Effects of caffeine on simple reaction time and movement time. Aviat Space Environ Med 58:1153–1156
Jacobson BH, Thurman-Lacey SR (1992) Effects of caffeine on motor performance by caffeine-naïve and -familiar subjects. Percept Mot Skills 74:151–157
James JE, Rogers PJ (2005) Effects of caffeine on performance and mood: withdrawal reversal is the most plausible explanation. Psychopharmacology 182:1–8
Kuznicki JT, Turner LS (1986) The effects of caffeine on users and non-users. Physiol Behav 37:397–408
Lieberman HR, Wurtman RJ, Emde GG, Roberts C, Coviella ILG (1987) The effects of low doses of caffeine on human performance. Psychopharmacology 92:308–312
Loke WH (1988) Caffeine effects on mood and memory. Physiol Behav 44:367–372
Richardson NJ, Rogers PJ, Elliman NA, O’Dell RJ (1995) Mood and performance effects of caffeine in relation to acute and chronic caffeine deprivation. Pharmacol Biochem Behav 52:313–320
Roache JD, Griffiths RR (1987) Interactions of diazepam and caffeine: behavioral and subjective dose effects in humans. Pharmacol Biochem Behav 26:801–812
Rogers PJ, Martin J, Smith C, Heatherley SV, Smit HJ (2003) Absence of reinforcing, mood and psychomotor performance effects of caffeine in habitual non-consumers of caffeine. Psychopharmacology 167:54–62
Rogers PJ, Richardson NJ, Elliman NA (1995) Overnight caffeine abstinence and negative reinforcement of preference for caffeine-containing drinks. Psychopharmacology 120:457–462
Smit H, Rogers PJ (2000) Effects of low doses of caffeine on cognitive performance, mood and thirst in low and higher caffeine consumers. Psychopharmacology 152:167–173
Smit H, Rogers PJ (2002) Effects of caffeine on mood. Pharmacopsychoecologia 15:231–257
Smith A (2002) Effects of caffeine on human behaviour. Food Chem Toxicol 40:1243–1255
Smith A, Kendrick A, Maben A (1994a) Effects of breakfast and caffeine on cognitive performance, mood and cardiovascular functioning. Appetite 22:39–55
Smith A, Maben A, Brockman P (1994b) Effects of evening meals and caffeine on cognitive performance, mood and cardiovascular functioning. Appetite 22:57–65
Smith A, Whitney H, Thomas M, Perry K, Brockman P (1997) Effects of caffeine and noise on mood, performance and cardiovascular functioning. Hum Psychopharmacol 12:27–33
Warburton DM (1995) Effects of caffeine on cognition and mood without caffeine abstinence. Psychopharmacology 119:66–70
Yeomans MR, Ripley T, Davies LH, Rusted JM, Rogers PJ (2002) Effects of caffeine on performance and mood depend on level of caffeine abstinence. Psychopharmacology 164:241–249
Yeomans MR, Javaherian S, Tovey HD, Stafford LD (2005) Attentional bias for caffeine-related stimuli in high but not moderate or non-caffeine consumers. Psychopharmacology 181:477–485
Watson JM, Lunt MJ, Morris S, Weiss MJ, Hussey D, Kerr D (2000) Reversal of caffeine withdrawal by ingestion of a soft beverage. Pharmacol Biochem Behav 66:15–18
Zajonc RB (1968) Attitudinal effects of mere exposure. J Pers Soc Psychol 9:1–27
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Attwood, A.S., Higgs, S. & Terry, P. Differential responsiveness to caffeine and perceived effects of caffeine in moderate and high regular caffeine consumers. Psychopharmacology 190, 469–477 (2007). https://doi.org/10.1007/s00213-006-0643-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-006-0643-5