
Abstract
Objective
This study evaluated whether alcohol attentional bias is an artifact of excessive drinkers’ impaired cognitive functioning, which adversely affects their performance on the classic Stroop test (a measure of inhibitory control) and the Shipley Institute of Living Scale (SILS; a measure of verbal and abstraction ability). Both tests measure aspects of executive cognitive functioning (ECF).
Methods
Social drinkers (N=87) and alcohol-dependent drinkers (N=47) completed a measure of alcohol consumption, classic and alcohol-related Stroop tests, and the SILS.
Results
A multivariate analysis of variance (MANOVA) showed that the dependent drinkers were poorer on the cognitive measures (SILS scores and classic Stroop interference) and had greater alcohol attentional bias than the social drinkers. An analysis of covariance (ANCOVA) in which the cognitive measures were controlled showed that the dependent drinkers’ greater alcohol attentional bias was not an artifact of their poorer cognitive performance.
Conclusion
The results are discussed in terms of cognitive–motivational models, which suggest that excessive drinking sensitizes alcohol abusers’ attentional responsiveness to alcohol-related stimuli to a degree that exceeds the adverse effects of alcohol on their general cognitive functioning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
People who abuse alcohol are often unaware of the factors that influence their decisions to drink (McCusker 2001; Wiers et al. 2002), leading some authors to conclude that alcohol abusers have little control over their drinking (Lyvers 2000; Skutle and Berg 1987). Drinkers’ automatic reactivity to alcohol stimuli is one of the mechanisms responsible for their lack of control (e.g., Tiffany 1990). It manifests itself as (a) a persistent preoccupation with alcohol (McCusker 2001; Roberts and Koob 1997) and (b) drinking alcohol despite awareness of the negative consequences of doing so (Roberts and Koob 1997).
Automatic reactions to stimuli cannot occur independently of a person’s attentional system. From the multitude of stimuli impinging on an individual’s sensory–perceptual system, attentional mechanisms filter in the most salient stimuli for further cognitive processing (MacLeod and MacDonald 2000). Attentional bias occurs when the attentional channeling is directed toward emotionally valued stimuli despite an individual’s efforts to ignore them (Williams et al. 1996). For example, when passing a liquor store, an alcohol abuser might be unable to ignore the alcohol products displayed in the window. Once the distraction has begun, it can activate mechanisms that eventuate in the act of drinking (Tiffany 1990). Because of its theoretical and applied implications, disorder-specific attentional bias has become an important topic of research (Williams et al. 1996).
Various paradigms have been used to study alcohol-related cognitive biases, examples of which include memory association (e.g., Stacy 1997), implicit association (e.g., Wiers et al. 2002), and knowledge acquisition (e.g., Pothos and Cox 2002) tasks. There are also paradigms that are specifically used to assess attentional bias for alcohol-related stimuli. They include dot-probe (Duka and Townshend 2004), flicker (Jones et al. 2003), and dual-task (Waters and Green 2003) paradigms. A modified version of the classic Stroop task (Stroop 1935), the emotional Stroop test, is particularly sensitive to attentional bias (Williams et al. 1996). An emotional Stroop test contains emotionally salient (e.g., alcohol-related) words and emotionally neutral words (e.g., building-related items) that are presented in different colors; the participant’s task is to name the colors while ignoring the meaning of the words. Attentional bias, or interference, occurs when participants color name the salient words more slowly than the neutral ones. Many studies have used this test to uncover cognitive processes underlying various kinds of psychopathology (see Williams et al. 1996), including alcohol and other substance abuse (Cox et al. 2005). Individuals with a specific psychopathology take longer to color name words related to their disorder than disorder-unrelated words. Disorder-related versions of the Stroop test are referred to as the emotional Stroop (Williams et al. 1996) because disorder-related stimuli are emotionally salient to people with the disorder.
The alcohol Stroop test contains alcohol-related and neutral words; on it, both alcohol-dependent drinkers and heavy social drinkers show attentional bias for the alcohol stimuli (Cox et al. 2005). There have been various explanations to account for interference by alcohol-related stimuli, including ones related to participants’ mood state, their relative speed of processing ink colors and word meanings, and their neural sensitization to alcohol-related stimuli. However, the strongest support is for explanations based on the emotional salience and concern-relatedness of the stimuli for individual participants (see Cox et al. 2005). According to this view, clinical samples process disorder-related stimuli differently than other individuals because the stimuli have positive or negative incentive value for clinical participants (e.g., Williams et al. 1996). Support comes from the observation that disorder-related attentional bias is reduced following successful treatment (e.g., Mogg et al. 1995; Watts et al. 1986).
Both animal (e.g., Koob 2003) and human (e.g., Robinson and Berridge 2003) models provide evidence that a history of alcohol abuse is associated with changes in brain organization and that the brain systems that are altered include neural circuits involved in incentive motivation and reactions to reward. Robinson and Berridge argue that although implicit S4–S associations activate this circuitry, the associations themselves can remain normal, even in addicted individuals. However, the neural system generates incentive salience, which is abnormal and leads to pathological “wanting” in addicted individuals.
Robinson and Berridge further argue that reactions to alcohol-related cues, which contribute to alcohol wanting, are mediated by alcohol-induced dysfunctions in the prefrontal cortical systems that are involved in emotional regulation, decision-making, judgment, and inhibitory processes. These processes are part of a network of executive cognitive functions (ECF; Bunge et al. 2000; Moselhy et al. 2001; Mantere et al. 2002). ECF is important in situations requiring error recognition and correction (Allman et al. 2001; Bush et al. 2000) and conflict monitoring and correction (van Veen et al. 2001).
The adverse effects of excessive alcohol consumption on the prefrontal lobes (e.g., Grant and Mohns 1975) are often related to functions such as planning, set shifting, and continuous performance (Marksteiner et al. 2002) and problem solving and abstract thinking (Lawton-Craddock et al. 2003). For example, it has been reported that alcohol abusers show poorer performance on the Shipley Institute of Living Scale Vocabulary (SILS-V) and Abstraction (SILS-A) scales than nonabusers (e.g., Nixon et al. 1995). The adverse effects are exacerbated by a long history of alcohol abuse.
Similarly, acute doses of alcohol impair information-processing abilities, including (a) stimulus detection, stimulus recognition, response selection, and response execution (Maylor and Rabbitt 1993) and (b) planning, inhibition, rule detection, coordination on dual tasks, and speed of processing (see Ciesielski et al. 1995; Deckel et al. 1995; Noel et al. 2001, 2002). Alcohol-dependent drinkers perform more poorly on incongruent trials (the word red in green ink) on the classic Stroop test than do control participants (e.g., Stetter et al. 1995; Stormark et al. 2000). Alcohol-related cognitive impairments are not limited to heavy and prolonged drinking (Brown et al. 2000); even small doses of alcohol can impair ECF and inhibitory processes (Vogel-Sprott et al. 2001).
Wells and Matthews (1999) suggested that distraction for disorder-specific stimuli is not isolated from the rest of cognitive system, including the ECF. ECF plays an important role in situations in which automatic cognitive processes are insufficient for task performance, and individuals need to use consciously their cognitive abilities for selective attention and task management. Selective attention and task management are processed in the dorsolateral prefrontal cortex (DLPFC; Smith and Jonides 1999), the anterior cingulate cortex (ACC; e.g., Cabeza and Nyberg 2000), and the thalamus (e.g., Fuentes 2001; Mega and Cummings 1994). Subdivisions of the DLPFC and the ACC are also involved in emotional (e.g., Davidson 1998; Davidson and Irwin 1999) and cognitive (Bush et al. 1999, 2000; Vogt et al. 1992; Whalen et al. 1998) processing of stimuli. Despite their spatial separation, the cognitive and emotional parts of the brain involved in executive processes interact with each other, such that increases in activity in one region are associated with reductions in activity in the other (Bantick et al. 2002).
Evidence also shows that overlapping brain regions (e.g., ACC) are involved in dual-attention tasks that require ECF and inhibitory processes (see MacLeod and MacDonald 2000) and in the processing of emotionally salient stimuli (e.g., Childress et al. 1999; George et al. 1997, 2001; Grant et al. 1996; Kilts et al. 2001; Serra-Mestres and Ring 2002). From this evidence, it was concluded that individuals’ sensitivity to disorder-related stimuli might involve specific brain regions, such as the ACC, in both selective attention and emotional regulation. The suggested overlap has led some researchers to believe that performance on the classic and emotional Stroop tests taps a common process (e.g., Pardo et al. 1990; Zack et al. 2001); hence, they question the validity of attentional distraction for disorder-specific stimuli on emotional Stroop tests, including the alcohol Stroop.
There is also evidence that casts doubt on the alleged overlap. Ravnkilde et al. (2002) reported that although interference on the classic Stroop is associated with activation of the left ACC, it is not associated with activation of regions specifically involved in performance on the emotional Stroop test, viz., the prefrontal cortex, supplementary motor cortex, thalamus, and cerebellum. Some authors (Derbyshire et al. 1998; Paulus et al. 2002; Salgado-Pineda et al. 2002) have suggested that the alleged regional overlap in the processing of classic and emotional Stroop stimuli is limited to analyses at the group level. They argued that variation at the individual level in the selection of an optimal response strategy could be attributed to participants’ different cognitive styles.
To conclude, there are doubts about whether attentional bias for alcohol-related stimuli reported in previous studies is genuine or whether it is an artifact of participants’ general cognitive ability, which may have been impaired by excessive drinking. That is, differences in alcohol attentional bias among individuals with different levels of alcohol consumption could be due to variations in their cognitive and inhibitory processes, rather than to their differential distractibility for salient vs neutral stimuli. To evaluate the validity of alcohol attentional bias, the present study assessed whether the stronger distraction of alcohol-dependent than social drinkers by alcohol-related stimuli is an artifact of dependent drinkers’ impaired cognitive functioning.
Hypotheses
The following hypotheses were tested:
-
(a)
Dependent drinkers perform more poorly than social drinkers on measures of cognitive performance (i.e., SILS and the classic Stroop).
-
(b)
Excessive drinking is associated with poorer cognitive flexibility and inhibitory processes, as measured by SILS and interference on the classic Stroop test.
-
(c)
Dependent drinkers show greater attentional bias for alcohol-related stimuli than social drinkers.
-
(d)
Differences in dependent drinkers’ and social drinkers’ alcohol attentional bias are not an artifact of differences in their general cognitive functioning.
The last hypothesis is based on the theory of current concerns (Klinger 1975, 1977, 1987, 1996; Klinger and Cox 2004), which states that people are distracted by stimuli related to their current concerns. According to the theory, drinking alcohol can become a person’s overriding current concern; having this concern corresponds to a motivational state through which the person’s cognitive processes are altered, causing increased attentional sensitivity to alcohol-related stimuli. The theory challenges the view that general cognitive impairment is responsible for disorder-specific attentional bias. Because alcohol-related attentional bias on the alcohol Stroop test has previously been observed among both social and dependent drinkers, the present hypotheses were tested with both types of drinkers.
Method
Participants
The social drinkers were 128 university undergraduate students from the University of Wales, Bangor, who were recruited from the School of Psychology Student Participant Panel (N=99) or other academic departments (N=29); the latter students were paid for their participation. The students were required not to have recently participated in a Stroop experiment (explained as a task requiring that the color of a series of words be named while the meaning of the words is ignored). Participants were told that they should not drink any alcohol on the day of the experiment prior to it. Participants who reported drinking more than six standard drinks during the night prior to the study were rescheduled for a future appointment. Six participants were not included in the final analyses because their data were faulty (i.e., incomplete questionnaires). Only participants who were drinkers and those who did not meet the Short Michigan Alcoholism Screening Test (SMAST; Selzer 1971) three-point cutoff for problem drinkers were included. Nondrinkers were excluded from the data analyses because personality differences between drinkers and nondrinkers have been frequently reported (e.g., King et al. 2003). The final sample included 87 participants (63% females). The mean age of the sample of social drinkers was 24.13 years (SD 9.35); their mean years of education was 14.13 (SD 0.75). Males and females did not differ in age, t(85)=1.09, p>0.05, or years of education, t(85)=0.028, p>0.05.
The alcohol-dependent participants were recruited from an inpatient alcohol detoxification and rehabilitation unit; 50 participants were tested, all of whom had a primary diagnosis of alcohol dependence. Potential participants whose medical records suggested that they suffered from neurological impairment or comorbid psychopathology were excluded. The participants were tested after they had recovered from detoxification or a minimum of 10 days after admission. Three participants were excluded because of faulty data. The final sample comprised 47 participants (28% females), whose mean age was 43.80 years (SD 7.95); their mean years of education was 11.04 (SD 2.19). Male and female participants did not differ in age, t(44)=1.63, p>0.05, or years of education, t(44)=0.23, p>0.05. However, male dependent drinkers drank more alcohol than female dependent drinkers, t(45)=2.35, p<0.01.
The composition of gender across the two samples was not equal, χ 2(1)=13.65, p=0.001, such that the student sample included a greater proportion of females than the abuser sample. In addition, alcohol abusers were older (mean 40.57, SD 7.87) than controls (mean 23.41, SD 8.56), t(132)=13.46, p=0.001. Students reported more years of formal education (mean 14.12, SD 0.86) than alcohol abusers (mean 11.04, SD 7.87), t(132)=11.70, p=0.001. Dependent drinkers drank more alcohol than social drinkers, t(132)=23.13, p<0.001.
Measures
Classic and alcohol Stroop tests
ECF-related abilities can be measured by tasks that are sensitive to frontal lobe damage, including the Wisconsin Card Sorting Test; WAIS Similarities, Digit Symbol, Digit Span, and Object Assembly; the Halstead–Reitan Categories Test; and the classic Stroop test (Connor et al. 2000; Dao-Castellana et al. 1998; Hoaken et al. 1998; Lyvers 2000). The classic Stroop test has been used to assess selective attention and task management. Reaction times (RTs) to incongruent stimuli (e.g., the word red in blue ink) provide a sensitive measure of inhibitory processes (Ardouin et al. 1999; Carter et al. 2000; Nassauer and Halperin 2003; Swick and Jovanovic 2002; Wright et al. 2003) and cognitive flexibility (Fuentes 2001; Steel et al. 2001; Wright et al. 2003). Adleman et al. (2002), in a developmental functional magnetic resonance imaging (fMRI) investigation of the Stroop interference task, suggested that the classic Stroop test can be reliably used to detect malfunctioning of the prefrontal cortex. Another reason for using the classic Stroop test to assess inhibitory processes and cognitive flexibility in the present study was that, like the alcohol Stroop, it is based on cognitive interference (Pardo et al. 1990).
The classic and alcohol Stroop were combined into one computerized test; having the words presented in a mixed randomized fashion reduces the chances that participants will develop response strategies to use when the stimuli presented are from a single semantic category (MacLeod 1991). The results of a pilot study showed that having incongruent and alcohol words intermixed still allowed alcohol-attentional bias to be observed; this concern arose because of the higher cognitive demand required to respond to the color incongruent stimuli.
The classic Stroop color names were red, yellow, blue, and green; each word was either congruent with the color in which it was displayed (e.g., red in red) or incongruent (e.g., red in green). The alcohol-related words and control words were compiled specifically for the present research.Footnote 1 Each list comprised a single semantic category (alcohol-related vs building-related), according to Green and Rogers (1993) recommendation. Each alcohol and neutral word was written in each of four colors (blue, green, yellow, and red), resulting in a total of 28 alcohol words and 28 control words in each block of stimuli. Each block was equivalent in terms of mean number of letters, number of syllables per word, and word frequency. The frequency of each word was derived from CELEX (Baayen et al. 1993), the most recently published lexical database that was suitable for this study. Unlike other databases (e.g., Kucera and Francis 1967), CELEX is based on written and spoken British rather than American usage of English words. The equivalence of the blocks (i.e., within and across the four stimulus blocks) on the matching variables was confirmed by analysis of variance. In addition to the alcohol and control words, there were 28 color congruent words and 28 color incongruent words, for a total of 112 words in each list. The order of presentation of the words within each block was completely randomized.
Shipley Institute of Living Scale
The Shipley Institute of Living Scale (SILS; Zachary 2000) measures general intellectual functioning in adults and adolescents. It is a paper-and-pencil, self-administered test consisting of vocabulary and abstraction subtests. Wechsler Adult Intelligence Scale-Revised (WAIS-R) full-scale IQ scores can be estimated from SILS raw scores. The SILS Abstraction Quotient (SILS-AQ) detects intellectual deterioration, defined as a markedly lower abstraction than vocabulary score; this score is adjusted for age and education.
Parker et al. (1980) found that the amount of alcohol that social drinkers drank per session was negatively correlated with their SILS-AQ. Wehr and Bauer (1999) found that the SILS was a better predictor of alcohol-dependent drinkers’ treatment completion than other tests of cognitive ability or of depression, anxiety, antisocial personality, or length, type, and severity of the addiction.
Alcohol Use Questionnaire
The Alcohol Use Questionnaire (AUQ; Cox 2000) assesses the quantity and frequency of respondents’ drinking during the prior year, including the typical quantity per occasion and the atypical quantity per occasion and the frequency of each. The questionnaire covers four types of alcoholic beverages: beer, wine, spirits, and alcopops.Footnote 2 It also asks for the number of days since the last drink and the amount of alcohol consumed on the last day of drinking. Average total consumption can be calculated for specific periods, e.g., weekly, monthly, or yearly. Mean annual alcohol consumption was calculated by averaging each participant’s typical and atypical consumption for the past year. In turn, weekly mean consumption was calculated by dividing mean annual consumption by 52; this was the alcohol-use measure that was employed in the data analyses.
Apparatus
SuperLab Pro (SKD) software (Cedrus Corporation 1999) was used to present the Stroop task. The words (Century School Book, 48-point bold on a black background) were presented individually in the center of a PC laptop (Toshiba Satellite 1700-200) with a color display screen (12.1-in. DSTN). The viewing distance was 36–40 cm. The laptop’s keyboard was used for input. A color dot in either red, yellow, blue, or green was placed on four of the keys; on each trial, the participant responded by pressing one of these keys.
Procedure
After giving informed consent, each participant completed the tests in the following order: SILS, classic and alcohol Stroop, SMAST, and AUQ. The AUQ was administered last to avoid priming participants’ responses on the alcohol Stroop test. Prior to the main Stroop tasks, participants were asked to name the colors of four assorted dots affixed to the “/?” (red), “,<” (yellow), “cC” (green), and “zZ” (blue) keys of the keyboard (the input device) and four colored patches on the display, to insure that they have no difficulty differentiating the colors used in the task. They were clearly instructed to ignore the meaning of the words displayed on the screen and to press as quickly and accurately as possible the color key that corresponded to the color in which each stimulus was presented. Although manual responses often produce somewhat lower interference than vocal responses, the degree of interference is still significant (Brown and Besner 2001; MacLeod 1991; Monahan 2001). As MacLeod (1991) concluded, the Stroop effect is not dependent on the response mode or the interaction between response mode and type of stimulus. The effect does not originate “at the finish line” (p. 183).
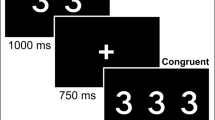
Prior to the main task, participants were provided with warm-up trials, during which they responded to 100 colored patches. There is inconsistency in the literature about the optimal intertrial interval (ITI). Interference has been observed in Stroop studies using ITIs that range from very short (e.g., 32 ms) to very long (e.g., 1,500 ms) (e.g., Kindt et al. 1997; Sharma and McKenna 2001). In the present study, the ITI was 800 ms, during which a fixation cross “+” appeared in the center of the display screen. Each stimulus remained on the screen until a response was made or 3 s had elapsed. The order of presentation of the four blocks of stimuli was counterbalanced across participants. To counteract fatigue, each participant was invited to rest for 2 min between each block. At the end of the session, the participant was debriefed, thanked, and dismissed.
Results
Trials on which an incorrect response or no response was made were designated as errors. Social drinkers’ and alcohol-dependent participants’ mean percentage of errors on congruent trials of the classic Stroop test was 3.66 and 4.27%, respectively; their mean percentage of errors on incongruent trials was 3.56 and 8.81%, respectively. On the alcohol Stroop test, the mean percentage of errors of the two types of drinkers on the trials with alcohol-related stimuli was 3.60 and 2.83%, respectively; it was 3.60 and 2.95%, respectively, on trials with neutral stimuli. The alcohol-dependent participants made significantly more errors on the classic than the alcohol Stroop test, t(46)=2.65, p<0.01; they made more errors on the incongruent color trials than the students did, t(132)=3.17, p<0.01. RTs only on trials on which correct responses were made were included in the subsequent analyses, and very fast (<400 ms) and very slow RTs (>2,000 ms) were excluded. On average, 4.2% of the social drinkers’ RTs (i.e., errors and out-of-range RTs) and 5.1% dependent-drinkers’ RTs on the Stroop tests were excluded. Each participant’s mean RT to the congruent color words on the classic Stroop test was subtracted from that participant’s mean RT to the incongruent color words; this yielded interference scores as an index of participants’ cognitive flexibility and inhibitory ability. Alcohol interference scores were calculated as participants’ mean RT to the alcohol-related words minus their mean RT to the neutral words.
Table 1 shows the means and standard deviations of social drinkers’ and alcohol-dependent participants’ SILS scores, drinking indices, and classic and alcohol Stroop interference scores. To determine if social and dependent drinkers differed on SILS scores, drinking indices, and classic and alcohol Stroop interference scores, a multivariate analysis of variance (MANOVA) was conducted with Group as the fixed factor and six dependent variables as shown in Table 1. Gender was not included in the analysis because the literature suggests that gender does not influence participants’ responses on the Stroop test (MacLeod 1991). Results of the MANOVA showed a main effect for Group, F(6,126)=96.06, p=0.0001, η 2=0.82 (F value is Wilks’ lambda). The results, as shown in Table 1, indicate that the two groups of drinkers differed from each other on each of the dependent variables. The dependent drinkers drank more alcohol and had larger classic and alcohol Stroop interference scores than the social drinkers. The dependent drinkers had lower SILS vocabulary and abstraction scores and a lower abstraction quotient than the social drinkers.
Correlations among the variables are shown in Table 2. SILS scores were negatively correlated with age and positively correlated with years of education. As expected, SILS scores were negatively correlated with weekly mean drinking, which suggests that drinking excessively adversely affected cognitive functioning. There were also negative relationships between SILS scores and classic and alcohol-related interference scores, suggesting that the less cognitively facile drinkers had greater difficulty inhibiting distracting stimuli. Finally, classic and alcohol Stroop interference scores were positively correlated with each other, indicating that drinkers who had difficulty inhibiting distraction for one category of stimuli also had difficulty with the other category. In short, the first three hypotheses were supported. Compared to the social drinkers, the dependent drinkers drank more alcohol, performed cognitively more poorly, and showed greater attentional bias for alcohol-related stimuli.
In prior research, alcohol-dependent drinkers’ attentional bias for alcohol-related stimuli has been compared with that of nondependent drinkers (see Cox et al. 2005). Yet, one question remains unanswered: Is dependent drinkers’ stronger interference on the alcohol Stroop test due to their poorer cognitive functioning? An analysis of covariance (ANCOVA) was used to test the study’s fourth hypothesis that dependent drinkers’ stronger alcohol attentional bias is not an artifact of their impaired cognitive functioning. In the General Linear Model (GLM), Group (social vs dependent drinkers) was entered as a fixed-effects factor; SILS-V, SILS-A, SILS-AQ, and classic Stroop interference as the covariates; and alcohol interference scores as the dependent variable. The results showed that after SILS-V [F(1,128)=0.14, p=0.70, η 2=0.001], SILS-A [F(1,128)=0.007, p=0.93, η 2=0.0001], SILS-AQ [F(1,128)=0.14, p=0.74, η 2=0.001], and classic interference scores [F(1,128)=0.57, p=0.57, η 2=0.004] had been controlled, the alcohol-dependent drinkers had significantly larger alcohol interference scores than the social drinkers [F(1,128)=13.87, p<0.0001, η 2=0.10, power=0.96]. The near-zero effect sizes for the cognitive covariates in the model support the hypothesis that differences between social and dependent drinkers’ alcohol attentional bias are not an artifact of the differences in their general cognitive ability, as measured in this study.Footnote 3
Discussion
The objectives of the study were as follows:
-
(a)
To test whether excessive alcohol consumption is associated with impaired ECF (as measured by SILS indices and the classic Stroop test) and whether social and dependent drinkers are different in ECF
-
(b)
To determine whether variations of drinkers’ ECF are associated with variations in their alcohol-related attentional bias
-
(c)
To test whether differences in social and dependent drinkers’ alcohol attentional bias are an artifact of differences in their ECF.
These goals were based on prior evidence that heavy alcohol consumption is associated with impairments in ECF and that performance on the alcohol Stroop test appears to involve activation of brain areas that overlap with the areas involved in performance on the classic Stroop test.
The results are as follows. First, weekly mean alcohol consumption was negatively correlated with ECF. Moreover, the dependent drinkers scored lower on all the SILS indices of cognitive functioning, and they showed greater interference on the classic Stroop test than the social drinkers. These results are consistent with the view that excessive drinking adversely affects drinkers’ ECF. Dependent drinkers’ greater interference on the classic Stroop test supports the view that they have poorer inhibitory control and cognitive flexibility than social drinkers (e.g., Wright et al. 2003). The results are also consistent with the evidence that heavy drinking is injurious to the brain (e.g., Fadda and Rossetti 1998). The results should be interpreted in the context of other findings that drinkers’ vulnerability to developing alcohol-related problems depends on many factors, including their biological predisposition, family history of drinking, age, gender, and current pattern of drinking (chronic vs binge) (Cox and Klinger 1988, 1990, 2004; Heather et al. 2001). However, dependent drinkers’ larger ECF impairments than social drinkers do not negate the evidence that binge or other problematic patterns of drinking among nondependent drinkers are associated with poor ECF (e.g., Blume et al. 2000; Zeigler et al. 2005). Second, consistent with prior results, dependent drinkers had greater attentional bias for alcohol-related stimuli than social drinkers. Third, both classic and alcohol Stroop interference scores were negatively correlated with SILS vocabulary and abstraction scores. Classic and alcohol interference scores were positively correlated with each other, an outcome that might call into question the validity of the difference between dependent and social drinkers in alcohol-specific attentional bias. Fourth, however, dependent drinkers’ stronger attentional bias for alcohol-related stimuli than social drinkers remained significant after scores of the two groups on general cognitive functioning had been controlled.
The relationship between excessive drinking and poor ECF does not, of course, necessarily imply causality. Rather, neuropsychological evidence indicates that problem drinking and ECF impairment contribute reciprocally to each other (e.g., Ciesielski et al. 1995). Because ECF dysfunction is associated with self-control problems and alcohol abusers characteristically have impairments in self-control, it is plausible that ECF impairment plays a significant role in the development of uncontrolled drinking (Lyvers 2000). That is, having poor ECF might cause a person to drink heavily, and the heavy drinking escalates into an abusive, chronic pattern. Such a pattern might take different forms, including regular heavy drinking or episodic drinking. High levels of blood alcohol concentration in the brain are associated with reduced frontal lobe glucose utilization and cerebral blood flow and increased risk of alcohol-related damage to the frontal lobes (see Moselhy et al. 2001). Therefore, the more severe the abusive pattern of drinking, the greater is the risk of ECF impairment, and theoretically, the relationship is reciprocal.
The present results support Stetter et al. (1995) suggestion that cognitive processing on the alcohol Stroop test is independent of putative neuropsychological deficits in alcohol-dependent drinkers. Nevertheless, the present results showed a significant correlation between classic and alcohol Stroop interference scores, supporting Zack et al. (2001) suggestion that classic and emotional Stroop tests tap a common construct and that a poor general inhibitory system adversely affects performance on the emotional Stroop test. However, the present results indicate that the concern-relatedness of stimuli influences selective attention of them beyond the influence that general cognitive functioning and inhibitory ability exert.
Koob (2003) and Robinson and Berridge (1993) have suggested that a neural circuit exists for alcohol-specific attentional bias, which is independent of general ECF. Recall that the ACC comprises distinct areas for processing cognitive and emotional appraisals of an event. There are both top-down and bottom-up relationships between frontal lobe and subcortical circuits, especially those in the amygdala. Cortical and subcortical circuits are involved in rapid preconscious detection of the emotional significance of stimuli. If there were a general ECF circuit for all emotionally salient stimuli (including alcohol-related ones), the inhibitory processes responsible for performance on the classic Stroop test would overshadow performance on the alcohol Stroop test. The present results confirmed that this is not the case.
The argument advanced here is consistent with the converging evidence that attentional processes are related to a person’s current concerns (Klinger 1975, 1977, 1987, 1996; Cox and Klinger 2004). As described earlier, a current concern is the cognitive–motivational state corresponding to a particular goal striving. Presumably, each current concern causes a circuit of specialized executive functions to be formed that is different from the circuits for other current concerns. In support of this point of view, participants have been shown to have greater attentional distraction for concern-related stimuli than for other kinds of emotionally significant stimuli (e.g., Bauer and Cox 1998; Crombez et al. 2000; de Ruiter and Brosschot 1994; Kinderman 1994), and the distraction occurs, regardless of participants’ current mood (e.g., Riemann and McNally 1995; Spinks and Dalgleish 2001). These results are also consistent with Algom et al. (2004) experiments showing that anxious participants’ slow RTs in the presence of threatening stimuli are independent of the lexical characteristics of the stimuli. Algom et al. also showed that anxious participants react slowly in the presence of threatening stimuli whether they are required to focus on or away from these stimuli.
It should be noted that the conclusions drawn from the present study are based on alcohol and classic Stroop tests administered to social and abusive drinkers. It is unknown how nondrinkers’ ECF would be related to their performance on the alcohol Stroop and other emotional Stroop tests. In addition, it is impossible to generalize the present findings to other measures of attentional bias, such as the flicker or dot-probe paradigms. Although the alcohol abusers and social drinkers differed considerably in age and education, these variables could not be statistically controlled through ANCOVA. That is, because both age and education were significantly correlated with the classic Stroop interference scores and SILS indices, age and education could not be controlled through covariance analysis because of problems with collinearity. Therefore, only the classic Stroop interference scores and SILS indices were entered into the ANCOVA model as covariates. Doing so indirectly corrected for age- and education-related influences on participants’ ECF (i.e., as measured by SILS indices and classic Stroop interference) that were related to the study’s fourth hypothesis—that dependent drinkers’ stronger alcohol attentional bias is not an artifact of their impaired cognitive functioning.
The results of the present study suggest that alcohol-attentional bias is a reliable phenomenon. It is also a clinically important component of abusive drinking, and interventions might be used to control it. In fact, several research groups have recently developed interventions to reduce the impact of alcohol attentional bias on excessive drinking (see Wiers et al. 2005).
Notes
The stimuli in the four blocks were as follows. Block 1: beer, whisky, scotch, liquor, tequila, bar, rum; gate, shed cupboard, tap, fence, toilet, ceiling. Block 2: shot, shorts, vodka, pint, liqueur, alcohol, bourbon; garden, shelf, alcove, carpet, chimney, radiator, stove. Block 3: wine, bitter, stout, pub, brandy, champagne, mead; hall, tail, patio, drainpipe, socket, doorknob, roof. Block 4: drink, sherry, cider, booze, spirit, gin, cocktail; bath, stairs, balcony, porch, lamp, fireplace, sink.
An alcopop is an alcoholic beverage that came on the market in the United Kingdom in 1995. It is a sweet, effervescent fruit drink, usually with about 5% of alcohol by volume.
In Cohen (1992), an f represents the effect size for an ANOVA model; values of 0.10, 0.25, and 0.40 are defined as small, medium, and large, respectively.
References
Adleman NE, Menon V, Blasey CM, White CD, Warsofsky IS, Glover GH, Reiss AL (2002) A developmental fMRI study of the Stroop color–word task. Neuroimage 16(1):61–75
Algom D, Chajut E, Lev S (2004) A rational look at the emotional Stroop phenomenon: a generic slowdown, not a Stroop effect. J Exp Psychol Gen 133(3):323–338
Allman JM, Hakeem A, Erwin JM, Nimchinsky E, Hof P (2001) The anterior cingulate cortex. The evolution of an interface between emotion and cognition. Ann N Y Acad Sci 935:107–117
Ardouin C, Pillon B, Peiffer E, Bejjani P, Limousin P, Damier P, Arnulf I, Benabid AL, Agid Y, Pollak P (1999) Bilateral subthalamic or pallidal stimulation for Parkinson’s disease affects neither memory nor executive functions: a consecutive series of 62 patients. Ann Neurol 46(2):217–223
Baayen HR, Piepenbrock R, van Rijn H (1993) The CELEX lexical database (CD-ROM). Linguistic Data Consortium, University of Pennsylvania, Philadelphia, PA
Bantick SJ, Wise RG, Ploghaus A, Clare S, Smith SM, Tracey I (2002) Imaging how attention modulates pain in humans using functional MRI. Brain 125(Pt 2):310–319
Bauer D, Cox WM (1998) Alcohol related words are distracting to both alcohol abusers and non-abusers in the Stroop colour-naming task. Addiction 93(10):1539–1542
Blume AW, Marlatt GA, Schmaling KB (2000) Executive cognitive function and heavy drinking behavior among college students. Psychol Addict Behav 14(3):299–302
Brown M, Besner D (2001) On a variant of Stroop’s paradigm: which cognitions press your buttons? Mem Cognit 29(6):903–904
Brown SA, Tapert SF, Granholm E, Delis DC (2000) Neurocognitive functioning of adolescents: effects of protracted alcohol use. Alcohol Clin Exp Res 24:164–171
Bunge SA, Klingberg T, Jacobsen RB, Gabrieli JD (2000) A resource model of the neural basis of executive working memory. Proc Natl Acad Sci U S A 97(7):3573–3578
Bush G, Frazier JA, Rauch SL, Seidman LJ, Whalen PJ, Jenike MA, Rosen BR, Biederman J (1999) Anterior cingulate cortex dysfunction in attention-deficit/hyperactivity disorder revealed by fMRI and the Counting Stroop. Biol Psychiatry 45(12):1542–1552
Bush G, Luu P, Posner MI (2000) Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn Sci 4(6):215–222
Cabeza R, Nyberg L (2000) Imaging cognition II: an empirical review of 275 PET and fMRI studies. J Cogn Neurosci 12(1):1–47
Carter CS, Macdonald AM, Botvinick M, Ross LL, Stenger A, Noll D, Cohen JD (2000) Parsing executive processes: strategic vs. evaluative functions of the anterior cingulate cortex. Proc Natl Acad Sci U S A 97(4):1944–1948
Cedrus Corporation (1999) SuperLab Pro SKD (version 2.1) [software]. Cedrus Corporation, San Pedro, CA, USA
Childress AR, Mozley PD, McElgin W, Fitzgerald J, Reivich M, O’Brien CP (1999) Limbic activation during cue-induced cocaine craving. Am J Psychiatry 156(1):11–18
Ciesielski KT, Waldorf AV, Jung RE (1995) Anterior brain deficits in chronic alcoholism—cause or effect? J Nerv Ment Dis 183(12):756–761
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159
Connor PD, Sampson PD, Bookstein FL, Barr HM, Streissguth AP (2000) Direct and indirect effects of prenatal alcohol damage on executive function. Dev Neuropsychol 18(3):331–354
Cox WM (2000) Alcohol Use Questionnaire. Unpublished questionnaire. University of Wales, Bangor
Cox WM, Klinger E (1988) A motivational model of alcohol use. J Abnorm Psychol 97:168–180
Cox WM, Klinger E (1990) Incentive motivation, affective change, and alcohol use: a model. In: Cox WM (ed) Why people drink: parameters of alcohol as a reinforcer. Gardner, New York, pp 291–314
Cox WM, Klinger E (2004) A motivational model of alcohol use: Determinants of use and change. In: Cox WM, Klinger E (eds) Handbook of motivational counseling: concepts, approaches, and assessment. Wiley, Chichester, UK, pp 121–138
Cox WM, Fadardi JS, Pothos EM (2005) The alcohol-Stroop test: theoretical considerations and procedural recommendations. Psychol Bull (in press)
Crombez G, Hermans D, Adriaensen H (2000) The emotional Stroop task and chronic pain: what is threatening for chronic pain sufferers? Eur J Pain 4(1):37–44
Dao-Castellana MH, Samson Y, Legault F, Martinot JL, Aubin HJ, Crouzel C, Feldman L, Barrucand D, Rancurel G, Feline A, Syrota A (1998) Frontal dysfunction in neurologically normal chronic alcoholic subjects: metabolic and neuropsychological findings. Psychol Med 28(5):1039–1048
Davidson RJ (1998) Affective style and affective disorders: perspectives from affective neuroscience. Cogn Emot 12(3):307–330
Davidson RJ, Irwin W (1999) The functional neuroanatomy of emotion and affective style. Trends Cogn Sci 3(1):11–21
Deckel AW, Bauer L, Hesselbrock V (1995) Anterior brain dysfunctioning as a risk factor in alcoholic behaviors. Addiction 90(10):1323–1334
Derbyshire SW, Vogt BA, Jones AK (1998) Pain and Stroop interference tasks activate separate processing modules in anterior cingulate cortex. Exp Brain Res 118(1):52–60
de Ruiter C, Brosschot JF (1994) The emotional Stroop interference effect in anxiety: attentional bias or cognitive avoidance? Behav Res Ther 32(3):315–319
Duka T, Townshend JM (2004) The priming effect of alcohol pre-load on attentional bias to alcohol-related stimuli. Psychopharmacology (Berl) 176(3–4):353–361
Fadda F, Rossetti Z (1998) Chronic ethanol consumption: from neuroadaptation to neurodegeneration. Prog Neurobiol 56:385–431
Fuentes LJ (2001) Selective attention deficit in schizophrenia. Rev Neurol 32(4):387–391
George MS, Ketter TA, Parekh PI, Rosinsky N, Ring HA, Pazzaglia PJ, Marangell LB, Callahan AM, Post RM (1997) Blunted left cingulate activation in mood disorder subjects during a response interference task (the Stroop). J Neuropsychiatry Clin Neurosci 9(1):55–63
George MS, Anton RF, Bloomer C, Teneback C, Drobes DJ, Lorberbaum JP, Nahas Z, Vincent DJ (2001) Activation of prefrontal cortex and anterior thalamus in alcoholic subjects on exposure to alcohol-specific cues. Arch Gen Psychiatry 58(4):345–352
Grant I, Mohns L (1975) Chronic cerebral effects of alcohol and drug abuse. Int J Addict 10(5):883–920
Grant S, London ED, Newlin DB, Villemagne VL, Liu X, Contoreggi C, Phillips RL, Kimes AS, Margolin A (1996) Activation of memory circuits during cue-elicited cocaine craving. Proc Natl Acad Sci U S A 93(21):12040–12045
Green MW, Rogers PJ (1993) Selective attention to food and body shape words in dieters and restrained nondieters. Int J Eat Disord 14(4):515–517
Heather N, Peters Timothy J, Stockwell T (2001) International handbook of alcohol dependence and problems. Wiley, Chichester
Hoaken PN, Giancola PR, Pihl RO (1998) Executive cognitive functions as mediators of alcohol-related aggression. Alcohol Alcohol 33(1):47–54
Jones BT, Jones BC, Smith H, Copely N (2003) A flicker paradigm for inducing change blindness reveals alcohol and cannabis information processing biases in social users. Addiction 98:235–244
Kilts CD, Schweitzer JB, Quinn CK, Gross RE, Faber TL, Muhammad F, Ely TD, Hoffman JM, Drexler KP (2001) Neural activity related to drug craving in cocaine addiction. Arch Gen Psychiatry 58(4):334–341
Kinderman P (1994) Attentional bias, persecutory delusions and the self-concept. Br J Med Psychol 67(Pt 1):53–66
Kindt M, Bierman D, Brosschot JF (1997) Cognitive bias in spider fear and control children: assessment of emotional interference by a card format and a single-trial format of the Stroop task. J Exp Child Psychol 66(2):163–179
King AC, Bernardy NC, Hauner K (2003) Stressful events, personality, and mood disturbance: Gender differences in alcoholics and problem drinkers. Addict Behav 28(1):171–187
Klinger E (1975) Consequences of commitment to and disengagement from incentives. Psychol Rev 82(1):1–25
Klinger E (1977). Meaning and void: inner experience and the incentives in people’s lives. University of Minnesota Press, Minneapolis
Klinger E (1987). Current concerns and disengagement from incentives. In: Halisch F, Kuhl J (eds) Motivation, attention, and volition. Springer, Berlin, Heidelberg, New York, pp 337–347
Klinger E (1996) The contents of thoughts: interference as the downside of adaptive normal mechanisms in thought flow. In: Sarason IG, Sarason BR, Pierce GR (eds) Cognitive interference: theories, methods, and findings. Lawrence Erlbaum, Hillsdale, NJ, pp 3–23
Klinger E, Cox WM (2004) Motivation and the theory of current concerns. In: Cox WM, Klinger E (eds) Handbook of motivational counseling: concepts, approaches, and assessment. Wiley, Chichester, UK, pp 3–27
Koob GF (2003) Alcoholism: allostasis and beyond. Alcohol Clin Exp Res 27(2):232–243
Kucera H, Francis WN (1967) Computational analysis of present-day American English. Brown University Press, Providence, RI
Lawton-Craddock A, Nixon SJ, Tivis R (2003) Cognitive efficiency in stimulant abusers with and without alcohol dependence. Alcohol Clin Exp Res 27(3):457–464
Lyvers M (2000) “Loss of control” in alcoholism and drug addiction: a neuroscientific interpretation. Exp Clin Psychopharmacol 8(2):225–249
MacLeod CM (1991) Half a century of research on the Stroop effect: an integrative review. Psychol Bull 109(2):163–203
MacLeod CM, MacDonald PA (2000) Interdimensional interference in the Stroop effect: uncovering the cognitive and neural anatomy of attention. Trends Cogn Sci 4(10):383–391
Mantere T, Tupala E, Hall H, Sarkioja T, Rasanen P, Bergstrom K, Callaway J, Tiihonen J (2002) Serotonin transporter distribution and density in the cerebral cortex of alcoholic and nonalcoholic comparison subjects: a whole-hemisphere autoradiography study. Am J Psychiatry 159(4):599–606
Marksteiner J, Bodner T, Gurka P (2002) Alcohol-induced cognitive disorder: alcohol dementia. Wien Med Wochenschr 152(3–4):98–101
Maylor EA, Rabbitt PM (1993) Alcohol, reaction time and memory: a meta-analysis. Br J Psychol 84(Pt 3):301–317
McCusker CG (2001) Cognitive biases and addiction: an evolution in theory and method. Addiction 96(1):47–56
Mega MS, Cummings JL (1994) Frontal–subcortical circuits and neuropsychiatric disorders. J Neuropsychiatry Clin Neurosci 6(4):358–370
Mogg K, Bradley BP, Millar N, White J (1995) A follow-up study of cognitive bias in generalized anxiety disorder. Behav Res Ther 33:927–935
Monahan JS (2001) Coloring single Stroop elements: reducing automaticity or slowing color processing? J Gen Psychol 128(1):98–112
Moselhy HF, Georgiou G, Kahn A (2001) Frontal lobe changes in alcoholism: a review of the literature. Alcohol Alcohol 36(5):357–368
Nassauer KW, Halperin JM (2003) Dissociation of perceptual and motor inhibition processes through the use of novel computerized conflict tasks. J Int Neuropsychol Soc 9(1):25–30
Nixon SJ, Parsons OA, Schaeffer KW, Hale RL (1995) A methodological study of the Shipley Institute of Living Scale in alcoholics and non-alcoholics: reliability, discriminating items and alternate forms. Appl Neuropsychol 2(3/4):155–160
Noel X, Van der Linden M, Schmidt N, Sferrazza R, Hanak C, Le Bon O, De Mol J, Kornreich C, Pelc I, Verbanck P (2001) Supervisory attentional system in nonamnesic alcoholic men. Arch Gen Psychiatry 58(12):1152–1158
Noel X, Sferrazza R, Van Der Linden M, Paternot J, Verhas M, Hanak C, Pelc I, Verbanck P (2002) Contribution of frontal cerebral blood flow measured by 99 mTc-bicisate SPECT and executive function deficits to predicting treatment outcome in alcohol-dependent patients. Alcohol Alcohol 37(4):347–354
Pardo JV, Pardo PJ, Janer KW, Raichle ME (1990) The anterior cingulate cortex mediates processing selection in the Stroop attentional conflict paradigm. Proc Natl Acad Sci U S A 87(1):256–259
Parker ES, Birnbaum IM, Boyd RA, Noble EP (1980) Neuropsychologic decrements as a function of alcohol intake in male students. Alcohol Clin Exp Res 4(3):330–334
Paulus MP, Hozack N, Frank L, Brown GG (2002) Error rate and outcome predictability affect neural activation in prefrontal cortex and anterior cingulate during decision-making. Neuroimage 15(4):836–846
Pothos EM, Cox WM (2002) Cognitive bias for alcohol-related information in inferential processes. Drug Alcohol Depend 66(3):235–241
Ravnkilde B, Videbech P, Rosenberg R, Gjedde A, Gade A (2002) Putative tests of frontal lobe function: a PET-study of brain activation during Stroop’s Test and verbal fluency. J Clin Exp Neuropsychol 24(4):534–547
Riemann BC, McNally RJ (1995) Cognitive processing of personally relevant information. Cogn Emot 9(4):325–340
Roberts AJ, Koob GF (1997) The neurobiology of addiction: an overview. Alcohol Health Res World 21(2):101–106
Robinson TE, Berridge KC (1993) The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Rev 18(3):247–291
Robinson TE, Berridge KC (2003) Addiction. Annu Rev Psychol 54(1):25–53
Salgado-Pineda P, Vendrell P, Bargallo N, Falcon C, Junque C (2002) Functional magnetic resonance in the evaluation of the activity of the anterior cingulate cortex using Stroop’s paradigm. Rev Neurol 34(7):607–611
Selzer ML (1971) The Michigan Alcoholism Screening Test: the quest for a new diagnostic instrument. Am J Psychiatry 127(12):89–94
Serra-Mestres J, Ring HA (2002) Evidence supporting a cognitive model of depression in Parkinson’s disease. J Nerv Ment Dis 190(6):407–410
Sharma D, McKenna FP (2001) The role of time pressure on the emotional Stroop task. Br J Psychol 92(Pt 3):471–481
Skutle A, Berg G (1987) Training in controlled drinking for early-stage problem drinkers. Br J Addict 82(5):493–501
Smith EE, Jonides J (1999) Storage and executive processes in the frontal lobes. Science 283(5408):1657–1661
Spinks H, Dalgleish T (2001) Attentional processing and levels of symptomatology in Seasonal Affective Disorder (SAD): a preliminary longitudinal study. J Affect Disord 62(3):229–232
Stacy AW (1997) Memory activation and expectancy as prospective predictors of alcohol and marijuana use. J Abnorm Psychol 106:61–73
Steel C, Haworth EJ, Peters E, Hemsley DR, Sharma T, Gray JA, Pickering A, Gregory L, Simmons A, Bullmore ET, Williams SC (2001) Neuroimaging correlates of negative priming. Neuroreport 12(16):3619–3624
Stetter F, Ackermann K, Bizer A, Straube ER, Mann K (1995) Effects of disease-related cues in alcoholic inpatients: results of a controlled “Alcohol Stroop” study. Alcohol Clin Exp Res 19(3):593–599
Stormark KM, Laberg JC, Nordby H, Hugdahl K (2000) Alcoholics’ selective attention to alcohol stimuli: automated processing? J Stud Alcohol 61(1):18–23
Stroop JR (1935) Studies of interference in serial verbal reaction. J Exp Psychol 18:643–662
Swick D, Jovanovic J (2002) Anterior cingulate cortex and the Stroop task: neuropsychological evidence for topographic specificity. Neuropsychologia 40(8):1240–1253
Tiffany ST (1990) A cognitive model of drug urges and drug-use behavior: role of automatic and nonautomatic processes. Psychol Rev 97(2):147–168
van Veen V, Cohen JD, Botvinick MM, Stenger VA, Carter CS (2001) Anterior cingulate cortex, conflict monitoring, and levels of processing. Neuroimage 14(6):1302–1308
Vogel-Sprott M, Easdon C, Fillmore M, Finn P, Justus A (2001) Alcohol and behavioral control: cognitive and neural mechanisms. Alcohol Clin Exp Res 25(1):117–121
Vogt BA, Finch DM, Olson CR (1992) Functional heterogeneity in cingulate cortex: the anterior executive and posterior evaluative regions. Cereb Cortex 2(6):435–443
Waters H, Green MW (2003) A demonstration of attentional bias, using a novel dual task paradigm, towards clinically salient material in recovering alcohol abuse patients? Psychol Med 33(3):491–498
Watts FN, McKenna FP, Sharrock R, Trezise L (1986) Colour naming of phobia-related words. Br J Psychol 77(Pt 1):97–108
Wehr A, Bauer LO (1999) Verbal ability predicts abstinence from drugs and alcohol in a residential treatment population. Psychol Rep 84(3 Pt 2):1354–1360
Wells A, Matthews G (1999) The cognitive science of attention and emotion. In: Dalgleish T, Power MJ (eds) Handbook of cognition and emotion. Wiley, Chichester, UK
Whalen PJ, Bush G, McNally RJ, Wilhelm S, McInerney SC, Jenike MA, Rauch SL (1998) The emotional counting Stroop paradigm: a functional magnetic resonance imaging probe of the anterior cingulate affective division. Biol Psychiatry 44(12):1219–1228
Wiers RW, van Woerden N, Smulders FT, de Jong PJ (2002) Implicit and explicit alcohol-related cognitions in heavy and light drinkers. J Abnorm Psychol 111(4):648–658
Wiers RW, Cox WM, Field M, Fadardi JW, Palfai T, Schoenmakers T et al (2005) The search for new ways to change implicit alcohol-related cognitions in heavy drinkers. Alcohol Clin Exp Res (in press)
Williams JM, Mathews A, MacLeod C (1996) The emotional Stroop task and psychopathology. Psychol Bull 120(1):3–24
Wright I, Waterman M, Prescott H, Murdoch-Eaton D (2003) A new Stroop-like measure of inhibitory function development: typical developmental trends. J Child Psychol Psychiatry Allied Discipl 44(4):561–575
Zachary RA (2000) Shipley Institute of Living Scale: revised manual. Western Psychological Services, Los Angeles
Zack M, Belsito L, Scher R, Eissenberg T, Corrigall WA (2001) Effects of abstinence and smoking on information processing in adolescent smokers. Psychopharmacology (Berl) 153(2):249–257
Zeigler DW, Wang CC, Yoast RA, Dickinson BD, McCaffree MA, Robinowitz CB, Sterling ML (2005) The neurocognitive effects of alcohol on adolescents and college students. Prev Med 40(1):23–32
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fadardi, J.S., Cox, W.M. Alcohol attentional bias: drinking salience or cognitive impairment?. Psychopharmacology 185, 169–178 (2006). https://doi.org/10.1007/s00213-005-0268-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-005-0268-0