
Abstract
Rationale
Model-based assessments of behavioral control have been used to study the acute effects of alcohol on the ability to execute and inhibit behavioral responses. Response inhibition appears more vulnerable to the impairing effects of alcohol than response execution. Current information processing models have yet to account for this observation.
Objectives
The present study used a reductionist approach to determine if the particular vulnerability of response inhibition to the effects of alcohol occurs at the level of the action (motor program). The study examined the effects of alcohol on the ability to execute and inhibit behavior in a context in which preliminary information signaled the likelihood that a response should be executed or suppressed. The engagement and disengagement of responses were directly compared under alcohol.
Methods
Adults (N=24) performed a cued go/no-go task that required quick responses to go targets and suppression of responses to no-go targets. Response requirements were manipulated by varying the nature of the action required whereby half of the participants made key press responses (response engagement) and the other half released ongoing key presses (response disengagement). Performance was tested under three doses of alcohol: 0.00, 0.45, and 0.65 g/kg.
Results
Dose-dependent increases in commission errors were only observed with response engagement and not with response disengagement. Reaction times were faster for response engagement than response disengagement.
Conclusions
Response disengagement affords some protection against alcohol-induced impairment of inhibition, indicating that not all aspects of motor processing requiring inhibition are equally impaired by alcohol.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute alcohol intoxication is associated with myriad negative outcomes including violent crimes, injuries, and automobile accidents (Pernanen 1976). Impaired self-control has long been associated with acute alcohol intoxication and is often a significant contributor to such negative consequences. Understanding impaired self-control and its behavioral manifestations is of widespread interest because this is a core concern for varying syndromes such as substance abuse, personality disorders, and attention deficit hyperactivity disorder (Evenden 1999; Lyvers 2000). Several theories postulated that two distinct and independent processes govern behavioral control: one that activates behavior and one that inhibits behavior (Fowles 1987; Gray 1976, 1977; Logan and Cowan 1984; Patterson and Newman 1993; Quay 1997). The two processes act in opposition to one another, and the relative strength of each is assumed to determine behavioral control. Deficient behavioral inhibition is inferred by observations of overactive, impulsive behavior (Logan et al. 1984) and is considered to be a primary mechanism by which alcohol impairs self-control (Fillmore 2003).
Model-based assessments of behavioral control have been used to study the acute effects of alcohol in humans (for review, see Fillmore 2003). These assessments, such as the cued go/no-go reaction time (RT) task, model behavioral control as the ability to activate a response to a go-signal quickly and suddenly inhibit a response when a stop-signal occurs (Logan and Cowan 1984; Miller et al. 1991; Logan 1994). Thus, independent measures of the countervailing activational and inhibitory aspects of behavioral control are obtained. Task analyses have determined that cued go/no-go task performance involves three stages of processing: (1) perception, (2) decision, and (3) action (Miller et al. 1991). Although relatively independent processes, many similarities between activation and inhibition have been demonstrated. No-go responses (i.e., response inhibition) depend on an active decision process similar to that involved in activating an overt response (De Jong et al. 1990; Hackley et al. 1990; Logan et al. 1984). Studies that have examined the effect of alcohol on subjects' behavioral control using the cued go/no-go task have found that alcohol produces the stereotypic, dose-dependent impairing effect on both the execution and inhibition of behavior (Abroms et al. 2003; Fillmore and Van Selst 2002; Marczinski and Fillmore 2003a,b, 2005).
However, the acute effects of alcohol do not always similarly impair activation and inhibition, as dissociations between the two mechanisms have been identified. In some contexts, inhibitory aspects are more vulnerable than activational aspects of behavioral control to the acute effects of alcohol (Abroms et al. 2003; Fillmore et al. in press; Marczinski and Fillmore 2003b; Vogel-Sprott et al. 2001). Neuropsychological accounts have argued that inhibitory actions (suppressing or delaying responses) are especially sensitive to the central nervous system (CNS) depressant effects of alcohol. In particular, the effects of alcohol are most disruptive when behavioral control relies heavily on the ability to suppress a sudden action (Conger 1956; Fowles 1987; Jentsch and Taylor 1999; Quay 1997). Laboratory studies using the cued go/no-go model of behavioral control have also highlighted that the complete suppression of a prepotent (instigated) behavioral response is impaired by a moderate dose of alcohol, whereas the activation of an alternative response is not (Abroms et al. 2003).
In summary, there is sufficient empirical evidence that inhibition appears particularly vulnerable to the acute effects of alcohol. However, reasons for this vulnerability are uncertain. Based on the three-stage model of information processing (perception, decision, and action), it seems reasonable to hypothesize that the vulnerability may lie at the last stage of processing. Previous manipulations of the perception and decision stages have not differentiated activation and inhibition in terms of alcohol impairment (Marczinski and Fillmore 2005; Fillmore 2004), leaving the action stage as the potential source of the dissociations between inhibition and activation. Moreover, most studies of alcohol effects of inhibitory control have modeled response inhibition as the ability to briefly suppress a prepotent (i.e., instigated) response, often a computer key press. These models operationalize inhibition as a discrete, brief process with a clear onset and offset. However, disinhibited behavior may also be manifested as the inability to maintain a task, such that an ongoing activity is terminated prematurely.
With regard to the effects of alcohol, no research has examined the degree to which the drug might impair inhibitory control over the disengagement of an ongoing response. To some extent, response disengagement and response engagement represent opposing motor sequences and could differ in the degree to which alcohol impairs inhibitory control over each function. The present study tested the possibility that alcohol-induced impairment of inhibitory control might differ depending on whether inhibitory control is required to prevent the premature engagement or the premature disengagement of a response. The cued go/no-go model was used to examine inhibitory control over the engagement and disengagement of responses. One group of participants was required to engage responses to go targets (press a key), and another group was required to disengage responses to go targets (release an ongoing key press). All task stimuli (cues and targets) were identical in each condition. Thus, the manipulation was confined to the level of the motor stage. The ability to engage and disengage responses was examined in response to three doses of alcohol: 0.0 (placebo), 0.45 and 0.65 g/kg.
Method
Participants
Twenty-four adults (12 women and 12 men) between the ages of 21 and 30 years (mean age=23.4 years, SD=2.4) participated in this study. The racial makeup of the sample was 79% Caucasian, 12.5% African–American, and 8.5% of participants did not report racial information. Volunteers completed questionnaires that provided demographic information, drinking habits, and physical and mental health status. Individuals with a self-reported psychiatric disorder, substance abuse disorder, head trauma, or other CNS injury were excluded from the study. Volunteers with a score of 5 or higher on the Short-Michigan Alcoholism Screening Test (S-MAST) (Selzer et al. 1975) were excluded from the study.
Recent use of amphetamine, barbiturates, benzodiazepines, cocaine, opiates, and tetrahydrocannabinol was assessed by means of urine analysis. Any volunteer who tested positive for the presence of any of these drugs was excluded from participation. No female volunteers who were pregnant or breast-feeding participated in the research, as determined by self-report and urine human chorionic gonadotrophin levels. Participants were recruited via notices posted on community bulletin boards and by classified newspaper advertisements. All volunteers provided informed consent prior to participating. The University of Kentucky Medical Institutional Review Board approved the study, and volunteers received $100 for participation.
Apparatus and materials
Cued go/no-go task
Participants performed a cued go/no-go RT task that has been used to demonstrate that alcohol can impair inhibitory and activational aspects of behavioral control (Abroms et al. 2003; Marczinski and Fillmore 2003a,b, 2005). A trial involved the following sequence of events: (a) presentation of a fixation point (+) for 800 ms; (b) a blank, white screen for 500 ms; (c) a cue displayed for one of five stimulus onset asynchronies (SOAs; 100, 200, 300, 400, and 500 ms); (d) a go or no-go target that remained visible until the participant made a response or 1,000 ms had elapsed; and (e) an intertrial interval of 700 ms. The task was operated using E-Prime experiment generation software (Schneider et al. 2002) and was performed on a personal computer.
The cue was a white rectangle (7.5×2.5 cm) framed in a 0.8-mm black outline that was presented in the center of the computer monitor against a white background. The cue was presented in either a horizontal (height=2.5 cm, width=7.5 cm) or vertical (height=7.5 cm, width=2.5 cm) orientation. The go and no-go target were green and blue, respectively. They were displayed on the monitor as a single hue that filled the interior of the rectangular cue after the duration of the SOA. Participants were instructed to press or release the forward slash (/) key on the keyboard as soon as a go (green) target appeared and to suppress any action when a no-go (blue) target appeared. Key presses or releases were made with the index finger of the preferred hand. The computer displayed how quickly a participant responded to each go target by presenting the milliseconds elapsed from target onset until the key press or release. Participants were encouraged to make fast responses (i.e., the fewest milliseconds).
The orientation of the cue (horizontal or vertical) signaled the probability that a go or no-go target would be displayed for both groups of participants. Cues presented horizontally preceded the go target on 80% of the trails and preceded the no-go target on 20% of the trials. Cues presented vertically preceded the no-go target on 80% of the trials and preceded the go target on 20% of the trials. Previous research has demonstrated that this level of cue validity produces highly cue-dependent inhibitory and activational mechanisms of behavioral control (Marczinski and Fillmore 2005).
The nature of the response was varied to manipulate the action level of information processing for the cued go/no-go task. The following two conditions were identical except for the response requirement.
Response engagement
In this condition, participants were required to execute a response by pressing the “/” key when the green target was presented and refrain from making a response when the blue target was presented.
Response disengagement
In this condition, subjects were required to begin each trial already engaged in a response (i.e., pressing the “/” key) using the index finger of their dominant hand. When a green target was presented, the subject was instructed to release their finger from the key, thus, disengaging the response. When a blue target was presented, the subject was required to maintain the ongoing response by keeping their finger on the “/” key.
The different SOAs (100, 200, 300, 400, and 500 ms) between cues and targets encouraged participants in both conditions to pay attention to the cues, and the variability and randomness of the SOAs prevented the participants from anticipating the exact onset of the targets. A test consisted of 500 trials that presented the four possible cue–target combinations. An equal number of vertical (250) and horizontal (250) cues were presented before an equal number of go (250) and no-go (250) target stimuli. Each cue–target combination was presented at each of the five SOAs, and an equal number of SOAs separated each cue–target combination. The presentation of cue–target combinations and SOAs was random. For each trial, the computer recorded whether or not a response occurred, and if one occurred, the RT was measured in milliseconds from the onset of the target until the key was pushed or released. To encourage fast and accurate responding, we presented feedback to the participant during the intertrial interval by displaying the words correct or incorrect along with the RT in milliseconds. A test required approximately 30 min to complete.
Personal drinking habits questionnaire
This questionnaire yielded three measures of a subject's current typical drinking habits: (a) frequency (the number of drinking occasions per week), (b) dose (milliliter of absolute alcohol per kilogram of body weight typically consumed during a single drinking occasion), and (c) duration (time span in hours of a typical drinking occasion) (Vogel-Sprott 1992).
Subjective effects
Participants completed a beverage-rating scale to report their perceived alcoholic content of the beverages in terms of bottles of beer containing 5% alcohol. The scale ranged from 0 to 10 bottles of beer, in 0.5-bottle increments (e.g., Fillmore and Vogel-Sprott 2000).
Procedure
Individuals responded to the advertisements by calling the laboratory to participate in a telephone intake-screening interview conducted by a research assistant. All sessions began between 10 a.m. and 6 p.m. Before each test session, participants were instructed to fast for 4 h and abstain from alcohol for 24 h. Urine samples were tested for the presence of drug metabolites in all participants (OnTrak TesTstiks, Roche Diagnostics Corporation, Indianapolis, IN, USA) and pregnancy in female participants (Mainline Confirms HGL, Mainline Technology, Ann Arbor, MI, USA) before each session. Blood alcohol concentrations (BACs) were determined from breath samples measured by an Intoxilyzer, Model 400 (CMI, Inc., Owensboro, KY, USA). At the beginning of each testing session, a zero BAC was verified for each participant. A research assistant who was unaware of the research hypotheses tested participants individually.
Equal numbers of participants (N=12) were randomly assigned to the response-engagement and response-disengagement conditions, with the limitation that the two groups were required to have equivalent gender ratios. The two groups each contained six male and six female participants.
Response requirement training and intake session
The purpose of the initial intake session was to familiarize participants with the lab environment and procedures, to obtain necessary intake information required for participation, and to train the participants in their assigned cued go/no-go task (response engagement or response disengagement) to ensure that they were familiar with the cued go/no-go task before the dose-administration sessions. To verify that the participants could easily distinguish the colors of the stimuli in the cued go/no-go task, we presented each participant with a color vision test that required them to discriminate between the green and blue colors that were used as go and no-go targets in the task. All of the participants easily completed this task requirement. Participants then performed the 30-min cued go/no-go task.
Alcohol test sessions (1–3)
Cued go/no-go task performance was tested under three doses of absolute alcohol: 0.0, 0.45, and 0.65 g/kg. Each dose was administered on a separate test session, and all participants received each dose. Dose administration was double blind, and dose order across the three sessions was randomized across participants. Sessions were separated by a minimum of 24 h and maximum of 3 days. Alcohol doses were calculated on the basis of body weight. On each session, participants received one of the three doses. The 0.65-g/kg dose produces an average peak BAC of 75 mg/100 ml and was chosen based on prior research that showed that response activation and response inhibition are reliably impaired at this BAC (Abroms et al. 2003; Fillmore and Vogel-Sprott 1999, 2000; Marczinski and Fillmore 2003a,b). The 0.45-g/kg dose was chosen because it produces a peak BAC of 50 mg/100 ml that represents the minimal threshold BAC that reliably impairs psychomotor and reaction time performance in laboratory tasks (Holloway 1995; Marczinski and Fillmore 2003a).
A dose was administered as absolute alcohol divided equally into two drinks containing one part alcohol and three parts carbonated mix. Participants had 1 min to finish each drink, and the second drink was served 5 min after the first drink. This dosing procedure produces a mean rate of rise in BAC of 1.0 mg/100 ml/min (Fillmore and Vogel-Sprott 1998). Thus, the peak BACs following 0.45 and 0.65 g/kg doses were expected to occur approximately 50 and 75 min, respectively, after drinking began. Once peak BAC is achieved, it remains at a relatively steady state for approximately 10 min (Fillmore and Vogel-Sprott 1998). The placebo dose (0.0 g/kg) consisted of a volume of carbonated mix that matched the total volume of the 0.45-g/kg alcohol drink. A small amount (3 ml) of alcohol was floated on the surface of the beverage. It was served in two glasses that had been sprayed with an alcohol mist that resembled condensation and provided a strong alcoholic scent as the beverages were consumed. Previous research has shown that individuals report that this beverage contains alcohol (e.g., Fillmore and Vogel-Sprott 1998).
Participants' cued go/no-go task performance was tested at 30 min after drinking began. Thus, testing occurred during the ascending period of the blood alcohol curve in the active dose conditions. The beverage rating scale was completed 60 min postbeverage administration, just after the test. BACs were measured at 30, 65, and 90 min postbeverage administration. During the placebo session, participants also provided breath samples at those times ostensibly to measure their BAC. After the test session concluded, the participants relaxed in a waiting room within the laboratory. Participants received a meal and remained at leisure to read magazines or watch television until their BAC fell below 40 mg/100 ml. Transportation home was provided as needed. Upon completing the final session, participants were paid and debriefed.
Criterion measures of task performance and data analyses
The two primary measures of interest were the participants' commission errors to no-go targets (failures of response inhibition) and their speed of responding to go targets (response activation). Omission errors are extremely infrequent in cued go/no-go task performance and were not a primary measure of interest in this study.
Failures of response inhibition
Failures of response inhibition were measured as the proportion of no-go targets in which a participant failed to inhibit a response of engagement or disengagement. These p-commission errors were calculated for each cue condition (go and no-go) on each test. The hypothesis that the inhibitory impairing effects of alcohol would differ for the two groups and the two cue conditions was tested by a 2 (Group, response engagement vs. response disengagement) × 3 (Dose, 0.0 vs. 0.45 vs. 0.65 g/kg) × 2 (Cue, go cue vs. no-go cue) mixed design analysis of variance (ANOVA). Group was considered a between-subjects factor, and Dose and Cue were considered within-subjects factors. Dose-dependent increases in p-commission errors for each cue condition for each group were assessed by a priori planned comparisons using dependent t tests comparing each active dose condition to the placebo condition.
Response activation
Response activation was measured by the RT to engage or disengage responses to go targets. Shorter RT indicated greater facilitation of response activation. A mean RT score for a participant was calculated for each cue condition. Responses with RT less than 100 ms and greater than 1,000 ms were excluded. These outliers were infrequent, occurring on average less than one trial per test. Scores were analyzed by a 2 (Group, response engagement vs. response disengagement) × 3(Dose, 0.0 vs. 0.45 vs. 0.65 g/kg) × 2 (Cue, go cue vs. no-go cue) mixed-design ANOVA. Dose-dependent increases in RT for each cue condition for each group were assessed by a priori planned comparisons using dependent t tests comparing each active dose condition to the placebo condition. Omission errors were infrequent and occurred on less that 2% of go target trials (∼two trials per test) for both the response-engagement task and the response-disengagement task.
Results
Drinking habits
No group differences were observed by t tests on any drinking habit measure (ps>.30). The sample reported a mean drinking frequency of 1.6 (SD=1.0) times per week, with a mean dose per occasion of 1.0 (SD=0.5) ml/kg. For a person weighing 70 kg, this dose would approximate four bottles of beer containing 5% alcohol per volume. The mean duration of drinking was 3.3 h (SD=0.9). No gender differences were observed by t tests on the dose and duration drinking habit measures (ps>.37). A gender difference was observed on the frequency drinking habit measure, t(22)=2.9, p=0.008, as males reported drinking 2.1 (SD=0.9) times a week, whereas females reported drinking 1.1 (SD=0.8) times a week.
Blood alcohol concentrations
No detectable BACs were observed in response to placebo. Higher BACs were obtained under the 0.65-g/kg dose compared with the 0.45-g/kg dose, F (1,16)=301.18, p<.001. The rise and fall of BACs over the course of the testing session resulted in a main effect of time, F (2,32)=6.50, p<.01. The 0.45-g/kg dose produced a mean (SD) BAC at 30, 65, and 90 min after drinking of 54.5 mg/100 ml (15.6), 51.6 mg/100 ml (8.6), and 42.6 mg/100 ml (10.7), respectively. The 0.65-g/kg dose produced a mean (SD) BAC at 30, 65, and 90 min after drinking of 80.0 mg/100 ml (17.4), 83.0 mg/100 ml (11.3), and 68.9 mg/100 ml (12.1), respectively. No main effects or interactions involving group or gender were observed (ps>.06).
Cued go/no-go task performance
Failures of response inhibition
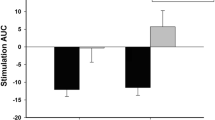
In both the response-engagement and response-engagement conditions, more errors occurred after invalid go cues than after valid no-go cues. More importantly, alcohol increased errors after invalid go cues only in the response-engagement condition, and not in the response-disengagement condition, as evidenced by a significant Group × Dose × Cue interaction, F (2,44)=3.46, p=0.04. Figure 1 shows the p-commission errors and illustrates this three-way interaction. A priori planned comparisons confirmed that for the response-engagement condition, p-commission errors following invalid go cues were significantly higher under both active doses compared with placebo (ps<.04). By contrast, in the response-disengagement condition, p-commission errors following invalid go cues did not differ significantly between either active dose condition and placebo (ps>.14). Furthermore, p-commission errors following valid no-go cues did not differ significantly between both active dose conditions and placebo (ps>.17), for both response engagement and response disengagement.

Mean commission errors to no-go targets after invalid go and valid no-go cues under three alcohol dose conditions: 0.0 (placebo), 0.45, and 0.65 g/kg for the response-engagement and response-disengagement groups (N=12/group). In the response-engagement condition, participants were required to press a key when a go target was presented and refrain from making a response when a no-go target was presented. In the response-disengagement condition, participants were required to release a key when a go target was presented and maintain an ongoing response when a no-go target was presented. Vertical bars show standard errors of the mean (N=12). *Significant differences from placebo (p<0.05)
Response activation
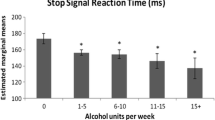
RT was faster in the response-engagement condition compared to the response-disengagement condition, F (1,22)=34.39, p<0.001. Alcohol increased RT following invalid no-go cues, but not following go cues, as evidenced by a significant Dose × Cue interaction, F (2,44)=3.81, p=0.03. Figure 2 plots the mean RT scores and illustrates this group difference and interaction. A priori planned comparisons revealed that in the response-engagement condition, RT following invalid no-go cues was significantly higher under both active doses compared with placebo (ps<.01). By contrast, in the response-disengagement condition, RT following no-go cues was significantly higher than placebo for the 0.65-g/kg dose (p=.01), but not for the 0.45-g/kg dose (p=.20). RT following valid go cues did not differ significantly between both active doses and placebo (ps>.34), for both the response-engagement and response-disengagement conditions.

Mean reaction time (RT) to respond to go targets after valid go and invalid no-go cues under three alcohol-dose conditions: 0.0 (placebo), 0.45, and 0.65 g/kg for the response-engagement and response-disengagement groups (N=12/group). In the response-engagement condition, participants were required to press a key when a go target was presented and refrain from making a response when a no-go target was presented. In the response-disengagement condition, participants were required to release a key when a go target was presented and maintain an ongoing response when a no-go target was presented. Vertical bars show standard errors of the mean (N=12). *Significant differences from placebo (p<0.05)
Subjective effect ratings
Beverage ratings increased as the dose of alcohol increased, F (2,44)=59.91, p<0.001. In the placebo, 0.45 and 0.65 g/kg conditions, subjects rated their beverages as having a mean (SD) alcohol content of 1.2 (SD=1.1), 3.4 (1.6), and 4.9 (2.2) bottles of beer, respectively. No other effects were significant (ps>0.60).
Discussion
This research utilized a reductionist approach to investigate whether the particular sensitivity of response inhibition to the impairing effects of alcohol can be isolated to the action stage (the motor program) of information processing. We used a manipulation known to only impact the action stage (and not perception or decision stages) of processing in the go/no-go decision. The results from the cued go/no-go task performance showed that alcohol impaired the ability to inhibit prepotent-engagement responses and slowed response times to engagement responses following invalid cues in a dose-dependent manner. By contrast, alcohol had no effect on the ability to inhibit prepotent-disengagement responses. In addition, alcohol only slowed disengagement responses following invalid cues in the 0.65-g/kg dose condition. Overall, RTs were faster for response engagement than for response disengagement. Thus, the results indicated that minor differences in response requirements had a dramatic impact on whether individuals demonstrated impairment in response inhibition under alcohol.
The differential effect of alcohol on response engagement and response disengagement cannot be attributed to differences in task stimuli or subject characteristics. The presentation of task cues and targets was identical in both of these task conditions so that perceptual demands were equivalent in both conditions. By using identical cue–target relationships, the tasks imposed similar perceptual and central processing demands on subjects with respect to conflicting cues. In addition, both conditions required 50% response activation trials (i.e., go targets) and 50% response inhibition trials (i.e., no-go targets). With regard to participant characteristics, there were no significant differences between task conditions in age, gender makeup, self-reported drinking habits, blood alcohol concentrations, or subjective effects obtained during the performance test period.
The primary implication of these results is that disengagement responses afford some protection against the impairing effects of alcohol, compared with engagement responses. Disengagement responses required a longer duration to complete, as evidenced by longer response times under all conditions compared to engagement responses. Such a finding coincides with previous observations that response alternation takes longer to complete than response inhibition and results in less impairment in inhibitory control (Abroms et al. 2003). However, the current study advances our current understanding of why slowing response time affords some protection for inhibition. As we equated the demands of the first two stages of information processing (perception and decision), the increased duration to perform the motor stage appears to be beneficial under alcohol, as evidenced by greater control over prepotent responses when the response is to be disengaged. Therefore, protection against alcohol-induced impairment of response inhibition can be localized to the final stage of processing (the level of the action). In addition, greater protection was afforded when valid cues correctly predicted the response required, and performance deteriorated in a dose-dependent manner when cues were invalid in the response engagement condition.
The results of this study provide a theoretical advance to current information processing models of alcohol-induced impairment of behavioral control. Evidence that disengagement responses are less vulnerable than engagement responses to the acute effects of alcohol is novel and emphasizes that motor components of cognition are important determinants in observed behavioral control. Interestingly, motor aspects of information processing are often considered inconsequential in laboratory experiments, as most tasks require simple key press responses. Since the advent of computerized cognitive experiments, researchers have relied heavily on the keyboard to record response times as this method provides sensitive RT measures that are a significant advance from older methods. As a result, a great deal of research, our own work included, has manipulated the perceptual and decision stages of information processing to determine the acute effects of alcohol on cognition (Fillmore 2004; Marczinski and Fillmore 2003a,b, 2005). However, our natural world has complex motor requirements where response engagement is only part of what must occur to maintain behavioral control. The results of the current experiment indicate that the action stage of information processing is not only important, but also is critically relevant for understanding alcohol-induced impairment of behavioral control.
These findings have practical implications in predicting when impulsive and inappropriate behaviors should occur under alcohol. For example, the results suggest that alcohol-induced impairment of driving skills should not be uniform. Driving requires numerous cognitive operations. For example, braking and accelerating require opposite motor programs, similar to those tested in this experiment. Our findings suggest that an engagement response (such as stepping on the brake pedal) would be more likely to be impaired under alcohol, whereby the individual might accidentally brake when not appropriate. By contrast, it is less likely that a disengagement response (such as releasing off the gas pedal) would be impaired under alcohol. Investigations with driving simulators are warranted to investigate this prediction.
References
Abroms BD, Fillmore MT, Marczinski CA (2003) Alcohol-induced impairment of behavioral control: effects on alteration and suppression of prepotent responses. J Stud Alcohol 64:687–695
Conger JJ (1956) Reinforcement theory and the dynamics of alcoholism. Q J Stud Alcohol 17:296–305
De Jong R, Coles MG, Logan GD, Gratton G (1990) In search of the point of no return: the control of response process. J Exp Psychol Hum Percept Perform 16:164–182
Evenden J (1999) Impulsivity: a discussion of clinical and experimental findings. J Psychopharmacol 13:180–192
Fillmore MT (2003) Drug abuse as a problem of impaired control: current approaches and findings. Behav Cogn Neurosci Rev 2:179–197
Fillmore MT (2004) Environmental dependence of behavioral control mechanisms: effects of alcohol and information processing demands. Exp Clin Psychopharmacol 12:216–223
Fillmore MT, Van Selst M (2002) Constraints on information-processing under alcohol in the context of response execution and response suppression. Exp Clin Psychopharmacol 10:417–424
Fillmore MT, Vogel-Sprott M (1998) Behavioral impairment under alcohol: cognitive and pharmacokinetic factors. Alcohol Clin Exp Res 22:1476–1482
Fillmore MT, Vogel-Sprott M (1999) An alcohol model of impaired inhibitory control and its treatment in humans. Exp Clin Psychopharmacol 7:49–55
Fillmore MT, Vogel-Sprott M (2000) Response inhibition under alcohol: effects of cognitive and motivational conflict. J Stud Alcohol 61:239–246
Fillmore MT, Marczinski CA, Bowman, AM (in press) Acute tolerance to alcohol effects on inhibitory and activational mechanisms of behavioral control. J Stud Alcohol
Fowles DC (1987) Application of a behavioral theory of motivation to the concepts of anxiety and impulsivity. J Res Pers 21:417–435
Gray JA (1976) The behavioral inhibition system: a possible substrate for anxiety. In: Feldman MP, Broadhurst A (eds) Theoretical and experimental bases of behavior therapies. Wiley, London, pp 3–41
Gray JA (1977) Drug effects of fear and frustration. Possible limbic site of action of minor tranquilizers. In: Iverson LL, Iverson SD, Snyder SH (eds) Handbook of psychopharmacology, vol 8. Plenum, New York, pp 433–529
Hackley SA, Schaffer R, Miller JO (1990) Preparation for Donder's type B and C reaction tasks. Acta Psychol 74:15–33
Holloway FA (1995) Low-dose alcohol effects on human behavior and performance. Alcohol Drugs Driv 11:39–56
Jentsch JD, Taylor JR (1999) Impulsivity resulting from frontostriatal dysfunction in drug abuse: implication for the control of behavior by reward-related stimuli. Psychopharmacology 146:373–390
Logan GD (1994) On the ability to inhibit thought and action: a user's guide to the stop-signal paradigm. In: Dagenbach D, Carr TH (eds) Inhibitory processes in attention, memory, and language. Academic, San Diego, pp 189–239
Logan GD, Cowan WB (1984) On the ability to inhibit thought and action: a theory of an act of control. Psychol Rev 91:295–327
Logan GD, Cowan WB, Davis KA (1984) On the ability to inhibit simple and choice reaction time responses: a model and a method. J Exp Psychol Hum Percept Perform 10:276–291
Lyvers M (2000) “Loss of control” in alcoholism and drug addiction: a neuroscientific interpretation. Exp Clin Psychopharmacol 8:225–249
Marczinski CA, Fillmore MT (2003a) Preresponse cues reduce the impairing effects of alcohol on the execution and suppression of responses. Exp Clin Psychopharmacol 11:110–117
Marczinski CA, Fillmore MT (2003b) Dissociative antagonistic effects of caffeine on alcohol-induced impairment of behavioral control. Exp Clin Psychopharmacol 11:228–236
Marczinski CA, Fillmore MT (2005) Alcohol increases reliance on cues that signal acts of control. Exp Clin Psychopharmacol 13:15–24
Miller J, Schaffer R, Hackley SA (1991) Effects of preliminary information in a go versus no-go task. Acta Psychol 76:241–292
Patterson CM, Newman JP (1993) Reflectivity and learning from aversive events: toward a psychological mechanism for the syndromes of disinhibition. Psychol Rev 100:716–736
Pernanen K (1976) Alcohol and crimes of violence. In: Kissin B, Begleiter H (eds) The biology of alcoholism: social aspects of alcoholism, vol 4. Plenum Press, New York, pp 351–444
Quay HC (1997) Inhibition and attention deficit hyperactivity disorder. J Abnorm Child Psychol 25:7–13
Schneider W, Eschman A, Zuccolotto A (2002) E-Prime user's guide. Psychology Software Tools, Pittsburgh, PA
Selzer ML, Vinokur A, Van Rooijen L (1975) A self-administered Short Michigan Alcoholism Screening Test (SMAST). J Stud Alcohol 36:117–126
Vogel-Sprott M (1992) Alcohol tolerance and social drinking: learning the consequences. Guilford Press, New York
Vogel-Sprott M, Easdon C, Fillmore M, Finn P, Justus A (2001) Alcohol and behavioral control: cognitive and neural mechanisms. Alcohol Clin Exp Res 25:117–121
Acknowledgements
This research was supported by Grant R01 AA12895 from the National Institute on Alcohol Abuse and Alcoholism.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Marczinski, C.A., Abroms, B.D., Van Selst, M. et al. Alcohol-induced impairment of behavioral control: differential effects on engaging vs. disengaging responses. Psychopharmacology 182, 452–459 (2005). https://doi.org/10.1007/s00213-005-0116-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-005-0116-2