
Abstract
The Standardised Field Sobriety Tests (SFST) were developed to test for alcohol intoxication but are currently being used by the State Police of Victoria (Australia) to test for driving impairment associated with drugs other than alcohol. The aim of the present study was to assess whether the SFSTs provide a sensitive measure of impairment following the consumption of a drug other than alcohol: delta-9-tetrahydrocannabinol (THC or cannabis). In a repeated-measures design, 40 participants consumed cigarettes that contained either 0% THC (placebo), 1.74% THC (low dose) or 2.93% THC (high dose). For each condition, after smoking a cigarette, participants performed the SFSTs on three occasions: 5 min (Time 1), 55 min (Time 2) and 105 min (Time 3) after the smoking procedure had been completed. The results revealed that there was a positive relationship between the dose of THC administered and the number of participants classified as impaired based on the SFSTs. Results also revealed that the percentage of participants classified as impaired decreased from Time 1 to Time 3 and that the addition of a new sign, head movements or jerks (HMJ), increased the percentage of participants classified as impaired in both the low and high THC conditions. These findings suggest that impaired performance on the SFSTs is positively related to the dose of THC administered and that the inclusion of HMJ as a scored sign in the SFSTs improves their predictive validity when testing for THC intoxication.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The Standardised Field Sobriety Tests (SFST) are currently being used by the Victorian State Police in Australia to test for driving impairment associated with drugs other than alcohol (Victorian Government Gazette 2000). The importance of such testing is highlighted by the fact that drugs other than alcohol have been detected in as many as 26.7% of drivers killed on Australian roads (Drummer et al. 2003a, b). However, the SFST battery was specifically developed to test for alcohol intoxication (Burns and Moskowitz 1977) and no empirical research has been performed to assess whether the SFSTs provide a sensitive measure of impairment following the consumption of a drug other than alcohol. Such research is required to determine whether the SFSTs are suitable for this purpose.
The SFSTs are tests of psychomotor and cognitive function and comprise the Horizontal Gaze Nystagmus (HGN), the Walk and Turn (WAT) and the One Leg Stand (OLS) tests (Burns and Moskowitz 1977; O’Keefe 2001). The SFST battery has been demonstrated to be a sensitive test of impairment related to blood alcohol concentrations (BAC) of up to 0.08% (Burns and Moskowitz 1977; Burns 1987). Furthermore, the SFSTs have previously been used in combination with physiological tests in order to assess whether individuals are under the influence of drugs (Bigelow et al. 1985; Compton 1986). However, these latter studies were performed in order to validate a 12-step testing program, the drug evaluation and classification program (DECP), rather than the SFST battery alone.
Cannabis (delta-9-tetrahydrocannabinol or THC) is the drug that has most commonly been detected in the specimens of drivers killed on Australian roads (Drummer et al. 2003a, b) and research has revealed that the consumption of THC leads to impaired cognitive and psychomotor performance (Ramaekers et al. 2004) as well as impaired driving performance (Moskowitz 1985; Hansteen et al. 1976; Smiley et al. 1981; Robbe and O’Hanlon 1993; Ramaekers et al. 2000, 2004). Therefore, the aim of the present study was to assess whether the SFSTs provide a sensitive measure of impairment following the consumption of THC. Specifically, the aims were: to determine whether consumption of THC results in impaired performance on the SFSTs and whether such impairment is related to the dosage of THC consumed; to identify which of the SFSTs, or which signs of the SFSTs, are the best predictors of impaired performance associated with THC intoxication; and to determine whether the scoring of a new sign, head movements or jerks (HMJ) during performance of the HGN test, improves the sensitivity of the SFSTs in assessing impairment following the consumption of THC. Head movements during the HGN test are considered to be a possible symptom of drug use (Victorian Government Gazette 2000) although the sign itself is not traditionally scored and is therefore not included in the SFST battery score. Therefore, in the present study, performance on the SFSTs will be assessed both with and without the sign HMJ being included in the scoring procedure.
Given that the consumption of THC has been shown to impair cognitive and psychomotor performance, it was hypothesised that the consumption of THC would result in impaired performance on the SFSTs and that there would be a positive relationship between impaired performance on the SFSTs and the dosage of THC consumed. Such a finding would support the use of the SFSTs in assessing whether the driving ability of motorists may be impaired following the consumption of a drug other than alcohol.
Method
Participants
Forty healthy participants (14 female and 26 male), aged between 21 and 35 years (M=25.5, SD=3.1) who had previously consumed cannabis were assessed. Participants were recruited through advertisements that were placed in local newspapers and on community and university noticeboards. The reported frequency of cannabis use of the subjects varied from once a week to once every 2–6 months. All participants were required to complete a medical examination that was performed by a medical practitioner. Exclusion criteria for participation were: history of cardiac disorders; history of substance abuse; history of mental health problems; history of allergic reactions to drugs and current medical illness.
Materials
Marijuana cigarettes
THC was administered to participants using cigarettes that were provided by the National Institute on Drug Abuse (NIDA) in the USA. Three different types of cigarettes were used with THC dosages of: 0% THC (placebo); a low dose of 1.74% THC (0.813 gm); and a high dose of 2.93% THC (1.776 gm). The active cigarettes contained Mississippi-grown Jamaican, Special Hybrid and Mexican marijuana. The moisture content of the low-dose cigarette was 10.8% and the moisture content of the high-dose cigarette was 11.5%. The placebo cigarettes contained Mississippi-grown Mexican marijuana which had a moisture content of 12.4%.
The Standardised Field Sobriety Tests
All three tests that comprise the SFST battery were administered, as per the administration procedures used by the Victoria Police (Victorian Government Gazette 2000). These procedures, based on those of Burns and Moskowitz (1977), are outlined below:
Horizontal and Vertical Gaze Nystagmus (HGN and VGN)
In this test, participants were required to focus on an object, located 12–15 in. in front of their face, as it moved horizontally and then vertically. The investigator separately observed the left and right eye for the following four signs: lack of smooth pursuit (LSP); distinct Nystagmus at maximum deviation (Nmax); Nystagmus onset before 45° (N45); and Nystagmus at the vertical position (VGN). If a total of four or more signs were observed, the participant was judged to be impaired to a degree equivalent to a blood alcohol concentration (BAC) of above 0.10%. An additional sign, head movements and/or jerks (HMJ), was also scored. It was recorded as being observed if, on more than one occasion, the participant was unable to keep their head still while following the moving stimulus with their eyes.
Walk and Turn (WAT)
In this test, the participant was required to take nine heel-to-toe steps along a straight line and then turn around and take another nine heel-to-toe steps back along the line. The investigator observed for eight signs of impairment, these being: could not keep balance while listening to the instructions of the test (NB); started the test before the instructions were completed (STS); stopped walking during the test (SW); did not touch heel-to-toe while walking (MHT); stepped off the line (SOL); used arms to maintain balance (AB); turned improperly (not as demonstrated during instructions) (IT); and took the incorrect number of steps (more or less than nine up and/or nine back) (INS). If the participant failed to complete the test, all eight signs were recorded as being observed. If two or more signs were observed, the participant was judged to be impaired to a degree equivalent to a BAC equal to or above 0.10%.
One Leg Stand (OLS)
In this test, the participant stood on one leg, with the other stretched out in front of them, while counting out aloud for 30 s starting from one thousand. The investigator observed for the following behaviors of the participant during performance: swayed while balancing on one leg (S); used arms to maintain balance (AB); hopped during test to maintain balance (H); put raised foot down (FD). If the participant put their foot down more than three times and/or failed to complete the test, all four signs were recorded as being observed. If two or more signs were observed, the participant was judged to be impaired to a degree equivalent to a BAC equal to or above 0.10%.
Procedure
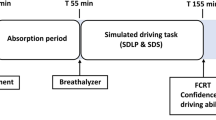
The study was approved by the Human Research Ethics Committee of Swinburne University of Technology and all participants provided informed consent. A randomised, counter-balanced, double blind, within-subject, repeated measures design was employed across three experimental sessions. In each session, an intravenous cannula was inserted into the participant’s forearm and a 10-ml blood sample was taken. The participant then consumed either a placebo, low-dose or high-dose cannabis cigarette using a controlled smoking procedure, similar to that used by Cone and Huestis (1993). Participants were instructed to inhale marijuana smoke for 2 s, hold the smoke in their lungs for 10 s (or for as long as they could if they could not hold for 10 s) and exhale and rest for 35 s. This procedure was repeated a maximum of eight times and was terminated if the cannabis cigarette had been fully consumed. Another 10-ml blood sample was then taken and a further five blood samples were taken every 20 min during the 2.5-h session. The SFSTs were performed at three time-points: 5 min after the smoking procedure had been completed (Time 1); 55 min after the smoking procedure had been completed (Time 2) and 105 min after the smoking procedure had been completed (Time 3). A research nurse was responsible for the administration of the cigarettes and for blood collection. Administration of the SFSTs was performed by an independent administrator. At the completion of testing, participants were provided with taxi transportation. To ensure an adequate washout period for THC, a minimum interval of 7 days was employed between each of the three testing sessions.
Data analysis
The seven blood samples taken from every participant were analysed for active Δ-9-THC levels using the gas chromatography/mass spectrometry (GC/MS) method, a method that is considered to be the most accurate means of testing for the presence of drugs in blood (Moeller and Kraemer 2002). The level of Δ-9-THC will subsequently be referred to as the level of THC in blood. A repeated-measures ANOVA was performed to determine whether the levels of THC in blood significantly differed between the three THC conditions at 0, 20, 50, 75, 100 and 125 min after smoking cannabis.
Under all three THC conditions, the percentage of participants that were classified as impaired was calculated for every sign of the SFSTs and for the individual tests of the SFSTs. Participants classified as impaired on two or more of the SFSTs (i.e. HGN, WAT and OLS) were classified as impaired on overall SFST performance. To determine which of the tests and which of the signs provided the best predictors of THC intoxication, chi-square (χ2) tests were performed to establish whether performance on each of the tests and presence of each of the signs was related to or independent of THC condition. Spearman’s coefficient (ρ) was then calculated to determine the strength and direction of that relationship.
Results
Blood THC levels
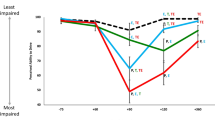
Blood samples were taken at seven different time-points during the testing procedure. The mean level of THC in blood, for the three smoking conditions, is displayed in Fig. 1. Immediately after the completion of the smoking procedure (0 min), the level of THC in the blood was 55.46 ng/ml in the low THC condition and 70.59 ng/ml in the high THC condition. The level of THC in blood then continually decreased and by 125 min after the completion of the smoking procedure, the level of THC in the blood was 2.53 ng/ml in the low THC condition and 2.42 ng/ml in the high THC condition.

Level of THC in plasma after smoking placebo, low- and high-dose cannabis cigarettes
SFST battery performance
The percentage of individuals who were classified as impaired based on the overall SFST battery performance for every THC condition, is displayed in Fig. 2 for Time 1 (5 min after the smoking procedure had been completed), Fig. 3 for Time 2 (55 min after the smoking procedure had been completed) and Fig. 4 for Time 3 (105 min after the smoking procedure had been completed). In these figures, performance on the SFSTs is displayed both with and without the sign HMJ being included in the SFST score.

Percentage of individuals classified as impaired on the Standardised Field Sobriety Tests (SFST) battery [both with and without head movements or jerks (HMJ)] at time 1, for every THC condition

Percentage of individuals classified as impaired on the SFST battery (both with and without HMJ) at time 2, for every THC condition

Percentage of individuals classified as impaired on the SFST battery (both with and without HMJ) at time 3, for every THC condition
At Time 1, impaired performance on the SFST battery was significantly related to THC condition (χ2=20.8, df=2, p<0.001) and this relationship was positive (ρ=0.4, p<0.001). When the sign HMJ was also included, the relationship between overall SFST battery performance and THC condition was found to be stronger (χ2=30.6, df=2, p<0.001) (ρ=0.5, p<0.001).
At Time 2, impaired performance on the SFST battery was significantly related to THC condition (χ2=12.3, df=2, p<0.005). This relationship was significant and positive (ρ=0.3, p<0.001). The relationship between SFST battery performance and THC condition was found to be stronger when the sign HMJ was included (χ2=16.7, df=2, p<0.001, ρ=0.4, p<0.001).
At Time 3, impaired performance on the SFST battery was significantly related to THC condition (χ2=7.9, df=2, p<0.05) and this relationship was found to be positive (ρ=0.3, p<0.01). When the sign HMJ was included, the relationship between overall SFST battery performance and THC condition was found to be stronger (χ2=10.6, df=2, p<0.01, ρ=0.3, p<0.005).
Individual SFST performance
Horizontal Gaze Nystagmus (HGN)
At Time 1 (5 min after the smoking procedure had been completed), none of the individual HGN signs (LSP, Nmax, N45, VGN) were significantly related to THC condition, nor was overall HGN performance. When HMJ was included as a scored sign however, overall HGN performance was related to THC condition (χ2=16.3, df=2, p<0.001). This relationship was positive (ρ=0.3, p<0.005). The inclusion of HMJ greatly increased the percentage of participants who were classified as impaired on the HGN test. In the low THC condition, 2.6% of participants were classified as impaired when HMJ was not included, compared with 33.3% of participants when HMJ was included. In the high THC condition, 5.1% of participants were classified as impaired when HMJ was not included, compared with 30.8% of participants when HMJ was included. The inclusion of HMJ did not increase the number of individuals classified as impaired in the placebo session.
At Time 2 (55 min after the smoking procedure had been completed), the HGN sign LSP was significantly related to THC condition (χ2=12.7, df=2, p<0.005) and this relationship was positive (ρ=0.3, p<0.001). Overall HGN impairment was significantly related to the level of THC (χ2=12.4, df=2, p<0.005) and the relationship was positive (ρ=0.3, p<0.005). When the sign HMJ was included in the overall HGN score, the relationship between THC condition and impairment on the HGN test was stronger than when HMJ was not included (χ2=18.4, df=2, p<0.001; ρ=0.4, p<0.001).
At Time 3 (105 min after the smoking procedure had been completed), the sign LSP was significantly related to THC condition (χ2=15.2, df=2, p<0.005). This relationship was positive (ρ=0.3, p<0.001). Overall HGN impairment was also significantly related to THC condition (χ2=7.5, df=2, p<0.05). This relationship was also positive (ρ=0.2, p<0.01). The relationship between HGN and THC condition was strengthened when HMJ was included as a scored sign (χ2=11.414, df=2, p<0.005) (ρ=0.310, p<0.005).
Walk and turn test
At Time 1, the WAT signs NB, MHT, SOL and AB were significantly related to THC condition (χ2=10.2, df=2, p<0.05; χ2=8.7, df=2, p<0.05; χ2=13.9, df=2, p<0.005; χ2=6.6, df=2, p<0.05). Each relationship was positive and significant (ρ=0.3, p<0.005; ρ=0.3, p<0.005; ρ=0.3, p<0.001, ρ=0.2, p<0.05, respectively). There was also a significant relationship between overall WAT performance and THC condition (χ2=12.5, df=2, p<0.005). This relationship was also positive (ρ=0.3, p<0.001).
At Time 2 the WAT signs NB, SOL, and AB were significantly related to THC condition (χ2=9.4, df=2, p<0.01; χ2=9.1, df=2, p<0.05; χ2=17.6, df=2, p<0.001). The relationships were all positive (ρ=0.3, p<0.005; ρ=0.3, p<0.01; ρ=0.4, p<0.001). There was also a significant relationship between overall WAT impairment and THC condition (χ2=10.0, df=2, p<0.01). This relationship was positive (ρ=0.3, p<0.005).
At Time 3, the WAT signs NB, SW and AB, were significantly related to THC condition at time three (χ2=6.6, df=2, p<0.05; χ2=8.4, df=2, p<0.05; χ2=8.1, df=2, p<0.05). These relationships were positive (ρ=0.2, p<0.05; ρ=0.2, p<0.05; ρ=0.3, p<0.005). There was also a significant relationship between overall WAT performance and THC condition at time three (χ2=6.1, df=2, p<0.05). This relationship was significant and positive (ρ=0.2, p<0.05).
One leg stand
At Time 1, all signs of the OLS test (S, AB, H and FD) were significantly related to THC condition (χ2=14.5, df=2, p<0.005; χ2=16.7, df=2, p<0.001; χ2=9.5, df=2, p<0.01; χ2=13.4, df=2, p<0.005). All relationships were positive (ρ=0.3, p<0.005; ρ=0.3, p<0.001; ρ=0.3, p<0.005; ρ=0.3, p<0.005, respectively). Overall OLS performance was also related to THC condition at time one (χ2=25.0, df=2, p<0.001). This relationship was also positive (ρ=0.4, p<0.001).
At Time 2, all the signs of the OLS test (S, AB, H and FD) were significantly related to THC condition (χ2=13.8, df=2, p<0.005; χ2=9.7, df=2, p<0.01; χ2=6.2, df=2, p<0.05; χ2=15.8, df=2, p<0.001). Each sign was also significantly correlated with THC condition (ρ=0.3, p<0.001; ρ=0.3, p<0.005; ρ=0.2, p<0.05; ρ=0.4, p<0.001). Subsequently, overall OLS impairment was also related to THC condition at time two (χ2=18.2, df=2, p<0.001). This relationship was also positive (ρ=0.4, p<0.001).
At Time 3, the OLS signs S, AB, and FD were significantly related to THC condition at time three (χ2=22.2, df=2, p<0.001; χ2=17.6, df=2, p<0.001; χ2=17.0, df=2, p<0.001). These relationships were all positive (ρ=0.4, p<0.001; ρ=0.4, p<0.001; ρ=0.4, p<0.001). Overall OLS impairment was also related to THC condition (χ2=19.0, df=2, p<0.001). This relationship was positive (ρ=0.4, p<0.001).
Discussion
The findings of the present study reveal that the consumption of THC does impair performance on the SFSTs. More specifically, the results revealed that the higher the content of THC consumed, the greater the number of participants that were classified as impaired to a degree equivalent to a BAC of above 0.10%. The results also revealed that when the sign HMJ was scored, the percentage of participants whose performance was classified as impaired was greater than when HMJ was not scored.
The results indicated that the consumption of cannabis containing either 1.74% THC or 2.93% THC impaired performance on the SFSTs. The level of THC in the blood related to the consumption of these levels of THC ranged between approximately 70 ng/ml and 2 ng/ml. At all three time-points (5, 55 and 105 min after the smoking procedure had been completed) performance on the overall SFST battery was moderately related to the level of THC consumed. In the high THC condition, 46.2% of individuals were classified as impaired at Time 1, 41% were classified as impaired at Time 2, and only 28.2% were classified as impaired at Time 3. These results suggest that the SFST battery is a moderate predictor of impairment caused by low and high doses of cannabis. These findings are consistent with those of Bigelow et al. (1985), in which 55% of drug intoxicated participants were classified as impaired, but are lower than the 94% of cases that were classified as impaired in Compton (1986). It is necessary to consider though, that in both of those previous studies the DECP sobriety testing method was employed, which includes not only the SFSTs, but also involves more detailed physiological testing procedures.
Previous research suggests that the DECP program has an optimal ability to predict impairment caused by cannabis consumption when 28 variables are used (Heishman et al. 1996). In contrast, the standard administration of the SFSTs involves only 16 variables. It is therefore possible that the scoring of more signs during performance of the SFSTs may result in a higher percentage of individuals being correctly classified as impaired by a drug. Indeed, the results of the present study indicate that when only one additional sign was scored, HMJ during the HGN, the percentage of individuals classified as impaired was increased by 10.2%. Importantly, the inclusion of the sign HMJ did not result in individuals in the placebo condition being misclassified. This suggests that HMJ only occurred as the result of THC intoxication and that the scoring of this sign did not increase the number of false positives that were recorded. These findings indicate that it would be beneficial to include HMJ when assessing performance on the SFSTs and also suggest that it may be pertinent to score even more drug-sensitive signs when assessing SFST performance. Since the SFST battery has not been validated for the detection of drugs, further research is required to determine whether the addition of new signs may improve the accuracy of the SFSTs in detecting impairment associated with THC consumption. The performance of subjects on the component tests of the SFSTs, the HGN, WAT and OLS, suggests that the administration of THC impairs an individual’s ability to execute fine movements, to follow instructions and to concentrate their attention on the task at hand. Therefore, additional tests and signs that assess these elements may be suitable additions to the SFST scoring procedure.
It is necessary to consider how the findings of the present study relate to real-world scenarios. The findings indicate that the SFSTs provide sensitive measures of impairment, even when a relatively low dose of THC has been consumed. It is difficult to ascertain whether the percentages of THC administered in the present study are similar to the percentage of THC contained in commonly obtained street cannabis as available data does not reveal the strength of seized cannabis. However, the blood levels that were observed in the present study were similar to the mean blood levels that have been reported in drivers killed on Australian roads (Drummer et al. 2003a).
It should also be considered that the present study was clinically controlled and that subjects were under the influence of THC only at the time of testing. As such, the findings of this study validate the application of the SFSTs to assess drivers who have consumed THC alone, but the application of the SFSTs to assess drivers who have consumed THC in combination with other drugs can only be inferred from the findings of the present study. Statistics from previous studies indicate that in many drivers, THC has been detected in combination with other drugs. The findings of Drummer et al. (2003a, b) indicate that for the period in which levels of THC were measured (1997–1999), 47% of drivers killed displayed THC alone, 36% displayed THC in combination with alcohol and 16.5% displayed THC in combination with drugs other than alcohol. Therefore, it is important that further studies are performed to determine whether roadside testing with the SFSTs may be suitable for assessing drivers who are under the influence of a combination of drugs.
Individual tests
Horizontal Gaze Nystagmus
Impaired performance on the HGN test was related to THC condition at Time 2 (55 min after the smoking procedure had been completed) and Time 3 (105 min after the smoking procedure had been completed) but not at Time 1 (5 min after smoking cannabis). Both Time 2 and Time 3 occurred during the elimination phase in which ‘dumped’ THC re-enters the blood stream (Chesher 1997). Using the standard scoring procedure for the SFSTs, the primary indicator of impairment during the HGN test was the sign LSP which was significantly related to THC dosage at Time 2 and Time 3. This finding is consistent with that of Fant et al. (1998) who found that the velocity of smooth pursuit eye tracking was significantly decreased following the consumption of both low and high doses of THC (1.8 and 3.6% THC) whilst performance on all other cognitive and psychomotor tests that were employed was not impaired. The findings are also consistent with those of Adler and Burns (1994) who found that LSP was present in 60% of individuals who had been arrested for drug use and whose specimen had tested positive for marijuana. However, many of those subjects had also tested positive for substances other than THC. It should be considered that in the present study, blood samples were only tested for THC and as such, it is possible that the LSP displayed by subjects may have occurred as the result of consumption of drugs other than cannabis. Participants were, however, requested to refrain from drug use for 7 days prior to the commencement of the testing session and were screened for past and present drug use using a medical questionnaire.
While LSP was the primary indicator of impairment during the HGN test when the standard scoring procedure was adopted, the scoring of the sign HMJ provided a better indicator. Of all the SFST signs that were scored, HMJ was the most commonly observed at both Time 1 and Time 2. Furthermore, scoring HMJ improved the strength and significance of the relationship between the HGN test and THC condition. This suggests that the inclusion of HMJ increases the likelihood that the HGN test will detect whether an individual is impaired after smoking cannabis containing either low or high levels of THC.
Walk and turn test
The WAT test was related to THC condition in all administrations of the test. Overall impairment on the WAT was related to the dose of THC, so that individuals were more likely to be classified as impaired (equivalent to a BAC above 0.10%) after smoking low or high dose THC cigarettes. Two signs of the WAT test were observed at all times—NB (No Balance) and AB (Arms used to Balance). At Time 1, Time 2 and Time 3, in both the low and high dose conditions, balance was significantly impaired. These findings suggest that the administration of THC impairs the ability to maintain balance, as well as to focus attention.
It is important to note that three signs of the WAT test were unrelated to the level of THC at all administrations of this test: MHT (Misses Heel to Toe), IT (Improper Turn) and INS (Incorrect Number of Steps). These signs appeared almost as often in the placebo session as they did in the THC conditions and are therefore likely to be observed irrespective of drug consumption. This suggests that the inclusion of these signs may result in a high incidence of false positives being recorded and as such, further research is required to determine whether such signs should be excluded from the SFST scoring procedures.
One leg stand test
Of the three tests of the SFSTs, the OLS test provided the best indicator of impairment associated with the administration of THC. Overall performance on the OLS was significantly related to the level of THC at all testing times, as was performance on all of the scored signs of this test, except for hopping at Time 3. It has previously been argued that the OLS may be too sensitive for determining drug use and that many individuals may not have very good balance even when they are not under the influence of drugs (Jackson et al. 2000). However, replication of the findings of the present study would suggest that it may be appropriate to weigh the OLS score more highly than the other two SFST scores when determining whether an individual is under the influence of THC.
In conclusion, the results of the present study suggest that smoking cannabis cigarettes that contained either 1.74% THC or 2.93% THC significantly impaired performance on the SFSTs. These findings suggest that in the absence of reliable and accurate physical tests of THC blood levels, the SFSTs may provide a valuable tool when screening for drug intoxication. Furthermore, the predictive validity of sobriety tests may be improved by scoring additional signs such as HMJ and/or by including additional tests of impairment. The findings of this study may be of benefit to law enforcement agencies in many countries that are currently using, or are considering using, performance tests to test for driving impairment associated with the consumption of a drug other than alcohol.
References
Adler EV, Burns M (1994) Drug Recognition Expert (DRE) validation study. Final report. Arizona Department of Public Safety and Southern California Research Institute
Bigelow GE, Bickel WE, Roache JC, Liebson IA, Nowowieski P (1985) Identifying types of drug intoxication: laboratory evaluation of a subject examination procedure (Johns Hopkins Study), final report. Behavioural Pharmacology Research Unit, Department of Psychiatry and Behavioural Sciences, Publication No. DOT HS 806 753
Burns M (1987) Sobriety tests for the presence of drugs. Alcohol Drugs Driv 3(1):25–29
Burns M, Moskowitz H (1977) Psychophysical Tests for DWI Arrest. U.S. Department of Transportation, National Highway Traffic Safety Administration. Final Report, Publication No. DOT-HS-5-01242
Chesher GB (1997) Cannabis and road safety: an outline of the research studies to examine the effects of cannabis on driving skill and actual driving performance. http://yarra.vicnet.net.au/~parlrsc/drugches.htm
Compton RP (1986) Field evaluation of the Los Angeles Police Department drug detection procedure (173 Case Study). A NHTSA Technical Report, National Highway Traffic Safety Administration. Publication No. DOT HS 807 012
Cone EJ, Huestis MA (1993) Relating blood concentrations of tetrahydrocannabinol and metabolites to pharmacological effects and time of marijuana usage. Ther Drug Monit 15:527–532
Drummer OH, Gerostamoulos J, Batziris H, Chu M, Caplehorn JRM, Robertson MD, Swann P (2003a) The incidence of drugs in drivers killed in Australian road traffic crashes. Forensic Sci Int 134:154–164
Drummer OH, Gerostamoulos J, Batziris H, Chu M, Caplehorn JRM, Robertson MD, Swann P (2003b) The involvement of drugs in drivers of motor vehicles killed in Australian road traffic crashes. Accident Anal Prev 943:1–10
Fant RV, Heishman SJ, Bunker EB, Pickworth WB (1998) Acute and residual effects of marijuana in humans. Pharmacol Biochem Behav 60(4):777–784
Hansteen RW, Miller RD, Lonero L, Reid LD, Jones B (1976) Effects of cannabis and alcohol on automobile driving and psychomotor tracking. Ann NY Acad Sci 282:240–256
Heishman SJ, Singleton EG, Crouch, DJ (1996) Laboratory validation study of drug evaluation and classification program: ethanol, cocaine, and marijuana. J Anal Toxicol 20(6):468–483
Jackson PG, Tunbridge RJ, Rowe DJ (2000) Drug recognition and field impairment testing: Evaluation of trials. In: Laurell H, Schlyter F (eds) Alcohol, drugs and traffic safety. Proceedings of the 15th International Conference on alcohol, drugs and traffic safety, Stockholm, Sweden, May 21–26, 2000
Moeller MR, Kraemer T (2002) Drugs of abuse monitoring in blood for control of driving under the influence of drugs. Ther Drug Monit 24(2):210–221
Moskowitz H (1985) Marijuana and driving. Accident Anal Prev 17:323–345
O’Keefe M (2001) Drugs driving-standardized field sobriety tests: a survey of police surgeons in Strathclyde. J Clin Forensic Med 8:57–65
Ramaekers JG, Lamers CTJ, Robbe HWJ, O’Hanlon JF (2000) Low doses of marijuana and alcohol severely impair driving when taken together. In: Laurell H, Schlyter F (eds) Alcohol, drugs and traffic safety. Proceedings of the 15th International Conference on Alcohol, Drugs and Traffic Safety, Stockholm, Sweden, May 21–26, 2000
Ramaekers JG, Berghaus G, van Laar M, Drummer OH (2004) Dose related risk of motor vehicle crashes after cannabis use. Drug Alcohol Depend 73(2):109–119
Robbe HWJ, O’Hanlon J (1993) Marijuana and actual driving performance. United States Department of Transportation, National Highway Traffic Safety Administration. Report No. DOT HS 808 078
Smiley A, Moskowitz H, Ziedman K (1981) Driving simulator studies of marijuana alone and in combination with alcohol. 25th Conference of the American Association for Automotive Medicine, Proceedings, 107–116
Victorian Government Gazette (2000) No. G 46 Thursday 16 November 2000, 2723 (G 46)–2725 (G 46). Traffic Alcohol Section, Victoria Police, Victoria Australia
Acknowledgements
The authors wish to thank the National Institute on Drug Abuse for supplying the THC cigarettes used in this study, Dr. Edward Ogden of Swinburne University and Professor Phillip Swann of Vicroads.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Papafotiou, K., Carter, J.D. & Stough, C. An evaluation of the sensitivity of the Standardised Field Sobriety Tests (SFSTs) to detect impairment due to marijuana intoxication. Psychopharmacology 180, 107–114 (2005). https://doi.org/10.1007/s00213-004-2119-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-004-2119-9