
Abstract
Rationale
Diazepam has well known amnestic and sedative effects but effects on fronto-executive function remain largely uninvestigated, especially on neuropsychologically validated tests of risk taking and orbitofrontal cortex function.
Objectives
We aimed to determine the impact of diazepam on a variety of executive tasks.
Methods
The effects of 5, 10 and 20 mg of diazepam on a battery of neuropsychological tests were investigated using a randomised, double blind, placebo-controlled design. Seventy-five adult men were recruited. The Rogers et al. (1999b) test of risk-taking was given along with tasks from the CANTAB battery.
Results
Diazepam impaired performance on the Tower of London test of planning, without influencing visual pattern recognition memory. Subjects who had taken diazepam made more risky choices on the risk-taking task. On two speeded reaction time tasks diazepam impaired discrimination sensitivity and increased the bias to respond.
Conclusions
In contrast to the well-known sedative effects of diazepam, we demonstrate disinhibitory effects on two speeded reaction time tasks. Our results show that diazepam can impair performance on reaction time tasks both by impairing sensitivity and by increasing the bias to respond. Furthermore diazepam impaired performance on tests of planning and risky decision making that depend predominantly on dorsolateral and orbitofrontal regions of the prefrontal cortex, respectively.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The ability of human subjects to make decisions enabling them to select optimal responses and strategies in a complex and changing environment is clearly of fundamental importance to people’s lives, and is the subject of a good deal of recent research both in the laboratory and within the clinical setting (see Rahman et al. 2001, for review). Much of this research has implicated a central role for specific regions of the orbital prefrontal cortex (PFC) and its connections with other brain structures in supporting these abilities (Bechara et al. 1994; Rahman et al. 1999). Diazepam, a benzodiazepine receptor agonist, is in wide clinical use as an anxiolytic, and has well-understood GABA-ergic effects (Feldman et al. 1996). In recent years, it has been implicated in effects on functions associated with processing within the orbital PFC (e.g. Blair and Curran 1999); however, there have been few, if any, studies of its effects on decision-making cognition.
In a series of studies, Coull et al. (1995a, 1995b) showed that diazepam influenced performance on a range of tasks sensitive to frontal lobe dysfunction including tests of planning, extra-dimensional attentional shifting and spatial working memory (Dias et al. 1996; Owen et al. 1990, 1995b). We used a more sensitive variant of the planning task used by Coull et al. (1995b) namely the One-touch Tower of London test (OTToL; Owen et al. 1990). This task has similar planning demands, but is designed to be less susceptible to premature initial moves, as may have occurred in previous studies of diazepam (Coull et al. 1995b). We tested the influence of diazepam on responding on the OTToL task in order to investigate any possible effects of the drug on planning when the opportunity of impulsive first moves was reduced. A variant on the intra-dimensional/extra-dimensional (3D ID/ED) set-shifting task using three concurrent stimulus dimensions has been developed to exert a greater attentional demand. We employed this task, along with the Rapid visual information processing task (RVIP) to further investigate the effects reported by Coull et al. (1995a) on sustained attention. The set-shifting tasks also include a component that involves reversal of previously established response contingencies, which appeared uninfluenced by diazepam.
This finding suggests no influence of diazepam on any tendency of a previously correct response to be incorrectly produced following a rapid change of task requirements. This was further investigated by the inclusion of a task requiring the successive reversal of response rules in a Go/No-Go discrimination. Both the RVIP and the Go/No-Go task are amenable to a signal detection analysis from which one can compute measures of discrimination sensitivity and the criterion for responding.
Further analyses of the effects of diazepam in terms of executive control were undertaken in the domain of decision making and resolution of conflict. Traditional models of anxiety in rats have relied on a notion of reinforcer “conflict”: for example, operant responding may simultaneously be rewarded with food and punished with electric shock. Effective anxiolytics, including diazepam, commonly increase responding in these paradigms (Feldman et al. 1996). A recent risk-taking task developed to investigate decision-making in humans (Rogers et al. 1999b), has elements in common with these traditional tasks. In the risk-taking task, the reward (and penalty) associated with gambling on a less likely outcome is larger than that associated with gambling on the more likely outcome. Possible effects of diazepam on decision making in this “conflict” situation were investigated by the inclusion of this risk-taking task.
Finally, diazepam has well recognised amnestic effects (e.g. Curran 1999). However the effects of diazepam on the immediate and delayed pattern recognition task from the CANTAB battery, previously used in psychopharmacological studies (Sahakian et al. 1988; Rubinsztein et al. 2000) and sensitive to temporal lobe lesions and amygdalo-hippocampectomy (Owen et al. 1995b), have previously not been assessed.
Materials and methods
The study was approved by the Local Research Ethics Committee (LREC 00/45) and all subjects gave informed consent.
Subjects
Seventy-five normal healthy male volunteers were recruited by advertisement in the community. Participants were a mix of students and individuals in part-time employment. None of the volunteers were receiving concurrent medication or had a history of severe medical, psychiatric or neurological illness. All volunteers were asked to abstain from alcohol for 24 h pre- and post-drug. Volunteers were also instructed not to drive or operate heavy machinery for 24 h after having taken the tablet. After having taken the capsule and until the end of the session subjects were asked not to consume anything containing caffeine. The study was conducted as two experiments. In experiment 1 (low dose diazepam) (n=45), each subject was randomly assigned to one of three groups. One group was given placebo, another 5 mg diazepam and the third 10 mg. In experiment 2 (high dose diazepam) (n=30) subjects were randomly assigned to one of two groups. One group received placebo and the other received 20 mg diazepam. Both the experimenter and the subject were blind to the contents of the capsule. Subject details are set out in Table 1.
Testing procedure
Before taking the capsule, all subjects completed the National Adult Reading Test (NART; Nelson 1982) in order to estimate verbal IQ. Cognitive testing began 40 min after the subject had taken the capsule. Computerised tests were performed on an Advantech PPC (120-T) touchscreen computer. Subjects were seated comfortably ~0.5 m away from the touch-sensitive screen. The tests were given in the following order: Risk, RVIP, Immediate pattern recognition, Go/No-Go, Delayed pattern recognition, One-touch Tower of London, 3D ID/ED.
Visual analogue scales (VAS; Bond and Lader 1974)
Prior to ingestion of either drug or placebo, subjects were asked to rate subjective feelings of alertness, contentedness and calmness, using the scales proposed by Bond and Lader (1974). Administration of this test was repeated 1 h after tablet ingestion, and at the end of testing.
“Risk” decision-making task (Rogers et al. 1999b)
In this task, subjects make gambling decisions on whether a token is hidden behind one of the red boxes or blue boxes at the top of the screen. The subject is told that there is an equal probability that the token will be hidden inside any of the six boxes, thus the odds in favour of each gamble is governed by the ratio of red to blue boxes. Each decision involves gambling a certain number of points associated with that choice on that trial.
The ratio of the coloured boxes (5:1, 4:2, 3:3) and the balance between the associated rewards (10 versus 90, 20 versus 80, 30 versus 70, 40 versus 60 and 50 versus 50) varied independently from trial to trial according to a fixed pseudo-random sequence. This sequence ensured that each balance of reward and each ratio of coloured boxes co-occurred an equal number of times, with the restriction that on all trials with an unequal ratio of red and blue boxes (i.e. 5:1 or 4:2) the larger reward was always associated with the least likely outcome (i.e. the colour with the fewest number of boxes), thus capturing the conflict in risk taking situations. The decision latency and average number of points per bet were recorded: A higher average bet reveals a tendency to risk larger amounts with correspondingly lower likelihoods of winning.
Rapid visual information processing (Sahakian et al. 1989)
This is a task of attentional vigilance with a working memory component from the CANTAB (www.camcog.com) battery. One of eight different digits appears in pseudo-random order on a computer screen at a rate of 100 digits per minute for 7 min. Subjects are asked to detect consecutive odd or even sequences of digits (viz 357; 246; 468; 579), and to register responses with a button press.
Target sequences occur at the rate of 16 every 2 min, and the computer calculates the number of button presses to each of the four target sequences, within a period of 1.5 s post-presentation (“hits”), the number of button presses which incorrectly identified a target sequence (“false alarms”), and the latency to press the response button for each correct “hit”. Performance indices comparable with previous studies (Coull et al, 1995a) were calculated from the results: A’ (sensitivity to difference between targets and non-targets) and B’’ (tendency to withhold responding), as derived from signal detection theory (Grier 1971). In order to avoid infinite values for the calculation of B’’, 0.5 was added to all data cells as proposed by Snodgrass and Corwin (1988).
Go/No-Go task
In this task, the subject was required to respond rapidly to some stimuli but withhold responding to others. The subject was presented with successive characters on the computer screen from one of the two stimulus categories present: letters and numbers. The task consisted of ten blocks. On each block, 18 stimuli were presented successively on the screen for 300 ms with an inter-stimulus interval of 900 ms. Half the stimuli were targets and half were non-targets and they were presented in a pseudo-random order.
The subject was instructed to tap the space bar of the keyboard as quickly as possible when a stimulus from the target category appeared. Before the start of each block written instructions were given as to whether the next target category was letters or numbers. The first two blocks were practice blocks. The target category then changed every alternate block until ten blocks had been completed. Thus blocks 3, 5, 7 and 9 were switch blocks, where the target category of the previous block became the non-target category, and vice versa. After each block, the subject was given feedback about errors and latency performance on that block. A low tone of 450 Hz sounded for 500 ms after each false positive error. Misses did not trigger any feedback from the computer. The mean correct “go” latency was calculated for each block, along with the overall proportion of misses and false positive errors across switch and non-switch blocks. These were used to calculate the sensitivity measure A’ and bias measure B’’(see above) for switch trials and non-switch trials.
One-touch Tower of London (Owen et al. 1995a)
This is a test of planning, modified from the CANTAB Tower of London task. Participants are first trained with a number of problems from the CANTAB Tower of London task, before moving onto this task for which two sets of coloured balls appear on the screen, one in the upper half of the screen and one in the lower half. The numbers 1–6 are printed in large boxes across the bottom of the screen. The participants are instructed to examine the positions of the balls on the screen and then to imagine how they might re-arrange the balls in the lower display to match the ones in the upper display. The participants are asked to find the solution that requires the minimum number of moves, and then to press the corresponding number on the bottom of the screen. If a subject’s first response is incorrect, he is required to try again until the correct number is selected. The importance of accuracy rather than speed of response is emphasised. After the practice problems, test trials of varying problem difficulty are given, arranged in a consistent, pseudorandom order. For the purposes of analysis, problems that could be completed in fewer than four moves were classified as easy and problems that could only be completed in four or more moves were classified as hard.
Three-dimensional ID-ED attentional set-shifting task (Rogers et al. 1999a)
This is a test of attentional set shifting based in part on the Wisconsin card sort test (Milner 1964) and its elaboration in the intradimensional/extradimensional set shifting task (Downes et al. 1989). There are eight stages described in detail in Rogers et al. (1999a). In all stages, participants were requested to learn a series of two alternative forced choice discriminations and their reversals. The stimuli varied independently along three dimensions of colour, number and shape. In the first stage the subject was required to learn a simple visual discrimination (SD) in which one exemplar was correct (e.g. red) and the other incorrect (e.g. blue). In this first stage the stimuli only varied across one dimension (e.g. colour). In the compound discrimination (CD) stage the contingencies remained the same but the stimuli varied across all three possible dimensions. In the intradimensional (ID) shift stage, the relevant dimension (e.g. colour) remained the same, but two entirely novel stimuli were presented. In the extradimensional (ED) shift stage participants were required to shift response set to a previously irrelevant dimension (e.g. shape). Each of these four stages was followed by a reversal stage in which the previously incorrect stimulus became the correct stimulus. If these discriminations were not achieved following 50 attempts the task was terminated. For each stage of the test that was completed the following measures were taken: the proportion of correct responses, and the latency to complete each stage.
Immediate and delayed pattern recognition (Sahakian et al. 1988; Rubinsztein et al. 2000)
This is a test from the CANTAB battery which assesses recognition memory for patterns. Twelve abstract coloured patterns were presented sequentially. In the recognition test, two patterns (one seen, one novel) were presented on each trial with the target patterns in the reverse order. Subjects were asked to respond by touching the pattern they had already seen. This procedure was then repeated with 12 new patterns. Delayed pattern recognition (DPR) was assessed by repeating the recognition phases after a 20-min interval.
Analysis
As two separate placebo groups were used, the data for each subject in the drug conditions were expressed as standard deviates of the performance on that measure in the relevant placebo group (as Z-scores). The size of this score therefore corresponds to the effect of the specific dose upon the measure.
ANOVA models were used to test for hypothesis about the effects of diazepam, using SPSS for Windows version 10. An overall effect of diazepam on a given measure was thus assessed by testing the F-statistic calculated from the intercept term in the ANOVA model; whereas the F-statistic contrasting the mean Z-scores for different dose groups assessed the dose-dependency of any effect. Appropriate repeated-measures factors were included in the model when required.
Results
Visual analogue scales
The effect of diazepam on these derived factors is shown in Table 2; they were analysed by ANCOVA models contrasting the three effects at the two post-drug tests, with the pre-drug (baseline) measure included as a covariate.
Alertness
There was no overall effect of drug on alertness, nor any dose-dependent effect (F<1). Subjects taking diazepam tended to get drowsier relative to their placebo control subjects as the experiment progressed [F(1,41)=5.462, P=0.024].
Contentment
Diazepam did not have any overall effect on the contentment measure, nor any dose or time-dependent effect [largest F(2,41)=1.95]. There was a significant interaction of drug dosage and time on the contentedness measure; there was a tendency for subjects in the 5 mg group to become relatively less contented than their controls across the session, with the opposite trend in the 20 mg group [F(2,41)=3.419, P=0.04].
Calmness
Diazepam tended to make people significantly calmer [F(1,41)=4.377, P=0.043], with different doses having different effects [F(1,42)=3.185, P=0.052]. The 5 mg dose produced a greater calming effect relative to placebo than did the 10 mg or 20 mg doses of diazepam. The effect of diazepam interacted with time [F(1,41)=6.220, P=0.017]; Table 2 shows that diazepam produced a greater calming effect at the first post-drug measurement.
Effects of sedation
Although diazepam produced significant sedative effects, none of the significant effects described below was abolished when VAS alertness score was included as a covariate. Furthermore, the VAS alertness score was never a significant covariate when included in the models described.
Immediate and delayed pattern recognition
Errors
There was no overall effect of diazepam on the number of errors made (F<1). There was a marginally significant trend for larger doses of diazepam to decrease accuracy more than small doses [F(2,42)=2.488, P=0.095]. There were no differences in the effects of diazepam between the two different delays (F<1).
Latency
There was no overall effect of diazepam on the latency for correct responses [F(1,42)=1.996, P=0.165]. There was a non-significant change in effect with dose [F(2,42)= 2.845, P=0.069]. Subjects taking 10 mg showed a slight decrease in latency relative to placebo, whereas subjects taking 5 mg were slower relative to placebo and subjects taking 20 mg were slowest of all.
3D ID/ED
Seven subjects failed to complete all eight stages: one subject from the first placebo group, and three from the 20 mg group failed at the EDS stage, and three from the 5 mg group failed at the EDR stage. The three subjects who did not attempt the EDR stage were given a proportion correct score of zero for this stage. Analysis contrasted performance on the pre-shift, ID shift and ED shift discriminations along with the grouped reversals due to the low variability in the preshift stages.
Proportion correct
There was no overall effect of diazepam on proportion correct, nor different effects of the different doses [larger F(2,42)=1.264, P=0.26]. The effect of diazepam did not change across stages (F<1), and there was no dose by stage interaction [F(6,1)=1.844, P=0.096].
Latency
Subjects on diazepam were slower than subjects on placebo [F(1,40)=5.017, P=0.030]. The effect of diazepam on latency was not influenced by stage, or dose, or any interaction between these factors [largest F(2,97)=92.2.72, P=0.10].
RVIP
Four subjects became distracted part way through this task and failed to complete it: two were in the second placebo group, one had taken 10 mg diazepam and one had taken 20 mg. These subjects are excluded from all analyses of this task.
Accuracy and response bias
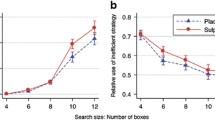
The effect of diazepam on the discriminability measure (A’) is shown in Fig. 1. Diazepam had a dose dependent effect on A’ [F(2,40)=9.151, P=0.001]; 20 mg reduced sensitivity more than did the 5 and 10 mg doses, which had no detectable effect. Diazepam also influenced the response bias measure B’’, (Fig. 1), consistent with the drug reducing the tendency to withhold a response [F(1,40)=8.572, P=0.006].

The top graph shows the effects of diazepam on A’ in the switch and non-switch conditions of the Go/No-Go task (GNG) and the RVIP task. The lower graph shows the effects of diazepam on B’’ in the switch and non-switch conditions of the GNG and the RVIP task. The bars represent Z-scores derived from the appropriate placebo condition
Latency
Diazepam 20 mg tended to lengthen reaction time more than lower doses [F(2,40)= 6.135, P=0.005].
Go/No-Go
Accuracy and response bias
Diazepam had a non-significant tendency to reduce the ability of subjects to discriminate targets from non-targets [F(1,42)=3.481, P=0.069]. However, as Fig. 1 shows, diazepam impaired sensitivity more on the switch blocks than on the non-switch blocks [F(1,42)=10.232, P=0.003] (see Fig. 1); This impariment was larger for the 20 mg than the 5 and 10 mg doses [F(2,42)=3.477, P=0.040].
Diazepam did not change the overall tendency to withhold a response (F<1), but differentially affected this measure on switch and non-switch trials [F(1,42)=5.675, P=0.022]. Further analyses showed an overall effect of diazepam in significantly increasing the “go” bias on switch blocks [t(44)=−2.119, P=0.040], but no effect on non-switch blocks [t(44)=1.311, P=0.197].
Latency
Diazepam had no overall nor dose-dependent effect on latency and there was no interaction with switching [largest F(1,42)=2.643].
Summary of Go/No-Go and RVIP
The requirements of these tasks are somewhat different, for example the “targets” (stimuli to which responding is correct) are sparser in the RVIP. This is reflected in differences in the response biases in all groups being more positive in the RVIP (see Table 2). Nevertheless, the difficulty of these tasks, as indexed by the A’ measure, is comparable, with the Go/No-Go being slightly easier, especially in the non-switch blocks. Diazepam had broadly similar effects of reducing sensitivity, and increasing the tendency to respond in the more difficult conditions (RVIP and Go/No-Go switch blocks; see Fig. 1).
Risk
The standardised effects of diazepam on the different measures from the Risk task are shown in Fig. 2.

The top graph shows the effects of diazepam on percent bet at different odds of winning (5:1, 4:2, 3:3) in the Risk decision-making task. The lower graph shows the effects of diazepam on the deliberation time. The bars represent Z-scores derived from the appropriate placebo condition
Average percent bet
Diazepam had no overall effect on average percent of points risked, nor was any effect influenced by different doses or ratio condition [largest F(2,84)=2.088, P=0.13]. There was a significant interaction between dose and ratio conditions on the effect of diazepam: Fig. 2 shows this to be due to a significant tendency for subjects who took 20 mg to bet more than their placebo controls in the critical 5:1 ratio condition [F(3,58)=5.035, P=0.005]. This condition is that in which there is greatest “conflict” between high reward magnitude and low reward probability.
Deliberation time
There was a non-significant tendency for diazepam to slow decisions in all groups (see Fig. 2) [F(1,42)=2.953, P=0.093]. The effect of diazepam on reaction time was not attenuated by dose, ratio nor any interaction of these factors (F<1).
One-touch Tower of London
Attempts needed
Diazepam did not produce an overall or dose-dependent effect on the number of attempts to solve problems (F<1). However, diazepam did have different effects on hard and easy problems—the increase in errors on hard problems was exaggerated after taking diazepam [F(1,42)=4.534, P=0.039] (see Fig. 3). This effect was dose-dependent [F(2,42)=6.328, P<0.01], with 20 mg increasing the number of attempts at the hard problems more than the other doses.

The top graph shows the effect of diazepam on the number of attempts needed to solve the Tower of London problem. The lower graph shows the effect of diazepam on the amount of time to solve a Tower of London problem in the first attempt. The bars represent Z-scores derived from the appropriate placebo condition
Latency
There was a significant dose-dependent effect of diazepam on latency to an accurate first response [F(2,42)=4.085, P=0.024]: 10 mg diazepam slowed solution more than did 5 or 20 mg diazepam. No other interactions or effects were significant [larger F(2,42)=1.141] (see Fig. 3). Analysis of the effect of diazepam on the latency to make any response, whether accurate or not, revealed no significant effects [largest F(2,42)=2.725], suggesting that the increase in solution latency was not an artefact of generalised increase in response latency, but rather an increase in thinking time required for accurate responding.
Summary
Diazepam 20 mg decreased accuracy on the problems with the greater planning component. Diazepam 10 mg significantly slowed responding without reducing accuracy. The increased latency seen after 10 mg diazepam was only seen in those problems that were solved correctly first time.
Discussion
Diazepam had detrimental effects on performance of tests requiring planning and decision-making that depend on the dorsolateral prefrontal cortex (Baker et al. 1996; Manes et al. 2002) or activate the orbitofrontal cortex (Rogers et al. 1999b). Diazepam also produced disinhibitory effects on two tests of speeded responding (Go/No-Go and RVIP) as well as reducing sensitivity to discriminate target stimuli. Despite the sedative doses used, none of the effects were secondary to sedation.
Planning
Diazepam has previously been reported to impair performance on the Tower of London task, but the effects were not always immediately evident (Coull et al. 1995b; Gorrisen et al. 1998). Coull et al. (1999b) pointed out that Gorrisen et al. (1998) might not have used the most sensitive measures. We used a more sensitive version of the task and demonstrated that a high dose of diazepam impairs planning: subjects taking 20 mg needed more attempts before making the correct responses on the harder problems. Also, subjects taking 10 mg diazepam took longer than other subjects to make an accurate first response. We have thus detected a mild planning deficit, manifest as lengthened thinking times, in the 10 mg group and an impairment of accuracy in the 20 mg group.
Disinhibition
We found that diazepam reduced sensitivity (A’) and the threshold for a response (B’’) in two tasks measuring sustained attention and response inhibition (RVIP and Go/No-Go). The results of the Risk task may similarly show a lowering of sensitivity to information, and a more disinihibitory response strategy: a high (20 mg) dose of diazepam made the subjects more likely to make a choice associated with the largest possible win, but the lowest possibility of success. This disinhibitory effect of diazepam could also account for the apparently “paradoxical” clinical observation of aggression in diazepam-sedated individuals (Joint Formulary Committee 2003).
Coull et al. (1995c) found that diazepam reduced A’ but had no significant effect on B’’ although their data for B’’ show the same tendency as seen here. The difference may have been due to our use of a corrected measure for B’’ (Snodgrass and Corwin 1988) which increased the sensitivity of the analysis. Diazepam also slowed all responses on the ID/ED task as seen previously (Coull et al. 1995a). We found no significant effect of diazepam upon extradimensional set shifting, although a deficit has previously been described by Coull et al. (1995a) using a different version of the task.
Memory
Curran (1999) notes that benzodiazepines do not impair performance on priming tests of indirect memory, e.g. word stem completion, degraded picture identification, with the exception of lorazepam, but that they do impair direct tests of episodic memory. We found no significant effect of diazepam on either immediate or delayed pattern recognition memory. Whilst this test is not unambiguously episodic in nature, as it could conceivably be solved via some indirect memory strategy such as relative familiarity, it is known to be sensitive to temporal but not frontal lobe damage in humans (Owen et al. 1995b), the anticholinergic scopolamine (Robbins et al. 1997), tryptophan depletion (Rubinsztein et al. 2001) and Alzheimer’s disease (Sahakian et al. 1988). The lack of effect on attentional set shifting and memory suggests some selectivity in the actions of diazepam.
Possible neural mechanisms
Diazepam reduced information sensitivity (A’) and decreased inhibition (B’’) on the RVIP task, which is known to activate a network of frontal and parietal cortex (Coull et al. 1996). A decrease in A’, without changes in B’’, resulting from an increased presentation rate, is associated with an increase in regional cerebral blood flow (rCBF) in lateral occipital cortex and the fusiform gyrus (Coull et al. 1995a); Similar changes in A’ produced by the adrenoreceptor agonist clonidine, are accompanied by altered connectivity between frontal and parietal cortices; between parietal cortex and thalamus; and between locus coeruleus and visual cortex (Coull et al. 1999a). Thus effects on A’ may be due to changes in frontal, parietal or even occipital areas.
We propose that the inhibition of frontal areas by diazepam, particularly dorsolateral and orbitofrontal regions, may be sufficient to explain the results on the RVIP, Go\No-Go and Risk tasks: Stuss et al. (2002) found that patients with damage to the right dorsolateral prefrontal cortex exhibited reduced sensitivity on a shape discrimination reaction time task but a similar bias to controls, whereas patients with left dorsolateral prefrontal cortex damage were unimpaired on sensitivity but had a reduced threshold for making a response. Reductions in B’’ (increased “go” bias, which may relate to the notion of motoric impulsivity) also parallel effects reported by Iversen and Mishkin (1970) in macaques after symmetrical inferior convexity ablation. Similarly, a functional brain imaging study of the Risk task (Rogers et al. 1999b) revealed greater rCBF in the high-risk 5:1 ratio, compared to a less extreme ratio (4:2), in orbital frontal and middle frontal regions of the PFC.
The effects on planning may also be explained in these terms: the impairment produced by the 10 mg dose is similar to that resulting from lesions of the orbitofronal cortex; at the 20 mg dose the profile of subjects resembles that of patients with lesions of the dorsal prefrontal cortex (Manes et al. 2002). A speculative interpretation of such dose dependent effects is that the net effect of diazepam upon the different regions of the prefrontal cortex varies as a function of dose.
Diazepam could influence frontal lobe function in a variety of ways: through a direct effect on GABA receptors on the neurons of the frontal cortex; through a direct effect on GABA receptors on any of the neurons participating in the thalamo-striatal-pallidal loops or any other subcortical regions that have a functional connectivity with the frontal cortex (e.g. amygdala or hippocampus); or by altering the activity of the ascending reticular systems. There is evidence that diazepam alters firing in the ascending serotoninergic and noradrenergic systems and has some of its effects via release of dopamine (Feldman et al. 1996). Robbins (2000) noted that manipulations of dopamine and noradrenaline tended to produce effects on tasks predominantly engaging dorsolateral or rostrolateral PFC whilst manipulations of the serotoninergic system tend to alter performance in tests sensitive to orbitofrontal dysfunction. In terms of the profile of deficits seen here, it is not possible to say that diazepam exerts predominantly either a dopaminergic or a serotoninergic profile.
We conclude that diazepam’s effects on tasks reliant on frontal lobe function are more complex than modulation of only serotonin or the catecholamines. These effects could be produced by direct effects on GABAergic transmission within the PFC, or possible dose-related effects on neuromodulators such as dopamine or 5-HT.
Summary and conclusion
Diazepam had effects on tests of frontal lobe function including both tests of planning (OTToL) and decision making (Risk) that depend predominantly on dorsolateral and orbitofrontal regions of the PFC. In contrast to the well-known amnestic and sedative effects of diazepam we also demonstrated diazepam’s disinhibitory effects on two speeded reaction time tasks. Our results suggest that diazepam can impair performance on reaction time tasks in two ways both by impairing sensitivity and by reducing the threshold for a response. Diazepam thus produced a range of effects on tasks known to be differentially sensitive to PFC dysfunction.
References
Baker S, Rogers R, Owen A, Frith C, Dolan R, Frackowiak R, Robbins T (1996) Neural systems engaged by planning: a PET study of the Tower of London task. Neuropsychologia 34:515–526
Bechara A, Damasio A, Damasio H, Anderson S (1994) Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 50:7–15
Blair RJ, Curran H (1999) Selective impairment in the recognition of anger induced by diazepam. Psychopharmacology 147:335–338
Bond A, Lader M (1974) The use of analogue scales in rating subjective feelings. Br J Med Psychol 47:211–218
Coull JT, Middleton HC, Robbins TW, Sahakian BJ (1995a) Clonidine and diazepam have differential effects on tests of attention and learning. Psychopharmacology 120:322–332
Coull JT, Middleton HC, Robbins TW, Sahakian BJ (1995b) Contrasting effects of clonidine and diazepam on tests of working memory and planning. Psychopharmacology 120:311–321
Coull JT, Sahakian BJ, Middleton HC, Young AH, Park SB, McShane RH, Cowen PJ, Robbins TW (1995c) Differential effects of clonidine, haloperidol, diazepam and tryptophan depletion on focused attention and attentional search. Psychopharmacology 121:222–230
Coull JT, Frith CD, Frackowiak RS, Grasby PM (1996) A fronto-parietal network for rapid visual information processing: a PET study of sustained attention and working memory. Neuropsychologia 34:1085–1095
Coull JT, Buchel C, Friston KJ, Frith CD (1999a) Noradrenergically mediated plasticity in a human attentional neuronal network. Neuroimage 10:705–715
Coull JT, Frith CD, Dolan RJ (1999b) Dissociating neuromodulatory effects of diazepam on episodic memory encoding and executive function. Psychopharmacology 145:213–222
Curran H (1999) Psychopharmacological approaches to Human Memory. In: Gazzaniga M (ed) The cognitive neurosciences. MIT Press, Cambridge, Mass., pp 797–804
Dias R, Robbins TW, Roberts AC (1996) Dissociation in prefrontal cortex of affective and attentional shifts. Nature 380:69–72
Downes JJ, Roberts AC, Sahakian BJ, Evenden JL, Morris RG, Robbins TW (1989) Impaired extra-dimensional shift performance in medicated and unmedicated Parkinson’s disease: evidence for a specific attentional dysfunction. Neuropsychologia 27:1329–1343
Feldman R, Meyer J, Quenzer L (1996) Sedative-hypnotic and anxiolytic drugs neuropsychopharmacology. Sinauer Associates, Sunderland, Mass., pp 673–732
Gorrisen MEE, Curran HV, Eling PATM (1998) Proactive interference and temporal context encoding after diazepam intake. Psychopharmacology 138:334–343
Grier JB (1971) Nonparametric indexes for sensitivity and bias: computing formulas. Psychol Bull 75:424–429
Iversen SD, Mishkin M (1970) Perseverative interference in monkeys following selective lesions of the inferior prefrontal convexity. Exp Brain Res 11:376–386
Joint Formulary Committee (2003) British National Formulary. British Medical Association and Royal Pharmaceutical Society of Great Britain, London, and British Medical Association and Royal Pharmaceutical Society of Great Britain, London
Manes F, Sahakian B, Clark L, Rogers R, Aitken M, Robbins T (2002) Decision-making processes following damage to the prefrontal cortex. Brain 125:624–639
Milner B (1964) Effects of different brain lesions on card sorting. Arch Neurol 9:100–110
Nelson HE (1982) National adult reading test manual. NFER-Nelson, Windsor, Berks
Owen AM, Downes JJ, Sahakian BJ, Polkey CE, Robbins TW (1990) Planning and spatial working memory following frontal lobe lesions in man. Neuropsychologia 28:1021–1034
Owen AM, Sahakian BJ, Hodges JR, Summers BA, Polkey CE, Robbins TW (1995a) Dopamine-dependent frontostriatal planning deficits in early Parkinson’s disease. Neuropsychology 9:126–140
Owen AM, Sahakian BJ, Semple J, Polkey CE, Robbins TW (1995b) Visuo-spatial short-term recognition memory and learning after temporal lobe excisions, frontal lobe excisions or amygdalo-hippocampectomy in man. Neuropsychologia 33:1–24
Rahman S, Sahakian BJ, Hodges JR, Rogers RD, Robbins TW (1999) Specific cognitive deficits in mild frontal variant frontotemporal dementia. Brain 122:1469–1493
Rahman S, Sahakian B, Cardinal RN, Rogers R, Robbins T (2001) Decision making and neuropsychiatry. Trends Cognit Sci 5:271–277
Robbins TW (2000) Chemical neuromodulation of frontal-executive functions in humans and other animals. Exp Brain Res 133:130–138
Robbins TW, Semple J, Kumar R, Truman MI, Shorter J, Ferraro A, Fox B, McKay G, Matthews K (1997) Effects of scopolamine on delayed-matching-to-sample and paired associates tests of visual memory and learning in human subjects: comparison with diazepam and implications for dementia. Psychopharmacology 134:95–106
Rogers RD, Blackshaw AJ, Middleton HC, Matthews K, Hawtin K, Crowley C, Hopwood A, Wallace C, Deakin JF, Sahakian BJ, Robbins TW (1999a) Tryptophan depletion impairs stimulus-reward learning while methylphenidate disrupts attentional control in healthy young adults: implications for the monoaminergic basis of impulsive behaviour. Psychopharmacology 146:482–491
Rogers RD, Owen AM, Middleton HC, Williams EJ, Pickard JD, Sahakian BJ, Robbins TW (1999b) Choosing between small, likely rewards and large, unlikely rewards activates inferior and orbital prefrontal cortex. J Neurosci 19:9029–9038
Rubinsztein J, Michael A, Paykel E, Sahakian B (2000) Cognitive Impairment in remission in bipolar affective disorder. Psychol Med 30:1025–1036
Rubinsztein JS, Rogers RD, Riedel WJ, Mehta MA, Robbins TW, Sahakian BJ (2001) Acute dietary tryptophan depletion impairs maintenance of “affective set” and delayed visual recognition in healthy volunteers. Psychopharmacology 154:319–326
Sahakian BJ, Morris RG, Evenden JL, Heald A, Levy R, Philpot M, Robbins TW (1988) A comparative study of visuospatial memory and learning in Alzheimer-type dementia and Parkinson’s disease. Brain 111:695–718
Sahakian BJ, Jones G, Levy R, Gray R, Warburton D (1989) The effects of nicotine on attention, information processing and the short term memory of patients with dementia of the Alzheimer type. Br J Psychiatry 154:797–800
Snodgrass JG, Corwin J (1988) Pragmatics of measuring recognition memory: applications to dementia and amnesia. J Exp Psychol Gen 117:34–50
Stuss DT, Binns MA, Murphy KJ, Alexander MP (2002) Dissociations within the anterior attentional system: effects of task complexity and irrelevant information on reaction time speed and accuracy. Neuropsychology 16:500–513
Acknowledgements
Funding was provided by a Wellcome Trust Programme Grant (019407) to Professor T.W. Robbins, Professor B.J. Everitt, Dr. A.C. Roberts and Professor B.J. Sahakian. J.B.D. was funded by Merck Sharp and Dohme, a James Baird Award from the University of Cambridge School of Clinical Medicine and an Oon Khye Beng studentship. The research was conducted within the MRC Centre for Behavioural and Clinical Neuroscience.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Deakin, J.B., Aitken, M.R.F., Dowson, J.H. et al. Diazepam produces disinhibitory cognitive effects in male volunteers. Psychopharmacology 173, 88–97 (2004). https://doi.org/10.1007/s00213-003-1695-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-003-1695-4