
Abstract
Rationale
While it is generally believed that administration of the dopamine precursor levodopa (l-dopa) exacerbates symptoms of schizophrenia, numerous reports suggest that adjunctive l-dopa may be beneficial. This body of literature has not been critically reviewed.
Objectives
On the basis of published studies, to determine whether l-dopa administered concomitantly with antipsychotic drugs provides a beneficial response in patients with schizophrenia.
Methods
This review examined 30 studies involving 716 patients. Due to wide methodological variability and limited statistical information, only five studies encompassing 160 patients could be included in a meta-analysis. The others were evaluated qualitatively.
Results
When l-dopa was added to antipsychotic drugs, the overall improvement was moderate (d=0.71) and highly significant (P<0.0001). There were 16 other studies in which l-dopa was added to antipsychotic drugs, but which did not meet criteria for inclusion in the meta-analysis. In these, worsening occurred in less than 20% of patients; the percentage of improved patients varied widely but had a central tendency around 50%.
Conclusions
In patients already on antipsychotic drugs, the addition of l-dopa can be beneficial. Dopamine agonists merit further consideration as adjuncts to antipsychotic drugs in the treatment of schizophrenia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The classical dopamine (DA) hypothesis holds that certain symptoms of schizophrenia are mediated by increased limbic DA transmission (Mathysse 1972). It was generated by two early observations. The first, that all clinically effective antipsychotic drugs (APDs) block DA receptors, endures to this day (Seeman and Tallerico 1998; http://kidb.bioc.cwru.edu/pdsp.php). The second, that DA agonists exacerbate psychotic symptoms in patients with schizophrenia, has been less consistently supported. The effects of the DA precursor l-dihydroxyphenylalanine (l-dopa) provide a case in point. Published reports describe l-dopa administration to over 700 patients with schizophrenia (Table 1). Of these, a small number of studies are often cited as evidence that l-dopa unequivocally exacerbates psychosis in schizophrenia (Lehrman and Sharav 1997). Yet l-dopa had also been recommended as an adjunct to typical APDs in treatment resistant patients, particularly in those with negative symptoms (Andreasen 1985; Meltzer et al. 1986; Pidgeon and Wolf 1989; Meltzer 1992; Wolkowitz 1993). Several factors may account for this inconsistency. Many l-dopa studies were reported in the non-English literature and were conducted before the implementation of rigorous research designs. Significant methodological differences between studies precluded easy comparisons. Furthermore, the widespread availability of atypical APDs has reduced interest in adjunctive treatments, particularly in those from the typical APD era. However, even atypical APDs may only partially treat the cognitive impairments and negative symptoms of schizophrenia (Chakos et al. 2001); these have been linked to deficient cortical DA transmission (Berman and Weinberger 1990; Callicott et al. 2000; Perlstein et al. 2001) and may constitute limiting factors for outcome (Green et al. 2000; Gold et al. 2002; Hoffman et al. 2003). Indeed, if satisfactory clinical outcome is redefined to include psychosocial rehabilitation and integration, then a significant number of patients await improved therapies (Kapur and Remington 2001). Such considerations prompted this review of the chronic use of l-dopa in schizophrenia.
In a few early investigations, high doses of l-dopa administered to patients with schizophrenia, in some cases after abrupt discontinuation of APDs, were reported to exacerbate or induce psychosis (Yaryura-Tobias et al. 1970a, 1970b; Angrist et al. 1973). In contrast, more numerous reports indicated that l-dopa administered concurrently with APDs improved clinical outcome in schizophrenia (Table 2). Thus, the literature suggested that APD status was a critical variable in the response to l-dopa and hence that the following hypotheses should be tested: 1) In APD-free patients, l-dopa is more likely than placebo to be associated with clinical worsening, 2) in APD-treated patients, l-dopa is more likely than placebo to be associated with clinical improvement.
Materials and methods
We conducted a computer based literature search (PubMed online, National Library of Medicine, Bethesda, Md., USA) using the key-word combinations “l-dopa AND schizophrenia” and “l-dopa AND psychosis” from 1965 through July 1 2003. All identified articles were screened and relevant references within those sources were also obtained (Table 1). Native speakers translated foreign-language articles. The initial minimal inclusion criteria for reports were: a) included adult subjects with schizophrenia, b) described or measured psychiatric response, c) treated subjects for at least 5 days with l-dopa, d) reported in a peer-reviewed journal. Upon further examination, we excluded all single-case reports (Garfinkel and Stancer 1976; Kay and Opler 1985), a report in which patients received l-dopa concomitantly with a monoamine oxidase inhibitor (Turner and Merlis 1964), as well as reports (Inanaga and Tanaka 1973; Gutierrez et al. 1979) in which the same subjects had been described in earlier publications (Inanaga et al. 1972; Beramendi et al. 1978). We also excluded one study of l-dopa effects on tardive dyskinesia because information on psychopathology in 60 patients was limited to the comment “No exacerbation of the psychosis was observed” (Ludatscher 1989). In contrast, we included other studies in which authors were primarily interested in l-dopa effects on tardive dyskinesia or extrapyramidal symptoms but also assessed psychiatric symptoms (Yaryura-Tobias et al. 1970b; Kawamura 1971; Sarai et al. 1973; Chouinard et al. 1987). In the one case where three independent studies were described in a single report (Asano et al. 1973), we considered the studies independently and have referred to them as a, b and c in the tables.
In total, 27 reports describing a total of 654 patients were included. Of the former, eight were in Japanese, one in Spanish and the remainder in English. The following information was extracted from each article: i) demographic data, ii) diagnostic criteria/selection methods, iii) l-dopa dose, duration of treatment, iv) concurrent medications, v) study design, vi) method for determination of psychiatric changes, vii) basis for conclusions (e.g. statistical analysis versus clinical impression). The approximate equivalence between the centrally active dose of l-dopa with and without a dopa-decarboxylase inhibitor was accepted as 4:1 (Cedarbaum 1987).
There was considerable methodological variability between the studies (Table 2). Although most used formal rating scales of psychopathology, some of the scales were symptom based (e.g. Brief Psychiatric Rating Scale), while others consisted of a single global score. Several reports provided only the direction of change in an overall score but neither its magnitude nor changes in individual factors. In view of such heterogeneity, we adhered as closely as possible to the approach used in each report for the assignment of outcome. For instance, when the BPRS was used but the actual BPRS scores not provided, we accepted the conclusions of the investigators as to the fraction of patients who improved and those who showed worsening (e.g. Angrist et al. 1973). When individual patient scores were provided, we adopted the investigators’ definition of significant response (e.g. 12-point change in BPRS) (Davidson et al. 1987).
Placebo-controlled studies in which treatment with APD+l-dopa could be compared to treatment with APD alone were subjected to meta-analysis (DSTAT). For the purposes of the meta-analysis, patients were assigned to one of two response groups; Poor response=no change or worsening, Good response=improved. More specifically, within the l-dopa+APD and the APD only groups in each study, each subject with a Poor response was assigned a value of “0” and a “1” was assigned to each subject with a Good response. Within-group variance and pooled variance were calculated using standard formulae. The effect size (PLdopa+APD−PAPD)/SDpooled ) for each study was converted to r, which was tested for significance using a one-tail t-test with the dfs associated with the correlation (N1+N2–2). These P-values are presented in Table 3, along with the corresponding effect sizes (d) and probability. The outcomes across the five studies were combined by averaging the d-values (effect sizes) (Rosenthal and Rosnow 1991), with each d weighted by the reciprocal of its variance. This procedure gives greatest weight to the most reliably estimated study outcomes, those with the largest sample sizes (Hedges and Olkin 1985).
Other reports were evaluated qualitatively. For studies in which l-dopa was openly added to patients already on APD, we constructed a table and plotted the number of subjects against the percentage who definitely improved or showed definite worsening in each study. For studies in which l-dopa was administered without concomitant APDs, all the patients were pooled and the overall percentage of patients who had definite clinical worsening was determined.
Results
The 27 studies involving 654 patients (Table 2) showed considerable heterogeneity of design, patient age (15–75 years), daily l-dopa dose (150–7000 mg), and duration of treatment (5 days to 18 months). Approximately 40% of all patients (n=261) were enrolled in double blind studies with a placebo control. For the majority of patients (n=530), diagnosis was based on clinical impression but outcome was determined on some formal scale (n=527).
There was no placebo-controlled study in which l-dopa was administered to APD-free patients. Similarly, there was no study in which l-dopa in combination with APDs was compared to l-dopa administration alone. In contrast, there were five placebo-controlled studies in which l-dopa was added to APD-treated patients (n=160) (Fleming et al. 1970; Asano et al. 1973; Buchanan 1975; Gerlach and Luhdorf 1975; Inanaga et al. 1975a), and which could be subjected to meta-analysis. While the effect sizes (Cohen’s d) for the l-dopa response (Table 3) were very heterogeneous, ranging from 0.27 (Inanaga et al. 1975a) to 3.6 (Asano et al. 1973), all were in the same direction. The overall composite effect size was 0.71 (between medium and large) and highly significant (P<0.00001). With only five studies, it was not possible to determine the source of heterogeneity. [Note: in the study with the greatest effect size (Asano et al. 1973), patients had been selected on the basis of a previous good response to open administration of l-dopa. If that study is excluded, the overall effect size becomes 0.59, still in the medium to large range, and remains highly significant, P<0.0003].
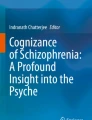
There were 16 non-placebo controlled studies in which l-dopa was added to patients already on APDs (Table 4). A plot of the percentage of those who improved against sample size showed that studies with a small sample size had a wide range of improvement with a central tendency around 50% (Fig. 1). A plot of sample size against the percentage of those who showed worsening demonstrates that in 13 studies, less than 20% of the patients showed worsening (Fig. 2); all three studies in which over 20% of patients worsened (Yaryura-Tobias et al. 1970a, 1970b; Calil et al. 1977) had very small patient samples (n≤4). A total of 64 patients in five studies received l-dopa without concomitant APDs; 38% of the latter showed definite worsening (Angrist et al. 1973; Alpert et al. 1978; Brambilla et al. 1979; Beramendi et al. 1980, Davidson et al. 1987).

Plot of number of patients per study against the percentage of patients on typical APDs who improved during l-dopa treatment

Plot of number of patients per study against the percentage of patients on typical APDs who showed worsening during l-dopa treatment
Discussion
We could not determine whether chronic l-dopa administration was more likely than placebo to cause worsening in APD-free patients. On the other hand, a meta-analysis showed that administration of l-dopa to patients concomitantly treated with APDs was associated with significant improvement. These statements must be understood within methodological limitations.
First, only a fraction of published studies (n=5/30, patient n=160/716) met criteria for inclusion in our meta-analysis. There was no placebo-controlled study in which chronic l-dopa was administered to APD-free patients with schizophrenia. While 38% of the pool of all APD-free patients treated with l-dopa had definite clinical worsening, the latter is mitigated by several considerations. All those patients received high doses (>1000 mg/day) of l-dopa, often after abrupt cessation of APDs (Angrist et al. 1973; Alpert et al. 1978; Brambilla et al. 1979; Beramendi et al. 1980, Davidson et al. 1987). Schizophrenia and particularly untreated schizophrenia are per se associated with an increased risk of exacerbation. Over a 10-month period, the general estimated prevalence of exacerbation in schizophrenia is 16% in APD-treated individuals but 56% in patients who are not taking APDs (Gilbert et al. 1995). The majority (84%) of patients in the current review who received l-dopa without concomitant APDs did so for less than 4 weeks (Angrist et al. 1973; Alpert et al. 1978; Brambilla et al. 1979; Beramendi et al. 1980; Davidson et al. 1987). Furthermore, insofar as l-dopa increases verbal communicativeness (Yaryura-Tobias et al. 1971), rating scales that depend on self-reporting of symptoms may overestimate the emergence of psychotic symptoms in the previously withdrawn patient. Thus the true risk of psychotic exacerbation associated with l-dopa administration to APD-free patients cannot be reliably determined. Our data do not refute, however, the possibility that APD-free patients with schizophrenia may be more vulnerable to l-dopa induced exacerbation than other psychiatric groups. In non-psychotic psychiatric conditions (e.g. major depression), the appearance of psychotic symptoms during l-dopa treatment tends towards the lower range of 0–15% of patients (Sathanathan et al. 1973; Dunner and Fieve 1975; Mendels et al. 1975; Shingu et al. 1979; Oren et al. 1994), but may be higher in patients with a psychotic affective illness (Bunney et al. 1971)
Our main goal was to determine whether adding l-dopa to APDs is beneficial; the overall l-dopa effect (0.71) suggests that it is moderately so. Unfortunately, the impact of l-dopa on individual symptoms and particularly on positive and negative symptoms could not be determined. While two (Inanaga et al. 1972, 1975a) of four studies which selected for patients with negative symptoms (Kawamura et al. 1971; Inanaga et al. 1972, 1975a; Nishikawa et al. 1972; Kai et al. 1976) considered the latter to be particularly responsive to l-dopa, the majority of studies did not specifically measure such symptoms. Furthermore, since APD-induced extrapyramidal effects can mimic negative symptoms, l-dopa’s anti-parkinsonian effects would need to be taken into account. Similarly, we could not analyze factors such as l-dopa dose, duration of treatment or duration of illness. One group posited that a beneficial l-dopa response was confined to patients within 5 years of illness onset (Inanaga et al. 1975b), but this could not be tested overall. It is particularly unfortunate that neuropsychological assessments were not done. l-dopa affects cognition in other neuropsychiatric conditions and cortical DA has been implicated in the cognitive deficits of schizophrenia (Berman and Weinberger 1990; Perlstein et al. 2001).
l-Dopa effects on the brain have been extensively studied. In vivo imaging confirms that exogenous l-dopa is converted to synaptic DA in normal primates (Tedroff et al. 1992) and in patients with Parkinson’s disease (Tedroff et al. 1996). In unmedicated patients with schizophrenia, the striatal DA system displays an increased rate of conversion of radiolabeled l-dopa to DA (Reith et al. 1994; Lindstrom et al. 1999), as well as higher concentrations of both baseline (Abi-Dargham et al. 2000) and amphetamine-releasable DA (Breier et al. 1997; Laruelle and Abi-Dargham 1999); the latter have been linked to positive symptoms of schizophrenia (Breier et al. 1997; Laruelle and Abi-Dargham 1999). Thus, any increased risk of psychotic relapse or exacerbation during chronic l-dopa administration in APD-free patients is probably due to l-dopa-induced potentiation of DA release in the limbic striatum.
Endogenous DA competes with DA receptor antagonists for binding to DA receptors. Manipulations that increase or decrease endogenous DA levels, respectively, lower or increase DA antagonist binding to striatal DA receptors in schizophrenia (Breier et al. 1997; Laruelle and Abi-Dargham 1999; Abi-Dargham et al. 2000). Thus the incremental DA released due to l-dopa administration would displace APD from D1, D2, D3 and/or D4 receptors, depending on the APD profile (http://kidb.bioc.cwru.edu/pdsp.php). If, however, therapeutic actions depend on APD occupancy of DA receptors, how could l-dopa-induced elevation of DA levels lead to improvement rather than to psychotic exacerbation? There are several possibilities.
One recent hypothesis suggests that prolonged DA receptor occupancy is not necessary for APD action (Kapur and Seeman 2001). Indeed, enhanced APD effects may derive from rapid occupancy but quick dissociation of the APD from D2 receptors. This dissociation occurs more quickly at high DA concentrations (Seeman and Tallerico 1999) and hence could be promoted by optimally elevating synaptic DA levels. Atypical APDs with weak D2 antagonist properties such as clozapine and quetiapine (Seeman and Tallerico 1998) are of particular interest; both drugs can reduce l-dopa induced psychosis in Parkinson’s disease (Meltzer et al. 1995; Trosch et al. 1998; Fernandez et al. 1999) yet are readily displaced from D2 receptors by endogenous DA (Seeman and Tallerico 1999). The latter raises the possibility that adjunctive l-dopa might be especially useful in patients with schizophrenia who are partial responders to clozapine or quetiapine.
A different mechanism by which elevated DA levels could prove beneficial involves the distinction between tonic and phasic DA release. It has been posited that in schizophrenia abnormally low levels of tonically released striatal DA lead to compensatory upregulation of enzymes of DA synthesis and of postsynaptic DA receptors; the exaggerated effects of phasically released DA are then expressed as positive symptoms (Grace 1991, 1993). Accordingly, maneuvers which increase tonic levels of synaptic DA should blunt the quantity and effects of phasically released DA (Grace 1991, 1993). l-Dopa administration would be expected to increase tonic DA levels; if in addition it did not reverse APD-induced depolarization blockade then co-administration of APD and l-dopa would meet the proposed requirements for enhanced antipsychotic efficacy (Grace 1993).
By definition, DA is a full agonist at all DA receptors. In contrast, partial DA agonists can act as agonists at presynaptic DA receptors and as antagonists at postsynaptic DA receptors; they can reduce net limbic DA transmission but with a lower relative tendency to increase the sensitivity of the postsynaptic DA receptors (for review, see Tamminga and Carlsson 2002). Indeed, such a mechanism may contribute to the therapeutic properties of the recently introduced APD aripiprazole (Burris et al. 2002; Yokoi et al. 2002). Partial agonism can be produced in vitro by combining a full direct agonist with a full antagonist (Ebert et al. 1994). Could partial agonism be achieved in vivo by combining the indirect DA agonist l-dopa with a full DA antagonist? It would require that l-dopa induced changes in DA levels i) enhance stimulation of presynaptic autoreceptors so as to attenuate limbic striatal DA release and/or synthesis, yet ii) be insufficient to markedly displace APD binding to postsynaptic DA receptors. Stimulation of the presynaptic autoreceptor can indeed attenuate the conversion of l-dopa to DA in vivo (Cumming et al. 1995, 1997). Whether the latter could more than offset the increase in DA synthesis attributable to higher l-dopa levels is not known.
Both APDs and l-dopa also affect DA transmission in cortical regions. In the rat, exogenous l-dopa produces a relatively larger and longer lasting increase in DA levels in the prefrontal cortex than in the striatum (Loeffler et al. 1997); the resulting prefrontal cortex DA levels correlate highly with serum l-dopa levels (Carey et al. 1995). Interestingly, schizophrenia is associated with an increased conversion of administered l-dopa to DA in the prefrontal cortex (Lindstrom et al. 1999). The latter may be compensation for reduced prefrontal cortex DA innervation (Akil et al. 1999) or an attempt at feedback inhibition (Kolachana et al. 1995) of excessive limbic DA release (Breier et al. 1997; Laruelle and Abi-Dargham 1999). In clinical research, the prefrontal cortex, and particularly the D1 receptors in the prefrontal cortex, have been implicated in working memory deficits, conceptual disorganization (Berman and Weinberger 1990; Perlstein et al. 2001; Abi-Dargham et al. 2002) as well as in the so-called negative symptoms of schizophrenia (Callicott et al. 2000). Given the relative preponderance of D1 relative to D2 receptors in cortical regions (Hall et al. 1994), augmentation of prefrontal cortex DA release during APD blockade of D2 receptors would preferentially increase stimulation of cortical D1 receptors. Since the DA neurons innervating the prefrontal cortex are resistant to APD-induced depolarization blockade (Chiodo and Bunney 1983; White and Wang 1983; Chen et al. 1992), l-dopa could produce a regionally selective sustained increase in DA levels. Indeed, the co-administration of l-dopa and APDs to patients with schizophrenia could have two functionally linked but regionally distinct beneficial effects. Direct augmentation of deficient limbic cortical DA transmission could improve cognitive deficits and negative symptoms. Furthermore, augmented PFC DA tone would reduce and hence normalize exaggerated effects of phasically released limbic striatal DA, thus attenuating positive symptoms (Grace 1991, 1993). There are other possibilities as well.
Several observations point to the existence of l-dopa specific receptors and suggest that l-dopa may act as a neuromodulator of DA and other systems (Opacka-Juffry and Brooks 1995; Misu et al. 1996). Indeed, l-dopa modulation of striatal DA neurotransmission has been demonstrated in primates in vivo (Tedroff 1997). Exogenous l-dopa can also increase brain noradrenaline synthesis under basal (Kato et al. 1987) as well as drug-stimulated conditions (Dolphin et al. 1976; Nguyen and Angers 1987; Buu 1989). Noradrenaline in turn, has been implicated in the pathophysiology of schizophrenia and in the therapeutic response to antipsychotic drugs (van Kammen and Kelley 1991; Friedman et al. 1999). Such mechanisms might also be involved in l-dopa effects on schizophrenia.
What are the clinical and research implications of our analysis? We conclude that high dose l-dopa should not be administered to APD-free patients with schizophrenia in the absence of a highly compelling reason, and then only with careful clinical and Institutional Review Board supervision. While we could not quantify the risk of exacerbation associated with l-dopa administration to APD-free patients, some risk is likely. At the very least, there is no evidence that administering l-dopa to APD-free patients is therapeutic. The possible role of l-dopa as an adjunct for patients with an inadequate APD response remains to be defined. Three challenges must be met. First, there is the perception that l-dopa administration to patients with schizophrenia is inherently unethical (e.g. Lehrman and Sharav 1997). The latter contention, in its most strident form, is not supported by the scientific data. Second, if the effect of l-dopa could not be adequately defined in studies involving over 700 patients, what justification is there for additional investigations? In this regard, we note that most available studies do not meet modern standards; the abundance of data cannot compensate for this. Third, one could argue that the availability of novel APDs has rendered adjunctive treatments obsolete. Unfortunately, significant symptoms as well as cognitive and psychosocial deficits persist in many patients treated with atypical APDs (Chakos et al. 2001). The latter may be a paradoxical consequence of the success of atypical APDs, insofar as their use has prompted a reappraisal of what constitutes a satisfactory treatment outcome (Kapur and Remington 2001). In this context, consideration of novel therapies, including adjunctive treatments is well justified. The results of our meta-analysis are consistent with studies of other DA agonists (Benkert et al. 1995). We are not recommending that clinicians routinely combine l-dopa with typical or atypical APDs for patients with schizophrenia who are poor or partial treatment responders. Nonetheless, further evaluation of l-dopa and other DA agonists as adjunctive treatments for schizophrenia is certainly warranted.
References
Abi-Dargham A, Rodenhiser J, Printz D, Zea-Ponce Y, Gil R, Kegeles LS, Weiss R, Cooper TB, Mann JJ, Van Heertum RL, Gorman JM, Laruelle M (2000) Increased baseline occupancy of D2 receptors by dopamine in schizophrenia. Proc Natl Acad Sci USA 97:8104–8109
Abi-Dargham A, Mawlawi O, Lombardo I, Gil R, Martinez D, Huang Y, Hwang DR, Keilp J, Kochan L, Van Heertum R, Gorman JM, Laruelle M (2002) Prefrontal dopamine D1 receptors and working memory in schizophrenia. J Neurosci 22:3708–3719
Akil M, Pierri JN, Whitehead RE, Edgar CL, Mohila C, Sampson AR, Lewis DA (1999) Lamina-specific alterations in the dopamine innervation of the prefrontal cortex in schizophrenic subjects. Am J Psychiatry 156:1580–1589
Alpert M, Friedhoff AJ, Marcos LR, Diamond F (1978) Paradoxical reaction to l-dopa in schizophrenic patients. Am J Psychiatry 135:1329–1332
Andreasen NC (1985) Negative syndrome in schizophrenia: strategies for long-term management. Adv Biochem Psychopharmacol 40:1–7
Angrist B, Sathananthan G, Gershon S (1973) Behavioral effects of l-dopa in schizophrenic patients. Psychopharmacologia 31:1–12
Asano T, Noma T, Matsuda K, Ikeda H, Otsuki S (1973) Effect of l-dopa on the hypochondriac complaints of the chronic psychotics. Seishin Igaku (in Japanese) 15:745–751
Benkert O, Muller-Siecheneder F, Wetzel H (1995) Dopamine agonists in schizophrenia: a review. Eur Neuropsychopharmacol 5:43–53
Beramendi V, Alpert M, Guimon J, Friedhoff A, Gutierrez M (1980) [Controlled study of l-dopa in schizophrenia with reference to the theory of hypersensitivity of dopamine receptors]. Arch Neurobiol (Madr) 43:107–124
Berman KF, Weinberger DR (1990) The prefrontal cortex in schizophrenia and other neuropsychiatric diseases: in vivo physiological correlates of cognitive deficits. Prog Brain Res 85:521–536
Brambilla F, Scarone S, Ponzano M, Maffei C, Nobile P, Rovere C, Guastalla A (1979) Catecholaminergic drugs in chronic schizophrenia. Neuropsychobiology 5:185–200
Breier A, Su TP, Saunders R, Carson RE, Kolachana BS, de BA, Weinberger DR, Weisenfeld N, Malhotra AK, Eckelman WC, Pickar D (1997) Schizophrenia is associated with elevated amphetamine-induced synaptic dopamine concentrations: evidence from a novel positron emission tomography method. Proc Natl Acad Sci USA 94:2569–2574
Buchanan FH, Parton RV, Warren JW, Baker EP (1975) Double blind trial of l-dopa in chronic schizophrenia. Aust N Z J Psychiatry 9:269–271
Bunney WEJ, Brodie HK, Murphy DL, Goodwin FK (1971) Studies of alpha-methyl-para-tyrosine, l-dopa, and l-tryptophan in depression and mania. Am J Psychiatry 127:872–881
Burris KD, Molski TF, Xu C, Ryan E, Tottori K, Kikuchi T, Yocca FD, Molinoff PB (2002) Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther 302:381–389
Buu NT (1989) Vesicular accumulation of dopamine following l-dopa administration. Biochem Pharmacol 38:1787–1792
Calil HM, Yesavage JA, Hollister LE (1977) Low dose levodopa in schizophrenia. Commun Psychopharmacol 1:593–596
Callicott JH, Bertolino A, Egan MF, Mattay VS, Langheim FJ, Weinberger DR (2000) Selective relationship between prefrontal N-acetylaspartate measures and negative symptoms in schizophrenia. Am J Psychiatry 157:1646–1651
Carey RJ, Pinheiro-Carrera M, Dai H, Tomaz C, Huston JP (1995) l-Dopa and psychosis: evidence for l-dopa-induced increases in prefrontal cortex dopamine and in serum corticosterone. Biol Psychiatry 38:669–676
Cedarbaum JM (1987) Clinical pharmacokinetics of anti-parkinsonian drugs. Clin Pharmacokinet 13:141–178
Chakos M, Lieberman J, Hoffman E, Bradford D, Sheitman B (2001) Effectiveness of second-generation antipsychotics in patients with treatment-resistant schizophrenia: a review and meta-analysis of randomized trials. Am J Psychiatry 158:518–526
Chen JP, Ruan D, Paredes W, Gardner EL (1992) Effects of acute and chronic clozapine on dopaminergic function in medial prefrontal cortex of awake, freely moving rats. Brain Res 571:235–241
Chiodo LA, Bunney BS (1983) Typical and atypical neuroleptics: differential effects of chronic administration on the activity of A9 and A10 midbrain dopaminergic neurons. J Neurosci 3:1607–1619
Chouinard G, Jones BD (1980) Neuroleptic-induced supersensitivity psychosis: clinical and pharmacologic characteristics. Am J Psychiatry 137:16–21
Chouinard G, Annable L, Mercier P, Turnier L (1987) Long-term effects of l-dopa and procyclidine on neuroleptic-induced extrapyramidal and schizophrenic symptoms. Psychopharmacol Bull 23:221–226
Cumming P, Kuwabara H, Ase A, Gjedde A (1995) Regulation of DOPA decarboxylase activity in brain of living rat. J Neurochem 65:1381–1390
Cumming P, Ase A, Laliberte C, Kuwabara H, Gjedde A (1997) In vivo regulation of DOPA decarboxylase by dopamine receptors in rat brain. J Cereb Blood Flow Metab 17:1254–1260
Davidson M, Keefe RS, Mohs RC, Siever LJ, Losonczy MF, Horvath TB, Davis KL (1987) l-Dopa challenge and relapse in schizophrenia. Am J Psychiatry 144:934–938
Dolphin A, Jenner P, Marsden CD (1976) Noradrenaline synthesis from l-dopa in rodents and its relationship to motor activity. Pharmacol Biochem Behav 5:431–439
Dunner DL, Fieve RR (1975) Affective disorder: studies with amine precursors. Am J Psychiatry 132:180–183
Ebert B, Madsen U, Lund TM, Lenz SM, Krogsgaard-Larsen P (1994) Molecular pharmacology of the AMPA agonist, (S)-2-amino-3-(3-hydroxy-5-phenyl-4-isoxazolyl)propionic acid [(S)-APPA] and the AMPA antagonist, (R)-APPA. Neurochem Int 24:507–515
Fernandez HH, Friedman JH, Jacques C, Rosenfeld M (1999) Quetiapine for the treatment of drug-induced psychosis in Parkinson’s disease. Move Disord 14:484–487
Fleming P, Makar H, Hunter KR (1970) Levodopa in drug-induced extrapyramidal disorders. Lancet 2:1186
Friedman JI, Adler DN, Davis KL (1999) The role of norepinephrine in the pathophysiology of cognitive disorders: potential applications to the treatment of cognitive dysfunction in schizophrenia and Alzheimer’s disease. Biol Psychiatry 46:1243–1252
Garfinkel PE, Stancer HC (1976) l-Dopa and schizophrenia. Can Psychiatr Assoc J 21:27–29
Gerlach J, Luhdorf K (1975) The effect of l-dopa on young patients with simple schizophrenia, treated with neuroleptic drugs: a double-blind cross-over trial with Madopar and placebo. Psychopharmacologia 44:105–110
Gilbert PL, Harris MJ, McAdams LA, Jeste DV (1995) Neuroleptic withdrawal in schizophrenic patients. A review of the literature. Arch Gen Psychiatry 52:173–188
Gold JM, Goldberg RW, McNary SW, Dixon LB, Lehman AF (2002) Cognitive correlates of job tenure among patients with severe mental illness. Am J Psychiatry 159:1395–1402
Grace AA (1991) Phasic versus tonic dopamine release and the modulation of dopamine system responsivity: a hypothesis for the etiology of schizophrenia. Neuroscience 41:1–24
Grace AA (1993) Cortical regulation of subcortical dopamine systems and its possible relevance to schizophrenia. J Neural Transm Gen Sect 91:111–134
Green MF, Kern RS, Braff DL, Mintz J (2000) Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull 26:119–136
Gutierrez M, Alpert M, Guimon J, Friedhoff AJ, Veramendi V (1979) [Controlled study on the possibilities of l-dopa in the residual extrapyramidal syndrome caused by neuroleptics]. Actas Luso Esp Neurol Psiquiatr Cienc Afines 7:181–188
Hall H, Sedvall G, Magnusson O, Kopp J, Halldin C, Farde L (1994) Distribution of D1- and D2-dopamine receptors, and dopamine and its metabolites in the human brain. Neuropsychopharmacology 11:245–256
Hedges LV, Olkin I (1985) Statistical methods for meta-analysis. Academic Press, Orlando, Fla.
Hoffmann H, Kupper Z, Zbinden M, Hirsbrunner HP (2003) Predicting vocational functioning and outcome in schizophrenia outpatients attending a vocational rehabilitation program. Soc Psychiatry Psychiatr Epidemiol 38:76–82
Inanaga K, Tanaka M (1973) Effects of l-dopa on schizophrenia. In: Ban TA (ed) Psychopharmacology, sexual disorders and drug abuse. North Holland Publishing Co., Amsterdam, pp 229–233
Inanaga K, Oshima M, Tachibana H, Nakamura K, Koketsu K (1971) Three cases of schizophrenia treated with l-dopa. Kurume Med J 18:161–168
Inanaga K, Inoue K, Tachibana H, Oshima M, Kotorii T (1972) Effect of l-dopa in schizophrenia. Folia Psychiatr Neurol Jpn 26:145–157
Inanaga K, Nakazawa Y, Inoue K, Tachibana H, Oshima M (1975a) Double-blind controlled study of l-dopa therapy in schizophrenia. Folia Psychiatr Neurol Jpn 29:123–143
Inanaga K, Ohshima M, Nagata T, Yamauchi I (1975b) Behavioral effects of l-dopa and thyrotropin-releasing hormone in schizophrenic patients: a preliminary report. Folia Psychiatr Neurol Jpn 29:197–205
Kai Y (1976) The effect of l-dopa and vitamin B6 in schizophrenia. Folia Psychiatr Neurol Jpn 30:19–26
Kapur S, Remington G (2001) Dopamine D(2) receptors and their role in atypical antipsychotic action: still necessary and may even be sufficient. Biol Psychiatry 50:873–883
Kapur S, Seeman P (2001) Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics?: a new hypothesis. Am J Psychiatry 158:360–369
Kato T, Karai N, Katsuyama M, Nakamura M, Katsube J (1987) Studies on the activity of l-threo-3,4-dihydroxyphenylserine (L-DOPS) as a catecholamine precursor in the brain. Comparison with that of l-dopa. Biochem Pharmacol 36:3051–3057
Kawamura T, Asada N, Kimura N, Tsukue I (1971) Psychiatric clinical findings of l-dopa effect, especially for psychic symptom and drug-induced parkinsonian symptoms in schizophrenia. Shinryo Shinyaku (in Japanese) 24:826–851
Kay SR, Opler LA (1985) l-Dopa in the treatment of negative schizophrenic symptoms: a single-subject experimental study. Int J Psychiatr Med 15:293–298
Kolachana BS, Saunders RC, Weinberger DR (1995) Augmentation of prefrontal cortical monoaminergic activity inhibits dopamine release in the caudate nucleus: an in vivo neurochemical assessment in the rhesus monkey. Neuroscience 69:859–868
Laruelle M, Abi-Dargham A (1999) Dopamine as the wind of the psychotic fire: new evidence from brain imaging studies. J Psychopharmacol 13:358–371
Lehrman NS, Sharav VH (1997) Ethical problems in psychiatric research. J Ment Health Admin 24:227–250
Lindstrom LH, Gefvert O, Hagberg G, Lundberg T, Bergstrom M, Hartvig P, Langstrom B (1999) Increased dopamine synthesis rate in medial prefrontal cortex and striatum in schizophrenia indicated by l-(beta-11C) DOPA and PET. Biol Psychiatry 46:681–688
Loeffler DA, LeWitt PA, Juneau PL, Camp DM, Arnold LA, Hyland K (1998) Time-dependent effects of levodopa on regional brain dopamine metabolism and lipid peroxidation. Brain Res Bull 47:663–667
Ludatscher JI (1989) Stable remission of tardive dyskinesia by l-dopa. J Clin Psychopharmacol 9:39–41
Matthysse S, Smith EL, Puck TT, Edelman GM (1972) Prospects for research on schizophrenia. VI. Biochemical hypotheses and new techniques. Neurosci Res Program Bull 10:446–455
Meltzer HY (1992) Treatment of the neuroleptic-nonresponsive schizophrenic patient. Schizophr Bull 18:515–542
Meltzer HY, Sommers AA, Luchins DJ (1986) The effect of neuroleptics and other psychotropic drugs on negative symptoms in schizophrenia. J Clin Psychopharmacol 6:329–338
Meltzer HY, Kennedy J, Dai J, Parsa M, Riley D (1995) Plasma clozapine levels and the treatment of l-dopa-induced psychosis in Parkinson’s disease. A high potency effect of clozapine. Neuropsychopharmacology 12:39–45
Mendels J, Stinnett JL, Burns D, Frazer A (1975) Amine precursors and depression. Arch Gen Psychiatry 32:22–30
Misu Y, Goshima Y, Ueda H, Okamura H (1996) Neurobiology of l-dopaergic systems. Prog Neurobiol 49:415–454
Nguyen TB, Angers M (1987) Effects of different monoamine oxidase inhibitors on the metabolism of l-dopa in the rat brain. Biochem Pharmacol 36:1731–1735
Nishikawa K, Higashayama I, Kasahara T (1972) l-Dopa treatment of chronic schizophrenia. Shinryo Shinyaku (in Japanese) 9:1439–1450
Ogura C, Kishimoto A, Nakao T (1976) Clinical effect of l-dopa on schizophrenia. Curr Ther Res Clin Exp 20:308–318
Opacka-Juffry J, Brooks DJ (1995) L-Dihydroxyphenylalanine and its decarboxylase: new ideas on their neuroregulatory roles. Mov Disord 10:241–249
Oren DA, Moul DE, Schwartz PJ, Wehr TA, Rosenthal NE (1994) A controlled trial of levodopa plus carbidopa in the treatment of winter seasonal affective disorder: a test of the dopamine hypothesis. J Clin Psychopharmacol 14:196–200
Otsuka T, Kumashioro E, Mizushima S, Maruko K, Koizumi S, Unno Y (1974) Effect of l-dopa on schizophrenia. Rinsho Seishin Igaku (in Japanese) 3:629–637
Perlstein WM, Carter CS, Noll DC, Cohen JD (2001) Relation of prefrontal cortex dysfunction to working memory and symptoms in schizophrenia. Am J Psychiatry 158:1105–1113
Pidgeon JF, Wolf MA (1989) [Dopaminergic agonists and schizophrenia] Agonistes dopaminergiques et schizophrenie. Psychiatr J Univ Ott 14:529–535
Reith J, Benkelfat C, Sherwin A, Yasuhara Y, Kuwabara H, Andermann F, Bachneff S, Cumming P, Diksic M, Dyve SE (1994) Elevated dopa decarboxylase activity in living brain of patients with psychosis. Proc Natl Acad Sci USA 91:11651–11654
Rosenthal B, Rosnow R (1991) Essentials of behavioral research: methods and data and analysis, 2nd edn. McGraw-Hill, New York
Sarai K, Kumura N, Ishii T, Iseki K, Imada HK, Kawamura T, Kino M, Echigo T (1973) Possibility of amine precursor therapy on schizophrenics by experimental study with l-dopa. Seishin Igaku (in Japanese) 15:189–196
Sathananthan G, Angrist BM, Gershon S (1973) Response threshold to levodopa in psychiatric patients. Biol Psychiatry 7:139–146
Seeman P, Tallerico T (1998) Antipsychotic drugs which elicit little or no parkinsonism bind more loosely than dopamine to brain D2 receptors, yet occupy high levels of these receptors. Mol Psychiatry 3:123–134
Shingu K, Kawai I, Yamada K (1979) Three cases of unipolar delusional depression responsive to l-dopa. Folia Psychiatr Neurol Jpn 33:511–515
Tamminga CA, Carlsson A (2002) Partial dopamine agonists and dopaminergic stabilizers in the treatment of psychosis. Curr Drug Target CNS Neurol Disord 1:141–147
Tedroff JM (1997) The neuroregulatory properties of l-dopa. A review of the evidence and potential role in the treatment of Parkinson’s disease. Rev Neurosci 8:195–204
Tedroff J, Aquilonius SM, Hartvig P, Lundqvist H, Bjurling P, Langstrom B (1992) Estimation of regional cerebral utilization of [11C]-l-3,4-dihydroxy-phenylalanine (DOPA) in the primate by positron emission tomography. Acta Neurol Scand 85:166–173
Tedroff J, Pedersen M, Aquilonius SM, Hartvig P, Jacobsson G, Langstrom B (1996) Levodopa-induced changes in synaptic dopamine in patients with Parkinson’s disease as measured by [11C]raclopride displacement and PET. Neurology 46:1430–1436
Trosch RM, Friedman JH, Lannon MC, Pahwa R, Smith D, Seeberger LC, O’Brien CF, LeWitt PA, Koller WC (1998) Clozapine use in Parkinson’s disease: a retrospective analysis of a large multicentered clinical experience. Move Disord 13:377–382
Turner W, Merlis S (1964) A clinical trial of pargyline and dopa in psychotic subjects. Dis Nerv Syst 25:538
van Kammen D, Kelley M (1991) Dopamine and norepinephrine activity in schizophrenia. An integrative perspective. Schizophr Res 4:173–191
White FJ, Wang RY (1983) Comparison of the effects of chronic haloperidol treatment on A9 and A10 dopamine neurons in the rat. Life Sci 32:983–993
Wolkowitz OM (1993) Rational polypharmacy in schizophrenia. Ann Clin Psychiatry 5:79–90
Yamauchi I (1972) Effects of l-dopa on schizophrenia. Seishin Igaku 14:941–949
Yamauchi M (1976) Effects of l-dopa and vitamin B6 on electroencephalograms of schizophrenic patients: a preliminary report. Folia Psychiatr Neurol Jpn 30:121–151
Yaryura-Tobias JA, Diamond B, Merlis S (1970a) The action of l-dopa on schizophrenic patients (a preliminary report). Curr Ther Res Clin Exp 12:528–531
Yaryura-Tobias JA, Wolpert A, Dana L, Merlis S (1970b) Action of l-dopa in drug induced extrapyramidalism. Dis Nerv Syst 31:60–63
Yaryura-Tobias JA, Diamond B, Merlis S (1971) Verbal communication with l-dopa treatment. Nature 234:224–225
Yokoi F, Grunder G, Biziere K, Stephane M, Dogan AS, Dannals RF, Ravert H, Suri A, Bramer S, Wong DF (2002) Dopamine D2 and D3 receptor occupancy in normal humans treated with the antipsychotic drug aripiprazole (OPC 14597): a study using positron emission tomography and [11C]raclopride. Neuropsychopharmacology 27:248–259
Acknowledgements
The authors thank Dr. Lee Friedman for his invaluable statistical consultation and Dr. Milton Strauss for his constructive review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
This research was conducted at and supported by the Louis Stokes Cleveland Department of Veterans Affairs Medical Center. Dr. Jaskiw has conducted clinical trials and/or received lecture sponsorship from the following: Abbot, Bristol-Myers-Squibb, Janssen, Lilly, Novartis, Pfizer, Zeneca. These data were first presented in preliminary form at the 5th International Congress for Schizophrenia Research, Warm Springs, Va., USA 1995.
Rights and permissions
About this article
Cite this article
Jaskiw, G.E., Popli, A.P. A meta-analysis of the response to chronic l-dopa in patients with schizophrenia: therapeutic and heuristic implications. Psychopharmacology 171, 365–374 (2004). https://doi.org/10.1007/s00213-003-1672-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-003-1672-y