
Abstract
Rationale
The acoustic startle response is inhibited when the startling stimulus is preceded by a weaker non-startling acoustic stimulus. This phenomenon, termed prepulse inhibition of acoustic startle (PPI), is impaired in schizophrenics compared to normal controls. To date, there is conflicting evidence regarding whether PPI impairments improve with antipsychotic treatment.
Objectives
To examine the effect of medication status on PPI in schizophrenic subjects.
Methods
First, we performed acoustic startle testing on 16 schizophrenic subjects when they were acutely decompensated off medication and later after they were stabilized on antipsychotic treatment. Second, in a between-group design, we tested 21 schizophrenic subjects off medication, 16 subjects on atypical neuroleptics, and 27 subjects on typical neuroleptics.
Results
In both the test-retest study and the between-group study, ANOVAs revealed no significant changes in startle to pulse alone stimuli, habituation of startle to pulse alone stimuli, PPI, latency to response onset, or latency to response peak between the treatment conditions.
Conclusions
Our results do not support the hypothesis that impaired sensorimotor gating in schizophrenia improves with antipsychotic treatment. Rather, impaired gating persists despite symptomatic improvement on medication.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Freud was the first to postulate the existence of a neuronal "barrier" that protected the organism from excessive sensory stimulation, the functioning of which was integral to the correct perception of reality (Freud 1895). Since the seminal observations of Kraepelin (1913) and Bleuler (1911) it has been recognized that patients with schizophrenia have abnormalities in information processing. Venables (1964) observed that these patients have impairments in their ability to filter out irrelevant stimuli. McGhie and Chapman (1961) noted that these patients have an inability to gate or screen out the "otherwise chaotic flow of information reaching consciousness," resulting in overstimulation and cognitive disintegration. These "sensorimotor gating deficits" are postulated to lead to sensory overload, thought disorder, and other psychotic symptoms (Venables 1964; Braff 1993). Numerous authors have noted and investigated the deficits in information processing seen in schizophrenic patients (Goldberg et al. 1991; Braff et al 1992; Goldberg and Gold 1995).
The acoustic startle response is a reflexive contraction of the skeletal muscles in response to a sudden acoustic stimulus. It occurs across mammalian species, can be easily measured, and is mediated by a simple subcortical circuit (Davis et al. 1982; Davis 1997; Koch 1998). In humans, the eyeblink component of the acoustic startle response can be easily and reliably measured by electromyographic (EMG) recording of the contractions of the orbicularis oculi muscle (Graham 1975). The modulation of this reflex by a preliminary non-startling stimulus is termed prepulse inhibition of the acoustic startle response (PPI), a paradigm that has been used as an operational measure of sensorimotor gating (Hoffman and Searle 1968; Graham 1975; Braff et al. 1978; Swerdlow et al. 1994). PPI is regulated by neuroanatomic regions implicated in the pathophysiology of schizophrenia, such as the prefrontal cortex, hippocampus, and nucleus accumbens (see Swerdlow et al. 2001). Furthermore, PPI is sensitive to pharmacological agents acting on dopaminergic, glutamatergic or serotonergic systems that are likewise implicated in schizophrenia (Swerdlow et al. 2001).
Patients with schizophrenia have a normal initial startle response, but have impaired habituation of startle (Geyer and Braff 1982; Bolino et al. 1992; Parwani et al. 2000). A number of studies have demonstrated an impairment in PPI in schizophrenics compared to normal controls (Braff et al. 1978, 1992, 1999, 2001; Grillon et al. 1992; Bolino et al. 1994; Schall et al. 1996; Kumari et al. 1999, 2000; Cadenhead et al. 2000; Parwani et al. 2000; Weike et al. 2000).
Impaired PPI has been proposed as a biologic marker of schizophrenia (Braff 1993; Swerdlow and Geyer 1998). However, the literature to date is inconclusive regarding whether impaired PPI is a stable abnormality across clinical conditions or is linked to the subjects being acutely ill or unmedicated. Most studies demonstrating abnormal PPI have been conducted on patients who were on antipsychotics at the time of testing (Braff et al. 1978, 1992, 1999; Grillon et al. 1992; Bolino et al. 1994; Schall et al. 1996; Kumari et al. 1998, 1999, 2000; Cadenhead et al. 2000), indicating that treatment does not fully normalize PPI deficits. It is possible, however, that the subjects in these studies would have demonstrated more severe deficits when they were unmedicated. Four published studies reported that medication status affects PPI (Kumari et al. 1998, 1999, 2000; Weike et al. 2000). However, one additional study did not detect group differences between schizophrenics with differing medication status (Parwani et al. 2000). To date, there are no published studies examining this issue with a repeated measures design.
In order to further study the relationship of PPI impairments to treatment status, we compared PPI in unmedicated versus medicated schizophrenic subjects using both a within-subject repeated measures design and a between-subject design.
Materials and methods
Study I: schizophrenic subjects tested pre- and post-treatment
Subjects
Sixteen male subjects with schizophrenia (mean age±SD=44.7±11.1) were enrolled after giving informed consent and signing an IRB approved consent form. The diagnosis of schizophrenia was established on the basis of chart reviews and the Structured Clinical Interview for DSM-IV, axis-1 (SCID-P). The subjects had no other psychiatric disorder (axis I or II), no active substance abuse nor history of substance dependence (aside from tobacco), nor did they have any active, clinically significant medical disorder. Subjects were recruited and enrolled if they had been off all antipsychotic medication for a minimum of 3 days (mean±SD=96.8±146.9 days off medication).
Study design
The subjects had clinical ratings and acoustic startle testing initially after they had been admitted to an acute psychiatric ward for acute decompensation, before they had received any antipsychotic treatment. They were then started on antipsychotic medication in an open label fashion as determined by their treating psychiatrist. All subjects were retested after 95.4±172.1 days of treatment when, in the treating clinician's opinion, they had returned to their clinical baseline. Six subjects were treated with haloperidol, one subject with perphenazine, one subject with mesoridazine, one subject with thiothixine, two with risperidone, three with olanzapine, and two with the putative novel antipsychotic M100907. Subject characteristics and symptom rating data are presented in Table 1.
Symptom ratings
The subjects' symptoms were rated with the Brief Psychiatric Rating Scale (BPRS; Overall and Gorham 1962). The BPRS total score was evaluated in addition to its subscale scores: positive symptoms, schizophrenia factor, and negative symptoms. Ratings were conducted by ED, AP, SS, or SM; the interclass correlation coefficient was 0.9.
Acoustic startle and PPI measurement
Acoustic startle and PPI testing was conducted with methods similar to that reported by Braff et al. (1992) and similar to methodology used in prior work from our laboratory (Parwani et al. 2000).
The subjects were screened with a brief hearing test to insure intact auditory ability using a Grason-Stadler audiometer (Model GS1710). All subjects were able to detect 25 dB[A] tones bilaterally at frequencies ranging from 250 to 8000 Hz.
The acoustic startle response (eyeblink component) was measured with an electromyographic (EMG) recording of the right orbicularis oculi muscle. Two 5 mm silver/silver chloride electrodes filled with gel were positioned approximately 1 cm under the pupil and 1 cm below the lateral canthus; a grounding electrode was placed behind the right ear over the mastoid. The measured impedance for each subject was less than 6 kohm. Recorded EMG activity was amplified and digitized using a computerized EMG startle response monitoring system (SR-LAB; San Diego Instruments). Amplifier gain was held constant at 1.0 for all subjects. The system was set to record 250 1-ms readings starting at the onset of the startle (pulse alone) stimulus. Subjects were seated in a chair next to the recording equipment and asked to look straight ahead and keep their eyes open during the test session. They were given no cognitive tasks to perform during testing.
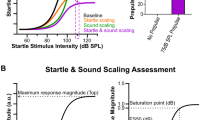
All acoustic stimuli were delivered binaurally through headphones (Maico,TDH-39-P). The startle session began with a 3-min acclimation period consisting of 70 dB [A] broadband noise that continued as background noise throughout the session. The pulse alone stimuli were 116 dB [A], 40 ms bursts of pure tone at a frequency of 1000 Hz with a near instantaneous rise time; the prepulse stimuli were 85 dB [A] 20 ms bursts of 1000 Hz pure tones presented 30, 60, or 120 ms prior to the startle stimulus. The startle session consisted of six blocks of 12 trials, for a total of 72 startle stimuli. Each block consisted of three pulse alone trials plus three trials of prepulse plus pulse at each of the three designated interstimulus intervals (30, 60, and 120 ms) presented in a pseudorandom order (randomized order except for the first trial in each block being a pulse alone trial). Each session began with an initial pulse alone trial. Inter-trial intervals were 11–45 s (average 26 s).
Pulse amplitudes are reported in machine digital units, where each digital unit equals 1.221 μV. Digital signals were smoothed by an averaging routine that calculates a rolling average of ten digital signals. The minimum response criterion for a peak was set at 10 arbitrary amplitude units.
Subjects whose mean amplitude of the three pulse alone trials in the first block was below 20 units were excluded from subsequent analyses in accordance with the criteria for non-startlers established by Braff et al. (1992). One subject was excluded by this criterion, so the final sample for PPI analyses included 15 subjects.
The onset latency (latency from stimulus to commencement of blink reflex) was defined by a shift of ten machine units from the baseline value occurring 21–120 ms after the pulse alone stimulus. Peak latency (latency from stimulus to maximum blink amplitude) is defined as the point of maximal amplitude occurring within 150 ms from the pulse alone stimulus. Responses in which onset and peak latencies differed by more than 95 ms were considered to be artifactual (not generated by the stimulus) and were discarded. Trials were also discarded if excessive EMG activity was observed during the first 20 ms of recording. Less than 5% of the trials were discarded using these parameters. On trials in which no scorable blink occurred, amplitude was recorded as zero.
Statistical analysis
Various analysis of variance (ANOVA) models were calculated on mean raw amplitude values and percent prepulse inhibition values (calculated for each block separately as [(mean pulse alone-mean prepulse)/mean pulse alone]×100). For startle data to pulse alone trials, overall ANOVA models included the within-subjects factors of Treatment status (two levels: unmedicated versus medicated) and Block (six levels: blocks 1–6). Next, an ANOVA was performed on raw startle amplitude data for blocks 1-3 to confirm the presence of PPI. In this model, a within-subjects factor of Trial type was used (four levels: pulse alone, 30 ms, 60 ms, and 120 ms ISI trial types).
For PPI and latency data, an ANOVA on collapsed data from blocks 1–3 was performed to circumvent confounds arising from reduced numbers of analyzable responses in later blocks. For PPI data, means for each trial type across blocks 1–3 were calculated and ANOVAs computed using within-subjects factors of Treatment status (two levels: unmedicated versus medicated) and Trial type (three levels: 30 ms, 60 ms, and 120 ms ISI trial types). ANOVAs on latency data were constructed in a similar manner, except that the Trial type factor had four levels (pulse alone, 30 ms, 60 ms, and 120 ms ISI trial types).
Significant main and interaction effects were followed up with appropriate post-hoc tests (Duncan's multiple range test). Alpha was set at 0.05 for all main effects and post-hoc tests. All variables were normally distributed (Kolmogorov-Smirnov test), except amplitude to pulse alone startle in blocks 1 and 2 of the unmedicated day, and pulse alone startle in blocks 1 and 4, and block 1 amplitude to the 120 ms prepulse trial on the medicated day. These variables differed from normality at the P=0.05 level because the cut-off of 0 for amplitude values resulted in skewness. ANOVA analyses were used because the F statistic is quite robust to deviations from normality due to skewness (Lindman 1974). Levene's test for homogeneity of variance was non-significant for all variables.
Analyses of rating data was conducted on BPRS total score and subscale totals using ANOVA with Treatment status as the within-subjects factor.
Study II: between-group study of schizophrenic subjects tested before or after treatment
Subjects
Sixty-four male subjects with schizophrenia (age=47.0±10.8) were enrolled after giving informed consent and signing an IRB approved consent form. Diagnostic and inclusion/exclusion criteria were identical to that of study I except that the subjects were not required to be unmedicated. The unmedicated subjects for this study were recruited from amongst newly admitted patients on the inpatient psychiatric unit at the Department of Veterans Affairs New York Harbor Healthcare System. Medicated subjects were recruited from the outpatient Mental Hygiene Clinic at the same medical center. Subject characteristics are presented in Table 2. Of the subjects on atypical antipsychotics, two were on clozapine, eight on olanzapine, four on risperidone, and two on sertindole. Of the subjects on typical antipsychotics, two were maintained on chlorpromazine, 16 on haloperidol, five on fluphenazine, one on perphenazine, one on trifluoperazine, and one on thioridizine.
Study design
The subjects received clinical ratings and acoustic startle testing on 1 day only. On the test day, they were either acutely decompensated and unmedicated (n=21), or at their stable clinical baseline on atypical (n=16) or typical (n=27) neuroleptic treatment. Sixteen of the unmedicated subjects in this dataset were also included as the 16 subjects of study 1.
Clinical ratings
Mental status was evaluated using the BPRS. The BPRS total score was evaluated as well as its subscale scores: positive symptoms, schizophrenia factor, and negative symptoms. Ratings were conducted by ED, AP, SS, or MS; the interclass correlation coefficient was 0.9.
Acoustic startle session
Methods for measurement of acoustic startle and PPI were identical to that used in study I.
Statistical analysis
The statistical approach was similar to that used in study I. Analysis of variance (ANOVA) models were calculated on mean raw amplitude values and percent prepulse inhibition values (calculated for each block separately as [(mean pulse alone-mean prepulse)/mean pulse alone]×100). For startle data to pulse alone trials, overall ANOVA models included the between-subjects factors of Medication group (three levels: atypicals versus typicals versus unmedicated) and the Block (six levels: blocks 1–6). Next, an ANOVA was performed on raw startle amplitude data for blocks 1–3 to confirm the presence of PPI. In this model, a within-subjects factor of Trial type was used (four levels: pulse alone, 30 ms, 60 ms, and 120 ms ISI trial types).
For PPI and latency data, ANOVAs on collapsed data from blocks 1–3 was performed to circumvent confounds arising from reduced numbers of analyzable responses in later blocks. For PPI data, means for each trial type across blocks 1–3 were calculated and ANOVAs computed using between-subjects factor of Medication group (three levels: atypicals versus typicals versus unmedicated) and Trial type (three levels: 30 ms, 60 ms, and 120 ms ISI trial types). ANOVA on latency data were constructed in a similar manner, except that the Trial type factor had four levels (pulse alone, 30 ms, 60 ms, and 120 ms ISI trial types).
Significant main and interaction effects were followed up with appropriate post-hoc tests (Duncan's multiple range test). Alpha was set at 0.05 for all main effects and post-hoc tests. The variables were normally distributed (Kolmogorov-Smirnov test) except amplitude to pulse alone trials, block 1 prepulse trials, onset latency for the 120 ms prepulse trials, and peak latency for the 30 ms prepulse trials. These variables differed from normality at the P=0.05 or P=0.01 level because these variables have an obligatory cutoff (0 machine units for amplitude values, 20 ms for onset latency, and 40 ms for peak latency) resulting in skewness. ANOVA analyses were used because the F statistic is quite robust to deviations from normality due to skewness (Lindman 1974). Levene's test for homogeneity of variance was non-significant for all variables.
Analyses of rating data were conducted on BPRS total scores and subscale totals using ANOVA with Medication group as the between-subjects factor.
Results
Study I: schizophrenic subjects tested pre- and post-treatment
Clinical ratings
As indicated in Table 1, there were significant declines in symptoms from the unmedicated to the medicated condition. ANOVAs computed using the within-subjects factor of Treatment status indicated improvement in BPRS total scores [F(1,15)=6.03, P=0.03], BPRS positive symptom subscale [F(1,15)=6.43, P=0.02], BPRS schizophrenia factor [F(1,15)=7.85, P=0.01], and the BPRS conceptual disorganization factor [F(1,15)=12.32, P=0.003]. There was no significant improvement in the BPRS negative symptom subscale [F(1,15)=2.39, P=0.14]. Supplemental ANOVAs constructed with Medication group as a between-group factor (atypicals versus typicals) and Treatment status (unmedicated versus medicated) as a within-subjects factor revealed similar significant declines in symptoms with treatment [BPRS total score: F(1,14)=6.41, P=0.02, BPRS positive symptom subscale: F(1,14)=6.35, P=0.02, BPRS schizophrenia factor: F(1,14)=8.93, P=0.01, and the BPRS conceptual disorganization factor: F(1,14)=14.32, P=0.002]. In this analysis, the BPRS negative symptom subscale again failed to improve significantly [F(1,14)=2.93, P=0.11]. In the above ANOVAs using Medication group as a between-subjects factor, there were no significant effects of Medication group or for the interaction of Medication group×Treatment status.
Startle amplitude and habituation
Differences in pulse alone startle amplitude values across blocks 1–6 were examined with a Treatment status (two levels: unmedicated and medicated)×Block (six levels) ANOVA design. In this model, the main effect of Treatment status was non-significant [F(1,14)=0.52, P=0.48]. The main effect of Block was significant [F(5,70)=7.87, P<0.0001], indicating habituation. The interaction of Treatment status×Block was non-significant [F(5,70)=0.79, P=0.56], indicating that habituation did not differ between the unmedicated and medicated states. The addition of a between-subjects factor of Medication (atypical versus typical) to the ANOVA model revealed no significance of the factors Medication [F(1,13)=0.21, P=0.65], Treatment status [F(1,13)=0.63, P=0.44], or the interaction of Medication×Treatment status [F(1,13)=0.26, P=0.62].
Means, standard deviations, and simple main effects on the pulse alone amplitude values are provided in Table 3.
Prepulse inhibition
Percent inhibition was examined across all three prepulse conditions (Trial type) in blocks 1–3 by an ANOVA model using Treatment status and Trial type as within-subjects factors. The factor Treatment status [F(1,14)=0.20, P=0.66; eta squared=0.014] was not significant, indicating that medication did not improve PPI. Trial type was significant [F(2,28)=14.98, P<0.0001] as expected, indicating more robust PPI in the trials with longer interstimulus intervals between the prepulse and pulse stimuli. The interaction of Treatment status×Trial type [F(2,28)=0.87, P=0.43] was not significant. Results are displayed in Table 2 and in Fig. 1. The addition of a between-subjects factor of Medication (atypical versus typical) to the ANOVA model revealed no significance of the factors Medication [F(1,13)=0.33, P=0.58], Treatment status [F(1,13)=0.09, P=0.78], or the interaction of Medication×Treatment status [F(1,13)=0.65, P=0.43].

Study I: blocks 1–3 PPI for Unmedicated and Medicated days, 30, 60, and 120 ms ISI trial types. ANOVA was non-significant for Treatment status
Response latencies
ANOVAs were computed on latency data from blocks 1–3. Onset latencies showed the expected latency facilitation whereby latency was shorter for the prepulse+pulse trials than for the pulse alone trials [F(3,42)=3.09, P=0.04]. Latency facilitation was also revealed by the ANOVA on peak latency data from blocks 1–3 [F(3,42)=13.75, P<0.0001]. There was no effect of Treatment status in the ANOVAs of onset [F(1,14)=0.82, P=0.38] or peak [F(1,14)=2.24, P=0.16] latencies.
Study II: between-group study of schizophrenic subjects tested before or during treatment
Clinical ratings
As indicated in Table 2, between-group ANOVAs on symptom ratings were significant for the effect of Medication group, indicating significantly greater symptoms in the unmedicated subjects compared to subjects treated with atypical and with typical antipsychotics [BPRS total scores: F(2,59)=10.72, P=0.0001, BPRS positive symptom subscale F(2,59)=14.15, P<0.0001, BPRS schizophrenia factor F(2,59)=15.27, P<0.0001, and the BPRS conceptual disorganization factor F(2,59)=13.50, P<0.0001]. There was no significant difference between medication groups in the BPRS negative symptom subscale [F(2,59)=1.21, P=0.31].
Startle to pulse alone trials and habituation
Startle amplitude to pulse alone stimuli in blocks 1–6 did not differ significantly between the three medication groups [ANOVA: F(2,61)=0.43, P=0.65] (Table 4). The main effect for Block was significant, indicating habituation in each of the three medication groups [F(5,305)=31.81, P<0.0001]. The interaction of Medication group and Block was not significant, indicating that each of the three groups habituated similarly [F(10,305)=0.83, P=0.60].
Startle amplitude to the four trial types across blocks 1–3 was examined by means of an ANOVA with Medication group as a between-subjects factor and Trial type as a within-subjects factor (four levels: pulse alone trials, prepulse+pulse with 30 ms ISI, prepulse+pulse with 60 ms ISI, and prepulse+pulse with 120 ms ISI). The ANOVA was non-significant for Medication group [F(2,61)=0.18, P=0.84]. The factor Trial type was significant [F(3,183)=36.75, P<0.0001], indicating the presence of PPI. The interaction of Medication group×Trial type was not significant [F(6,183)=1.20, P=0.31], indicating that the three medication groups had similar PPI.
Prepulse inhibition
Percent inhibition was examined across all three prepulse conditions (Trial type) in blocks 1–3 by ANOVA using Medication group as a between-subjects factor and Trial type as a within-subjects factor (Fig. 2). The effect of Trial type was significant as expected [F(2,122)=13.08, P<0.0001] but the effect of Medication group [F(2,61)=0.46, P=0.64; eta squared=0.015] and the interaction of Medication group×Trial type [F(4,122)=1.29, P=0.28] were not.

Study II: blocks 1–3 PPI for 30, 60, and 120 ms ISI trial types for three medication groups. ANOVA was non-significant for Unmedicated versus Atypicals versus Typicals
Response latencies
Both onset and peak latencies showed the expected latency facilitation whereby latency was shorter for the 30 ms trial types than for the pulse alone trials (Onset: F(3,171)=5.42, P=0.001; Peak: F(3,168)=16.87, P<0.0001], but there was no effect of Treatment group [Onset: F(2,57)=0.72, P=0.49; Peak: F(2,56)=2.80, P=0.07], indicating that treatment status did not affect onset or peak latencies. There was no significant interaction of Treatment group with Trial type [Onset: F(6,171)=0.95, P=0.46; Peak: F(6,168)=0.54, P=0.78].
Comparison of prepulse inhibition in schizophrenic subjects to normal controls
Although the current study was not designed to compare startle and PPI in schizophrenic subjects to that of normal controls, an analysis was conducted comparing subjects in the current study with 21 normal controls from a previously published study (Parwani et al. 2000). An ANOVA computed with a between-subjects factor of Group (two levels: normals and schizophrenics) on block 1 PPI was significant for the factor Group [F(1,83)=5.02, P=0.03], confirming that the schizophrenic subjects in the current study have impaired PPI.
Discussion
The main finding of this study was that treatment condition did not significantly alter acoustic startle, habituation of acoustic startle, or PPI. This finding was consistent across both our test-retest design (study I, unmedicated versus medicated days), and our between-subjects design (study II, unmedicated versus typical neuroleptic versus atypical antipsychotic).
The means for startle to pulse alone stimuli as well as PPI were similar to what we have reported previously for schizophrenic subjects (Parwani et al. 2000), and are also comparable to data on schizophrenics reported by other groups using similar startle session designs (Braff et al. 1992; Perry and Braff 1994).
A methodological issue relevant to our choice of strategy for analyzing PPI data is whether startle amplitude differences between subject groups could have a significant confounding effect on PPI calculated as a percent. We examined this question in 216 individuals tested to date in the same paradigm in our laboratory. There is no significant correlation between pulse alone startle and percent PPI in any block. An ANCOVA performed on PPI using startle to pulse alone trials in Block 1 as a covariate found no change in results compared to a corresponding ANOVA calculated without covariate analysis. This suggests that the analysis of PPI does not require the use of pulse alone amplitude as a covariate.
The clinical ratings differed robustly between the treatment conditions in both study I and study II, indicating that our unmedicated subjects were significantly more symptomatic than our medicated subjects. Neither of our datasets is designed to assess medication effects on PPI separately from differences arising from relative symptom remission.
It is possible that we did not detect PPI differences across different medication conditions because of insufficient power. The sample size we report here in our between group study has a power of 0.8 (t-test, 1-tailed, α=0.05) to detect a reduction in PPI of 20% between medicated and unmedicated subject groups. For comparison, a recent review (Hamm et al. 2001) indicated that the typical difference in percent PPI between schizophrenic subjects and normal controls in studies published to date was 20%. While our sample size is not sufficient to rule out significant differences between groups of less than 20%, the very low effect sizes in our PPI analyses suggests that there is not a meaningful difference in PPI between our unmedicated and medicated subjects.
The findings from this study contrast with results obtained from other groups who have studied the effect of treatment status on PPI. Kumari et al. (1998) reported a trend level difference in PPI between schizophrenic patients treated with typical neuroleptics and those treated with atypicals, suggesting that treatment can improve sensorimotor gating. A follow-up study from the same group (Kumari et al. 2000) with a larger sample size failed to replicate this PPI difference, although their subjects on typical antipsychotics differed from normals while their subjects on atypicals did not. The same group (Kumari et al. 1999) found impaired PPI in subjects on typical neuroleptics but normal PPI in clozapine treated schizophrenics. Weike et al. (2000) found impaired PPI in five unmedicated schizophrenics but PPI comparable to that of normal controls in 20 medicated subjects. A study conducted by our group (Parwani et al. 2000) found no differences in PPI between unmedicated and medicated schizophrenic subjects. All the above cited studies employed between-group designs. A second study from our group (Duncan et al., unpublished data), using both a within-subjects and between-group design, did not detect significant differences in PPI between subjects treated with olanzapine and haloperidol.
A related strategy to assess the relationship between PPI and clinical state has been to search for correlations between symptom severity and the degree of PPI impairment. Other groups have reported that PPI correlates with some aspects of clinical symptomatology such as thought disorder (Perry and Braff 1994; Perry et al. 1999), Wisconsin Card Sort performance (Butler et al. 1991), measures of distractibility and attention (Karper et al. 1996), and global ratings of positive and negative symptoms (Braff et al. 1999). Our group has examined the relationship between symptom severity and PPI in 55 schizophrenics studied in our laboratory and found modest correlations between positive and negative symptom severity and severity of PPI disruption (Duncan et al., unpublished data).
It has been postulated that impaired PPI is a biological marker of schizophrenia (Braff 1993; Swerdlow and Geyer 1998). We would expect such a biological marker to be predominantly stable across unmedicated and medicated conditions. Evidence supporting PPI as a stable biological marker for schizophrenia comes from the study of individuals postulated to be in the schizophrenia spectrum of disorders but who do not have the confounding effects of overt psychosis. Both schizotypal personality disordered patients (Cadenhead et al. 1993) and "psychosis-prone" individuals, tested both in a passive attend condition (Simons and Giardina 1992) and in an active task paradigm (Schell et al. 1995), have deficits in PPI similar to those seen in schizophrenia.
It might appear that there is an inherent contradiction between the correlations cited above linking symptom severity and impaired PPI and our finding of no improvement in gating with treatment that improves clinical symptoms. However, the effect size of the difference between schizophrenics and normals is rather modest in the first place, and many schizophrenic subjects have PPI within 1 SD of the mean for normals (Hamm et al. 2001). It is possible that a ceiling effect is at work, such that only a rather modest increase in gating is required to restore PPI to the range seen in normal controls. In the face of this ceiling effect we would expect that significant changes in PPI with treatment status would be difficult to detect in a heterogenous group of schizophrenic subjects. Hence, the evolving literature in this area reveals somewhat conflicting results regarding medication effects on PPI (Kumari et al. 1998, 1999, 2000; Parwani et al. 2000; Weike et al. 2000).
In the current study, our medicated subjects remained quite symptomatic as is revealed by their BPRS scores (Tables 1 and 2). The improvements in symptoms may not have been robust enough and the "room for improvement" in gating may be too small to allow for the reliable detection of gating improvement with treatment. It is possible that subjects who had a complete or near complete remission in symptoms on medication might have a more robust improvement in PPI.
The above discussion notwithstanding, our finding supports the concept of impaired PPI in schizophrenia being a predominantly stable abnormality persisting across treatment conditions (Braff 1993; Swerdlow and Geyer 1998). We would expect that such a stable abnormality could be transmitted genetically and hence would be found in family members. Indeed, one study has already reported such an abnormality in first degree relatives of schizophrenics (Cadenhead et al. 2000).
In summary, our data lend support to the hypothesis that impaired sensorimotor gating in schizophrenia is a predominantly stable abnormality that does not improve with treatment. Impaired gating may identify a subset of schizophrenics comprising a distinct endophenotype.
References
Bleuler E (1950) Dementia Praecox oder die Gruppe der Schizophrenien, 1911 (Dementia praecox or the group of schizophrenias). International University Press, New York
Bolino F, Manna V, DiCicco L, DiMichele V, Daneluzzo E, Rossi A, Cassachia M (1992) Startle reflex habituation in functional psychoses: a controlled study. Neurosci Lett 142:126–128
Bolino F, DiMichele V, DiCicco L, Manna V, Daneluzzo E, Cassachia M (1994) Sensorimotor gating and habituation evoked by electrocutaneous stimulation in schizophrenia. Biol Psychiatry 36:670–679
Braff DL (1993) Information processing and attention dysfunctions in schizophrenia. Schizophr Bull 19:233–259
Braff DL, Stone C, Callaway E, Geyer M, Glick I, Bali L (1978) Prestimulus effects of human startle reflex in normals and schizophrenics. Psychophysiology 15:339–343
Braff DL, Grillon C, Geyer MA (1992) Gating and habituation of the startle reflex in schizophrenic patients. Arch Gen Psychiatry 49:206–215
Braff DL, Swerdlow NR, Geyer MA (1999) Symptom correlates of prepulse inhibition deficits in male schizophrenic patients. Am J Psychiatry 156:596–602
Braff DL, Geyer MA, Light GA, Sprock J, Perry W, Cadenhead, KS, Swerdlow NR (2001) Impact of prepulse characteristics on the detection of sensorimotor gating deficits in schizophrenia. Schizophr Res 49:171–178
Butler RW, Jenkins MA, Geyer MA, Braff DL (1991) Wisconsin card-sorting deficits and diminished sensorimotor gating in a discrete subgroup of schizophrenic patients. In: Tamminga CA, Schultz SC (eds) Schizophrenia research (Advances in Neuropsychiatry and Psychopharmacology, vol 1). Raven Press, New York, pp 163–168
Cadenhead, KS, Geyer MA, Braff DL (1993) Impaired startle prepulse inhibition and habituation in patients with schizotypal personality disorder. Am J Psychiatry 150:1862–1867
Cadenhead KS, Swerdlow NR, Shafer KM, Diaz M, Braff DL (2000) Modulation of the startle response and startle laterality in relatives of schizophrenic patients and in subjects with schizotypal personality disorder: evidence of inhibitory deficits. Am J Psychiatry 157:1660–1668
Davis M (1997) The neurophysiological basis of acoustic startle modulation: Research on fear motivation and sensory gating. In: Lang PJ, Simons RF, Balaban MT (eds) Attention and orienting: sensory and motivational processes. Erlbaum, London, pp 69–96
Davis M, Gendelman D, Tischler M, Gendelman P (1982) A primary acoustic startle circuit: lesion and stimulation studies. J Neurosci 2:791–905
Freud S (1895) Project for a scientific psychology I. Standard Edition 1:295–346
Geyer MA, Braff DL (1982) Habituation of the blink reflex in normals and schizophrenic patients. Psychophysiology 19:1–6
Goldberg TE, Gold JM (1995) Neurocognitive functioning in patients with schizophrenia: an overview. In: Bloom FE, Kupfer DJ (eds) Psychopharmacology: the fourth generation of progress. Raven Press, New York, pp 1245–1257
Goldberg TE, Gold JM, Braff DL (1991) Neuropsychological functioning and time-linked information processing in schizophrenia. In: Tasman A, Goldfinger SM (eds) Review of psychiatry (vol 10). American Psychiatric Press, Washington, pp 60–78
Graham FK (1975) The more or less startling effects of weak prestimuli. Psychophysiology 12:238–248
Grillon C, Ameli R, Charney DS, Krystal J, Braff DL (1992) Startle gating deficits occur across prepulse intensities in schizophrenic patients. Biol Psychiatry 32:939–943
Hamm A, Weike A, Schupp H (2001) The effect of neuroleptic medication on prepulse inhibition in schizophrenia patients: current status and future issues. Psychopharmacology 156:259–265
Hoffman HS, Searle JL (1968) Acoustic and temporal factors in the evocation of startle. J Acoustic Soc Am 43:269–282
Karper LP, Freeman GK, Grillon C, Morgan CA, Charney D, Krystal J (1996) Preliminary evidence of an association between sensorimotor gating and distractibility in psychosis. Neuropsychiatr Clin Neurosci 8:60–66
Koch M (1998) The neurobiology of startle. Prog Neurobiol 59:107–128
Kraepelin E (1919) Dementia praecox and paraphrenia, 1913 (translated by Barclay RM). E & S Livingston, Edinburgh
Kumari V, Soni W, Gray JA, Sharma T (1998) Prepulse inhibitory deficits in schizophrenia: the effects of typical and atypical antipsychotic drugs. J Psychopharmacol 12:A67
Kumari V, Soni W, Sharma T (1999) Normalization of information processing deficits in schizophrenia with clozapine. Am J Psychiatry 156:1046–1051
Kumari V, Soni W, Mathew VM, Sharma T (2000) Prepulse inhibition of the startle response in men with schizophrenia. Arch Gen Psychiatry 57:609–614
Lindman HR (1974) Analysis of variance in complex experimental designs. Scott, Forresman, New York
McGhie A, Chapman J (1961) Disorders of attention and perception in early schizophrenia. Br J Med Psychol 34:103–116
Overall JE, Gorham DR (1962) The Brief Psychiatric Rating Scale. Psychol Rep 10:799–812
Parwani A, Duncan E, Bartlett E, Madonick S, Rajan R, Chappell P et al. (2000) Prepulse inhibition of acoustic startle in acute and chronic schizophrenics. Biol Psychiatry 47:662–669
Perry W, Braff DL (1994) Information-processing deficits and thought disorder in schizophrenia. Am J Psychiatry 151:363–367
Perry W, Geyer MA, Braff DL (1999) Sensorimotor gating and thought disturbance measured in close temporal proximity in schizophrenic patients. Arch Gen Psychiatry 56:277–281
Schall U, Schon A, Zerbin D, Eggers C, Oades RD (1996) Event-related potentials during an auditory discrimination with prepulse inhibition in patients with schizophrenia, obsessive-compulsive disorder and healthy subjects. Int J Neurosci 84:15–33
Schell AM, Dawson ME, Hazlett EA, Filion DL (1995) Attentional modulation of startle in psychosis prone college students. Psychophysiology 32:266–273
Simons RF, Giardina BD (1992) Reflex modification in psychosis-prone young adults. Psychophysiology 29:8–16
Swerdlow NR, Geyer MA (1998) Using an animal model of deficient sensorimotor gating to study the pathophysiology and new treatments of schizophrenia. Schizophr Bull 24:285–301
Swerdlow NR, Braff DL, Taaid N, Geyer MA (1994) Assessing the validity of an animal model of deficient sensorimotor gating in schizophrenic patients. Arch Gen Psychiatry 51:139–154
Swerdlow NR, Geyer MA, Braff DL (2001) Neural circuit regulation of prepulse inhibition of startle in the rat: current knowledge and future challenges. Psychopharmacology 156:194–215
Venables P (1964) Input dysfunction in schizophrenia. In: Maher BA (ed) Progress in experimental personality research. Academic Press, Orlando, pp 1–47
Weike AI, Bauer U, Hamm AO (2000) Effective neuroleptic medication removes prepulse inhibition deficits in schizophrenia patients. Biol Psychiatry 47:61–70
Acknowledgements
This work was completed with the support of a Department of Veterans Affairs Merit Review Grant (E.D.), the Department of Veterans Affairs New York Harbor Healthcare System, the Atlanta Veterans Affairs Medical Center, the Department of Psychiatry and Behavioral Sciences at Emory University School of Medicine, Pfizer Inc., and Eli Lilly and Company. The editorial assistance of Barbara Lewison is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Duncan, E.J., Szilagyi, S., Efferen, T.R. et al. Effect of treatment status on prepulse inhibition of acoustic startle in schizophrenia. Psychopharmacology 167, 63–71 (2003). https://doi.org/10.1007/s00213-002-1372-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-002-1372-z