
Abstract
Previous studies showed that amiodarone causes state-dependent inhibition of Na+ channels thereby mediating an atrial-selective drug effect. The aim of the present study was to investigate the impact of the new antiarrhythmic compound dronedarone on Na+, Ca2+ and hyperpolarization-activated cyclic nucleotide-gated ion channels. Monophasic action potentials (MAP) and effective refractory period (ERP) were studied in arterially perfused left atria and ventricular wedge preparations of the pig. Fast Na+ and Ca2+ currents in isolated guinea pig ventricular myocytes as well as human HCN4 channels expressed in Chinese hamster ovary (CHO) cells were investigated with the patch-clamp technique. In left atrial epicardial tissue, dronedarone (3 μM) had no effect on the MAP duration, but the drug caused a significant prolongation of the ERP from 145 ± 9 to 184 ± 17 ms (n = 6; p < 0.05). In guinea pig ventricular myocytes, dronedarone exhibited a state-dependent inhibition of the fast Na+ channel current with an IC50 of 0.7 ± 0.1 μM, when the holding potential (V hold) was −80 mV. The maximal block at the highest concentration used was 77 ± 8%. In contrast, when V hold was −100 mV, inhibition with 10 μM dronedarone was only 9 ± 3% (n = 7). Dronedarone blocked Ca2+ currents elicited by rectangular pulses at V hold = −40 mV with an IC50 value of 0.4 ± 0.1 μM (maximal block by 10 μM dronedarone, 80 ± 6%), whereas at V hold = −80 mV, 10 μM dronedarone blocked only 20 ± 6% (n = 4) of the current. Applying an action potential clamp (V hold = −80 mV) yielded an IC50 of 0.4 ± 0.3 μM. Human HCN4 channels expressed in CHO cells were blocked by dronedarone with an IC50 of 1.0 ± 0.1 μM. Inhibition of fast Na+ and Ca2+ channels by dronedarone depends on the cell’s resting membrane potential (state-dependent block) favouring an atrial-selective mode of action. Besides fast Na+ and Ca2+ channels, dronedarone also inhibits HCN4 currents. This might contribute to the clinically observed reduction in heart rate seen in patients in sinus rhythm after dronedarone treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dronedarone is a non-iodinated benzofuran derivative, pharmacologically related to amiodarone, which showed positive outcomes in recent clinical trials. In the phase II studies EURIDIS and ADONIS (Singh et al. 2007), dronedarone significantly reduced the time to recurrence of atrial fibrillation (AF), and in the large phase III ATHENA trial, the combined endpoint of cardiovascular hospitalization or mortality was significantly reduced in patients with AF (Hohnloser et al. 2009). Like amiodarone, dronedarone is a multichannel blocker (Doggrell and Hancox 2004). Recently, it was reported that chronic amiodarone treatment exhibits an atrial-selective effect by reducing the atrial effective refractory period (ERP) more potently than the ventricular ERP (Burashnikov et al. 2008). Furthermore, the authors found that both in coronary-perfused atrial and ventricular canine wedge preparations, the ERP increased to a greater degree than the respective action potential duration (APD). This discrepancy between ERP and APD was particularly observed in the atria. The greater ERP prolongation in the atria was caused, in large part, by the development of post-repolarization refractoriness (PRR). One possible explanation for this effect is the state-dependent inhibition of Na+ channels by amiodarone, which means that the binding of the drug is increased when the channel is in its inactivated state. As the resting membrane potential in atria is more depolarized than in ventricles, amiodarone is considered to block atrial Na+ channels more potently than ventricular ones (Burashnikov et al. 2008; Burashnikov and Antzelevitch 2009). One aim of the present study was to investigate whether dronedarone displays a similar atrial-selective inhibition of the fast Na+ channel as amiodarone.
In animal studies, dronedarone reduced heart rate (Finance et al. 1995; Manning et al. 1995b; Varro et al. 2001) and induced a marked reduction in rabbit sinus node automaticity (Celestino et al. 2007). It is well established that a reduction in heart rate can be achieved by inhibition of the hyperpolarization-activated ion channel current (I f) in the sinoatrial node (DiFrancesco 2006). The responsible isoforms of the hyperpolarization-activated cyclic nucleotide-gated ion channel 1 (HCN1), 2 and 4 are expressed in the heart, with HCN4 being the major component in the pacemaker region (Thollon et al. 2007). In order to investigate the effect of dronedarone on HCN4 currents, we performed patch-clamp experiments on Chinese hamster ovary (CHO) cells expressing the human HCN4 channel.
Methods
Arterially perfused ventricular wedge and left atrium of the pig
All investigations with animals conform to the Guide for the Care and Use of Laboratory Animals published by the US National Institute of Health (NIH publication no. 85-23, revised 1996) and were performed by technicians specifically trained and experienced in animal care following approval by the Ethical Review Board of the State of Hessen and in accordance with the German Animal Protection Law.
Male castrated pigs of the German landrace (15–20 kg; Jochen Schäfer, Nendershausen, Germany) were anaesthetized with intravenous application of pentobarbital (30 mg/kg). In addition, 400 U/kg of heparin Na-salt was applied intravenously. During deep anaesthesia, hearts were excised via left thoracotomy resulting in humane euthanasia. Hearts were immediately immersed in cold (4°C), oxygenated cardioplegic solution (in millimolars): NaCl 118; KCl 20; NaHCO3 25; MgSO4 1.2; NaH2PO4 1.2; glucose 20 and pyruvic acid sodium salt 2; gassed with 95% O2 + 5% CO2. The method of preparing isolated, arterially perfused ventricular or atrial preparations was adopted from the wedge preparation technique described elsewhere (Yan and Antzelevitch 1996).
Atrial preparation
Left and right ventricles as well as the right atrium were excised with scissors. The remaining left atrium was cannulated via the ramus circumflexus of the left coronary artery and perfused at a constant flow of 12 ml/min with cardioplegic solution. All blood vessels that were not supplying the left atrium were ligated. The tissue was immersed into an organ bath heated to 37°C and was perfused (12 ml/min) and superfused (20 ml/min) with Tyrode solution (in millimolars): NaCl, 118 mM; KCl, 4.7 mM; CaCl2, 2.5 mM; NaHCO3, 25 mM; MgSO4, 1.2 mM; NaH2PO4, 1.2 mM; glucose, 5 mM and pyruvic acid sodium salt, 2 mM; gassed with 95% O2 + 5% CO2. The tissue was allowed to equilibrate for 30 min under constant electrical stimulation with 2.5 Hz (rectangular pulses of 1 to 3 V and 1 to 2 ms duration).
Ventricular preparation
The left and right atria were excised with scissors. A wedge was excised consisting of about 2 cm of ventricular tissue on both sides of the ramus interventricularis of the left coronary artery and about 1 cm of the septum. The ramus interventricularis was cannulated and perfused (12 ml/min) with cardioplegic solution. The major leaking blood vessels were tied off with silk sutures to prevent loss of perfusate. The tissue was immersed into an organ bath heated to 37°C and was arterially perfused (12 ml/min) with Tyrode solution containing 20 mM KCl. In addition, the whole tissue was continuously superfused with the same solution. After 10 min, KCl was reduced in four steps (each 10 min in duration) to 4.7 mM and was equilibrated for 30 min under electrical stimulation with a frequency of 2.5 Hz.
Monophasic action potentials (MAP) were recorded with a custom-built electrode that combined the possibility of MAP detection along with tissue stimulation. The electrode was mounted on a micromanipulator (Leitz, Wetzlar, Germany) and gently pressed on the tissue. The MAP and bath electrode were connected to a microelectrode amplifier (type 309, Hugo-Sachs Elektronik, March-Hugstetten, Germany). The stimulation electrodes were connected to a personal computer, equipped with the recording and analysing software Iso 2 (MFK Niedernhausen, Germany). For recording of the ERP, a second stimulus S2 was applied about 100 ms after the first stimulus S1, and the time interval S1–S2 was increased in steps of 5 or 10 ms at stimulation frequencies of 2.5 Hz. The S1–S2 interval for the first triggered MAP was considered as ERP. In ventricular preparations, the MAP duration at 90% repolarization (MAPD90) was measured, whereas in atrial preparations the MAP duration at 80% repolarization (MAPD80) was recorded.
Recording of Na+ and Ca2+ currents with the patch-clamp technique
Male guinea pigs (350–500 g; Dunkin Hartley, Harlan Laboratories GmbH, Eystrup, Germany) were sacrificed by concussion followed by exsanguination, according to Close et al. (1997). The heart was quickly removed and retrogradely perfused via the aorta at 37°C, first for 5 min with Ca2+-free Tyrode solution (in millimolars): NaCl, 143 mM; KCl, 5.4 mM; MgCl2, 0.5 mM; NaH2PO4, 0.25 mM; 4-(2-hydroxyethyl)-1-piperazineethanesulphonic acid (HEPES), 5 mM and glucose, 10 mM; pH adjusted to 7.2 with NaOH. Then, the perfusion was continued with the Tyrode solution containing 15 μM CaCl2 and 0.03% collagenase (type CLS II, Biochrom KG, Berlin, Germany) until atrial tissue softened (5–7 min). Thereafter, the heart was washed with storage solution (in millimolars): KCl, 40 mM; KH2PO4, 20 mM; MgCl2, 1 mM; ethylene glycol tetraacetic acid (EGTA), 2 mM; glucose, 10 mM; taurine, 20 mM; l-glutamic acid, 50 mM and HEPES, 10 mM (pH 7.2 with KOH). The left ventricle was cut into small pieces, and myocytes were dispersed by gentle shaking. Cells were then filtered through a nylon mesh. Thereafter, cells were washed twice by sedimentation and kept at room temperature in storage solution.
Whole-cell currents were recorded with an EPC-9 patch-clamp amplifier (HEKA Elektronik, Lambrecht, Germany). A small aliquot of cell-containing solution was placed in a perfusion chamber, and after a brief period of allowing cell adhesion to the bottom, the chamber was continuously perfused with bathing solution. Patch pipettes were pulled from borosilicate glass capillaries and were heat-polished. When filled with pipette solution, they had a resistance of 2 to 3 MΩ. Offset voltages generated when the pipette was inserted in NaCl solution (1 to 5 mV) were zeroed before formation of the seal. After formation of the whole-cell mode, the series resistance was compensated by 40–60% and the electrical capacitance caused by the cell membrane was compensated by the EPC-9 compensation network. The cell capacitance was 178 ± 9 pF (n = 22), and the series resistance was 5 to10 MΩ. The cell potential was in the range of −70 to −80 mV.
When fast Na+ channel current was recorded, the pipette solution was composed of (in millimolars) CsCl, 130 mM; MgCl2, 2 mM; CaCl2, 1 mM; EGTA, 15 mM; Mg-ATP, 4 mM; glucose, 10 mM and HEPES, 10 mM (pH = 7.2 with CsOH), and the bathing solution was composed of (in millimolars) NaCl, 20 mM; choline chloride, 110 mM; CsCl, 3 mM; MgCl2, 1 mM; sucrose, 40 mM; glucose, 5 mM and HEPES, 5 mM (pH = 7.4 with CsOH). Voltage pulses (20 ms) were applied from the holding potential of −100 mV or −80 to −30 mV with a frequency of 1 Hz. The peak of the current was evaluated, and the percent inhibition referenced to the current in absence of dronedarone was calculated (control). In order to reduce the amplitude of the Na+ channels, experiments were performed at room temperature.
Ca2+ channels were recorded in Na+-free bathing solution with all K+ currents blocked. The bathing solution consisted of (in millimolars) N-methyl-d-glucamine (NMDG), 125 mM; CsCl, 5 mM; CaCl2, 1.8 mM; MgCl2, 1 mM; tetraethyl ammonium chloride salt (TEA-Cl), 20 mM; glucose, 11.5 mM and HEPES, 10 mM; pH = 7.4 with HCl/CsOH. The tip of the pipette was filled with (in millimolars) CsCl, 110 mM; EGTA, 10 mM; TEA-Cl, 20 mM; Mg-ATP, 5 mM and HEPES,10 mM; pH = 7.2 with HCl/CsOH, and the pipette was back-filled with CsCl, 80mM; EGTA, 40 mM; TEA-Cl, 20 mM; Mg-ATP, 5 mM and HEPES, 10 mM; pH = 7.2 with HCl/CsOH. Ca2+ currents were evoked by voltage pulses from the holding potential (either −80 or −40 mV) to 0 mV for 300 ms with a frequency of 0.2 Hz. The peak current was evaluated and the percent inhibition referenced to the current in absence of dronedarone was calculated (control). All experiments with Ca2+ channels were performed at 36 ± 1°C.
For both the measurement of Na+ as well as Ca2+ channels, dronedarone was allowed to equilibrate for 10 min. Time-matched control measurements were carried out in which cells were recorded for 10 min in absence of the drug.
Action potential clamp
Ca2+ currents were also recorded with the action potential clamp method. An action potential was recorded from sharp microelectrode experiments in a guinea pig papillary muscle (Fig. 4a). The action potential was stored in the Pulse software and served as the command voltage in the patch-clamp experiments. The bathing solution had the same composition as reported above for rectangular pulses, but in addition, it contained 5 μM HMR1098, 1 μM dofetilide and 1 μM HMR1556 to inhibit K ATP, I Kr and I Ks currents, respectively. The pipette solution was the same as shown above. After recording of a control trace, one concentration of dronedarone was applied for 10 min, and then a solution containing 200 μM CdCl2 was perfused into the bath. It is considered that this concentration of CdCl2 completely blocked the Ca2+ channels. The inhibition of the Ca2+ current by dronedarone was evaluated by subtraction of the trace obtained with CdCl2 and by measuring the area under the curve of the difference current. The percent inhibition of this electrical charge was plotted. The values recorded under control conditions and in presence of CdCl2 were considered as 0% and 100% inhibition, respectively.
Recording of hHCN4 currents expressed in CHO cells
Human HCN4 (hHCN4) cDNA (GenBank accession number AJ132429) was subcloned into the eukaryotic expression vectors pcDNA3.1 and pcDNA3.1/zeo (Invitrogen, Groningen, Netherlands). Chinese hamster ovary (CHO) cells (American Type Culture Collection, Rockville, MD, USA) were transfected with hHCN4 expression constructs. Transfection was carried out using Lipofectamine (Life Technologies/Gibco BRL, Karlsruhe, Germany) according to the manufacturer’s instructions. To boost channel expression, CHO cells were consecutively transfected with hHCN4 expression constructs. Stably transfected cells were grown in Iscove medium (Biochrom AG, Berlin, Germany) containing 10% foetal calf serum and 2 mM l-glutamine, with addition of 350 μg/ml Zeocin (Invitrogen) and 900 μg/ml G418 (PAA Laboratories). Cultures were maintained at 37°C in 5% CO2. Cells were detached by exposure to Accutase® (PAA Laboratories), reseeded and kept in culture for 2–4 days before use.
Cells were assayed using the standard whole-cell patch-clamp technique. Cells were removed from the tissue culture flask by addition of 2 ml Accutase for 5 min and placed in a perfusion chamber. The extracellular solution contained (in millimolars) NaCl, 110 mM; KCl, 30 mM; CaCl2, 1.8 mM; MgCl2, 0.5 mM and HEPES, 5 mM; pH adjusted to 7.4 with NaOH. The intracellular solution contains (in millimolars) KCl, 120 mM; NaCl, 10 mM; MgCl2, 1.1 mM; EGTA, 1 mM and HEPES, 10 mM; pH adjusted to 7.2 with KOH. Experiments were carried out at room temperature. The mean cell capacitance was 44 ± 4 pF (n = 25). Rectangular pulses from a holding potential of −35 to −110 mV were applied for 3 s with a frequency of 0.05 Hz. The difference in the current between the end and the start of the voltage pulse was recorded.
Statistics
Values are given as mean ± SEM. Statistical analysis was performed using Student’s t test for either paired or unpaired samples. A value of p < 0.05 was considered statistically significant.
Materials
Dronedarone was synthesized in the laboratories of medicinal chemistry of Sanofi-Aventis in France, and amiodarone hydrochloride was purchased from Sigma, Germany. Ivabradine was extracted from tablets (Procolaran, Servier, France) in the medicinal chemistry department of Sanofi-Aventis in Frankfurt, Germany. Dronedarone, amiodarone and ivabradine were dissolved in DMSO (10 mM) and further diluted in the measuring solution. The highest concentration of dronedarone that could be held in solution was 10 μM. The vehicle DMSO in concentrations up to 0.1% (which was the highest concentration used in this study) had no significant effects on Na+, Ca2+ or HCN4 currents. In contrast, there was a considerable current run-down over the exposure time of 10 min that was taken into account when dose–response curves were calculated.
Results
Arterially perfused porcine ventricular wedges and atria
We studied the effect of dronedarone (3 μM) on arterially perfused ventricular and left atrial preparations obtained from pig hearts. Therefore, we recorded the APD as well as the ERP.
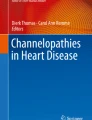
In six ventricular wedge preparations (Fig. 1a, b) from individual animals, we observed no statistically significant effects of dronedarone neither on the duration of the MAPD90 nor on the ERP.

Effect of dronedarone (3 μM) on the monophasic action potential in ventricle (a, b) and in left atrial (c, d) preparations; a and c show original recordings of the MAP in the arterially perfused preparations. The solid line represents the recording in absence of dronedarone (control) and the dashed line the recording in presence of the compound. The pacing frequency was 2.5 Hz; b and d represent statistical analysis of MAPD and ERP from six to seven individual animals
In the atrial preparation (Fig. 1c, d), dronedarone also had no significant effect on the MAPD80, but contrary to the finding in the ventricle, the drug prolonged the refractory period in the atrium from 145 ± 9 to 184 ± 17 ms (n = 6; p < 0.05).
Patch-clamp recordings in guinea pig ventricular myocytes
Investigation of Na+ channels
As the elongation of the ERP without an influence on the APD could be due to an inhibition of fast Na+ channels, we studied the underlying current in isolated guinea pig cardiomyocytes.
Fast Na+ currents were investigated by applying rectangular voltage pulses from the holding potential of either −80 mV or −100 to −30 mV. After performing a control recording, either dronedarone or vehicle was added to the bathing solution and washed in for 10 min. The current run-down in absence of the drug was taken into account for the calculation of the dose–response curve. Figure 2 demonstrates typical current traces obtained with pulses from a holding potential of −80 and −100 mV, respectively, and the inhibition of the Na+ currents by dronedarone. As depicted in Fig. 2c, the inhibition of the Na+ current by dronedarone yielded an IC50 value of 0.7 ± 0.1 μM when the cells were clamped at a holding potential of −80 mV. The maximal block was 77 ± 8% at a dronedarone concentration of 10 μM. In contrast, the efficacy of dronedarone was greatly reduced when V hold was −100 mV. Under these conditions, even the highest concentration of dronedarone (10 μM) produced only a slight inhibition of the current by 9 ± 3% (n = 7). Because of the minimal effect of dronedarone at the holding potential of −100 mV, an IC50 value could not be calculated.

Effect of dronedarone on Na+ channels in guinea pig ventricular cardiomyocytes. a Typical recordings of whole-cell Na+ currents obtained by voltage pulses from the holding potential of −80 to −30 mV. b Typical recordings of whole-cell Na+ currents as shown in a but starting from a holding potential of −100 mV. c Summary of results obtained with dronedarone on whole-cell Na+ currents. When the holding potential was −80 mV (filled circles), the curve fit to the logistic function yielded an IC50 of 0.7 ± 0.1 μM. The maximal block was about 80% of the total current. At holding potential of −100 mV (open circles), maximal current block was only about 10%. The number of experiments for each data point is given in brackets
Investigation of Ca2+ channels
The block of Ca2+ channels by dronedarone was first investigated with rectangular voltage pulses starting from different holding potentials. When voltage pulses were applied from V hold = −40 to 0 mV (Fig. 3a), we obtained an IC50 value for the inhibition by dronedarone of 0.4 ± 0.1 μM (Fig. 3c). The maximal block by 10 μM dronedarone was found to be 80±6%. As the physiological membrane potential is more negative, we repeated the recordings with voltage pulses starting from V hold = −80 mV (Fig. 3b, with Na+ currents blocked by NMDG+). Under these conditions, inhibition of the Ca2+ current even by the highest concentration of dronedarone (10 μM) was less pronounced and amounted to only 20 ± 6% (n = 4). These results indicate that inhibition of Ca2+ channels by dronedarone is state dependent. Next, we applied action potential clamps in order to record the Ca2+ current under more physiological conditions. A typical action potential was recorded with the sharp electrode technique in a guinea pig papillary muscle (Fig. 4a), stored in the patch-clamp electronic device and served as the test potential in voltage clamp experiments. Figure 4b demonstrates typical current traces obtained by clamping the cell on the voltage given by the action potential, under control conditions, in presence of different concentrations of dronedarone and in presence of 200 μM cadmium. The difference in current between the respective current trace and the current in presence of cadmium is considered as Ca2+ current and is demonstrated in Fig. 4c. The curve fit of the current blocked by dronedarone yielded an IC50 of 0.4 ± 0.3 μM (Fig. 4d).

Effect of dronedarone on Ca2+ channel currents recorded with rectangular voltage pulses. a Voltage pulse from the holding potential of −40 to 0 mV. b Voltage pulse from the holding potential of −80 to 0 mV. c Summary of results. When the holding potential was −40 mV (filled circles), the logistic function yielded an IC50 of 0.4 ± 0.1 μM. At the holding potential of −80 mV (open circles), even the inhibition due to the highest concentration of dronedarone was in the range of the intrinsic current run-down

Effect of dronedarone on Ca2+ channel currents recorded with the action potential clamp technique. a Voltage pulse used for clamping the myocytes. b Current traces obtained under control conditions, in the presence of 200 μM CdCl2 and dronedarone (0.3 and 1 μM). c Difference current between the trace obtained with CdCl2 and compound. d The curve fit to the logistic function yielded an IC50 of 0.4 ± 0.3 μM. The number of experiments for each data point is given in brackets
Effect of dronedarone on hHCN4 channels in CHO cells
CHO cells expressing the hHCN4 channel were fragile and, therefore, were tested at room temperature with the whole-cell patch-clamp technique. Voltage pulses were applied from V hold = −35 to −110 mV for 3 s at a frequency of 0.05 Hz. When only vehicle was added to the bathing solution, a decrease of the current by 26 ± 5% (n = 5) was observed after the recording time of 10 min. This run-down was taken into account by inserting the data point of 26 ± 5% as control value (Fig. 5b).

Patch-clamp recordings of hHCN4 currents in CHO cells. a Typical current traces obtained by voltage pulses from the holding potential of −35 to −110 mV for 3 s in the absence (control) and presence of dronedarone. b Curve fit to the logistic function yielded an IC50 value of 1.0 ± 0.1 μM. The number of experiments for each data point was 5
As demonstrated in Fig. 5a, after application of the voltage pulse, an inward current developed, which did not reach steady state within the pulse duration of 3 s. Addition of dronedarone caused a significant attenuation of the current at the end of the pulse, yielding an IC50 value of 1.0 ± 0.1 μM (Fig. 5b).
Similar experiments were also performed with amiodarone and ivabradine. Both compounds dose-dependently inhibited the hHCN4 current at the end of the 3-s pulse, yielding an IC50 value of 0.8 ± 0.1 μM for amiodarone (n = 6–13) and an IC50 value of 1.1 ± 0.2 μM for ivabradine (n = 5–7).
Discussion
The present work shows that dronedarone influences the ERP in atrial but not ventricular tissue without an impact on the APD. This may be due to a state-dependent blocking behaviour of the drug as will be discussed in the following.
Atrial-selective effect of dronedarone
Starting point of our work was the ex vivo study from Burashnikov et al. (2008) showing an atrial-selective effect of the antiarrhythmic drug amiodarone. Using coronary-perfused atrial and ventricular wedge preparations isolated from untreated and chronic amiodarone-treated dogs, it was observed that chronic amiodarone prolonged the APD predominantly in atria compared to ventricles. The ERP was even more prolonged than the APD in both ventricular and atrial preparations due to the development of post-repolarization refractoriness (PRR). The authors explained this effect by a state-dependent inhibition of the Na+ channels by amiodarone. In the present study, we could show that dronedarone has an atrial-selective effect also. While the drug did not significantly influence the MAPD90 or the ERP in porcine ventricular wedge preparations, it elongated the ERP in the atrium. This ERP elongation appeared without a change in the MAPD80 which is well in line with recently published results from dog atria (Burashnikov et al. 2010). The authors also found a significant elongation of the ERP by about 10% without a change in the MAPD70 after acute dronedarone administration.
The atrial-selective action of dronedarone is further in accord with the results gained by Manning et al. (1995a). The authors reported that acute application of dronedarone and amiodarone to anaesthetized dogs had no effects on the QT-time corrected by heart rate (QTc time) (Manning et al. 1995a). Slight prolongation of the ventricular ERP was observed in the latter study with both compounds at dosages of 2.5 mg/kg, whereas no significant effects were observed at 1 mg/kg. In contrast, significant prolongation of atrial ERP with already 1 mg/kg dronedarone was recorded, indicating that dronedarone exhibits a more pronounced effect on atrial than on ventricular ERP in anaesthetized dogs.
Effect of dronedarone on the fast Na+ channel
The PRR seen in atrial tissue could be explained by the state-dependent block of fast Na+ channels. Therefore, we studied the underlying current in isolated guinea pig cardiomyocytes. In previous studies, it was demonstrated that dronedarone inhibits the Na+ current in human cardiomyocytes (Lalevee et al. 2003), and in guinea pig papillary muscle, the compound reduced the upstroke velocity of the action potential, indicating block of the fast sodium channel (Gautier et al. 2003). While the Na+ channel-blocking ability of dronedarone is well established, the present study demonstrates that this inhibition is strongly dependent on the holding potential of the applied voltage pulse. In guinea pig cardiomyocytes, we were surprised to see that there was only a minor inhibition at the concentration of 10 μM dronedarone when the holding potential was −100 mV, whereas a pronounced inhibition (IC50 = 0.7 ± 0.1 μM) occurred at a holding potential of −80 mV. This points to a state-dependent blocking behaviour of dronedarone.
It is well known that the structurally related drug amiodarone caused a state-dependent inhibition of the fast Na+ current (Kodama et al. 1999; Mason et al. 1983; Sheldon et al. 1989). The blocking ability of amiodarone was more pronounced for channels in the inactivated state (in depolarized cells during the systolic phase) than for resting channels (during the diastolic interval). Consequently, the block of Na+ channels was accentuated in vitro at more depolarized holding potentials (Mason et al. 1984). Atrial cells possess intrinsically a more depolarized resting membrane potential than ventricular ones. For example, it was reported that the resting membrane potential in canine atria is −83 mV compared to −86 mV in canine ventricular muscle cells (Burashnikov et al. 2007). Own recordings revealed resting potentials in pig atrial myocytes of −77 ± 1 mV (n = 18) compared to −84 ± 2 mV (n = 7) in pig ventricular myocytes (Bogdan et al. 2009). Furthermore, the action potential shape of atrial cells is characterized by a slow phase 3 repolarization. This implies that during the repolarization period, atrial Na+ channels will rest in the inactivated state for a longer time than ventricular ones. The more depolarized resting membrane potentials together with the slow repolarization in atrial compared to ventricular cells may explain the atrial-selective effect of drugs binding to the inactivated state of the channel. For dronedarone, binding kinetics to the fast Na+ channels have not been reported. Because of the close structural similarity between dronedarone and amiodarone, it is likely that dronedarone also preferentially binds to the inactivated state.
In addition, differences in the inactivation characteristics or in channel composition (β-subunit) of Na+ channels of atrial and ventricular cells could also play a role in the different behaviour of these channels (Burashnikov et al. 2007).
Inhibition of Ca2+ channels
Ca2+ channel currents are frequently recorded by means of voltage pulses starting from a depolarized holding potential, in order to avoid activation of the fast Na+ channels. However, this might overestimate the efficacy of a compound if its block is state dependent. A strong dependence of Ca2+ channel inhibition on the holding potential was observed with the dihydropyridine nitrendipine (Kamp et al. 1988) and with amiodarone (Nishimura et al. 1989), where the block was more pronounced when the holding potential was depolarized. A similar observation was obtained in the present study with dronedarone, which (at 10 μM) blocked Ca2+ channel currents to 80% when the holding potential was −40 mV, whereas inhibition was only 20%, when V hold was −80 mV. This indicates that the compound binds preferentially to the inactivated state of the channel. As the Ca2+ channels undergo a complex activation and inactivation process during an action potential, we thought it to be more realistic to perform action potential clamp and to evaluate the total charge flowing through the channels (Linz and Meyer 1998a). In these recordings, the total amount of Ca2+ charge was defined by the amount which is blocked by 200 μM CdCl2. Previously, it was reported that the Cd2+-sensitive current is carried mainly via L-type Ca2+ channels (Linz and Meyer 1998b). Half-maximal inhibition of the Cd2+-sensitive current by dronedarone under action potential clamp conditions was at 0.4 ± 0.3 μM. This value complies with the one we found with rectangular pulses from V hold = −40 mV.
It should be noted that this voltage protocol does not discriminate between L-type and T-type Ca2+ channels. Whereas T-type Ca2+ channels are not activated at V hold = −40 mV, these channels are activated at negative holding potentials (−90 mV) (Mitra and Morad 1986), but the amount of current is small compared to the L-type Ca2+ channel (Sipido et al. 1998).
Inhibition of the hHCN4 channel
The HCN form a gene family consisting of four isoforms HCN1–4, which are expressed strongly in the brain and heart (Santoro and Tibbs 1999), where they are mainly responsible for pacemaker activity (for review, see Baruscotti et al. 2005). In the sinoatrial node of the heart, HCN1, HCN2 and HCN4 are expressed, with HCN4 being the major component in the pacemaker region in humans (Seifert et al. 1999). Inhibition of the pacemaker current (I f) attenuates diastolic depolarization, leading to slowing of the heart rate (DiFrancesco 1986). Pharmacologists aimed to benefit from this mechanism and developed several compounds which inhibit the channel underlying I f, in order to reduce heart rate in patients with heart failure. Ivabradine was recently shown to be beneficial in heart failure patients who have heart rates of 70 beats/min or more (Fox et al. 2008). Ivabradine was shown to inhibit the human isoform of HCN4 expressed in HEK cells with an IC50 value of 2.0 μM (Bucchi et al. 2006), and when expressed in CHO cells, an IC50 value of 0.5 μM was reported (Thollon et al. 2007). The slight variation compared to the IC50 value of 1.1 μM obtained in the present study could be due to the higher temperature and different voltage protocols in the previous studies. The present study revealed that both dronedarone and amiodarone blocked the hHCN4 channel current with IC50 values of 1.0 and 0.8 μM, respectively, similar to the potency of ivabradine. Thus, it is likely that the bradycardic effects of dronedarone (Singh et al. 2007) or amiodarone (Delle et al. 2001) in patients in sinus rhythm are at least partly due to the inhibition of the pacemaker current in the sinoatrial node (Rocchetti et al. 1998). On the other hand, as both drugs exhibit calcium antagonism and β-blockade (Gautier et al. 2004; Chatelain et al. 1995), the amount of heart rate reduction caused by inhibition of the pacemaker current I f remains elusive.
Conclusion
The present study showed a marked state-dependent inhibition of Na+ and Ca2+ currents by dronedarone, favouring a more pronounced channel block at depolarized resting membrane potentials. According to the fact that atrial cells exhibit less negative resting membrane potentials than ventricular ones, ex vivo experiments confirmed an elongation of the ERP in atria but not in ventricles. The elongation of atrial ERP by inhibition of the Na+ channels may contribute to the clinical finding that dronedarone is effective against atrial fibrillation (Singh et al. 2007).
Furthermore, clinical trials showed a significant reduction of the heart rate in patients receiving dronedarone (Singh et al. 2007). The bradycardic effect could be partly explained by the present finding that dronedarone inhibits HCN4 channels underlying the pacemaker current.
Study limitations
All investigations of the present study were performed with acute application of dronedarone. In clinical practice, however, the drug is given to patients orally over a longer period of time. There may be differences in both applications as observed, for example, in rabbit atrial preparation (Sun et al. 2002). Moreover, extrapolations of results obtained from any in vitro animal preparations to the clinic should be done with caution. The present study showed that dronedarone exerts a marked state-dependent block of Na+ channels and, therefore, blocks Na+ channels in atrial tissue more effectively than in ventricles. However, diseased atria of patients may respond differently than those of healthy animals. For example, PRR was not observed after cardioversion of persistent atrial fibrillation in patients treated with amiodarone (Pandozi et al. 2003), which is in contrast to the effects observed with chronic amiodarone in the canine wedge preparation (Burashnikov et al. 2008).
References
Baruscotti M, Bucchi A, DiFrancesco D (2005) Physiology and pharmacology of the cardiac pacemaker ("funny") current. Pharmacol Ther 107:59–79
Bogdan R, Goegelein H, Ruetten H (2009) Viable heart slices: action potential recordings from atrial and ventricular tissues. Acta Physiol 195(suppl 669):64
Bucchi A, Tognati A, Milanesi R, Baruscotti M, DiFrancesco D (2006) Properties of ivabradine-induced block of HCN1 and HCN4 pacemaker channels. J Physiol 572:335–346
Burashnikov A, Antzelevitch C (2009) Atrial-selective sodium channel block for the treatment of atrial fibrillation. Expert Opin Emerg Drugs 14:233–249
Burashnikov A, Di Diego JM, Zygmunt AC, Belardinelli L, Antzelevitch C (2007) Atrium-selective sodium channel block as a strategy for suppression of atrial fibrillation: differences in sodium channel inactivation between atria and ventricles and the role of ranolazine. Circulation 116:1449–1457
Burashnikov A, Di Diego JM, Sicouri S, Ferreiro M, Carlsson L, Antzelevitch C (2008) Atrial-selective effects of chronic amiodarone in the management of atrial fibrillation. Heart Rhythm 5:1735–1742
Burashnikov A, Belardinelli L, Antzelevitch C (2010) Acute dronedarone is inferior to amiodarone in terminating and preventing atrial fibrillation in canine atria. Heart Rhythm 7:1273–1279
Celestino D, Medei E, Moro S, Elizari MV, Sicouri S (2007) Acute in vitro effects of dronedarone, an iodine-free derivative, and amiodarone, on the rabbit sinoatrial node automaticity: a comparative study. J Cardiovasc Pharmacol Ther 12:248–257
Chatelain P, Meysmans L, Matteazzi JR, Beaufort P, Clinet M (1995) Interaction of the antiarrhythmic agents SR 33589 and amiodarone with the beta-adrenoceptor and adenylate cyclase in rat heart. Br J Pharmacol 116:1949–1956
Close B et al (1997) Recommendation for euthanasia of experimental animals. Part 2. Lab Anim 31:1–32
Delle KG, Geppert A, Neunteufl T, Priglinger U, Haumer M, Gschwandtner M, Siostrzonek P, Heinz G (2001) Amiodarone versus diltiazem for rate control in critically ill patients with atrial tachyarrhythmias. Crit Care Med 29:1149–1153
DiFrancesco D (1986) Characterization of single pacemaker channels in cardiac sino-atrial node cells. Nature 324:470–473
DiFrancesco D (2006) Funny channels in the control of cardiac rhythm and mode of action of selective blockers. Pharmacol Res 53:399–406
Doggrell SA, Hancox JC (2004) Dronedarone: an amiodarone analogue. Expert Opin Investig Drugs 13:415–426
Finance O, Manning A, Chatelain P (1995) Effects of a new amiodarone-like agent, SR 33589, in comparison to amiodarone, d, l-sotalol, and lignocaine, on ischemia-induced ventricular arrhythmias in anesthetized pigs. J Cardiovasc Pharmacol 26:570–576
Fox K, Ford I, Steg PG, Tendera M, Ferrari R (2008) Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a randomised, double-blind, placebo-controlled trial. Lancet 372:807–816
Gautier P, Guillemare E, Marion A, Bertrand JP, Tourneur Y, Nisato D (2003) Electrophysiologic characterization of dronedarone in guinea pig ventricular cells. J Cardiovasc Pharmacol 41:191–202
Gautier P, Guillemare E, Djandjighian L, Marion A, Planchenault J, Bernhart C, Herbert JM, Nisato D (2004) In vivo and in vitro characterization of the novel antiarrhythmic agent SSR149744C: electrophysiological, anti-adrenergic, and anti-angiotensin II effects. J Cardiovasc Pharmacol 44:244–257
Hohnloser SH, Crijns HJ, EM Van, Gaudin C, Page RL, Torp-Pedersen C, Connolly SJ (2009) Effect of dronedarone on cardiovascular events in atrial fibrillation. N Engl J Med 360:668–678
Kamp TJ, Sanguinetti MC, Miller RJ (1988) Voltage-dependent binding of dihydropyridine calcium channel blockers to guinea pig ventricular myocytes. J Pharmacol Exp Ther 247:1240–1247
Kodama I, Kamiya K, Toyama J (1999) Amiodarone: ionic and cellular mechanisms of action of the most promising class III agent. Am J Cardiol 84:20R–28R
Lalevee N, Nargeot J, Barrere-Lemaire S, Gautier P, Richard S (2003) Effects of amiodarone and dronedarone on voltage-dependent sodium current in human cardiomyocytes. J Cardiovasc Electrophysiol 14:885–890
Linz KW, Meyer R (1998a) Control of L-type calcium current during the action potential of guinea-pig ventricular myocytes. J Physiol 513(Pt 2):425–442
Linz KW, Meyer R (1998b) The late component of L-type calcium current during guinea-pig cardiac action potentials and its contribution to contraction. Pflugers Arch 436:679–688
Manning A, Thisse V, Hodeige D, Richard J, Heyndrickx JP, Chatelain P (1995a) SR 33589, a new amiodarone-like antiarrhythmic agent: electrophysiological effects in anesthetized dogs. J Cardiovasc Pharmacol 25:252–261
Manning AS, Bruyninckx C, Ramboux J, Chatelain P (1995b) SR 33589, a new amiodarone-like agent: effect on ischemia- and reperfusion-induced arrhythmias in anesthetized rats. J Cardiovasc Pharmacol 26:453–461
Mason JW, Hondeghem LM, Katzung BG (1983) Amiodarone blocks inactivated cardiac sodium channels. Pflugers Arch 396:79–81
Mason JW, Hondeghem LM, Katzung BG (1984) Block of inactivated sodium channels and of depolarization-induced automaticity in guinea pig papillary muscle by amiodarone. Circ Res 55:278–285
Mitra R, Morad M (1986) Two types of calcium channels in guinea pig ventricular myocytes. Proc Natl Acad Sci USA 83:5340–5344
Nishimura M, Follmer CH, Singer DH (1989) Amiodarone blocks calcium current in single guinea pig ventricular myocytes. J Pharmacol Exp Ther 251:650–659
Pandozi C, Gentilucci G, Calo L, Castro A, Lamberti F, Loricchio ML, Santini L, Magris B, Bulava A, Peichl P, Santini M (2003) Relations between monophasic action potential duration and refractoriness after cardioversion of persistent atrial fibrillation: results in wash-out and amiodarone-treated patients. Ital Heart J 4:257–263
Rocchetti M, Bertrand JP, Nisato D, Gautier P (1998) Cellular electrophysiological study of dronedarone, a new amiodarone-like agent, in guinea pig sinoatrial node. Naunyn-Schmiedeberg’s Arch Pharmacol 358(suppl 2):R617
Santoro B, Tibbs GR (1999) The HCN gene family: molecular basis of the hyperpolarization-activated pacemaker channels. Ann NY Acad Sci 868:741–764
Seifert R, Scholten A, Gauss R, Mincheva A, Lichter P, Kaupp UB (1999) Molecular characterization of a slowly gating human hyperpolarization-activated channel predominantly expressed in thalamus, heart, and testis. Proc Natl Acad Sci USA 96:9391–9396
Sheldon RS, Hill RJ, Cannon NJ, Duff HJ (1989) Amiodarone: biochemical evidence for binding to a receptor for class I drugs associated with the rat cardiac sodium channel. Circ Res 65:477–482
Singh BN, Connolly SJ, Crijns HJ, Roy D, Kowey PR, Capucci A, Radzik D, Aliot EM, Hohnloser SH (2007) Dronedarone for maintenance of sinus rhythm in atrial fibrillation or flutter. N Engl J Med 357:987–999
Sipido KR, Carmeliet E, Van de Werf F (1998) T-type Ca2+ current as a trigger for Ca2+ release from the sarcoplasmic reticulum in guinea-pig ventricular myocytes. J Physiol 508(Pt 2):439–451
Sun W, Sarma JS, Singh BN (2002) Chronic and acute effects of dronedarone on the action potential of rabbit atrial muscle preparations: comparison with amiodarone. J Cardiovasc Pharmacol 39:677–684
Thollon C, Bedut S, Villeneuve N, Coge F, Piffard L, Guillaumin JP, Brunel-Jacquemin C, Chomarat P, Boutin JA, Peglion JL, Vilaine JP (2007) Use-dependent inhibition of hHCN4 by ivabradine and relationship with reduction in pacemaker activity. Br J Pharmacol 150:37–46
Varro A, Takacs J, Nemeth M, Hala O, Virag L, Iost N, Balati B, Agoston M, Vereckei A, Pastor G, Delbruyere M, Gautier P, Nisato D, Papp JG (2001) Electrophysiological effects of dronedarone (SR 33589), a noniodinated amiodarone derivative in the canine heart: comparison with amiodarone. Br J Pharmacol 133:625–634
Yan GX, Antzelevitch C (1996) Cellular basis for the electrocardiographic J wave. Circulation 93:372–379
Acknowledgements
We acknowledge the skillful assistance of Ms. Karin Kopp and Mr. Roland Klein in performing the experiments.
Conflict of interest
All authors are employees of Sanofi-Aventis Germany GmbH.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bogdan, R., Goegelein, H. & Ruetten, H. Effect of dronedarone on Na+, Ca2+ and HCN channels. Naunyn-Schmied Arch Pharmacol 383, 347–356 (2011). https://doi.org/10.1007/s00210-011-0599-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00210-011-0599-9