
Abstract
Cyclophosphamide (CP) is widely used, alone or in combination with other chemotherapeutic agents, for treatment of neoplastic diseases. Its urotoxicity may cause dose-limiting side-effects, for example hemorrhagic cystitis. The agent most often used to prevent this side-effect is mesna (2-mercaptoethane sulfonate). Overproduction of reactive oxygen species during inflammation is one reason for possible urothelial injury. The aim of this study was to evaluate whether combinations of quercetin and epigallocatechin 3-gallate (EGCG), flavonoid antioxidants and mesna could prevent cystitis induced by cyclophosphamide, better than mesna alone. A total of 38 male Sprague–Dawley rats were divided into five groups. Four groups received single dose of CP (100 mg kg−1) intraperitoneally at the same time. Group 2 received CP only, group 3 received mesna (3×21.5 mg kg−1), group 4 received a single dose of mesna+EGCG (2×20 mg kg−1), and group 5 received a single dose of mesna+quercetin (2×20 mg kg−1), before and after CP injection. Group 1 (not treated) served as control. CP injection alone resulted in severe cystitis. Mesna resulted in some, but not full, protection against CP toxicity. Quercetin and catechine, together with mesna, resulted in full protection against CP toxicity, on the basis of histopathology of the urinary bladder. It was concluded that oxidants might be important in the pathogenesis of CP-induced cystitis, and that flavonoid antioxidants, used in addition to mesna, may help to ameliorate bladder damage.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cyclophosphamide (CP) is used, alone or in combination with other drugs, for treatment of neoplastic diseases (Levine and Richie 1989). Hemorrhagic cystitis (HC) is a major dose-limiting side-effect of CP (West 1997). The incidence of this side-effect is related to dosage and can be as high as 75% in patients receiving a high intravenous CP dose. The urological side-effects vary from transient irritative voiding symptoms, including urinary frequency, dysuria, urgency, suprapubic discomfort, and stangury with microhematuria, to life-threatening HC (Gray et al. 1986). Bladder fibrosis, necrosis, contracture, and vesicoureteral reflux and a 4% mortality rate among patients with massive bladder hemorrhage have also been reported (Levine and Richie 1989; West 1997). The urotoxicity of these nitrogen mustard group cytostatics is not based on direct alkylating activity but on the formation of renally excreted 4-hydroxy metabolites, in particular acrolein (Kurovski and Wagner 1997).
Mesna contains a sulfhydryl compound that binds acrolein within the urinary tract and detoxifies it; the resulting inert thioether does not induce damage to the uroepithelium (Goren et al. 1997; Kurovski and Wagner 1997). Although mesna has been widely used as an agent against CP-induced cystitis, significant HC, defined as an episode of symptomatic (burning, frequency, and dysuria), microscopic, or macroscopic hematuria, has been encountered clinically (West 1997).
It has recently been shown that increasing nitric oxide (NO) production is involved in the detrimental effects of CP on the bladder (Korkmaz et al. 2003; Oter et al. 2004; Ribeiro et al. 2002). This toxicity is probably related to reactive nitrogen species (RNS), in particular a peroxynitrite (ONOO−), overproduction by reaction of NO with superoxide (O .−2 ) which is associated with inflammation (Szabo 1996). The overproduction of reactive oxygen species (ROS) and RNS during inflammation leads to considerable oxidant stress, cellular injury, and necrosis via several mechanisms including peroxidation of membrane lipids, protein denaturation, and DNA damage (Virag et al. 2003).
The antioxidative defense system includes enzymes such as superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) (Mates et al. 1999), and non-enzyme antioxidants, for example carotenoids (Cuzzocrea and Reiter 2001) and flavonoids (Pietta 2000). These agents are key elements in reducing molecular damage by reactive oxygen and nitrogen species, and there is extensive literature describing these actions.
Because detoxifying acrolein with mesna does not remove HC symptoms completely, and NO has been shown to be involved in the pathogenesis, CP-induced HC is probably not only because of direct contact of acrolein with the bladder mucosa but also related to increased ROS and RNS production. In this study we examined whether flavonoid antioxidants together with mesna give better results than mesna alone in preventing CP-induced bladder damage.
Materials and methods
Animals
A total of 38 male Sprague–Dawley rats weighing 190–220 g were divided into five groups by randomization. Animals were given food and water ad libitum.
The drug administration schedule is presented in Table 1.
Experimental induction of HC
The animals were given a urotoxic dose of 100 mg kg−1 CP (Sigma–Aldrich, Taufkirchen, Germany; C0768) in 2 mL saline. Group 1 animals were injected with the same amount of saline, as controls.
Mesna and antioxidant administration
Mesna (Sigma–Aldrich; M1511; 21.5 mg kg−1) was administered 20 min before CP injection, and continued every 4 h for a total of three doses (total dose 64.5 mg kg−1). In groups 4 and 5, epigallocatechin 3-gallate (EGCG) (Cayman, Ann Arbor, MI, USA; 70935) and quercetin (Sigma–Aldrich; Q0125), were given instead of two doses of mesna (2×20 mg kg−1 for both). All drug administration was performed intraperitoneally (i.p.) as shown in Table 1.
Tissue preparation
After 24 h of cystitis induction, rats were sacrificed using high-dose i.p. injection of ketamine hydrochloride (85 mg kg−1) and xylazine hydrochloride (12.5 mg kg−1) to prevent inadvertent bladder puncture. The bladders were removed intact, evacuated of residual urine, cleaned to remove connective and lipoid tissue from around the wall, and weighed to determine if edema was present. The bladders were then cut into two equal pieces from the dome to the bottom. One-half was stored at −80°C to measure bladder malondialdehyde (MDA); the rest was fixed for 24 h in 10% buffered formaldehyde. Tissues were embedded in paraffin and at least four cross-sections 4–5 μm thick were taken from each bladder and stained with hematoxylin–eosin. Histopatological examination was performed by a pathologist and a histologist in single blind fashion and scored for edema, hemorrhage, and inflammation on a scale of 0 (normal) to 4 (severe changes). Mucosal ulceration was scored as 0 (normal), 1 (epithelial denuding), 2 (focal ulceration), 3 (widespread epithelial ulceration) and 4 (submucosal ulceration). Bladder MDA was measured as described elsewhere (Topal et al. 2004).
Definitions of hematuria
Hematuria was graded on a scale of 0–3 by performing dip-stick analysis in the urine specimens obtained by abdominal massage 6, 12 and 24 h after CP injection.
Statistics
The results are expressed as the median (min–max) and P<0.05 was assessed as statistically significant. All of the numeric data were analyzed first by using the nonparametric Kruskal–Wallis test to discover whether there was any difference between groups. The Mann-Whitney U-test was then performed to analyze two groups consecutively.
Results
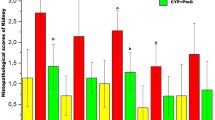
The control animals had cytologically normal bladders with assigned scores of 0 for all four conditions edema, hemorrhage, inflammation, and ulceration. Severe histologic changes and higher grades of hematuria were observed for animals receiving CP (group 2) and severe ulceration and erosion was encountered in four of the seven bladders, as shown in Fig. 1. No ulceration was observed in any other slides.

Histological picture of representative bladder walls in cross section. Saline, normal bladder; CP, meaningful edema, leukocyte infiltration, hemorrhage and severe epithelial ulceration (H&E, ×100); MMM, significant protection against inflammation and ulceration damage (P<0.05 vs. CP); meaningful edema and hemorrhage are easily seen in this group (P>0.05 vs. CP); MQQ and MCC, significantly different from CP group for all conditions (H&E, ×100 for both); note that slight edema and hemorrhage are present in these treatment groups; there are no significant histological differences between MQQ and MCC. (E epithelial cell layer; L lumen; U ulceration. CP cyclophosphamide, MMM 3×mesna, MQQ 1×mesna+2×quercetin, MCC 1×mesna+2×EGCG)
In the treatment group that received mesna only, statistically significant protection against inflammation and ulceration was observed, as shown in Table 2 (P<0.05 vs. group 2). Edema and hemorrhage histologic damage was present (P>0.05 vs. group 2) (Fig. 1).
Addition of quercetin and EGCG resulted in protection when given with mesna. Moreover, increased MDA levels in the CP group were significantly reduced by all treatments (Fig. 2). Nevertheless, flavonoid antioxidants reduced MDA almost to control levels (P<0.05 for groups 4 and 5 vs. CP, P>0.05 for group 3 vs. CP).

MDA levels in bladder tissue [median (min−max)]: control [0.2 (0.09−0.37)], CP [0.85 (0.69−0.97)], MMM [0.48 (0.39−0.68)], MQQ [0.32 (0.23−0.4)], MCC [0.26 (0.14−0.4)]. CP administration severely increased MDA and flavonoids reduced MDA significantly to nearly saline level (P<0.05 for MQQ and MCC vs. CP). Mesna also reduced MDA levels but not statistically significantly (P>0.05 vs. CP). (CP cyclophosphamide, MMM 3×mesna, MQQ 1×mesna+2×quercetin, MCC 1×mesna+2×EGCG)
Macroscopic hematuria continued in the CP group and almost disappeared in the treatment groups especially in the mesna alone and the mesna+EGCG groups.
Discussion
Cyclophosphamide, an antineoplastic alkylating agent, is used to treat neoplastic, immune-mediated, and transplant-related diseases; HC is a major therapy-limiting side-effect of CP. The main features of HC are urothelial damage, transmural edema, hemorrhage, mucosal ulceration, and epithelial necrosis. These can be demonstrated within 24 h of a single dose (Gray et al. 1986; Table 2, Fig. 1).
Hemorrhagic cystitis is now accepted as non-microbial inflammation and the pathogenesis of HC may be summarized as cytokine production leading to iNOS induction. There is evidence that urinary bladder epithelial cells express reactivity to iNOS in the cytoplasm, leading to peroxynitrite production (Ribeiro et al. 2002). Increased NO production is probably responsible for the cystitis, because S-methylisothiourea (an iNOS-selective inhibitor) almost abolishes CP-induced bladder damage (Szabo 1996; Cuzzocrea and Reiter 2001). This improvement is thought to result from a decrease in NO production. Nevertheless, in a recent study antioxidants exerted protective effects on CP-induced bladder damage when combined with mesna (Yildirim et al. 2004). In recent studies ternatin, a flavonoid (Vieira et al. 2004), and berberine, an alkaloid (Xu and Malave 2001), were demonstrated to have preventive effects against CP-induced hemorrhagic cystitis.
Flavonoids, which are available in common fruits and vegetables, inhibit enzymes responsible for superoxide anion production, for example xanthine oxidase (Hanasaki et al. 1994) and protein kinase C (Ursini et al. 1994). Flavonoids have also been shown to inhibit cyclooxygenase, lipoxygenase, microsomal monooxygenase, glutathione S-transferase, mitochondrial succinoxidase, and NADH oxidase, all involved in the generation of reactive oxygen species (Brown et al. 1998). Beneficial effects of flavonoids appear in various experimental models of inflammation (Rotelli et al. 2003).
In this work MDA levels and histopatologic examination showed that EGCG and quercetin had antioxidant properties. The reason of this may be because it is not only an antioxidant but also a peroxynitrite scavenger (Yokozawa et al. 2004).
In essence, the results of this study suggest that flavonoid antioxidants may help to ameliorate CP-induced cystitis when combined with mesna. Moreover, a variety of substances derived from edible plants have also been shown to have anti-inflammatory, anti-mutagenic, and anti-cancer properties (Park and Surh 2004). During CP treatment patients may be encouraged to consume more fruit and vegetables rich in flavonoids, for example cranberry, apple, grape, strawberry, peach, lemons, etc. (Boyer and Liu 2004).
References
Boyer J, Liu RH (2004) Apple phytochemicals and their health benefits. Nutrition J 3:5
Brown JE, Khodr H, Hider RC, Rice-Evans C (1998) Structural dependence of flavonoid interactions with Cu2+ ions: implications for their antioxidant properties. Biochem J 330:1173–1178
Cuzzocrea S, Reiter RJ (2001) Pharmacological action of melatonin in shock, inflammation, and ischemia/reperfusion injury. Eur J Pharmacol 426:1–10
Goren MP, McKenna LM, Goodman TL (1997) Combined intravenous and oral mesna in outpatients treated with ifosfamide. Cancer Chemother Pharmacol 40:371–375
Gray KJ, Engelmann UH, Johnson EH, Fishman IJ (1986) Evaluation of misoprostol cytoprotection of the bladder with cyclophosphamide (cytoxan) therapy. J Urol 133:497–500
Hanasaki Y, Ogawa S, Fukui S (1994) The correlation between active oxygens scavenging and antioxidative effects of flavonoids. Free Radic Biol Med 16:845–850
Korkmaz A, Oter S, Deveci S, Ozgurtas T, Topal T, Sadir S, Bilgic H (2003) Involvement of nitric oxide and hyperbaric oxygen in the pathogenesis of cyclophosphamide induced hemorrhagic cystitis in rats. J Urol 170:2498–2502
Kurovski V, Wagner T (1997) Urinary excretion of ifosfamide, 4-hydroxyfosfamide, 3- and 2-dechloroethylifosfamide, mesna, and dimesna in patients on fractionated intravenous ifosfamide and concomitant mesna therapy. Cancer Chemother Pharmacol 39:431–439
Levine AL, Richie PJ (1989) Urological complications of cyclophosphamide. J Urol 141:1063–1069
Mates JM, Perez-Gomez P, Nunez de Castro I (1999) Antioxidant enzymes and human disease. Clin Biochem 32:595–603
Oter S, Korkmaz A, Oztas E, Yildirim I, Topal T, Bilgic H (2004) Inducible nitric oxide synthase inhibition in cyclophosphamide induced hemorrhagic cystitis in rats. Urol Res 32:185–189
Park OJ, Surh YJ (2004) Chemopreventative potential of epigallocatechin gallate and genistein: evidence from epidemiological and laboratory studies. Toxicol Lett 150:43–56
Pietta PG (2000) Flavonoids as antioxidants. J Nat Prod 63:1035–1042
Ribeiro RA, Feritas HC, Campos MC, Santos CC, Figueiredo FC, Brito GA, Cunha FQ (2002) Tumor necrosis factor-α and interleukin-1β mediate the production of nitric oxide involved in the pathogenesis of ifosfamide induced hemorrhagic cystitis in mice. J Urol 67:2229–2234
Rotelli AE, Guardia T, Juàrez AO, de la Rocha NE, Pelzer LE (2003) Comparative study of flavonoids in experimental models of inflammation. Pharmacol Res 48:601–606
Szabo C (1996) The pathophysiological role of peroxynitrite in shock, inflammation, and ischemia-reperfusion injury. Shock 6:79–88
Topal T, Oter S, Korkmaz A, Sadir S, Metinyurt G, Korkmazhan ET, Serdar MA, Bilgic H, Reiter RJ (2004) Exogenously administered and endogenously produced melatonin reduce hyperbaric oxygen-induced oxidative stress in rat lung. Life Sci 75:461–467
Ursini F, Maiorino M, Morazzoni P, Roveri A, Pifferi G (1994) A novel antioxidant flavonoid (IdB 1031) affecting molecular mechanisms of cellular activation. Free Radic Biol Med 16:547–553
Vieira MM, Macedo FY, Filho JN, Costa AC, Cunha AN, Silveira ER, Brito GA, Ribeiro RA (2004) Ternatin, a flavonoid, prevents cyclophosphamide and ifosfamide-induced hemorrhagic cystitis in rats. Phytother Res 18:135–141
Virag L, Szabo E, Gergely P, Szabo C (2003) Peroxynitrite-induced cytotoxicity: mechanism and opportunities for intervention. Toxicol Let 141:113–124
West NJ (1997) Prevention and treatment of hemorrhagic cystitis. Pharmacother 17(4):696–706
Xu X, Malave A (2001) Protective effect of berberine on cyclophosphamide-induced haemorrhagic cystitis in rats. Pharmacol Toxicol 88:232–237
Yildirim I, Korkmaz A, Oter S, Ozcan A, Oztas E (2004). Contribution of antioxidants to preventive effect of mesna in cyclophosphamide-induced hemorrhagic cystitis in rats. Cancer Chemother Pharmacol 54(5):469–473
Yokozawa T, Rhyu DY, Cho EJ (2004) (−)-Epicatechin 3-O-gallate ameliorates the damages related to peroxynitrite production by mechanisms distinct from those of other free radical inhibitors. J Pharm Pharmacol 56(2):231–239
Acknowledgements
The “Gulhane Military Medical Academy Animal Care and Use Committee” approved the experimental procedures. All animals received care according to the criteria outlined in the “Guide for the Care and Use of Laboratory Animals” of the National Academy of Sciences and the National Institutes of Health. The experiments comply with current national laws.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ozcan, A., Korkmaz, A., Oter, S. et al. Contribution of flavonoid antioxidants to the preventive effect of mesna in cyclophosphamide-induced cystitis in rats. Arch Toxicol 79, 461–465 (2005). https://doi.org/10.1007/s00204-005-0647-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00204-005-0647-7