
Abstract
Summary
In 50–79-year-olds who participated in the Tromsø Study (1994–1995), the risk of non-vertebral osteoporotic fractures during 15 years follow-up increased by 22% in men and 9% in women per 1 SD lower grip strength. The strongest association was observed in men aged 50–64 years.
Introduction
We aimed to explore whether low grip strength was associated with increased risk of non-vertebral osteoporotic fracture in the population-based Tromsø Study 1994–1995.
Methods
Grip strength (bar) was measured by a Martin Vigorimeter and fractures were retrieved from the X-ray archives at the University Hospital of North Norway between 1994 and 2010. At baseline, weight and height were measured, whereas information on the other covariates were obtained through self-reported questionnaires. Cox regression was used to estimate the hazard ratio (HR) of fracture in age- and gender-specific quintiles of grip-strength, and per 1 SD lower grip strength. Similar analyses were done solely for hip fractures. Adjustments were made for age, height, body mass index (BMI), marital status, education, smoking, physical activity, use of alcohol, self-perceived health, and self-reported diseases.
Results
In 2891 men and 4002 women aged 50–79 years, 1099 non-vertebral osteoporotic fractures—including 393 hip fractures—were sustained during the median 15 years follow-up. Risk of non-vertebral osteoporotic fracture increased with declining grip strength: hazard ratios per SD decline was 1.22 (95% CI 1.05–1.43) in men and 1.09 (95% CI 1.01–1.18) in women. HR for fracture in lower vs. upper quintile was 1.58 (95% CI 1.02–2.45) in men and 1.28 (95% CI 1.03–1.59) in women. The association was most pronounced in men aged 50–64 years with HR = 3.39 (95% CI 1.76–6.53) in the lower compared to the upper quintile.
Conclusions
The risk of non-vertebral osteoporotic fracture increased with declining grip-strength in both genders, particularly in men aged 50–64 years.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Norway has the world’s highest hip and forearm fracture incidence rates [1, 2]. In spite of a reported decline in the age-specific incidence of hip fractures in Norway [3] and other Western countries in the last decades [2, 4], the future burden of hip fractures is expected to increase due to aging populations [5, 6]. The consequences for the society and the impacted individuals are significant, entailing pain and suffering, loss of function and quality of life, and reduced life expectancy [6,7,8].
The causes of osteoporotic fractures are multifactorial. Osteoporosis [9] and falls [10] are important risk factors. However, less than half of the fractures occur in patients with bone mineral density (BMD) in the osteoporotic range (T-score < − 2.5) [11], so relying on BMD screening only will not be sufficient for prediction of future fracture [12].
As neuromuscular strength and control are associated with several of the shared risk factors for osteoporosis and falls, i.e., age, physical activity, and alcohol use, we wanted to explore a simple physical measure like grip strength and its association with fracture. Handgrip strength is a powerful predictor of disability, morbidity, and mortality [13,14,15,16,17]. We have reported a strong inverse relation between handgrip strength and mortality in the Tromsø Study [18].
Although grip strength cannot be assumed a strong proxy for overall muscle strength [19], it might be an indicator of frailty and thus a predictor of fall-risk [20, 21]. Poor grip strength has also been suggested as one of the primary indicators of sarcopenia in the updated frailty definition [22].
In a review, comprising six case-control and five cohort studies published 1992–2014, Denk et al. [17] reported that all the studies described some evidence for a relationship between handgrip strength and hip fracture incidence. The largest of the included case-control studies (246 fractures) [23] found a linear increased risk through decreasing quartiles, and an adjusted odds ratio of 3.27 (95% CI 1.54–6.97), ptrend = 0.0005, for the lowest vs the highest quartile. However, the extensive PURE study [14] based on data from 17 different countries, not included in the review, did not find any increased risk of fracture with decreasing grip strength. On the other hand, the Osteoporotic Fractures in Men (MrOS) Study reported an association between increased grip strength and lower risk of both osteoporotic and hip fracture [24]. Few if any other studies have investigated the relationship between grip strength and fractures other than at the hip. Thus, evidence on grip strength and overall fracture risk are sparse and disparate, and potential differences between men and women have not been systematically or thoroughly investigated.
The aim of the present study was to explore whether lower handgrip strength was associated with a higher risk of non-vertebral osteoporotic fracture during 15 years follow-up.
Methods
Study population
The Tromsø Study is a longitudinal population-based multi-purpose study focusing on lifestyle-related diseases, risk factors, quality of life, and use of drugs (www.tromsostudy.com). The study was initiated in 1974 inviting all inhabitants of the municipality of Tromsø in predefined age groups to survey and questionnaires [25]. The study has been repeated seven times, the last one in 2015/2016—each time inviting earlier participants as well as recruiting new ones. In the current analysis, we have used baseline data from the fourth wave (Tromsø 4) in 1994–1995, inviting all individuals aged 25 years or older living in Tromsø (n = 37,558) to the first phase of the study, of whom 27,158 participated (72%) [25]. All men aged 55–74 years, all women aged 50–74 years, and a random sample of 5–10% of the remaining age groups between 25 and 84 years (n = 10,542 in total) were preselected to undergo more extensive phase II examinations including measurement of grip strength, with a final participation rate of 75% [18]. The current study includes all participants in the second phase aged 50–79 years (at the time of screening) with valid measure of grip strength, and with measured height and weight from the first phase—i.e., 2891 men and 4002 women (99.3% of all phase II participants aged 50–79 years). Participants outside this age range were not included because of few osteoporotic fractures below age 50, and very few participants 80 years or above in phase II (n = 20).
Grip strength and all covariates were measured only in 1994-1995.
Baseline measurements and questionnaires
Height (cm) and weight (kg) were measured with participants wearing light clothing and no shoes, and body mass index (BMI) in kilogram per square meter was constructed. Each participant filled in two self-administered questionnaires. The first one-page questionnaire was enclosed with the invitation and contained some key subjects about diseases and risk factors, such as smoking habits, self-perceived health, and physical activity. The second questionnaire (separate for people aged < 70 and those aged > 70 years), was handed out at the survey station, filled in at home and returned by mail in a pre-addressed stamped envelope. This four-page questionnaire covered much of the same topics like sociodemographic factors, diseases and symptoms, use of medication, and lifestyle factors. About 90% of the participants responded to the second questionnaire [25].
Bisphosphonates or any other anti-osteoporosis drugs (except estrogen) were not on the market in Norway at the time of the baseline examination.
Measurement of grip strength—exposure variable
Grip strength (in bar units) of the non-dominant hand was measured using a Martin Vigorimeter [26]. All assessments were done by trained health professionals using a standardized protocol [18, 27]. The Martin Vigorimeter comes with three balloon sizes, and we used the largest and medium-sized balloons for men and women, respectively. Each participant was allowed two attempts, and the highest score registered was recorded and used in analyses [18, 27].
Fracture registration—outcome variables
All non-vertebral fractures were registered from the X-ray archives of the University Hospital of North Norway in Tromsø, Norway [28]. The nearest alternative radiographic service or fracture treatment facility is located 250 km from Tromsø. Fractures that would be missed were fractures occurring while inhabitants were traveling with no control X-ray after returning home, in addition to fractures not radiographically examined. The computerized records in the radiographic archives contain the national personal identification number, date of the fracture, fracture codes, and descriptions. All abnormally coded radiographic examinations on participants in the Tromsø 4 survey were reviewed. In addition, the discharge records were reviewed with respect to hip fractures. The validation of the fracture registration has been reported [29]. Our analyses of non-vertebral osteoporotic fractures include fractures of the distal forearm (distal radius, distal ulna), hip (femoral neck, trochanter), pelvis, and proximal humerus. This will henceforth be referred to as “osteoporotic fractures.” We also performed separate analyses with hip fracture as outcome. Each individual’s first fracture (osteoporotic fracture or hip fracture, respectively) after baseline measurement of grip strength was included in the presented analyses. For the analyses of osteoporotic fractures, all individuals with an osteoporotic fracture before baseline were excluded. Correspondingly, for the analyses of hip fractures, individuals with a hip fracture before baseline measurement of grip strength were excluded. Because 14 fewer individuals had sustained a hip fracture than an osteoporotic fracture before baseline, the total sample sizes in Tables 2 and 3 differ slightly.
Covariates
Covariates reported to be associated with grip strength or osteoporotic fractures were selected a priori for inclusion as possible confounders. Age, height (cm), and BMI were used as continuous variables in gender-specific analyses. Marital status was dichotomized into single (never married/divorced/separated/widowed) vs. married/registered partner based on previous findings of single men as a vulnerable group [30]. Information about age, gender, and marital status was obtained from Statistics Norway. All other baseline variables obtained from questionnaires were categorized with missing information included as a separate category. Years of education had five levels ranging from 7 to 10 years in school to 4 or more years at college/university. Two questions about light physical activity (not sweating or out of breath) and strenuous physical activity (sweating or out of breath) in leisure time had four response categories ranging from none (score 1) to 3 h or more per week (score 4). The answers to these two questions were summed up (resulting score 1–8), and then grouped in four physical activity levels—the lowest group with score 1–3 and the highest with 6–8. The frequency of alcohol consumption was assessed by asking whether or not the respondents were teetotaller and how many times a month the consumers used alcohol (not counting low-alcohol beer)—from none to several times a month. These questions were combined and grouped into five categories—from never drinking alcohol to drinking more than once a week. Smoking status was used with three categories current, former, and never smokers. Self-perceived health was measured by a question with four categories from poor to very good. The participants were also asked whether they had any of the following conditions or diseases: myocardial infarction, angina pectoris, cerebral stroke/brain hemorrhage, asthma, or diabetes. Those answering yes to one or more of these questions were categorized as having a disease. The participants were asked about the regular use of a number of different drugs subsequently grouped according to ATC-codes [31]. Women were asked about use and brand name of estrogen tablets/patches (ATC-codes G03C, G03F), and the answers were dichotomized into current use vs. no use/no answer.
Statistics
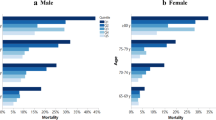
Data were analyzed in IBM SPSS Statistics for Windows (Version 24.0, Armonk, NY). Baseline data were described according to age- (50–59, 60–69, 70–79 years) and gender-specific quintiles of grip strength as previously reported [18]. In brief, we used the cut points for the quintiles in each of the three age groups for each gender and then combined these quintiles. Differences between the quintiles were tested by Pearson’s two-sided chi-squared test for categorical variables and F test (ANOVA) for continuous variables. In addition to the covariates described above, we also tested the association between quintile of grip strength and time to fracture (mean number of years) in both genders and for both fracture outcomes.
Incidence rates of fractures according to quintiles of grip strength were calculated. Cox proportional hazards regression was performed for osteoporotic and hip fractures, separately. All analyses were performed stratified by gender. Because we had a hypothesis of decreasing risk of fracture with increasing grip strength, we used the upper quintile as a reference category. For both fracture outcomes, three models with an increasing number of covariates were constructed. In the basic model (model 1), we adjusted for age, the intermediate model (model 2) additionally for height and BMI, whereas the fully adjusted model (model 3) also included marital status, level of education, physical activity, consumption of alcohol, smoking, self-perceived health, and self-reported diseases. In women, we also adjusted for use of postmenopausal hormone therapy (estrogen). In the Cox models, p values for the linear associations between grip strength quintiles and fractures were reported. Corresponding Cox analyses were performed estimating hazard ratios per age- and gender-specific standard deviation (SD) lower grip strength.
For incomplete covariates, missing values in each variable were treated as a separate category in the fully adjusted regression model (model 3). The number of participants with missing values was low: physical activity n = 10, alcohol consumption n = 28, marital status n = 2, education n = 43, smoking n = 5, self-perceived health n = 10, and one or more diseases n = 3. Overall, these constituted 1.5% of the participants with valid information on grip strength, height, and BMI. Only 219 women 50–79 years with valid information on gip strength, height, and BMI, reported current use of estrogen. Additional adjustment for this variable did not change the results and is not included in the tables.
To verify the final conclusions, complete-case analyses (without the missing categories) were also performed including all variables in model 3.
Interaction terms were entered to test whether grip strength interacted multiplicatively with age, gender, height, or BMI for each fracture type.
Log minus log curves suggested no deviation from the proportional hazards assumption for grip strength. A p value below 0.05 (two-sided test) was considered statistically significant.
Follow-up time was assigned from the date of participation in Tromsø 4 (1994–1995) to date of any first fracture, emigration, death, or end of follow-up (January 31, 2010). Information on deaths and emigration was obtained from Statistics Norway. Crude incidence rates were calculated and presented as the number of fractures per 10,000 person-years of follow-up time.
Results
Baseline characteristics
Baseline characteristics of participants by age- and gender-specific quintiles of handgrip strength are shown in Table 1. Most variables in Table 1 were associated with grip strength (p< 0.05). We observed that men and women in the two lowest grip strength quintiles had the lowest height and the lowest BMI. They also had the highest proportion of individuals who were daily smokers, had a low level of education (7–10 years), low level of physical activity, poor/not very good self-perceived health, and reported one or more diseases. No statistically significant associations were found between the quintiles of grip strength and time to fracture (results not shown in tables).
Osteoporotic fracture
A total of 231 men (8.0 %) and 868 women (21.8%) suffered an osteoporotic fracture during a median of 14.6 years follow-up. Mean age (SD) at fracture was 73.8 (7.7) years in men and 71.2 (8.4) years in women. Compared with the upper quintile of grip strength, men in the two lowest quintiles had the highest hazard ratios of any osteoporotic fracture adjusted for age, height, and BMI (Table 2, model 2). Adjusting for all covariates gave only minor changes in the risk estimates (Table 2, model 3). In women, the highest fracture risk was found in the lowest grip strength quintile in all models, and the estimates did not change with full adjustments (Table 2).
In both genders, the increased hazard ratio per 1 SD reduced grip strength was statistically significant (Table 2).
Except for age in men (p < 0.001), there was no significant interactions. Thus, we did age-stratified fully adjusted analyses for two strata of men: 50–64 years and 65–79 years. Only men aged 50–64 years had significantly increased risk of osteoporotic fracture in the lower compared with the upper grip strength quintile (HR = 3.39, 95% CI 1.76–6.53). In these men, the HR was 1.36 (95% CI 1.11–1.68) per 1 SD lower grip strength. In men 65–79 years old, the corresponding HR was 1.06 (95% CI 0.85–1.34). (Results not shown in tables).
Hip fracture
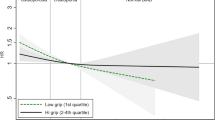
During the median follow-up of 14.7 years, 131 (4.5%) men and 262 (6.5%) women suffered a hip fracture. Mean age (SD) at hip fracture was 75.6 (7.0) and 76.2 (7.4) in men and women, respectively. Reduced grip strength was not significantly associated with hip fracture in men (p > 0.05), but women in the lowest quintile of grip strength had 51% higher risk of hip fracture compared to women in the upper quintile (Table 3, model 3). When combining the genders, participants in the lowest grip strength quintile had 34% higher risk of hip fracture than those in the upper quintile (Fig. 1, ptrend = 0.022).

Hazard ratios (HR) with 95% confidence intervals (CI) for hip fracture in quintiles of grip strength measured with Martin Vigorimeter (bar) in men and women combined aged 50–79 years. The upper quintile is reference.
None of the interaction terms tested for hip fractures were statistically significant.
Complete-case analyses for both osteoporotic and hip fracture gave similar results as those shown in Tables 2 and 3.
Discussion
In this large population-based study from Tromsø, Norway, low grip strength was associated with higher rates of osteoporotic fractures in both men and women. The association was strongest in men 50–64 years. Low grip strength was also associated with higher rates of hip fracture in women.
Comparison with existing studies
Our main findings regarding hip fracture correspond with the conclusions of the systematic review by Denk et al. [17]. However, none of the original studies’ primary objectives was to assess the relationship between handgrip strength and hip fracture risk. Because the studies were not comparable with regard to design, analyses, population, primary objectives, and dynamometer brand, the review authors did not comment on the strength of the relationship. In one of the original papers included in the review, the magnitude of the association between grip strength and hip fracture was comparable with our results for HR per 1 SD [32], whereas the HR in the Norwegian case-control study [23] had much higher OR for the lowest vs. the highest quartile. The participants in the study were, however, about 10 years older compared to the mean age in our study, and the researchers used quartiles not quintiles.
As already mentioned, the PURE study with data from 17 different countries [14] did not report any associations between grip strength and fractures. However, they did not present the types of fractures included, the number of fractures, or any gender-specific analyses. Moreover, the age-distribution was 35–70 years with a median age 50 years, whereas about 50% of hip fractures in Norway occur after passing 80 years [3]. The authors report, however, that case-fatality from fractures was higher in individuals with low grip strength measured before the fracture [14], implying that low muscle strength may predispose to a fatal outcome when sustaining a fracture.
In men, we found an inverse association between grip strength and osteoporotic fracture, and most pronounced in men aged 50–64 years. It is interesting to notice that men aged 50–59 years—not older men, drinking frequently or consuming high quanta of alcohol had increased risk of hip fracture in Cohort of Norway [33]. A post hoc analysis in our data of the association between grip-strength and hip fracture in men aged 50–64 years, revealed a significantly increased hazard ratio with lower grip strength (HR = 1.35, 95% CI 1.00–1.83 per 1 SD in grip strength).
In a paper from the MrOS study (men aged > 65 years) published in 2008, no association was reported between grip strength and hip fractures [34], whereas more recent results with updated fracture follow-up showed statistically significant inverse associations between grip strength and both osteoporotic and hip fractures [24]. The HR estimates for osteoporotic fractures in MrOs per 1 SD reduced grip strength were in the same magnitude as those for men in our study (Table 2) and within the confidence interval for our insignificant results for hip fracture (Table 3). We did not find a statistically significant inverse association between grip strength and osteoporotic fracture in men 65–79 in our study, but this might depend on lack of power.
Our findings, together with conclusions from several other studies [13, 14, 16, 17], could have important public health implications. Grip strength is, in comparison with other physical measures, easily measured, cheap, and highly reproducible in clinical practice [35, 36]. An intriguing implication is that grip strength might act as a biomarker of aging across the life course [37], which is supported by the observed inverse association between grip strength and fracture risk in men 50–64 years in our data. Grip strength could, at least partly, be attributed to exposures accumulating from early life onwards. Findings from studies of birth cohorts have shown that early life factors have long-term associations with grip strength in adulthood [38].
Loss of grip strength is unlikely to depend on a single final common pathway for the adverse effects of aging, but it might be a particularly good marker of the combined impact of behavior, and any underlying biological aging processes contributing to change in muscle function [39]. Results from the National Health and Nutrition Examination Survey [40] support this suggestion. In this US study, they found that weak grip strength was independently associated with physical limitations, lower body weight, and not reporting good health status, and conclude that grip strength could be a useful indicator for overall health assessment in older adults. Although handgrip strength cannot be assumed a proxy for overall muscle strength [19], grip strength is associated with many more markers of frailty than chronological age in men and women 64–74 years old [39]. One component of frailty is low bone mineral density (BMD), one of the main risk factors for fracture. Low grip strength has been found to correlate with low BMD and osteoporosis in postmenopausal women [41]. Thus, we may postulate that part of the association between grip strength and fracture goes through BMD. The same may be the case for physical limitations and low self-perceived health which both have shown to be associated with hip fractures [42]. Low BMI is a well-known risk factor for hip fracture. We have, however, adjusted for this variable in our study, as well as for self-perceived health and physical activity.
It has been suggested that grip strength could be an indicator of vitamin D status, since vitamin D might be of importance in maintaining or improving muscle strength and mobility in older adults. However, a systematic review and meta-analysis from 2016 did not find any improvement in handgrip strength after the administration of vitamin D with or without simultaneous calcium supplements [43].
On a general note, many studies that find inverse associations between grip strength and different health outcomes [13,14,15,16,17] including sarcopenia [22], indicate that handgrip strength might be an indicator of overall health. This is also underlined by the fact that handgrip strength has been found to be an independent predictor of in-hospital complications [44] and physical function and recovery after hip fracture [45].
Measuring grip strength
In this study, we used Martin Vigorimeter to measure the non-dominant arm, and we used the highest value of two attempts in each participant. There is considerable variation in devices, protocols, and procedures for the measurement of grip strength, which makes a comparison between studies very difficult [17, 35]. There is also evidence that variation in approach can affect the values recorded [35]. One study concluded that Martin Vigorimeter was a reliable and a more practical tool than the Jamar dynamometer [26], but another study comparing these two instruments, indicated a very high correlation between the two measures [36]. Although the literature indicates that the morphological parameters of the hand and lower arm might introduce some bias in the results of grip strength measurements, a study comparing the two most commonly used grip strength devices concluded that the influence of anatomical factors on grip strength measured with Martin Vigorimeter was low [36]. A standardized method would enable more consistent assessments of grip strength and thus a more reliable way to compare results from different studies [35].
Mean age at fracture
In our study, mean age at first fracture was about 72 and 76 years, respectively for osteoporotic and hip fracture, and about the same in men and women. Because the age-group with measured grip strength in our sample was 50–79 years at baseline in 1994–1995, the majority of participants had not yet reached the peak age of hip fracture.
Strengths and limitations
A strength of this study is the population-based design, the validated fracture register [29], and a high attendance rate [25]. The Tromsø Study also includes substantial information regarding several risk factors for fracture, enabling the appropriate handling of confounders. Our study is one of the few prospective studies in this field [17], where grip strength was measured years before the fracture event. The median follow-up was close to 15 years, reducing the risk of reverse causation. However, during this long follow-up, individual changes could have occurred in the grip strength, health behaviors, health status, and/ or use of medication affecting bone and falls. Measuring these factors at only one time point might introduce bias in our results. However, most likely such potential biases should have led to underestimation of the association between grip strength and fractures.
Although having adjusted for several possible confounders in our study—including lifestyle factors, BMI, height, several diseases, and self-perceived health—there might still be residual confounding. We have, for example, no information about long-time use of glucocorticoids.
Conclusion
In this population-based cohort study with a median of 15 years follow-up, we found an increased risk of non-vertebral osteoporotic fracture with lower levels of grip strength in both men and women, and the association was most pronounced in men aged 50–64 years. In women, we found an association between grip strength and hip fracture. Grip strength may be a useful method of identifying individuals who are at high risk of fractures and who might benefit from further health assessments and preventive interventions to avoid serious events.
References
Lofthus CM, Frihagen F, Meyer HE, Nordsletten L, Melhuus K, Falch JA (2008) Epidemiology of distal forearm fractures in Oslo, Norway. Osteoporos Int 19:781–786
Cauley JA, Chalhoub D, Kassem AM, El-Hajj Fuleihan G (2014) Geographic and ethnic disparities in osteoporotic fractures. Nat Rev Endocrinol 10:338–351
Søgaard AJ, Holvik K, Meyer HE, Tell GS, Gjesdal CG, Emaus N, Grimnes G, Schei B, Forsmo S, Omsland TK (2016) Continued decline in hip fracture incidence in Norway: a NOREPOS study. Osteoporos Int 27:2217–2222
Cooper C, Cole ZA, Holroyd CR, Earl SC, Harvey NC, Dennison EM, Melton LJ, Cummings SR, Kanis JA, IOF CSA Working group on fracture epidemiology (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22:1277–1288
Omsland TK, Magnus JH (2014) Forecasting the burden of future postmenopausal hip fractures. Osteoporos Int 25:2493–2496
Kanis JA, Cooper C, Rizzoli R, Abrahamsen B, Al-Daghri NM, Brandi ML, Cannata-Andia J, Cortet B, Dimai HP, Ferrari S, Hadji P, Harvey NC, Kraenzlin M, Kurth A, McCloskey E, Minisola S, Thomas T, Reginster JY, European Society for Clinical and Economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO) (2017) identification and management of patients at increased risk of osteoporotic fracture: outcomes of an ESCEO expert consensus meeting. Osteoporos Int 28:2023–2034
Veronese N, Maggi S (2018) Epidemiology and social costs of hip fracture. Injury 49:1458–1460
Solbakken SM, Meyer HE, Stigum H, Søgaard AJ, Holvik K, Magnus JH, Omsland TK (2017) Excess mortality following hip fracture: impact of self-perceived health, smoking, and body mass index. A NOREPOS study. Osteoporos Int 28:881–887
Kanis JA, McCloskey EV, Harvey NC, Johansson H, Leslie WD (2015) Intervention thresholds and the diagnosis of osteoporosis. J Bone Miner Res 30:1747–1753
Järvinen TL, Michaëlsson K, Jokihaara J, Collins GS, Perry TL, Mintzes B, Musini V, Erviti J, Gorricho J, Wright JM, Sievänen H (2015) Overdiagnosis of bone fragility in the quest to prevent hip fracture. BMJ 350:h2088
Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner WS, Nevitt MC, Cummings SR, Osteoporotic fractures research group (2003) BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res 18:1947–1954
Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J, Burckhardt P, Cooper C, Christiansen C, Cummings S, Eisman JA, Fujiwara S, Glüer C, Goltzman D, Hans D, Krieg MA, La Croix A, McCloskey E, Mellstrom D, Melton LJ 3rd, Pols H, Reeve J, Sanders K, Schott AM, Silman A, Torgerson D, van Staa T, Watts NB, Yoshimura N (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18:1033–1046
Cooper R, Kuh D, Cooper C, Gale CR, Lawlor DA, Matthews F, Hardy R, FALCon and HALCyon Study Teams (2011) Objective measures of physical capability and subsequent health: a systematic review. Age Ageing 40:14–23
Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A Jr, Orlandini A, Seron P, Ahmed SH, Rosengren A, Kelishadi R, Rahman O, Swaminathan S, Iqbal R, Gupta R, Lear SA, Oguz A, Yusoff K, Zatonska K, Chifamba J, Igumbor E, Mohan V, Anjana RM, Gu H, Li W, Yusuf S, Prospective Urban Rural Epidemiology (PURE) Study investigators (2017) Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 386:266–273
Karlsen T, Nauman J, Dalen H, Langhammer A, Wisløff U (2017) The combined association of skeletal muscle strength and physical activity on mortality in older women: The HUNT2 Study. Mayo Clin Proc 92:710–718
Celis-Morales CA, Welsh P, Lyall DM, Steell L, Petermann F, Anderson J, Iliodromiti S, Sillars A, Graham N, Mackay DF, Pell JP, Gill JMR, Sattar N, Gray SR (2018) Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: prospective cohort study of half a million UK Biobank participants. BMJ 361:k1651
Denk K, Lennon S, Gordon S, Jaarsma RL (2018) The association between decreased hand grip strength and hip fracture in older people: A systematic review. Exp Gerontol 111:1–9
Strand BH, Cooper R, Bergland A, Jørgensen L, Schirmer H, Skirbekk V, Emaus N (2016) The association of grip strength from midlife onwards with all-cause and cause-specific mortality over 17 years of follow-up in the Tromsø Study. J Epidemiol Community Health 70:1214–1221
Yeung SSY, Reijnierse EM, Trappenburg MC, Hogrel JY, McPhee JS, Piasecki M, Sipila S, Salpakoski A, Butler-Browne G, Pääsuke M, Gapeyeva H, Narici MV, Meskers CGM, Maier AB (2018) Handgrip strength cannot be assumed a proxy for overall muscle strength. J Am Med Dir Assoc 19:703–709
Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K (2013) Frailty in elderly people. Lancet 381:752–762
Cöster ME, Karlsson M, Ohlsson C, Mellström D, Lorentzon M, Ribom E, Rosengren B (2018) Physical function tests predict incident falls: a prospective study of 2969 men in the Swedish Osteoporotic Fractures in Men study. Scand J Public Health 29:1403494818801628. https://doi.org/10.1177/1403494818801628
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M, Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2 (2019) Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 48:16–31
Meyer HE, Henriksen C, Falch JA, Pedersen JI, Tverdal A (1995) Risk factors for hip fracture in a high incidence area: a case-control study from Oslo, Norway. Osteoporos Int 5:239–246
Harvey NC, Odén A, Orwoll E, Lapidus J, Kwok T, Karlsson MK, Rosengren BE, Ribom E, Cooper C, Cawthon PM, Kanis JA, Ohlsson C, Mellström D, Johansson H, McCloskey E (2018) Measures of physical performance and muscle strength as predictors of fracture risk independent of FRAX, falls, and aBMD: A meta-analysis of the Osteoporotic Fractures in Men (MrOS) Study. J Bone Miner Res 33:2150–2157
Jacobsen BK, Eggen AE, Mathiesen EB, Wilsgaard T, Njølstad I (2012) Cohort profile: The Tromso Study. Int J Epidemiol 41:961–967
Sipers WM, Verdijk LB, Sipers SJ, Schols JM, van Loon LJ (2016) The Martin Vigorimeter represents a reliable and more practical tool than the Jamar Dynamometer to assess handgrip strength in the geriatric patient. Am Med Dir Assoc 17:466.e1-7
Strand BH, Bergland A, Jørgensen L, Schirmer H, Emaus N, Cooper R (2019) Do More Recent Born Generations of Older Adults Have Stronger Grip? A Comparison of Three Cohorts of 66- to 84-Year-Olds in the Tromsø Study. J Gerontol A Biol Sci Med Sci 74:528–533
Ahmed LA, Schirmer H, Berntsen GK, Fønnebø V, Joakimsen RM (2006) Self-reported diseases and the risk of non-vertebral fractures: the Tromsø study. Osteoporos Int 17:46–53
Joakimsen RM, Fønnebø V, Søgaard AJ, Tollan A, Størmer J, Magnus JH (2001) The Tromsø study: registration of fractures, how good are self-reports, a computerized radiographic register and a discharge register? Osteoporos Int 12:1001–1005
Skirbekk V, Hardy M, Strand BH (2018) Women's spousal choices and a man's handshake: Evidence from a Norwegian study of cohort differences. SSM Popul Health 5:1–7
WHO Collaborating Centre for Drug Statistics Methodology (2012) Guidelines for ATC classification and DDD assignment 2013, 16th edn. Oslo, Norwegian Institute of Public Health
Robbins JA, Schott AM, Garnero P, Delmas PD, Hans D, Meunier PJ (2005) Risk factors for hip fracture in women with high BMD: EPIDOS study. Osteoporos Int 16:149–154
Søgaard AJ, Ranhoff AH, Meyer HE, Omsland TK, Nystad W, Tell GS, Holvik K (2018) The association between alcohol consumption and risk of hip fracture differs by age and gender in Cohort of Norway: a NOREPOS study. Osteoporos Int 29:2457–2467
Cawthon PM, Fullman RL, Marshall L, Mackey DC, Fink HA, Cauley JA, Cummings SR, Orwoll ES, Ensrud KE Osteoporotic fractures in Men (MrOS) research group (2008) Physical performance and risk of hip fractures in older men. J Bone Miner Res 23:1037–1044
Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Cooper C, Sayer AA (2011) A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing 40:423–429
Neumann S, Kwisda S, Krettek C, Gaulke R (2017) Comparison of the grip strength using the Martin-Vigorimeter and the JAMAR-dynamometer: establishment of normal values. In Vivo 31:917–924
Lara J, Cooper R, Nissan J, Ginty AT, Khaw KT, Deary IJ, Lord JM, Kuh D, Mathers JC (2012) A proposed panel of biomarkers of healthy ageing. BMC Med 13:222
Dodds R, Denison HJ, Ntani G, Cooper R, Cooper C, Sayer AA, Baird J (2012) Birth weight and muscle strength: a systematic review and meta-analysis. J Nutr Health Aging 16:609–615
Syddall H, Cooper C, Martin F, Briggs R, Aihie Sayer A (2003) Is grip strength a useful single marker of frailty? Age Ageing 32:650–656
Forrest KYZ, Williams AM, Leeds MJ, Robare JF, Bechard TJ (2018) Patterns and correlates of grip strength in older Americans. Curr Aging Sci 11:63–70
Li YZ, Zhuang HF, Cai SQ, Lin CK, Wang PW, Yan LS, Lin JK, Yu HM (2018) Low grip strength is a strong risk factor of osteoporosis in postmenopausal women. Orthop Surg 10:17–22
Hannan MT, Weycker D, McLean RR, Sahni S, Bornheimer R, Barron R, Travison TG, Kiel DP (2019) Predictors of imminent risk of nonvertebral fracture in older, high-risk women: the Framingham osteoporosis study. JBMR Plus 3:e10129
Rosendahl-Riise H, Spielau U, Ranhoff AH, Gudbrandsen OA, Dierkes J (2017) Vitamin D supplementation and its influence on muscle strength and mobility in community-dwelling older persons: a systematic review and meta-analysis. J Hum Nutr Diet 30:3–1
Ji HM, Han J, Bae HW, Won Y (2017) Combination of measures of handgrip strength and red cell distribution width can predict in-hospital complications better than the ASA grade after hip fracture surgery in the elderly. BMC Musculoskelet Disord 18:375
Selakovic I, Dubljanin-Raspopovic E, Markovic-Denic L, Marusic V, Cirkovic A, Kadija M, Tomanovic-Vujadinovic S, Tulic G (2019) Can early assessment of hand grip strength in older hip fracture patients predict functional outcome? PLoS One 14:e0213223
Acknowledgements
We would like to thank Professor Vinjar Fønnebø, UiT The Arctic University of Norway; Dr Anne Tollan, MD PhD, Hoddles Creek, Victoria, Australia; Professor Ragnar Martin Joakimsen, University Hospital of North Norway, Tromsø, Norway; Professor Gro Rosvold Berntsen, Norwegian Centre for E-health Research, University Hospital of North Norway; Professor Lone Jørgensen, UiT The Arctic University of Norway; Associate Professor, Dr Luai A. Ahmed, Institute of Public Health, United Arab Emirates University, Al Ain, UAE; and the Tromsø Study for their priceless contributions in collection and quality assurance of the data used in this paper. We are also grateful to all the study participants. Without their support through the whole history of the Tromsø Study, there would have been nothing to report.
Funding
No external funding has been received to finance this project.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All participants in the Tromsø Study gave informed written signed consent. The study and the data linkages have been approved by the Norwegian Data Inspectorate, the Regional Committee for Medical and Health Research Ethics (North) (2011/1659/REK nord), UiT The Arctic University of Norway, and Norwegian Institute of Public Health. The study has been conducted in full accordance with the Helsinki Declaration of the World Medical Association.
Conflicts of interest
Anne Johanne Søgaard, Jeanette H Magnus, Åshild Bjørnerem, Kristin Holvik, Anette Hylen Ranhoff, Nina Emaus, Haakon E Meyer, and Bjørn Heine Strand declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Søgaard, A.J., Magnus, J.H., Bjørnerem, Å. et al. Grip strength in men and women aged 50–79 years is associated with non-vertebral osteoporotic fracture during 15 years follow-up: The Tromsø Study 1994–1995. Osteoporos Int 31, 131–140 (2020). https://doi.org/10.1007/s00198-019-05191-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-019-05191-4