
Abstract
Summary
This systematic review and meta-analysis summarized the results from nine eligible observational studies. Lithium use was significantly associated with a decrease risk of fractures.
Introduction
The association between lithium use and risk of fracture is uncertain. To date, there have been no meta-analyses that have studied the association between the two. We conducted a systematic review and meta-analysis to examine the effect of lithium medication on the risk of fracture.
Methods
A comprehensive literature search was performed in PubMed, Embase, and MEDLINE to include eligible observational studies. Three reviewers conducted the literature search, study selection, study appraisal, and data abstraction independently. Random effects models were used to obtain the overall estimate for meta-analysis. Cochran’s Q and Higgins’ I2 were used to assess heterogeneity. A funnel plot and Egger’s regression test were employed to assess publication bias.
Results
Of the 3819 studies that were identified by our search strategy, eight were eligible for the systematic review, while seven of them qualified for the meta-analysis. In studies that reported risk ratio (RR) of fracture as an outcome (five studies [n = 1,134,722]), lithium use was associated with a 20% decrease in risk of fracture (RR = 0.80; 95% CI, 0.73–0.87; p < 0.01). A decreased risk of fracture associated with lithium was also observed in studies that adjusted for previous fractures (RR = 0.81; 95% CI, 0.73–0.89; p < 0.01). The decreased risk of fracture associated with lithium use remained consistent in all the analyses with different inclusion criteria. Neither significant heterogeneity nor significant publication bias was observed.
Conclusion
The present systematic review and meta-analysis demonstrated that lithium use was associated with a significant decreased risk of fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporotic fracture has been recognized as a worldwide public health concern since the last century. Around the world, an estimated 200 million people are affected by osteoporosis [1], and every year, there are around nine million fractures caused by osteoporosis [2]. Within the population over 50 years of age, around 20% of males will experience osteoporotic fractures, while more than 30% of females will suffer from the same condition [3,4,5]. As a consequence of the progressive aging of the global population, the incidence of osteoporotic fracture is expected to rise rapidly. In the USA alone, the number of hip fractures is estimated to triple by 2040 [6]. The economic and social burdens caused by osteoporotic fractures are already regarded as critical issues among many developed countries [7,8,9], and the social burdens caused by osteoporotic fractures have also arisen among developing countries. For instance, in China alone, around 70 million Chinese are affected by osteoporosis, which alone results in around 700,000 hip fractures in China every year [10].
Lithium is one of the most effective medications for the long-term treatment of bipolar disorder [11, 12]. It has been demonstrated to be efficient in the treatment of acute mania and depression and to be serviceable in decreasing the risk of suicide [13]. Our previous meta-analysis demonstrated that antidepressants, including tricyclic antidepressants and selective serotonin reuptake inhibitors, are associated with increased fracture risk [14, 15]. However, the effect of lithium use on fracture risk and bone mineral density (BMD) is uncertain. Some studies suggest that lithium use is related to bone loss since lithium medication usually leads to a hyperparathyroid state [16,17,18,19] that increases the risk of bone loss, while other studies suggest that lithium use is associated with an increase in BMD [20] and a decrease in fracture risk [21,22,23].
We conducted a comprehensive systematic review and meta-analysis to assess all eligible observational studies in order to examine the effect of lithium use on BMD and fracture risk, both quantitatively and qualitatively. We also investigated whether such an effect varied by sex, age, geographical location, study size, alcohol use, or adjustment for comorbidities.
Materials and methods
This systematic review and meta-analysis was guided by Meta-analyses of Observational Studies in Epidemiology (MOOSE) [24], and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [25] was used as a reference. A protocol was also preregistered in the International Prospective Register of Systematic Reviews, where the objectives, literature search strategy, inclusion criteria, exclusion criteria, methods of study selection, data abstraction, and methods of statistical analysis were elaborated upon. The protocol is available at the following URL:https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=60499.
Eligibility criteria
Observational studies that investigated the association between lithium use and fracture risk or BMD were eligible for inclusion in our systematic review, while studies were eligible for the meta-analysis if they met the following criteria: (1) observational studies, (2) human participants, (3) lithium use as exposure, and (4) risk of fracture or BMD as the outcome, with corresponding 95% CIs or other data that could be used for variance calculation. Exclusion criteria for our meta-analysis were as follows: (1) risk of osteoporosis without fracture as the outcome and (2) duplicated studies.
Literature search
A comprehensive literature search of PubMed through February 16, 2018, was conducted (Supplemental Table 2). “Lithium,” “bone loss,” “bone fracture,” “fracture,” “bone density,” and “osteoporosis” were the medical subject heading (MESH) terms for our literature search. The keyword “bone mineral density” was also used during the search. We restricted the search to the English language and to human studies only. Using similar strategies, searches of MEDLINE Web of Science and Embase database were performed as well. Three investigators (B.L., S.Z., and A.D.R.) conducted the literature search independently. Librarians were consulted to ensure the comprehensiveness of the literature search. We also searched unpublished data, including abstracts, theses, and dissertations, by using the Google search engine. The reference lists of original studies and relevant meta-analysis articles and review articles were reviewed independently by the three reviewers.
Study selection
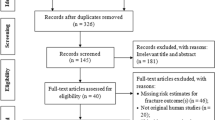
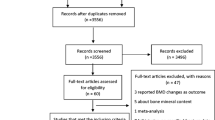
To identify potential eligible studies, the titles and abstracts of all references obtained in the literature search were screened independently by the three reviewers. During this stage, references that were agreed upon by all three reviewers to be irrelevant to this systematic review and meta-analysis were excluded, while the remaining references were assessed for eligibility by examining the full-text contents. All three reviewers independently scrutinized the full contents to assess eligibility. Fleiss’ kappa statistic, as an adaptation of Cohen’s kappa for three or more raters, was used to assess the agreement between the three investigators [26]. Areas of uncertainty or disagreement were adjudicated by a fourth reviewer (Q.W.). The process of study selection is presented as a PRISMA flow diagram (Fig. 1).

Flow diagram of study selection
Data abstraction
The following study characteristics were extracted: author(s), study name, publication year, study population and region, study design, and participant age, sex, and race. Additional characteristics such as study size, dose of lithium use, former use of other antidepressants, and other medications were extracted for further analysis. We also extracted hazard ratios (HR), relative risks (RR), and odds ratios (OR) of fracture associated with lithium use and the corresponding standard errors. For the studies with BMD as the outcome, the mean differences between lithium users and non-users and the corresponding standard deviations or standard errors were abstracted. If the original studies contained more than one estimate for the same outcome, we chose the one that was adjusted for the largest number of confounders. All data abstraction was conducted using REDCap, which is a browser-based application designed for researchers performing data collection. Three reviewers (B.L., S.Z, and A.D.R) performed data abstraction and data entry independently. Fleiss’ kappa was calculated to examine the level of inconsistency among the three reviewers, and any inconsistency with the data abstraction and data entry was discussed and adjudicated by a fourth reviewer (Q.W). To ensure accuracy, all three reviewers examined the data at least twice. Since we were able to obtain all the necessary information from the papers alone, we did not contact the authors for more information.
Study appraisal
The Newcastle-Ottawa quality assessment scales for cohort studies and case-control studies were used to examine risk of bias and to gauge the methodology quality of the included studies. For each study, we calculated a quality score based on a prespecified questionnaire [27]. For cohort studies, the following eight criteria were used for quality assessment: representativeness of the exposed cohort, selection of non-exposed cohort, ascertainment of exposure, demonstration that outcome of interest was not present at the start of the study, comparability of cohorts on the basis of the design or analysis, assessment of outcome, follow-up duration long enough for outcomes to occur, and adequacy of follow-up of cohorts. For case-control studies, the following eight criteria were used for quality assessment: adequacy of the case definition, selection of controls, definition of the controls, representativeness of the cases, comparability of cases and controls on the basis of the design or analysis, ascertainment of exposure, the same method of ascertainment for cases and controls, and non-response rate. The score for both cohort and case-control studies ranged from 0 to 9, where a score of 9 indicates the strongest regarding methodology. Information about the Newcastle-Ottawa Scale for each study is summarized in Supplemental Table 2. As the MOOSE group [24] recommends, the quality scores were not used as weights in conducting the meta-analysis. However, the quality scores were used in the sensitivity analyses.
Statistical analysis
The primary summary measures in the meta-analysis were confounder-adjusted RRs for fracture. Since the absolute risk of osteoporotic fractures is low, OR approximates RR [28]. Additionally, HR is broadly equivalent to RR [29]. Hence, in our statistical analysis, we approximated HRs and ORs as RRs. The natural logarithmic-transformed RRs were used to stabilize the variance, and the variances of the log-transformed RRs were calculated using CIs or p values given in the original studies. The reciprocal of the variance for each study was used as the weight of the corresponding study to calculate the overall effect size. The mean difference of BMD between the lithium-treated group and control group was calculated for each study, and the variances for the mean differences in BMD were computed by pooling individual variances or using CIs.
Several sensitivity analyses‚ in which the effect of lithium use on fracture risk were analyzed under different inclusion criteria, were conducted to assess the robustness of the major findings in our meta-analysis. We also performed several prespecified subgroup analyses to determine if fracture risk associated with lithium use was influenced by age, sex, geographical location, sample size of the study, or previous fractures and if the study had been controlled for other antidepressant uses.
The heterogeneity was assessed by Cochran’s Q statistic and Higgins’ I2 statistic. We expected the existence of heterogeneity since we had combined the outcomes from both case-control studies and cohort studies. Moreover, the participants from the original studies were different in terms of sex, age, race, ethnicity, location, and the fact that the studies had distinctive settings. Nevertheless, Cochran’s Q statistic (p = 0.61) and zero Higgins’ I2 indicated no significant heterogeneity among the fracture outcomes. Although no significant heterogeneity was detected, a random effects model was employed in the meta-analysis instead of a fixed effects model since the included epidemiologic studies were conducted differently with regard to study setting, study design, and study population. Thus, the true effect size may differ from study to study [30].
To provide a visual inspection of publication bias, a funnel plot was generated, and to examine publication bias quantitatively, Egger’s regression test was employed. All data analyses were performed using R statistical software.
Results
Study characteristics
A total of 3819 relevant references were identified in our initial search, and after removing any duplicates, 3057 records were identified as potential references. We screened the titles and abstracts of all the references and identified 65 studies for full-text review, with moderate agreement among the three investigators (k = 0.75). After full review of these 65 studies, eight studies [16, 20,21,22,23, 31,32,33] met the inclusion criteria for systematic review, with high agreement among three investigators (k = 0.92). All eligible studies were published in English. The characteristics of the included studies are presented in Table 1. Six [21,22,23, 31,32,33] reported risk of fracture as an outcome, while two [16, 20] reported BMD as an outcome. For two studies that reported BMD as an outcome, both reported PTH levels. Both studies reported BMD at lumbar spine and femoral neck. However, only one study [20] reported BMD at trochanter and Ward’s triangle. Of the two studies that reported BMD as an outcome, both found that the lithium-treated groups were associated with higher BMD at the lumbar spine and femoral neck compared to the control groups. Of the six studies that reported risk of fracture as an outcome, all of them found that lithium use was associated with a decreased risk of fracture.
All eight studies [16, 20,21,22,23, 31,32,33] were eligible for the meta-analysis. However, two of the eight studies were conducted with the same population [23, 33]. From these two studies, we selected the one that defined the exposure consistently with the other four studies that reported fracture risk [33] and we excluded the other [23]. Among the seven studies eventually included in the meta-analysis, five were case-control studies [16, 20,21,22, 33] and two were cohort studies [31, 32]. In total, there were 1,134,722 individuals that comprised our systematic review and meta-analysis. The number of participants ranged from 50 in the study by Nordenstrom [16] to 498,347 in the study by Vestergaard [23]. The mean age of participants varied from 43 in the study by Su [32] to 64.2 in the study by Bolton [31]. Among all the studies included, only the study by Bolton [31] reported the proportion of postmenopausal women. In this study, 99% of women participants are postmenopausal. All the studies included both male and female participants, and all the studies controlled for both sex and age. Alcohol consumption, as a potential risk factor for fracture, was controlled for in three studies [31,32,33], and the Charlson Comorbidity Index was controlled for in three studies [31,32,33]. The Newcastle-Ottawa Scale quality scores ranged from 7 to 9, with six studies scoring greater than 7 [16, 20, 23, 31,32,33].
Meta-analysis
In the five studies that reported risk of fracture, three case-control studies reported ORs [n = 1,024,984] and two cohort studies reported HRs [n = 109,485]. The approximate RRs (95% CIs) of fracture due to lithium use for each study and the overall RR are presented in the forest plot (Fig. 2). The approximate RR was less than 1 for each of the five studies included, and overall, a 20% decrease in fracture risk (RR = 0.80, 95% CI, 0.73–0.87, p < 0.001) was associated with lithium use. Both Cochran’s Q statistic (p = 0.60) and Higgins’ I2 statistic (0%) suggested that no heterogeneity was present.

Risk of fracture associated with lithium by individual studies and by all studies combined. The horizontal lines represent 95% CIs for the effect estimates. The size of the square boxes specifies the weights of studies. The diamond stands for the overall effect size
Both studies that reported BMD as the outcome were case-control studies [16, 20]. Increases in mean BMD at the lumbar spine (0.06 g/cm2, − 0.15–0.26, p = 0.62) and femoral neck (0.06 g/cm2, − 0.15–0.26, p = 0.60) in the lithium-user group were observed.
Sensitivity analysis
All of the estimated fracture risks associated with lithium use were significant under the different study inclusion criteria (Table 2). For instance, the overall RR almost remained unchanged when only the studies with more than 100,000 participants were included in the analysis. When only the studies with less than 100,000 participants were included in the analysis, the overall RR decreased slightly to 0.74, and when only the studies from Europe were included, the overall RR increased slightly to 0.81. When excluding the two studies that did not provide the definition of exposure as “ever use of lithium” [31, 32], the overall RR varied little. Furthermore, when the analysis was limited to the studies with quality scores greater than 7 [31,32,33], the overall RR decreased slightly to 0.78. Since all the original studies included in the meta-analysis reported the number of female participants and male participants specifically, we also calculated the gender ratios of the studies, where the gender ratio is defined as the number of female participants to the number of male participants. When we only included the studies with gender ratios greater than 2 [22, 31], the overall RR decreased significantly to 0.68. When the analysis was confined to the studies that adjusted for the Charlson Comorbidity Index [31,32,33], the overall RR decreased slightly to 0.78. When the analysis was confined to studies that had adjusted for previous falls [21, 33], the overall RR was 0.74. When only the studies that adjusted for psychotic diseases [22, 31,32,33] were included, the overall RR decreased to 0.76. Finally, when the studies that did not adjust for prior use of bone active drug were excluded [22, 33], the overall RR increased slightly to 0.85.
Publication bias
The funnel plot (Fig. 3) revealed no publication bias, while the result from Egger’s regression test suggested that any publication bias was insignificant (p = 0.63). Since the results from both the funnel plot and Egger’s test suggested no publication bias for this study, the trim-and-fill correction procedure was not implemented.

Funnel plot with 95% confidence limits. The horizontal axis represents the effect size. The vertical axis stands for the standard error
Discussion
A comprehensive systematic review and meta-analysis were conducted to assess the association between lithium treatment and risk of fracture, based on all eligible studies from a wide range of geographical areas and subjects. In our systematic review, results from the six studies with fracture data were consistent in finding that lithium treatment is associated with a decreased fracture risk, while the two studies with BMD data found that individuals treated with lithium had a higher BMD compared to those who were not treated with lithium. Meanwhile, the pooled overall result from our meta-analysis found that lithium use was associated with a 20% decreased risk of fracture. Such results were consistently significant in all sensitivity analyses and subgroup analyses (Table 1), which indicate that our findings are robust. Moreover, the pooled results of the two studies that reported BMD suggested that lithium use is associated with an increased BMD at the lumbar spine and femoral neck. All the results that we obtained suggest that lithium use may decrease risk of fracture through its effect on BMD.
The mechanisms through which lithium may decrease risk of fracture are likely to be complex. Lithium may have a positive effect on BMD by affecting the transport of calcium. Research on animals found that lithium activates the canonical WNT path through its effect on the enzyme named GSK-3β [34]. Lithium may also have an effect on the calcium-sensing receptor transduction system in organs such as renal tubules [35]. By affecting the transport of calcium in a positive direction, lithium creates a friendly environment for the absorption of calcium, hence leading to increased BMD. As several former studies have suggested, decreased BMD is associated with increased risk of fracture [3, 36]. Therefore, lithium use is likely to decrease the risk of fracture by increasing BMD. In addition, bipolar disorder is associated with increased fracture risk [32, 37]. As an effective and widely used medication to treat bipolar disorder, lithium may decrease fracture risk by alleviating symptoms of bipolar disorder. Moreover, bipolar disorder is found to be associated with poor health behaviors such as smoking and increased alcohol consumption [38,39,40], and such health behaviors have been observed to affect bone metabolism [41]. Thus, for patients with bipolar disorder, lithium treatment may decrease the risk of fracture by alleviating the above conditions associated with bipolar disorder. However, several studies [16,17,18,19,20] suggest that since lithium use is associated with increased PTH level, long-term treatment of lithium might be associated with hyperparathyroidism. Hyperparathyroidism may induce hypercalcemia, which leads to bone resorption. Hence, it is likely that an appropriate dose of lithium medication is associated with slight increase in PTH level, which results in anabolic effect on bones and a decrease in the risk of fracture. The appropriate dose for lithium medication, which leads to a protective effect on bone, is warranted for additional investigation.
There are some limitations in our meta-analysis and systematic review. First, since only studies in the English language were included, language bias was expected to be an issue. To address this, we performed an additional search in PubMed, Embase, and MEDLINE for non-English-language studies only. However, after reviewing all the abstracts, no additional studies met our inclusion criteria. Secondly, important sources of heterogeneity such as variation in lithium dosage, duration of lithium use, and associated indications could not be assessed, because this information either was not available or was mixed in most of the included studies. Thirdly, the existence of other diseases may have confounded the effect of lithium use. However, even with the inclusion of only the studies that had been adjusted for comorbidities, our results remained consistent. In addition, because there are more case-control studies and fewer cohort studies that met inclusion criteria for this meta-analysis research, our findings are subject to selection bias from these case-control studies, even though our analysis suggested no evidence for publication bias in this meta-analysis. Finally, because a limited number of original studies were eligible for the meta-analysis, a meta-regression could not be conducted. Instead, we conducted sensitivity analyses and subgroup analyses, using the information that was available in the original articles.
In summary, we conducted the first systematic review and meta-analysis on the association between lithium use and fracture risk and demonstrated that lithium use is associated with a significant decreased risk of fracture. As a highly prevalent condition, osteoporotic fracture has caused an elevation of social and economic burden worldwide. Thus, the discovered link between lithium treatment and risk of fracture will have a crucial impact on global public health. Future large perspective studies are warranted to explain and expand upon how lithium is associated with a decreased risk of fracture and its association with BMD.
Abbreviations
- BMD:
-
Bone mineral density
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
- MOOSE:
-
Meta-analysis of Observational Studies in Epidemiology
- PRISMA:
-
Preferred Reporting Items for Systematic Review and Meta-analyses
- OR:
-
Odds ratio
- RR:
-
Risk ratio or relative risk
- REDCap:
-
Research Electronic Data Capture
References
Pisani P, Renna MD, Conversano F, Casciaro E, di Paola M, Quarta E, Muratore M, Casciaro S (2016) Major osteoporotic fragility fractures: risk factor updates and societal impact. World J Orthop 7:171–181. https://doi.org/10.5312/wjo.v7.i3.171
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726–1733. https://doi.org/10.1007/s00198-006-0172-4
Melton LJ, Atkinson EJ, O’Connor MK et al (1998) Bone density and fracture risk in men. J Bone Miner Res Off J Am Soc Bone Miner Res 13:1915–1923. https://doi.org/10.1359/jbmr.1998.13.12.1915
Melton LJ, Chrischilles EA, Cooper C et al (1992) Perspective. How many women have osteoporosis? J Bone Miner Res Off J Am Soc Bone Miner Res 7:1005–1010. https://doi.org/10.1002/jbmr.5650070902
Kanis JA, Johnell O, Oden A et al (2000) Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int 11:669–674
Schneider EL, Guralnik JM (1990) The aging of America. Impact on health care costs. JAMA 263:2335–2340
Hernlund E, Svedbom A, Ivergård M et al (2013) Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 8:136. https://doi.org/10.1007/s11657-013-0136-1
Svedbom A, Hernlund E, Ivergård M et al (2013) Osteoporosis in the European Union: a compendium of country-specific reports. Arch Osteoporos 8:137. https://doi.org/10.1007/s11657-013-0137-0
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22:465–475. https://doi.org/10.1359/jbmr.061113
Chinese Health Promotion Society Summary statement of osteoporosis white paper China 2008. Chin J Health Manag. 2009; 3 (3:):148–154
Burgess S, Geddes J, Hawton K, et al (2001) Lithium for maintenance treatment of mood disorders. Cochrane Database Syst Rev CD003013 . doi: https://doi.org/10.1002/14651858.CD003013
Kessing LV, Søndergård L, Kvist K, Andersen PK (2005) Suicide risk in patients treated with lithium. Arch Gen Psychiatry 62:860–866. https://doi.org/10.1001/archpsyc.62.8.860
Tondo L, Hennen J, Baldessarini RJ (2001) Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 104:163–172
Wu Q, Qu W, Crowell MD, Hentz JG, Frey KA (2013) Tricyclic antidepressant use and risk of fractures: a meta-analysis of cohort and case-control studies. J Bone Miner Res Off J Am Soc Bone Miner Res 28:753–763. https://doi.org/10.1002/jbmr.1813
Wu Q, Bencaz AF, Hentz JG, Crowell MD (2012) Selective serotonin reuptake inhibitor treatment and risk of fractures: a meta-analysis of cohort and case-control studies. Osteoporos Int 23:365–375. https://doi.org/10.1007/s00198-011-1778-8
Nordenström J, Elvius M, Bågedahl-Strindlund M, Bian Zhao, Törring O (1994) Biochemical hyperparathyroidism and bone mineral status in patients treated long-term with lithium. Metabolism 43:1563–1567
Mak TW, Shek CC, Chow CC et al (1998) Effects of lithium therapy on bone mineral metabolism: a two-year prospective longitudinal study. J Clin Endocrinol Metab 83:3857–3859. https://doi.org/10.1210/jcem.83.11.5269
Christiansen C, Baastrup PC, Transbøl I (1980) Development of “primary” hyperparathyroidism during lithium therapy: longitudinal study. Neuropsychobiology 6:280–283. https://doi.org/10.1159/000117770
Mallette LE, Khouri K, Zengotita H et al (1989) Lithium treatment increases intact and midregion parathyroid hormone and parathyroid volume. J Clin Endocrinol Metab 68:654–660. https://doi.org/10.1210/jcem-68-3-654
Zamani A, Omrani GR, Nasab MM (2009) Lithium’s effect on bone mineral density. Bone 44:331–334. https://doi.org/10.1016/j.bone.2008.10.001
Wilting I, de Vries F, Thio BMKS, Cooper C, Heerdink ER, Leufkens HGM, Nolen WA, Egberts ACG, van Staa TP (2007) Lithium use and the risk of fractures. Bone 40:1252–1258. https://doi.org/10.1016/j.bone.2006.12.055
Bolton JM, Metge C, Lix L, Prior H, Sareen J, Leslie WD (2008) Fracture risk from psychotropic medications: a population-based analysis. J Clin Psychopharmacol 28:384–391. https://doi.org/10.1097/JCP.0b013e31817d5943
Vestergaard P, Rejnmark L, Mosekilde L (2005) Reduced relative risk of fractures among users of lithium. Calcif Tissue Int 77:1–8. https://doi.org/10.1007/s00223-004-0258-y
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(264–269):W64
Fleiss JL (1971) Measuring nominal scale agreement among many raters. Psychol Bull 76:378–382
Wells GA, Shea B, O’Connell D, et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses
Ressing M, Blettner M, Klug SJ (2010) Data analysis of epidemiological studies: part 11 of a series on evaluation of scientific publications. Dtsch Arztebl Int 107:187–192. https://doi.org/10.3238/arztebl.2010.0187
Nurminen M (1995) To use or not to use the odds ratio in epidemiologic analyses? Eur J Epidemiol 11:365–371
Furukawa TA, Guyatt GH, Griffith LE (2002) Can we individualize the “number needed to treat”? An empirical study of summary effect measures in meta-analyses. Int J Epidemiol 31:72–76
Bolton JM, Morin SN, Majumdar SR et al (2017) Association of mental disorders and related medication use with risk for major osteoporotic fractures. JAMA Psychiatry 74:641–648. https://doi.org/10.1001/jamapsychiatry.2017.0449
Su J-A, Cheng B-H, Huang Y-C, Lee CP, Yang YH, Lu ML, Hsu CY, Lee Y, McIntyre RS, Chin Lin T, Chin-Hung Chen V (2017) Bipolar disorder and the risk of fracture: a nationwide population-based cohort study. J Affect Disord 218:246–252. https://doi.org/10.1016/j.jad.2017.04.037
Vestergaard P, Rejnmark L, Mosekilde L (2006) Anxiolytics, sedatives, antidepressants, neuroleptics and the risk of fracture. Osteoporos Int 17:807–816. https://doi.org/10.1007/s00198-005-0065-y
Clément-Lacroix P, Ai M, Morvan F et al (2005) Lrp5-independent activation of Wnt signaling by lithium chloride increases bone formation and bone mass in mice. Proc Natl Acad Sci U S A 102:17406–17411. https://doi.org/10.1073/pnas.0505259102
Lazarus JH, Davies CJ, Woodhead JS et al (1987) Effect of lithium on the metabolic response to parathyroid hormone. Miner Electrolyte Metab 13:63–66
Berger C, Langsetmo L, Joseph L, Hanley DA, Davison KS, Josse RG, Prior JC, Kreiger N, Tenenhouse A, Goltzman D, the CaMos Research Group (2009) Association between change in BMD and fragility fracture in women and men. J Bone Miner Res Off J Am Soc Bone Miner Res 24:361–370. https://doi.org/10.1359/jbmr.081004
Hsu C-C, Hsu Y-C, Chang K-H, Lee CY, Chong LW, Wang YC, Hsu CY, Kao CH (2016) Increased risk of fracture in patients with bipolar disorder: a nationwide cohort study. Soc Psychiatry Psychiatr Epidemiol 51:1331–1338. https://doi.org/10.1007/s00127-016-1242-3
Diaz FJ, James D, Botts S, Maw L, Susce MT, de Leon J (2009) Tobacco smoking behaviors in bipolar disorder: a comparison of the general population, schizophrenia, and major depression. Bipolar Disord 11:154–165. https://doi.org/10.1111/j.1399-5618.2009.00664.x
Gonzalez-Pinto A, Gutierrez M, Ezcurra J et al (1998) Tobacco smoking and bipolar disorder. J Clin Psychiatry 59:225–228
Cassidy F, Ahearn EP, Carroll BJ (2001) Substance abuse in bipolar disorder. Bipolar Disord 3:181–188
Alghadir AH, Gabr SA, Al-Eisa E (2015) Physical activity and lifestyle effects on bone mineral density among young adults: sociodemographic and biochemical analysis. J Phys Ther Sci 27:2261–2270. https://doi.org/10.1589/jpts.27.2261
Acknowledgements
We thank X Goodman for her advice on the literature search strategy.
Sources of funding
The project was supported by the Fund of Knowledge from the University of Nevada, Las Vegas.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Role of sponsors
In the data collection, management, analysis, and interpretation and in the preparation, review, approval, and study design of the manuscript, funding sponsors were not involved.
Conflicts of interest
None.
Electronic supplementary material
Supplemental Table 1
(DOCX 57.7 kb)
Supplemental Table 2
(DOCX 43.6 kb)
Rights and permissions
About this article

Cite this article
Liu, B., Wu, Q., Zhang, S. et al. Lithium use and risk of fracture: a systematic review and meta-analysis of observational studies. Osteoporos Int 30, 257–266 (2019). https://doi.org/10.1007/s00198-018-4745-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4745-9