
Abstract
Summary
Daily consumption of 50 g of dried plum (equivalent to 5–6 dried plums) for 6 months may be as effective as 100 g of dried plum in preventing bone loss in older, osteopenic postmenopausal women. To some extent, these results may be attributed to the inhibition of bone resorption with the concurrent maintenance of bone formation.
Introduction
The objective of our current study was to examine the possible dose-dependent effects of dried plum in preventing bone loss in older osteopenic postmenopausal women.
Methods
Forty-eight osteopenic women (65–79 years old) were randomly assigned into one of three treatment groups for 6 months: (1) 50 g of dried plum; (2) 100 g of dried plum; and (3) control. Total body, hip, and lumbar bone mineral density (BMD) were evaluated at baseline and 6 months using dual-energy X-ray absorptiometry. Blood biomarkers including bone-specific alkaline phosphatase (BAP), tartrate-resistant acid phosphatase (TRAP-5b), high-sensitivity C-reactive protein (hs-CRP), insulin-like growth factor-1 (IGF-1), and sclerostin were measured at baseline, 3 months, and 6 months. Osteoprotegerin (OPG), receptor activator of nuclear factor kappa-B ligand (RANKL), calcium, phosphorous, and vitamin D were measured at baseline and 6 months.
Results
Both doses of dried plum were able to prevent the loss of total body BMD compared with that of the control group (P < 0.05). TRAP-5b, a marker of bone resorption, decreased at 3 months and this was sustained at 6 months in both 50 and 100 g dried plum groups (P < 0.01 and P < 0.04, respectively). Although there were no significant changes in BAP for either of the dried plum groups, the BAP/TRAP-5b ratio was significantly (P < 0.05) greater at 6 months in both dried plum groups whereas there were no changes in the control group.
Conclusions
These results confirm the ability of dried plum to prevent the loss of total body BMD in older osteopenic postmenopausal women and suggest that a lower dose of dried plum (i.e., 50 g) may be as effective as 100 g of dried plum in preventing bone loss in older, osteopenic postmenopausal women. This may be due, in part, to the ability of dried plums to inhibit bone resorption. This clinical trial was registered at ClinicalTrials.gov: NCT02325895.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The prevalence of age-related bone loss is greater in women than in men [1, 2], and in 25 to 30 % of aging women, this loss results in major orthopedic problems [1]. In the United States (U.S.) alone, a conservative estimate is that nearly half of all women over the age of 50 years will suffer a fracture due to osteoporosis, resulting in more than 1.5 million fractures per year including painful and often debilitating hip fractures [3]. Over the past several decades, there have been significant advances in our understanding of the etiology and pathophysiology of osteoporosis, as well as the development of pharmaceutical agents for its treatment [4, 5]. There are currently numerous drug therapies aimed at reducing either bone loss or increasing bone formation. Nonetheless, these drugs are known to have negative side effects, high costs, and low compliance and maximally can prevent the rate of fractures by 50 % [4, 5]. Calcium and vitamin D supplementation has been recommended as a safe, nutritional approach to help reduce bone loss [6]; however, the U.S. Preventive Services Task Force has stated that calcium and vitamin D supplementation should not be used as a primary fracture prevention strategy [7]. In addition to diet and other lifestyle factors such as physical activity, there is evidence to suggest that functional foods can improve growth and development as well as reduce the risk of chronic diseases such as osteoporosis [8].
Among the functional foods that have been shown to have bone-protective effects, dried plum (Prunus domestica L.) is uniquely able to prevent and reverse bone loss in rat models of osteoporosis [9–12]. More relevantly, in a short-term clinical study [13], we demonstrated that supplementation of 100 g/day of dried plum over 3 months improved biomarkers of bone formation in postmenopausal women. We also carried out a 12-month study [14] in which postmenopausal women were asked to consume 100 g of dried plum daily. That study demonstrated the ability of dried plum to completely prevent the loss of bone mineral density (BMD).
Several rodent studies have provided insight into the mechanisms by which dried plum exerts its bone-protective effects [9–12, 15]. Age-related bone loss, including that which occurs in postmenopausal women, may be partly associated with decreased production of certain growth factors such as insulin-like growth factor-1 (IGF-1). We and others have shown that dried plum can increase IGF-1 levels in both humans [10] and animal models [9, 11]. Another mechanism by which dried plums prevent bone loss is via their strong antioxidant properties [16]. For instance, using an aged mouse model of osteoporosis, Rendina et al. [17] showed that dried plum increased circulating levels of glutathione peroxidase which is a strong enzymatic antioxidant. Another mechanism by which dried plum may prevent bone loss is through its anti-inflammatory properties. We [18] and other investigators [19] have demonstrated the effectiveness of dried plum polyphenol extract in reducing the production of proinflammatory molecules such as cyclooxygenase-2. In an ex vivo part of a study by Rendina et al. [20], the effectiveness of dried plum in reducing tumor necrosis factor alpha in induced splenocytes was shown. Altogether, although the exact mechanisms of action by which dried plum exerts its effects on bone are still unknown, research findings thus far indicate that dried plum may modify bone formation [9, 10, 12, 17] and bone resorption [12, 14] through modulation of osteoblast and osteoclast activities by increasing bone-specific alkaline phosphatase (BAP) [12, 14], IGF-1 [9, 12, 14], and reducing serum tartrate-resistant acid phosphatase-5b (TRAP-5b) [14], sclerostin [21], receptor activator of nuclear factor kappa-B ligand (RANKL), and osteoprotegerin (OPG) gene expression [12] .
Aside from the paucity of literature addressing the mechanisms of action by which dried plum prevents bone loss, clinical studies are needed to demonstrate whether more reasonable amounts of dried plum, e.g., 50 g of dried plum, can also be effective in preventing bone loss. Hence, the present study was designed to determine the extent to which this lower dose of dried plum (50 g) prevents the loss of BMD and improves bone biomarkers in older, osteopenic postmenopausal women. We hypothesized that a 50 g dose of dried plum during calcium and vitamin D supplementation would prevent loss of BMD equally to a 100 g dose and more effectively than a calcium and vitamin D supplementation regimen alone.
Methods
Participants
A total of 84 postmenopausal women, 65–79 years of age, not on hormone replacement therapy for at least 3 months before the initiation of the study were recruited from the greater San Diego, California area between August 2012 and September 2013. Recruitment took place in the community via flyers at local gyms, senior centers, markets, and word of mouth. Women with osteoporosis (i.e., BMD T-score at any site below 2.5 standard deviation of the mean) were excluded from the study. Furthermore, subjects treated with any prescription medications known to alter bone and calcium metabolism such as calcitonin, bisphosphonates, raloxifene, and/or anabolic agents such as parathyroid hormone, growth hormone, or steroids within 3 months before the start of the study were excluded. In addition, subjects with metabolic bone disease, renal disease, cancer, cardiovascular disease, diabetes mellitus, respiratory disease, gastrointestinal disease, liver disease or other chronic diseases, and heavy smokers (>20 cigarettes/day) were excluded. Women who regularly consumed dried plum or prune juice were not included in the study. A complete medical history and a dietary vitamin D and calcium questionnaire (SCQ2002) were obtained from the subjects before initiating the treatments. The subjects were advised to maintain their usual physical activity and diet pattern throughout the duration of the study. This clinical trial was registered at ClinicalTrials.gov: NCT02325895.
Study design
Of the 84 screened volunteers, 48 eligible osteopenic postmenopausal women, whose BMD T-score were between −1 and −2.5, were randomly assigned to one of the three dietary treatment groups for 6 months: 50 g/day of dried plum (n = 16), 100 g/day of dried plum (n = 16), or 0 g/day of dried plum (n = 16; control group). The amount of dried plum was based on the findings of our long-term clinical trial [13] which indicated that the consumption of 100 g of dried plum per day for 12 months significantly improved BMD of the ulna and spine compared to a comparative control (75 g dried apple). Due to the purported laxative properties of dried plum, the aim of this study was to compare 50 to 100 g/day dried plum to find out if a lower dose would also have a positive impact on BMD. The composition of dried plum per 100 g obtained from Food Processor version 7.50 (ESHA Research, Salem, OR) is as follows: energy = 239 kcal, protein = 2.61 g, fat = 0.52 g, total fiber = 7.10 g, calcium = 51 mg, phosphorus = 79 mg, total carbohydrates = 62.7 g. The study participants were asked to gradually incorporate dried plum into their diets and to monitor their compliance with a self-monitoring calendar. Briefly, participants were given customized calendars and were asked to record the days they missed consuming the study regimen. They were also asked to return any unused portion of the study regimen for compliance monitoring purposes. All participants received 500 mg of calcium carbonate plus 10 μg (400 IU) of vitamin D3 (cholecalciferol) daily.
Dietary and physical activity assessment and anthropometric measurements
A medical history questionnaire was obtained at the beginning of the study. The subjects completed a three-day food record at baseline, 3 months, and 6 months. Dietary analysis was performed using food analysis software (Food Processor version 7.50; ESHA Research, Salem, OR, USA). Similarly, physical activity patterns were assessed at baseline and analyzed based on energy expenditure/week using the CHAMPS Physical Activity Questionnaire for Older Adults (Palo Alto, CA, USA), which is designed to capture all physical activity commonly completed by the age group studied. Anthropometric data were collected at baseline and 6 months and height and weight were used to calculate BMI (kg/m2). Characteristics of study participants are displayed in Table 1.
Bone density assessments
Bone density was assessed at the beginning and at the end of the treatment by dual-energy X-ray absorptiometry (LUNAR Prodigy Advanced, GE Healthcare Lunar, Madison, WI, USA) equipped with appropriate software for whole-body, lumbar spine, hip, and forearm BMD. Densitometer stability was evaluated by performance of phantom scans on the dates of all data acquisition. The precision of this technique, presented as the coefficient of variation (CV), was 0.65 % for the lumbar spine, 0.73 % for the total hip, 0.85 % for forearm, and 0.55 % for total body locations.
Serum bone marker measurements
Venous blood samples were obtained after an overnight fast from each subject at baseline, 3 months, and 6 months of the study for various analyses. Blood samples were centrifuged at 1200 g for 15 min at 4 °C, and serum samples were separated, divided into aliquots, and stored at −80 °C until analyses. Changes in high-sensitivity C-reactive protein (hs-CRP), IGF-1, BAP, TRAP-5b, and sclerostin were analyzed at baseline, 3 months, and 6 months. Changes in 25-hydroxy vitamin D (25-OH vitamin D), RANKL, calcium, phosphorous, and OPG level were analyzed at baseline and 6 months. Serum total RANKL, OPG, hs-CRP, and IGF-1 were measured using ELISA kits from ALPCO Diagnostics (Salem, NH, USA). Total BAP, TRAP-5b, 25-OH vitamin D, and sclerostin levels were measured using ELISA kits from QUIDEL Corporation (San Diego, CA, USA). Calcium and phosphorous were measured using Stanbio reagents (Stanbio Laboratory, Boerne, TX).
Statistical analysis
Data were analyzed using analysis of variance methods with PROC MIXED in PC SAS (Version 9.1, SAS Institute, Cary, NC) analyzing the main and interaction effects of the two factors, treatment (0, 50, or 100 g/day dried plum), and time (baseline, 3 months, and 6 months). Since each subject was measured at baseline and various time intervals, repeated measures models were utilized. The mean changes in each time point for the treatment groups were compared by analyzing interaction effects of the two factors, treatment and time, using the SLICE option in an LSMEANS statement. Data are reported as least square mean ± standard error (SE). Unless otherwise indicated, P < 0.05 was regarded as statistically significant.
Results
Baseline characteristics, anthropometric measurements, dietary intake, and physical activity assessments
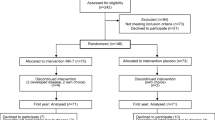
Forty-two women (13 on 0 g/day dried plum, 16 on 50 g/day dried plum, and 13 on 100 g/day dried plum) completed the study. The attrition rate was 18.75 % for 0 g/day, 0 % for 50 g/day, and 18.75 % for 100 g/day (Fig. 1). As expected, baseline characteristics were not significantly different for women who completed the study (Table 1). Age, last menstrual period age, height, body weight, and BMI were similar at baseline and between the three treatment groups. The 42 participants who remained in the study adhered to the regimens, as indicated by a self-monitoring calendar provided to them on a monthly basis. Overall, the dried plum treatment at both doses of 50 and 100 g/day was well accepted and considered to be palatable, as stated by the subjects. The compliance to the dried plum regimens was on average 95 % for 50 g dried plum and 97 % for 100 g dried plum group. Analysis of the 3-day food records indicated that the participants’ food intakes were not significantly different from their corresponding baseline values between the three treatment groups throughout the study period (Table 2). Physical activity levels were assessed at baseline and there were no significant differences in activity levels between the treatment groups (Table 1). Additionally, total calcium and vitamin D intake were evaluated at baseline using calcium and vitamin D intake history questionnaire, and similarly, there were no significant differences in calcium and vitamin D intake between treatment groups (Table 1). Glomerular filtration rate (GFR) was calculated using serum creatinine level, age, race, and gender (National Kidney Foundation) to evaluate kidney function. All participants had GFR values over 60 mL/min/1.73 m2 indicating healthy kidney function before and after the treatment.

Flowchart of the study design and study participants
Bone mineral density
Both 50 g/day dried plum and 100 g/day dried plum had bone-protective effects as indicated by no net change from baseline in total body BMD, whereas the control group continued to lose bone (Fig. 2). Although the observed changes from baseline for BMD of L1 to L4 were not significantly (P = 0.08) different than the control group, there was a strong positive trend for increased spine BMD for both 50 g/day dried plum and 100 g/day dried plum treatment groups. There were no detectable differences in changes for the total hip and ulna BMD among control, 50 g/day dried plum, or 100 g/day dried plum groups.

Bone mineral density (BMD) changes (ratio) from baseline of total body, total hip, L1 to L4, and ulna after 6 months of consumption of 0, 50, and 100 g of dried plum. Bars represent mean ± SE. * = different from 0 g (control; P < 0.05)
Serum bone markers
Mean serum concentrations of biomarkers of bone metabolism, BAP, TRAP-5b, sclerostin, IGF-1, and hs-CRP (a marker of inflammation) are presented in Table 3. Both 50 g/day and 100 g/day dried plum consumption resulted in a reduction in serum TRAP-5b levels, a marker of bone resorption, at 3 months compared to baseline, and this was sustained throughout the study (Table 3) while there were no significant changes in serum TRAP-5b levels in the control group (0 g/day dried plum). Mean IGF-1 levels decreased significantly in the control group while they did not change in dried plum groups over time (Table 3). Mean serum levels of BAP, sclerostin, and hs-CRP were not significantly different at any time point between groups or on a time-wise basis (Table 3).
The changes of BAP/TRAP-5b ratio were not significantly different in the control group but this ratio increased at 6 months in the 50 g/day (P = 0.02) and 100 g/day (P = 0.01) dried plum groups (Table 3).
There were no significant differences in mean serum levels of RANKL, OPG, 25-OH vitamin D, calcium, and phosphorous in 50 and 100 g dried plum groups during the 6-month treatment period (Table 3). Similarly, no significant changes were observed for the RANKL/OPG ratio.
Discussion
We previously showed that the daily consumption of 100 g of dried plum (equivalent to 10 to 12 dried plums) prevented bone loss in healthy, osteopenic postmenopausal women over a period of 12 months [14]. Nonetheless, consuming this amount on a daily basis may be an unrealistic expectation for individuals aiming to improve their bone health. Hence, the intent of the present study was to examine whether a lower dose (i.e., 50 g) of dried plum would also exert similar bone-protective effects in older osteopenic postmenopausal women. As hypothesized, our results confirmed that consuming 50 and 100 g of dried plum per day effectively prevented the loss of BMD of the total body and L1–L4 in postmenopausal women, albeit values were only statistically significantly different from changes in the control group for the total body. Although the exact mechanisms of action by which dried plum prevents bone loss are still unknown, previous research indicates that dried plum may modify bone formation [9–11, 17] and bone resorption [12, 14] through modulation of osteoblast and osteoclast activities. In order to further understand the mechanisms of action by which dried plum prevents bone loss in humans, the current study evaluated its effects on several biomarkers indicative of bone health. Our results showed that TRAP-5b, an enzyme involved in bone resorption [22–24], was reduced by both doses of dried plum at 3 months and that these reduced levels were maintained at 6 months. Another observation in the present study was that the ratio of BAP/TRAP-5b was significantly greater in both dried plum groups in comparison with the control group. The reason for this observation is likely that the levels of TRAP-5b were reduced and maintained at 3 and 6 months, respectively, in both dried plum groups while BAP levels remained constant in all groups throughout the course of the study. These findings suggest that dried plum may have prevented bone loss through reductions in bone resorption. Simonavice et al. [25] investigated the effects of daily consumption of 90 g dried plum and resistance training on bone health in postmenopausal breast cancer survivors (stages 0–III) and also observed similar changes in serum TRAP-5b levels after 6 months. Contrary to the abovementioned findings, our initial 3-month clinical study examining dried plums and bone health [13] demonstrated that dried plum consumption led to significantly improved serum levels of biochemical markers of bone formation (i.e., IGF-1 and BAP), whereas there were no changes in the control group or in serum (i.e., TRAP-5b) and urinary (i.e., deoxypyridinoline and helical peptide) biochemical markers of bone resorption. At the time of this study, the results suggested that dried plum had positive effects on bone formation without influencing bone resorption. Yet, with the exception of TRAP-5b and the BAP/TRAP-5b ratio, all measured biomarkers were not found to be altered by dried plum consumption in the current study. The authors cannot offer an explanation for this observation other than the fact that blood biomarkers may not be fully indicative of what is happening at the cellar level [26]. Hence, these biomarkers should be interpreted with caution and greater value should be placed on the resulting BMD values as they are more clinically relevant.
Dried plums are rich in traditional nutrients including vitamin K, potassium, magnesium, and boron, as well as bioactive compounds including chlorogenic acid and neochlorogenic acid, which are potent antioxidants [27]. These nutrients and non-nutrients and their associated physiological functions are known to be important for bone health [28] and are key reasons that the bone-protective effects of dried plum have been evaluated. It is not currently known which compounds in dried plum are responsible for their bone-protective effects or whether the whole food is required to provide the most protection against bone loss. Although the current study was not designed to evaluate this, based on the results of the present study, it is suggested that the nutrients responsible for the bone-protective effects of dried plum may hit a threshold at 50 g, since a dose-dependent effect was not observed above this dose. This indicates that doses lower than 50 g/day should be evaluated for their impact on bone health.
There are several possible limitations in the current study. First, a 6-month intervention is not an ideal length of time to see intervention-induced effects on bone density; therefore, future studies should be longer in duration. Second, the population was restricted to older, osteopenic postmenopausal women, and limits extrapolation to other populations. Third, the study was not designed to evaluate the bone-protective effects of specific bioactive compounds present in dried plum vs. the whole food, and future studies should be designed to evaluate this. Fourth, measurements of serum biomarkers were limited in the current study and other serum biomarkers of bone formation (e.g., procollagen type 1N-terminal propeptide [P1NP]) and bone resorption (e.g., collagen type 1 C-telopeptide [CTX]) and urinary biomarkers (e.g., calcium, potassium, and phosphorus) were not assessed and should therefore be considered as a limitation.
In conclusion, the results of the current study suggest that daily consumption of 50 g of dried plum for 6 months may be as effective as 100 g of dried plum in preventing bone loss in older, osteopenic postmenopausal women. These findings may, in part, be attributed to the inhibition of bone resorption as noted by improvements in TRAP-5b, therefore allowing bone formation to continue as indicated by an improvement in the BAP/TRAP-5b ratio. Longer-term studies are necessary to confirm the findings of this study as bone studies of less than 1 year are typically not considered optimal when measuring treatment effects on BMD. Therefore, conducting a study 1 year in duration or longer with a larger sample size may result in significant differences in sites such as the spine as well as greater improvements in total body BMD. Overall, these findings are very promising and further confirm the bone-protective effects of dried plum in older, osteopenic postmenopausal women.
Abbreviations
- BMD:
-
Bone mineral density
- TRAP-5b:
-
Tartrate-resistant acid phosphatase-5b
- BAP:
-
Bone-specific alkaline phosphatase
- 25-OH vitamin D:
-
25-hydroxy vitamin D
- IGF-1:
-
Insulin-like growth factor-1
- hs-CRP:
-
High-sensitivity C-reactive protein
- RANKL:
-
Receptor activator of nuclear factor kappa-B ligand
- OPG:
-
Osteoprotegerin
- SOST:
-
Sclerosteosis gene
- CRP:
-
C-reactive protein
- P1NP:
-
Procollagen type 1N-terminal propeptide
- CTX:
-
Collagen type 1 C-telopeptide
References
Colón-Emeric CS, Saag KG (2006) Osteoporotic fractures in older adults. Best Pract Res Clin Rheumatol 20(4):695–706
Looker AC, Melton LJ, Harris TB, Borrud LG, Shepherd JA (2010) Prevalence and trends in low femur bone density among older US adults: NHANES 2005–2006 compared with NHANES III. J Bone Miner Res 25(1):64–71
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22(3):465–75
Sambrook PN, Chen JS, Simpson JM, March LM (2010) Impact of adverse news media on prescriptions for osteoporosis: effect on fractures and mortality. Med J Aust 193(3):154–6
Reid IR (2015) Short-term and long-term effects of osteoporosis therapies. Nat Rev Endocrinol 11(7):418–28
Cúneo F, Costa-Paiva L, Pinto-Neto AM, Morais SS, Amaya-Farfan J (2010) Effect of dietary supplementation with collagen hydrolysates on bone metabolism of postmenopausal women with low mineral density. Maturitas 65(3):253–7
Moyer VA (2013) Vitamin D and calcium supplementation to prevent fractures in adults: US preventive services task force recommendation statement. Ann Intern Med 158(9):691–696
Ferrari CK (2007) Functional foods and physical activities in health promotion of aging people. Maturitas 58(4):327–39
Deyhim F, Stoecker BJ, Brusewitz GH, Devareddy L, Arjmandi BH (2005) Dried plum reverses bone loss in an osteopenic rat model of osteoporosis. Menopause 12(6):755–62
Arjmandi BH, Lucas EA, Juma S, Soliman A, Stoecker BJ, Khalil DA, Smith BJ, Wang C (2001) Dried plums prevent ovariectomy-induced bone loss in rats. JANA 4(1):50–6
Bu SY, Lucas EA, Franklin M, Marlow D, Brackett DJ, Boldrin EA, Devareddy L, Arjmandi BH, Smith BJ (2007) Comparison of dried plum supplementation and intermittent PTH in restoring bone in osteopenic orchidectomized rats. Osteoporos Int 18(7):931–42
Franklin M et al (2006) Dried plum prevents bone loss in a male osteoporosis model via IGF-I and the RANK pathway. Bone 39(6):1331–42
Arjmandi BH, Khalil DA, Lucas EA, Georgis A, Stoecker BJ, Hardin C, Payton ME, Wild RA (2002) Dried plums improve indices of bone formation in postmenopausal women. J Womens Health Gend Based Med 11(1):61–68
Hooshmand S, Chai SC, Saadat RL, Payton ME, Brummel-Smith K, Arjmandi BH (2011) Comparative effects of dried plum and dried apple on bone in postmenopausal women. Br J Nutr 106(06):923–930
Mühlbauer RC, Lozano A, Reinli A, Wetli H (2003) Various selected vegetables, fruits, mushrooms and red wine residue inhibit bone resorption in rats. J Nutr 133(11):3592–3597
Vinson JA J, Zubik L, Bose P, Samman N, Proch J (2005) Dried fruits: excellent in vitro and in vivo antioxidants. Am Coll Nutr 24(1):44–50
Rendina E, Hembree KD, Davis MK, Marlow D, Clarke SL, Halloran BP, Lucas EA, Smith BJ (2013) Dried plum’s unique capacity to reverse bone loss and alter bone metabolism in postmenopausal osteoporosis model. PLoS One 8(3):e60569
Hooshmand S, Kumar A, Zhang JY, Johnson SA, Chai SC, Arjmandi BH (2015) Evidence for anti-inflammatory and antioxidative properties of dried plum polyphenols in macrophage RAW 264.7 cells. Food Funct 6(5):1719–25
Bu SY, Hunt TS, Smith BJ (2009) Dried plum polyphenols attenuate the detrimental effects of TNF-alpha on osteoblast function coincident with up-regulation of Runx2, Osterix and IGF-I. J Nutr Biochem 20(1):35–44
Rendina E, Lim YF, Marlow D, Wang Y, Clarke SL, Kuvibidila S, Lucas EA, Smith BJ (2012) Dietary supplementation with dried plum prevents ovariectomy-induced bone loss while modulating the immune response in C57BL/6J mice. J Nutr Biochem 23(1):60–8
Hooshmand S, Brisco JR, Arjmandi BH (2014) The effect of dried plum on serum levels of receptor activator of NF-kappaB ligand, osteoprotegerin and sclerostin in osteopenic postmenopausal women: a randomised controlled trial. Br J Nutr 112(1):55–60
Szulc P, Bauer DC, Eastell R (2013) Biochemical markers of bone turnover in osteoporosis, in primer on the metabolic bone diseases and disorders of mineral metabolism. John Wiley & Sons, Inc, pp 297–306
Bolarin D (1996) Biochemical markers for the assessment of skeletal growth in children. Nig Quart J Hosp Med 6:256–261
Gundberg C, Looker AC, Nieman SD, Calvo MS (2002) Patterns of osteocalcin and bone specific alkaline phosphatase by age, gender, and race or ethnicity. Bone 31(6):703–708
Simonavice E, Liu PY, Ilich JZ, Kim JS, Arjmandi BH, Panton LB (2014) The effects of a 6-month resistance training and dried plum consumption intervention on strength, body composition, blood markers of bone turnover, and inflammation in breast cancer survivors. Appl Physiol Nutr Metab 39(6):730
Seeman E, Nguyen TV (2015) Bone remodeling markers: so easy to measure, so difficult to interpret. Osteoporos Int.
Mubarak A, Swinny EE, Ching SY, Jacob SR, Lacey K, Hodgson JM, Croft KD, Considine MJ (2012) Polyphenol composition of plum selections in relation to total antioxidant capacity. J Agric Food Chem 60(41):10256–62
Hooshmand S, Arjmandi BH (2009) Viewpoint: dried plum, an emerging functional food that may effectively improve bone health. Ageing Res Rev 8(2):122–127
Acknowledgments
We gratefully acknowledge the valuable assistance of the following students at San Diego State University: Mariana Beleche, Sofie Blicher, Jayme Brisco, Bich Thuy Callens, Zachary Clayton, Amanda Cravinho, Jennifer Cullison, Sofia Garcia, Jackie Gaylis, Montserrat Gonzalez, Mairi McLachlan, Tasnim El Mezain, Rose Miller, Ivette Navarro, Dawn Ortiz and, Yenina Vereda. This project was supported by the SDSU Research Foundation grant no. 242409 and a grant from the California Dried Plum Board (grant no. 57114A). The authors thank the California Dried Plum Board for providing us with dried plums and we gratefully acknowledge Nutrisystem, Inc. supplying calcium and vitamin D supplements for the study. The authors’ responsibilities were as follows: SH, MK, and BHA designed the research; SH, DM, and PS conducted the research; SH, MK, and SCC analyzed data; MEP performed statistical analysis; SH, DM, PS, SAJ, and BH wrote the paper; MK, SAJ, and BHA had substantial involvement in manuscript revision before submission; SH had primary responsibility for final content. All authors edited and approved the final version. Shirin Hooshmand, Dina Metti, Pouneh Shamloufard, Mark Kern, Bahram H. Arjmandi, Sheau C. Chai, Sarah A. Johnson, and Mark E. Payton declared that they had no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The Institutional Review Board at San Diego State University approved all procedures involving human subjects. Written informed consent was obtained from all subjects.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Hooshmand, S., Kern, M., Metti, D. et al. The effect of two doses of dried plum on bone density and bone biomarkers in osteopenic postmenopausal women: a randomized, controlled trial. Osteoporos Int 27, 2271–2279 (2016). https://doi.org/10.1007/s00198-016-3524-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3524-8