
Abstract
Summary
Falls and fractures share several common risk factors. Although past falls is not included as an input variable in the FRAX calculator, we demonstrate that FRAX probability predicts risk of incident falls in the MrOs Sweden cohort.
Introduction
Although not included in the FRAX® algorithm, it is possible that increased falls risk is partly dependent on other risk factors that are incorporated into FRAX. The aim of the present study was to determine whether fracture probability generated by FRAX might also predict risk of incident falls and the extent that a falls history would add value to FRAX.
Methods
We studied the relationship between FRAX probabilities and risk of falls in 1836 elderly men recruited to the MrOS study, a population-based prospective cohort of men from Sweden. Baseline data included falls history, clinical risk factors, bone mineral density (BMD) at femoral neck, and calculated FRAX probabilities. Incident falls were captured during an average of 1.8 years of follow-up. An extension of Poisson regression was used to investigate the relationship between FRAX, other risk variables, and the time-to-event hazard function of falls. All associations were adjusted for age and time since baseline.
Results
At enrolment, 15.5 % of the men had fallen during the preceding 12 months (past falls) and 39 % experienced one or more falls during follow-up (incident falls). The risk of incident falls increased with increasing FRAX probabilities at baseline (hazard ratio (HR) per standard deviation (SD), 1.16; 95 % confidence interval (95%CI), 1.06 to 1.26). The association between incident falls and FRAX probability remained after adjustment for past falls (HR per SD, 1.12; 95%CI, 1.03 to 1.22). High compared with low baseline FRAX score (>15 vs <15 % probability of major osteoporotic fracture) was strongly predictive of increased falls risk (HR, 1.64; 95%CI, 1.36 to 1.97) and remained stable with time. Whereas past falls were a significant predictor of incident falls (HR, 2.75; 95%CI, 2.32 to 3.25), even after adjustment for FRAX, the hazard ratio decreased markedly with increasing follow-up time.
Conclusions
Although falls are not included as an input variable, FRAX captures a component of risk for future falls and outperforms falls history with an extended follow-up time.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Falls are common in the elderly, with the prevalence of prior falls estimated as 42 % in community-dwelling people aged 75 years or more [1]. They are a major public health concern in terms of morbidity/quality of life, mortality, and cost to health and social services. Elders with injuries following falls have a subsequent increase in requirement for institutional care, decline in functional status, and increased use of medical services [1]. Although 5–10 % of falls in older adults lead to skeletal injury [1], there is limited evidence that an intervention aimed at reducing falls will lead to a subsequent reduction in fractures [2, 3]. Indeed, a lack of uniformly reliable data [4, 5], and a dearth of evidence indicating that fracture risk attributable to falls risk might be amenable to pharmacological treatment [6] meant that “past falls” was not incorporated as an input variable to the FRAX calculator. In contrast, two other fracture risk tools, both generated from single cohorts [7–9], do incorporate past falls. Since falls and fractures share many of the same risk factors, for example, increasing age, smoking, alcohol consumption, and frailty [1, 5, 10–12], we hypothesized that baseline fracture probability, as calculated by FRAX, would predict risk of future falls, and tested this hypothesis in the MrOS Sweden cohort.
Methods
Participants
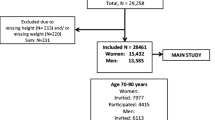
MrOS is a multi-center, prospective cohort study of elderly men in Sweden, Hong Kong, and the USA [13]. The present study is based on data from MrOS Sweden, details of which have been described previously [14, 15]. In brief, men aged 69–81 years were randomly identified using national population registers. To be eligible for the study, men had to be able to walk without aid, provide self-reported data, and give written informed consent. There were no other exclusion criteria, other than bilateral hip arthroplasty. The participation rate in MrOS Sweden was 45 %. The MrOS Sweden cohort comprises 3014 men of whom 2989 (99 %) had information on past and incident falls. The number of men who had sufficient information to estimate FRAX probability was 1853 (61 %). The present analysis is based on 1836 men with data on past falls, FRAX probability, and incident falls up to 3 years post-enrolment.
Exposure variables
At baseline, height (centimeters) and weight (kilograms) were measured, and BMI was calculated as kilograms per square meter. The international MrOS questionnaire [13] was administered at baseline to collect information about current smoking, number and type of medications, fracture history, family history of hip fracture, past medical history (rheumatoid arthritis) and high consumption of alcohol (three or more glasses of alcohol-containing drinks per day), calculated from the reported frequency, and amount of alcohol use. Previous fracture at baseline was documented as forearm, vertebral, hip, or humerus fractures after the age of 50 years regardless of trauma. For glucocorticoid exposure, this was documented in MrOs as use at least three times per week in the month preceding the baseline assessment. Apart from rheumatoid arthritis, there was no information on secondary causes of osteoporosis, and the input variable was set to no for all men. Self-reported falls during the 12 months preceding the baseline were recorded by questionnaire (past falls). Areal bone mineral density (BMD) was measured at the femoral neck using Hologic QDR 4500/A-Delphi (Hologic, Bedford, MA) or Lunar Prodigy (GE Lunar Corp., Madison, WI) depending on center, with cross-calibration of instruments. A T-score was calculated using NHANES young women as a reference value [16].
Ten-year probability of fracture (FRAX) was calculated using clinical risk factors described above with and without femoral neck BMD. As the gradients of risk for incident falls were very similar with either model, results for the models without femoral neck BMD are presented. The Swedish FRAX model version 3.8 was used. The FRAX probability of fracture estimates the risk of a hip fracture alone and of a major osteoporotic fracture (hip, humerus, vertebral, or forearm fracture).
Outcomes
Information on falls during follow-up was recorded by participants in a diary and collated by triannual postcards (incident falls), with falls assumed to happen halfway between visits. Thus, if a fall was reported at 8 months, the fall was assumed to have occurred halfway between the fourth and eighth-month visit, i.e., at 6 months. Twenty-six percent of men had gaps in their reporting of the diaries. In the primary analysis, follow-up time during the gap was ignored; thus, neither the observation time nor the information of endpoint was used during the time of the gap, and so missing diaries were defined as “no fall.” Two sensitivity analyses were undertaken: First, the end of follow-up was defined as the time of the first missing diary entry, and second, all diaries were used regardless of missing entries. Deaths were documented from the National Cause of Death Register up to the end of 2009. This register comprises records of all deaths in Sweden and is more than 99 % complete. Emigrants were followed up to the day of emigration. Participants were followed until death, migration, fall, or end of study.
Statistical methods
In order to compare the performance of FRAX probability with that of a history of past falls, a dichotomous variable was created such that the percentage of men who had a high fracture risk was similar to the percentage who had had previously fallen (15.4 %). Thus, 283 men (15.4 %) had a FRAX probability of major osteoporotic fracture, calculated without BMD, above 15.0 %, and the dichotomized FRAX score was therefore classified as high (>15.0 %) or low (≤15.0 %) risk. Fisher’s permutation test was used to compare baseline variables in men with and without falls at baseline. An extension of Poisson regression models [17] was used to study the association between FRAX, other risk variables, and the future risk of falling. All associations were adjusted for age and time since baseline. In contrast to logistic regression, the Poisson regression utilizes the length of each individual’s follow-up period and the hazard function is assumed to be exp(β0 + β1·current time from baseline + β2·current age + β3 variable of interest). The observation period of each participant was divided in intervals of 1 month. One fall per person, and time to the first fall were counted. In further analyses, time to subsequent falls (up to the seventh fall) was counted. Where interactions with age and time since baseline were explored, age and time were used as continuous variables and examples given at specific ages and times. The association between predictive factors and risk of falls was described as a hazard ratio (HR) or gradient of risk (GR = HR per 1 standard deviation change in predictor in the direction of increased risk). The distribution of FRAX probabilities was transformed to be a normally distributed variable using the inverse of the standardized normal distribution function, so comparability could be achieved to other variables described using GR. The cut off value for high (>15.0 %) or low (≤15.0 %) fracture probability is, fortuitously, consistent with Swedish assessment guidelines [18]. Two-sided p values were used for all analyses and p < 0.05 was considered to be significant.
Results
Characteristics of participants
Compared with the 1178 men not included in the current analysis, the 1836 men included were similar in terms of age (p = 0.14), BMD T-score (p > 0.30), and occurrence of past falls (p = 0.070). The mean follow-up time was 1.8 years (range, 0.0 to 3.0 years) after the baseline examination. Men with past falls (n = 284, 15.5 %) had a higher prevalence of previous fracture and parental history of hip fracture, together with higher FRAX probabilities (Table 1). A total of 720 men experienced one or more incident falls during follow-up. Thirty-nine percent had ≥1 fall, 20 % had ≥2 falls, 11 % had ≥3 falls, 6 % had ≥4 falls, 4 % had ≥5 falls, 2 % had ≥6 falls, and 2 % had ≥7 falls. Men who fell during follow-up had a higher baseline prevalence of previous fracture, past falls, alcohol use, and higher FRAX probabilities (Table 2).
Risk factors for incident falls
The risk of new falls rose with increasing FRAX probabilities at baseline (HR per standard deviation (SD), 1.16; 95 % confidence interval (95%CI), 1.06 to 1.26). The association between incident falls and FRAX probability remained after adjustment for past falls (HR per SD, 1.12; 95%CI, 1.03 to 1.22, Table 3) and appeared to strengthen with increasing number of incident falls (Table 4). When the FRAX probability of osteoporotic fracture was calculated without the use of BMD, men with a high fracture probability (>15.0 %) had greater risk for future falls than men with low (≤15 %) baseline probability (HR, 1.64; 95%CI, 1.36 to 1.97). The risk of incident falls was greater when there was a past fall recorded at baseline (HR, 2.75; 95%CI, 2.32 to 3.25). The association between incident and past falls remained after adjustment for FRAX probabilities (HR, 2.68; 95%CI, 2.26 to 3.18, Table 3). Sensitivity analyses with regard to falls history, as described in the “Methods” section, yielded results very similar to those from the primary analysis.
Interactions with age and time from baseline
The gradient of risk for past falls predicting incident falls decreased with age, but the formal interaction between occurrence of past falls and age was not statistically significant (p = 0.19). At 70 years, the HR for incident falls in the past fallers compared with that in past non-fallers was 3.44 (95%CI, 2.38 to 4.99), and at 80 years, the HR was 2.43 (95%CI, 1.88 to 3.12). Conversely, the predictive ability of high versus low FRAX probability for incident falls increased with age although, again, the interaction did not achieve formal statistical significance (p = 0.055). At the age of 70 years, the HR for incident falls in participants with high compared with low baseline fracture probability was 1.03 (95%CI, 0.61 to 1.74), and at 80 years, the HR was 1.93 (95%CI, 1.50 to 2.49).
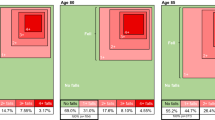
The prediction of incident falls using past falls and FRAX probability differed in their relationship with time since participant enrolment. Thus, the predictive ability of past falls for incident falls decreased markedly with time since baseline (p = 0.002), such that after 1-year follow-up, the HR for incident falls was 2.68 (95%CI, 2.25 to 3.19) and, after 3 years, the HR was 1.31 (95%CI, 0.78 to 2.19). In contrast, the predictive ability of high versus low FRAX probability at baseline appeared to be stable with time (p for interaction between fracture probability and time >.30): After 1 year, the HR for incident falls among participants with high compared with low baseline FRAX probability was 1.64 (95%CI, 1.36 to 1.97), and after 3 years, this was 1.62 (95%CI, 0.99 to 2.64; Fig. 1).

Hazard ratio (95 % confidence interval) for the association between baseline falls, FRAX, and the risk of incident falls with increasing follow-up time. Past falls are classified as yes/no; FRAX is dichotomized to FRAX probability of major osteoporotic fracture calculated without BMD above or below 15 % (high/low fracture risk). Associations are adjusted for age and current time
Discussion
These results demonstrate that both baseline probability of future fracture, as calculated by FRAX, and a history of past falls independently predict risk of future falls. However, the predictive power of these two indices with increasing follow-up time contrasted markedly. The risk associated with baseline FRAX probability appeared stable over time, in contrast to that associated with past falls, which attenuated over 3 years of follow-up. Thus, although past falls do not constitute an input variable in the FRAX algorithm, the fracture probability generated appears to include a component of incident falls risk.
Although falls and fractures are closely linked, to our knowledge, this is the first study in which the probability of future fracture has been shown to also predict risk of incident falls. Many previous studies, in different populations, have documented strong associations between propensity to fall and risk of future fracture [10, 11, 19–26]. Indeed, most non-vertebral low-trauma fractures occur as a result of a fall from standing height or less [27], and a history of multiple falls increases the fracture risk over a single fall in any given time span [10, 22]. In a recent UK study from the Hertfordshire Cohort [28], in a subset of 368 men and 407 women, the hazard ratio for fracture associated with a history of past falls was 6.96 (95%CI, 2.42 to 20.01) for men, and 2.64 (95%CI, 1.21 to 5.78) for women, independently of femoral neck BMD and clinical risk factors used in FRAX. The present findings complement these results by demonstrating that in addition to the explanatory power associated with previous falls, the fracture probability generated by FRAX also explains part of the risk for future falls, independently of past falling. The disparity between hazard ratio for men and women in the Hertfordshire study [28] may suggest that male fallers are frailer and therefore more likely to fracture. The current analysis was undertaken only in men, and we were unable, therefore, to identify whether there might be sex-specific differences in the gradient of risk between FRAX probability and falls incidence. In the Hertfordshire study, stratification of fracture risk by frequency of previous falls was not documented; this has been demonstrated elsewhere, albeit not in relation to FRAX, generally with a positive relationship between increasing number of falls in the past and increased fracture probability in the future [5, 24, 25]. Indeed, we documented an increasing gradient of risk between FRAX and falls, as the number of incident falls increased. Importantly, for long-term risk assessment, although both FRAX probability and prior history of falls independently predicted risk of future falls, the gradient of risk for FRAX predicting falls was stable through follow-up. In contrast, the gradient of risk for past fall predicting incident fall was initially greater than that for FRAX but attenuated with increasing follow-up time, such that at 3 years, the gradient of risk was similar to that with FRAX. These findings suggest that history of past falls is likely to provide less robust predictive power than FRAX over longer periods.
Calculation of hazard ratios for incident falls associated with individual clinical risk factors and hip BMD allowed us to elucidate which individual risk factors might account for the majority of the predictive power of the FRAX probability for incident fall. The hazard ratio for previous fracture was similar to that for previous falls, and although alcohol intake of three or more units per day was a statistically significant predictor of fractures, a finding consistent with previous data [1, 5, 12, 24], overall there was no one clear individual risk factor which dominated the predictive model. Thus, for all risk factors other than current smoking and rheumatoid arthritis, the hazard ratio was at least 1.2 and the predictive power of the overall FRAX score appeared to comprise contributions from the majority of contained variables. Interestingly, femoral neck BMD T-score was only weakly associated with falls risk, and so the risk gradient for future falls associated with FRAX probability was similar whether BMD was included or excluded from the calculations. Given the narrow age range in this male cohort, it may be that we had insufficient power to detect a statistically significant effect here.
The history of falls and FRAX has been well documented [5]. Thus, although it is possible to incorporate falls into risk calculators derived from single cohorts in which these outcomes have been recorded accurately [7–9, 29, 30], the lack of standardized documentation of fall events across the 20 cohorts used in the development of the FRAX tool has meant that the use of prior falls as a clinical risk factor was not possible. An additional consideration is that, although there have been several studies demonstrating the efficacy of multi-modal interventions for the prevention of falls [31–36], there is only limited evidence that such approaches might lead to a reduction in fractures [2, 3, 5]. Furthermore, there is little evidence that falls risk is amenable to intervention with pharmacological agents such as bisphosphonates, one of the founding premises of the FRAX methodology [4, 5]. Baseline risk of falling, however, did not appear to alter anti-fracture efficacy of clodronate in one study [37]. There has been much debate over recent years as to whether previous falls could be directly incorporated into FRAX, and the above limitations suggest that currently they could not, in any meaningful sense. However, guidance on the incorporation of the increased fracture risk associated with previous falls has been published [4], and so FRAX probability of future fracture may be inflated by 30 % (multiplied by 1.3) in a person with a history of falls. Our results complement this approach by demonstrating that a component of the risk associated with falls is contained within FRAX probability, independently of previous falls and in the absence of falls as an input variable. Our present results therefore inform clinical care, demonstrating that those assessed as at high risk of fracture are likely to be at increased risk of falls and that further clinical assessment may be required to ameliorate this risk. Further prospective studies in cohorts with wider age ranges, other ethnicities, and most importantly women are now warranted to replicate and extend these findings.
We studied a well-characterized cohort drawn from the general population with prospective recording of falls. However, there are some limitations that should be considered in the interpretation of our findings [38]. First, the population studied was male, and of a narrow age range (69–81 years), so limiting generalizability of our findings. Second, data on incident falls were missing in some participants. However, we explored a number of different methods for imputing these missing falls data, all of which yielded similar results. Third, the definition of prior fracture and glucocorticoid use differed from those usually specified for incorporation into FRAX. Furthermore, there was no information on causes of secondary osteoporosis, and this variable was therefore set to missing. The effect of these considerations on our findings is uncertain but may have led to an overall underestimation of risk. Finally, we did not have information on the severity of a fall, or whether fall was associated with injury. However, we did document an increasing gradient of risk between baseline FRAX probability and number of incident falls.
In conclusion, we have demonstrated that the baseline probability of future fracture, calculated using FRAX clinical risk factors with or without BMD, identifies those at increased risk of falling, and unlike history of falls, the risk identified is stable with follow-up time. Thus, although previous falls are not explicitly included in the FRAX calculation, part of the risk associated with falls is captured and therefore will inform stratification of future fracture risk.
References
Masud T, Morris RO (2001) Epidemiology of falls. Age Ageing 30(Suppl 4):3–7
Cameron ID, Gillespie LD, Robertson MC, Murray GR, Hill KD, Cumming RG, Kerse N (2012) Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev 12:CD005465. doi:10.1002/14651858.CD005465.pub3
Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, Lamb SE (2012) Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 9:CD007146. doi:10.1002/14651858.CD007146.pub3
Kanis JA, Hans D, Cooper C, Baim S, Bilezikian JP, Binkley N, Cauley JA, Compston JE, Dawson-Hughes B, El-Hajj Fuleihan G, Johansson H, Leslie WD, Lewiecki EM, Luckey M, Oden A, Papapoulos SE, Poiana C, Rizzoli R, Wahl DA, McCloskey EV (2011) Interpretation and use of FRAX in clinical practice. Osteoporos Int 22(9):2395–2411. doi:10.1007/s00198-011-1713-z
Masud T, Binkley N, Boonen S, Hannan MT (2011) Official positions for FRAX(R) clinical regarding falls and frailty: can falls and frailty be used in FRAX(R)? from joint official positions development conference of the international society for clinical densitometry and international osteoporosis foundation on FRAX(R). J Clin Densitom 14(3):194–204. doi:10.1016/j.jocd.2011.05.010
McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, Adami S, Fogelman I, Diamond T, Eastell R, Meunier PJ, Reginster JY (2001) Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 344(5):333–340. doi:10.1056/nejm200102013440503
Hippisley-Cox J, Coupland C (2009) Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ 339:b4229
Nguyen ND, Frost SA, Center JR, Eisman JA, Nguyen TV (2007) Development of a nomogram for individualizing hip fracture risk in men and women. Osteoporos Int 18(8):1109–1117. doi:10.1007/s00198-007-0362-8
Nguyen ND, Frost SA, Center JR, Eisman JA, Nguyen TV (2008) Development of prognostic nomograms for individualizing 5-year and 10-year fracture risks. Osteoporos Int 19(10):1431–1444. doi:10.1007/s00198-008-0588-0
Dargent-Molina P, Favier F, Grandjean H, Baudoin C, Schott AM, Hausherr E, Meunier PJ, Breart G (1996) Fall-related factors and risk of hip fracture: the EPIDOS prospective study. Lancet 348(9021):145–149
Geusens P, Milisen K, Dejaeger E, Boonen S (2003) Falls and fractures in postmenopausal women: a review. J Br Menopause Soc 9(3):101–106
Pearson D, Taylor R, Masud T (2004) The relationship between social deprivation, osteoporosis, and falls. Osteoporos Int J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 15(2):132–138. doi:10.1007/s00198-003-1499-8
Orwoll E, Blank JB, Barrett-Connor E, Cauley J, Cummings S, Ensrud K, Lewis C, Cawthon PM, Marcus R, Marshall LM, McGowan J, Phipps K, Sherman S, Stefanick ML, Stone K (2005) Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study—a large observational study of the determinants of fracture in older men. Contemp Clin Trials 26(5):569–585. doi:10.1016/j.cct.2005.05.006
Mellstrom D, Vandenput L, Mallmin H, Holmberg AH, Lorentzon M, Oden A, Johansson H, Orwoll ES, Labrie F, Karlsson MK, Ljunggren O, Ohlsson C (2008) Older men with low serum estradiol and high serum SHBG have an increased risk of fractures. J Bone Miner Res 23(10):1552–1560. doi:10.1359/jbmr.080518
Mellstrom D, Johnell O, Ljunggren O, Eriksson AL, Lorentzon M, Mallmin H, Holmberg A, Redlund-Johnell I, Orwoll E, Ohlsson C (2006) Free testosterone is an independent predictor of BMD and prevalent fractures in elderly men: MrOS Sweden. J Bone Miner Res 21(4):529–535. doi:10.1359/jbmr.060110
Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, Johnston CC Jr, Lindsay R (1998) Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 8(5):468–489
Breslow NE, Day NE (1987) Statistical methods in cancer research. IARC Sci Publ No 32 Volume II:p 131–135
Socialstyrelsen (2012) Nationella riktlinjer för rörelseorganens sjukdomar 2012. Osteoporos, artros, inflammatorisk ryggsjukdom och ankyloserande spondylit, psoriasisartrit och heumatoid artrit Stöd för styrning och ledning. Sweden
Albrand G, Munoz F, Sornay-Rendu E, DuBoeuf F, Delmas PD (2003) Independent predictors of all osteoporosis-related fractures in healthy postmenopausal women: the OFELY study. Bone 32(1):78–85
Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, Cauley J, Black D, Vogt TM (1995) Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med 332(12):767–773. doi:10.1056/nejm199503233321202
Wainwright SA, Marshall LM, Ensrud KE, Cauley JA, Black DM, Hillier TA, Hochberg MC, Vogt MT, Orwoll ES (2005) Hip fracture in women without osteoporosis. J Clin Endocrinol Metab 90(5):2787–2793. doi:10.1210/jc.2004-1568
Gardsell P, Johnell O, Nilsson BE, Nilsson JA (1989) The predictive value of fracture, disease, and falling tendency for fragility fractures in women. Calcif Tissue Int 45(6):327–330
Kaptoge S, Benevolenskaya LI, Bhalla AK, Cannata JB, Boonen S, Falch JA, Felsenberg D, Finn JD, Nuti R, Hoszowski K, Lorenc R, Miazgowski T, Jajic I, Lyritis G, Masaryk P, Naves-Diaz M, Poor G, Reid DM, Scheidt-Nave C, Stepan JJ, Todd CJ, Weber K, Woolf AD, Roy DK, Lunt M, Pye SR, O'Neill TW, Silman AJ, Reeve J (2005) Low BMD is less predictive than reported falls for future limb fractures in women across Europe: results from the European Prospective Osteoporosis Study. Bone 36(3):387–398. doi:10.1016/j.bone.2004.11.012
Frost M, Abrahamsen B, Masud T, Brixen K (2012) Risk factors for fracture in elderly men: a population-based prospective study. Osteoporos Int J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 23(2):521–531. doi:10.1007/s00198-011-1575-4
Sambrook PN, Cameron ID, Chen JS, Cumming RG, Lord SR, March LM, Schwarz J, Seibel MJ, Simpson JM (2007) Influence of fall related factors and bone strength on fracture risk in the frail elderly. Osteoporos Int J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 18(5):603–610. doi:10.1007/s00198-006-0290-z
Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH (2003) Interventions for preventing falls in elderly people. Cochrane Database Syst Rev 4:CD000340. doi:10.1002/14651858.CD000340
Harvey N, Dennison E, Cooper C (2010) Osteoporosis: impact on health and economics. Nat Rev Rheumatol 6(2):99–105. doi:10.1038/nrrheum.2009.260
Edwards MH, Jameson K, Denison H, Harvey NC, Sayer AA, Dennison EM, Cooper C (2013) Clinical risk factors, bone density and fall history in the prediction of incident fracture among men and women. Bone 52(2):541–547. doi:10.1016/j.bone.2012.11.006
Sambrook PN, Flahive J, Hooven FH, Boonen S, Chapurlat R, Lindsay R, Nguyen TV, Diez-Perez A, Pfeilschifter J, Greenspan SL, Hosmer D, Netelenbos JC, Adachi JD, Watts NB, Cooper C, Roux C, Rossini M, Siris ES, Silverman S, Saag KG, Compston JE, LaCroix A, Gehlbach S (2011) Predicting fractures in an international cohort using risk factor algorithms without BMD. J Bone Miner Res Off J Am Soc Bone Miner Res 26(11):2770–2777. doi:10.1002/jbmr.503
Cooper C, Harvey NC (2012) Osteoporosis risk assessment. BMJ 344:e4191. doi:10.1136/bmj.e4191
Miake-Lye IM, Hempel S, Ganz DA, Shekelle PG (2013) Inpatient fall prevention programs as a patient safety strategy: a systematic review. Ann Intern Med 158(5 Pt 2):390–396. doi:10.7326/0003-4819-158-5-201303051-00005
Martin JT, Wolf A, Moore JL, Rolenz E, DiNinno A, Reneker JC (2013) The effectiveness of physical therapist-administered group-based exercise on fall prevention: a systematic review of randomized controlled trials. J Geriatr Phys Ther (2001) 36(4):182–193. doi:10.1519/JPT.0b013e3182816045
Karlsson MK, Magnusson H, von Schewelov T, Rosengren BE (2013) Prevention of falls in the elderly—a review. Osteoporos Int J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 24(3):747–762. doi:10.1007/s00198-012-2256-7
Pfortmueller CA, Lindner G, Exadaktylos AK (2014) Reducing fall risk in the elderly: risk factors and fall prevention, a systematic review. Minerva Med 105(4):275–281
Lovarini M, Clemson L, Dean C (2013) Sustainability of community-based fall prevention programs: a systematic review. J Saf Res 47:9–17. doi:10.1016/j.jsr.2013.08.004
Gillespie LD, Robertson MC, Gillespie WJ, Lamb SE, Gates S, Cumming RG, Rowe BH (2009) Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 2:CD007146. doi:10.1002/14651858.CD007146.pub2
Kayan K, Johansson H, Oden A, Vasireddy S, Pande K, Orgee J, Kanis JA, McCloskey EV (2009) Can fall risk be incorporated into fracture risk assessment algorithms: a pilot study of responsiveness to clodronate. Osteoporos Int 20(12):2055–2061. doi:10.1007/s00198-009-0942-x
Johansson H, Oden A, Lerner UH, Jutberger H, Lorentzon M, Barrett-Connor E, Karlsson MK, Ljunggren O, Smith U, McCloskey E, Kanis JA, Ohlsson C, Mellstrom D (2012) High serum adiponectin predicts incident fractures in elderly men: Osteoporotic fractures in men (MrOS) Sweden. J Bone Miner Res 27(6):1390–1396. doi:10.1002/jbmr.1591
Acknowledgments
We thank the participants of MrOs Sweden. The study was supported by the Swedish Research Council, ALF/LUA research grants in Gothenburg, and the King Gustav V and Queen Victoria Frimurarestiftelse Research Foundation. NCH and HJ are joint first authors.
Author roles
All authors contributed to manuscript drafting, review, and finalization. NCH wrote the first draft of the manuscript and oversaw its preparation; HJ and AO undertook statistical analysis; MKK, BR, OL, CO, and DM designed and implemented MrOS Sweden and provided data; CC contributed expertise on fracture epidemiology; EM and JAK oversee FRAX and provided FRAX methodology; DM is guarantor.
Conflicts of interest
NH has received consultancy, lecture fees, and honoraria from Alliance for Better Bone Health, AMGEN, MSD, Eli Lilly, Servier, Shire, Consilient Healthcare, and Internis Pharma. JAK has received consulting fees, advisory board fees, lecture fees, and/or grant support from the majority of companies concerned with skeletal metabolism. EVM has received consultancy, lecture fees, research grant support, and/or honoraria from ActiveSignal, Alliance for Better Bone Health, AMGEN, Bayer, Consilient Healthcare, GE Lunar, Hologic, Internis Pharma, Lilly, MSD, Novartis, Pfizer, Roche, Servier, Tethys, UCB, and Univadis. CC has received consultancy, lecture fees, and honoraria from AMGEN, GSK, Alliance for Better Bone Health, MSD, Eli Lilly, Pfizer, Novartis, Servier, Medtronic, and Roche.
Author information
Authors and Affiliations
Corresponding author
Additional information
Nicholas C. Harvey and Helena Johansson are joint first authors.
Rights and permissions
About this article

Cite this article
Harvey, N.C., Johansson, H., Odén, A. et al. FRAX predicts incident falls in elderly men: findings from MrOs Sweden. Osteoporos Int 27, 267–274 (2016). https://doi.org/10.1007/s00198-015-3295-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3295-7