
Abstract
Summary
To study the cost of osteoporotic fracture in China, we performed a prospective study and compared the costs of the disease in referral patients with fractures in three of the most common sites. Our results indicated that the economic burden of osteoporotic fracture to both Chinese patients and the nation is heavy.
Introduction
This paper aims to study the cost of osteoporotic fracture in China and thus to provide essential information about the burden of this disease to individuals and society.
Methods
This prospective observational data collection study assessed the cost related to hip, vertebral, and wrist fracture 1 year after the fracture based on a patient sample consisting of 938 men and women. Information was collected using patient records, registry sources, and patient interviews. Both direct medical, direct non-medical, and indirect non-medical costs were considered.
Results
The annual total costs were highest in hip fracture patients (renminbi, RMB 27,283 or USD 4,330, with confidence interval (RMB 25715, 28851)), followed by patients with vertebral fracture (RMB 21,474 or USD 3,409, with confidence interval (RMB 20082, 22866)) and wrist fracture (RMB 8,828 or USD 1,401, with confidence interval (RMB 7829, 9827)). The direct medical care costs averaged approximately RMB 17,007 per year per patient, of which inpatient costs, drugs, and investigations accounted for the majority of the costs. Nonmedical direct costs were much less compared to direct healthcare costs and averaged approximately RMB 1,846.
Conclusion
These results indicate that the economic burden of osteoporotic fracture to both Chinese patients and China was heavy, and the proportion of the costs in China demonstrated many similar features and some significant differences compared to other countries.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoporosis (OP) and its associated fractures are highly prevalent conditions. The prevalence rate of osteoporosis in older adult ranges between 13 and 30 % for the USA and UK [1–3]. The mean prevalence of osteoporosis in adults is estimated at 13 % in China [4]. The National Institute of Health estimates that 50 % of females and 25 % of males over the age of 50 years in the USA will have an osteoporotic fracture in their remaining lifetime [5]. Due to its social and economic implications, osteoporosis is a major public health concern and has received great attention in many countries worldwide [6, 7].
An estimation of the economic burden of osteoporotic fracture is of great relevance to enable a rational distribution of healthcare resources. The socioeconomic effects of OP and its associated fractures have been intensively studied in many economically advanced countries, such as the USA, Germany, Canada, and Sweden [5, 8–10]. China may carry a large proportion of the financial burden of osteoporotic fracture because approximately 20 % of the world’s population aged 60 years and older lives in China. However, very few studies have estimated the cost of osteoporotic fracture in China. A preliminary estimate of select expenses on osteoporotic hip fracture has been determined for developed cities of China, such as Beijing [11] and Shanghai [12]. However, these studies relied on data obtained prior to 2003. As a result, these findings may no longer accurately depict the healthcare and economic outcomes of a rapidly expanding at-risk population. In addition, there has been no study on the cost of osteoporotic fracture in other developing areas of mainland China, which has a very different health insurance policy compared to Beijing or Shanghai.
To provide fresh baseline data for future evaluations of the economic effects of osteoporotic fracture on health in western China (where the prevalence rate of OP and its associated fractures is greater than in any other area of China [13]), a study collecting prospective observational data was initiated in January 2010 with the purpose of obtaining relevant estimates of the costs associated with osteoporotic fractures of the hip, vertebrae, and wrist in western China. The Costs and Effects of Osteoporosis-Related Fractures study (CEORF study) on continuously enrolled patients with a fracture at three main hospitals in western China was performed. This study followed the patients over a period of 12 months after the fracture event.
Methods
Subjects and interviews
The CEORF study included patients who had suffered from an osteoporosis-related fracture of the hip, vertebrae, or wrist and who have been treated at the orthopedics department at one of three Chinese hospitals. The participating centers included Chengdu Military General Hospital in Chengdu, West China Hospital in Chengdu, and Xijing Hospital in Xi’an. Attendees (outpatients and inpatients) were recruited between January 2010 and December 2012. A similar study design has previously been successfully used in the Swedish KOFOR study [8] and ICUROS study [14].
According to the ICD-10 diagnostic code, the fractures studied in the research include S12.0 fracture of first cervical vertebra, S12.1 fracture of second cervical vertebra, S12.2 fracture of other specified cervical vertebra, S12.7 multiple fractures of cervical spine, S22.0 fracture of thoracic vertebra, S32.0 fracture of lumbar vertebra, S62.0 fracture of navicular [scaphoid] bone of hand, S62.1 fracture of other carpal bone(s), S72.0 fracture of neck of femur, S72.1 fracture of neck of femur, and S72.2 subtrochanteric fracture.
The study was approved by the local ethics committees, including the Research Ethics Committee, Medical School of Sichuan University, Fourth Military Medical University, and Chengdu Military General Hospital, China. A written informed consent from each patient was obtained prior to enrollment in the study.
The following set of criteria was used to determine whether the patients included in the study were osteoporotic:
-
At least one mention of osteoporosis between the years 2010 and 2012 according to the ICD-10 diagnostic code1 (M80, M81).
-
Fractures occurring within 30 days prior to the first osteoporosis diagnosis or anytime thereafter. Fractures occurring up to 30 days prior to the patient’s first osteoporosis diagnosis were considered osteoporotic because osteoporosis is often undiagnosed until after the fracture occurs.
-
Fractures were confirmed using X-ray examination.
Patients seeking care for multiple fractures were not eligible for the study. Patients with diagnoses at any time in their claims history for other conditions that elevated fracture risk were excluded. Specifically, patients with diagnoses for metastatic cancer, bone cancer, multiple myeloma, and Paget’s disease of bone were excluded because these patients used specific cancer drugs (anastrozole, letrozole, exemestane, leuprorelin, goserelin, triptorelin, nafarelin, histrelin, deslorelin, flutamide, bicalutamide, nilutamide, cetrorelix, abarelix, and ganirelix) or underwent surgical castration [15, 16]. In addition, patients who were judged by the investigative orthopedists to be unable to complete the questionnaires due to dementia or other psychological problems were excluded from the study.
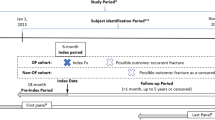
Data regarding resource use related to the fractures were collected by questionnaires given at baseline and at 4 and 12 months after fracture occurrence. Patients were further contacted by telephone after they were identified and then asked to come back to the hospital to get interviewed. Investigative orthopedists, who received uniform training on the study, interviewed all of the target patients in the outpatient clinic or inpatient wards in the orthopedics department.
The questionnaire included two main components: the first part (part I) requested patient characteristics, such as sociodemographic details, information on concurrent conditions, and the main clinical features of the fracture; Resource use and cost data were derived from the second part of the questionnaire (part II), which consisted of two sections. Part IIa assessed resource use, including drug treatment, number of outpatient visits and inpatient admissions, means of transportation to the clinic, and specific equipment. For each drug treatment, the patients were asked to provide the main reasons for not using a specific drug. The choices included the following: (1) the doctor did not recommend this drug use, (2) economic reasons, (3) the drug’s side effects and (4) other. For part IIb, the costs of inpatient care, cost of medical consultation, drugs, physical investigation, purchase of equipment needed due to the fracture, medically related travel expenses, professional home care, and productivity loss due to sick leave and early disability retirement were directly assessed. To ensure the accuracy of the recall information during the interview, the patients were accompanied by a caregiver and brought their medical records, which included their outpatient and inpatient records. The patients’ baseline characteristics, background information, and perceived health status just prior to and health status after the occurrence of the fracture were obtained. At 4- and 12-month follow-ups, information about resource use since the patients’ last visit and current health status was collected. Only data of patients with complete follow-ups were analyzed.
Estimation of costs
There are three kinds of medical security system, namely, urban basic medical insurance, basic medical insurance for urban residents, and the new rural cooperative medical care, all of which could be a co-payment of inpatient, but not for outpatient care or home help. Patients themselves pay for transportation, home care, preventive foods, and equipment. The information of the medical insurance for each patient was recorded. Because the reimbursement by the different systems is very different, both direct medical, direct non-medical, and indirect non-medical costs were considered, without considering the medical insurance reimbursement.
The annual direct costs included the diagnosis and treatment of osteoporosis and its complications, e.g., the treatment of fractures attributed to osteoporosis. The direct costs of the illness were grouped according to diagnosis (X-ray examinations, bone mineral density (BMD) measurement, etc.) or treatment (cost of medicines, medical consultations, hospitalization, equipment, etc.). The unit costs were derived from the Sichuan Province public health administration tariff for 2007 (annual listing of all licensed drugs in China and their prices), local taxi and public transportation published fares, Sichuan guidelines for mileage reimbursement, and the local fees for home care and home help service provided by the local authorities.
Indirect costs, including costs of lost working days due to visits to the hospitals, were also determined. At the baseline interview, the patients provided information on their pre-fracture working status (full time work/part-time work/not employed). At 4- and 12-month follow-up interviews, the patients provided their current working situation and, if they were working, then they reported how many days they had been on sick leave due to the fracture for those specific days (i.e., 0–4 months and 4–12 months after fracture). The daily wage for manual unskilled work (renminbi, RMB 60) was arbitrarily assigned to each working day lost, independent of the self-declared family income or patient occupation. Evaluations of productivity loss due to long-term sick leave and early retirement were based on the Sichuan Province average annual income (RMB 32,784) according to the 2012 annual statistics almanac of Sichuan. Most of the patients arrived at the hospital with an attendant. The cost related to the loss in wages for the attendant who accompanied the patient to the clinic was also included in the indirect cost. The initial valuation of cost items was represented in Chinese currency (RMB). For reference, the exchange rate was US $1 = RMB 6.3 in 2012.
Medical care resource units and unit costs are shown in Table 1 of the “Electronic supplementary material”. Non-medical resource units and unit costs are shown in Table 2 of the “Electronic supplementary material”.
Data entry and statistics
Data entry was performed using Microsoft Access database (Microsoft, 2003). Cost data were usually positively skewed, which was similar for the data obtained in this study. However, the median cost was zero for highly skewed data. Thus, the mean values and ranges were provided. Statistical analyses were performed using SPSS. For comparisons between groups, Kruskal–Wallis analysis of variance was performed. Confidence intervals for cost estimates were done using bootstrapping techniques.
Results
Patient characteristics
We studied a cohort of 1,005 consecutive patients. Of the patients in the study, 29 patients (2.9 %) dropped out after initial follow-up, and another 38 patients (3.7 %) dropped out during the subsequent 12-month period. The reason for dropout include death (16 cases), refusal to continue the follow-up (32 cases), and change of address (19 cases). Only data of patients with complete follow-ups were analyzed.
The baseline information and patient characteristics for the 938 fracture patients (437 hip fractures, 209 vertebral fractures, and 292 wrist fractures) who complete the full follow-up are shown in Table 1. A comparison on key variables between the patients included in the analyses and the dropouts is provided in Table 3 of the “Electronic supplementary material”. All participants were permanent residents of West China. The patients’ mean age was 70.6 ± 12.5 years (range, 46 to 91 years). The proportion of women exceeded 71 % in all three fracture groups. The patients’ self-declared family income was RMB 2,307 ± 548 (range, RMB 750–40,000) per month. More than half of the patients were residing in urban locations. No patient above the age of 65 years had been working prior to the fracture. The Medicare coverage in the cohort is 64.3 % (the urban basic medical insurance, 21.0 %; the basic medical insurance for urban residents, 29.0 %; the new rural cooperative medical care, 14.3 %).
Resource utilization
Medical care
The total number of diagnostic and therapeutic activities (outpatient and hospitalization) for each fracture category is shown in Table 2. The highest number of patients with medical services was patients with a hip fracture. Patients with a wrist fracture had the smallest number of diagnostic and therapeutic interventions. Medical consultations in the clinic were the most common intervention in each category. The average number of outpatient contacts with primary care and hospital medical care were 3.3 and 6.0 per patient per year, respectively. Most patients had an osteoporotic fracture related to hospitalization history. There were 751 hospitalizations for 593 patients (63 %) during the 12 months after the fracture (mean, 0.8 hospitalization per year per patient). The indication for hospitalization included care for fracture (501 cases), pain (229 cases), or rehabilitation (21 cases). The proportion of patients hospitalized in relation to the fracture was 100 % for hip fracture, 47 % for vertebral fracture, and 24 % for wrist fracture. The number of hospitalizations ranged from one to four. The mean duration of hospital stay was 13.9 days. Patients with a hip fracture had the greatest amount of hospitalization, with an average of 1.2 admissions per patient during the year after fracture. Patients with a wrist fracture showed the smallest amount of hospitalization, with 0.3 admissions per patient.
Diagnostic tests were predominant in vertebral fracture patients, followed by patients with hip fractures. For diagnostic tests, a total of 5,441 X-ray examinations, 2,627 BMDs, 282 MRIs, and 844 CT scans were performed during the 12 months after fracture for 938 patients. A rare number of people received rehabilitation or physical therapy. Most of the patients (81 %) provided the reason for why they did not receive rehabilitation or physical therapy, which was because they did not think it was necessary. The other provided reason was due to economic burden.
Drugs used
The fracture-related pharmaceutical use at 4 and 12 months is shown in Table 3. Of the 938 patients, 894 patients (95.3 %) received polytherapy and 44 patients (4.7 %) received monotherapy at 4 months after fracture. The most commonly used drug was calcium/vitamin D (99 %), followed by pain relievers (95 %), calcitonin (51 %), and bisphosphonates (29 %). Calcium/vitamin D and pain relievers were the most common treatments in each category. Anti-osteoporosis dugs (bisphosphonates, calcitonin, estrogens, SERMs, PTH, etc.) were mostly used in patients with fresh fractures (<4 months after fracture), and its use tended to decrease with fracture healing. Most of the patients (93 %) stated that the reason they stopped using the anti-osteoporosis drugs was due to the economic burden of these specific drugs. The other reason was that they did not want to use the drug or because they did not know about the drugs. The proportion of patients in polytherapy was significantly higher when comparing patients with hip or vertebral fractures to patients with a wrist fracture.
The majority of patients were buying drugs from the hospital (66.5 %) or other pharmacies (33.5 %). Additional traditional Chinese medicine drugs were used, particularly “Qiang Gu Jiao Nang (Chinese patent medicines)” by 7.9 % of the patients and different types of bone protective soups by 3.0 % of the patients.
Transportation
The mean distance to the nearest general practitioner and community hospital were 1.8 ± 2.1 and 3.4 ± 3.8 km, respectively, and to the nearest general hospital and osteoporosis center were 25.6 ± 15.3 and 76.6 ± 51.2 km, respectively. All of the patients used a transportation tool to reach the clinic. Public transportation and taxis were used by 55.8 and 41.2 % of the patients, respectively, whereas private cars or bicycles were used by only 2.5 and 0.5 % of the patients, respectively. In addition, most of the patients (88.1 %) visited the clinic with at least one companion.
Home care and production loss
In addition to obtaining help from family members, 44 % of the patients also required a private nursemaid. Informal care (i.e., care by family members) were not included in the cost estimates. To improve their medical treatment, 33 % of the patients bought preventive healthcare foods.
There were 98 patients of working age, which was defined as being over the age of 18 years and under the age of 60 years in China. Twenty-three patients were occasionally on sick leave, and 46 patients had retired early. Ten patients were out of work due to the disease. The other 19 patients had not worked prior to the osteoporotic fracture. The average loss in working days related to the osteoporotic fracture was 302 ± 35 days of the patients’ working age.
Costs
All relevant costs due to the disease were collected, including direct healthcare costs (inpatient and outpatient care, diagnostic tests, drug costs, rehabilitation and physical therapy), direct nonmedical costs (social services, traffic fees, preventive care foods, and specific equipment, such as orthosis, bed lifts, rails, walking aids, wheelchairs), and indirect costs due to production losses (sick leave, early retirement, and out-of-work losses). The mean cost per patient for 1 year after fracture is summarized in Table 4.
The direct medical care costs averaged approximately RMB 17,007 per year per patient, of which the inpatient costs, drugs, and investigation accounted for the majority of the cost. Nonmedical direct costs were much less than the direct healthcare costs, averaging approximately RMB 1,846. Costs due to a loss in productivity averaged approximately RMB 877 per patient per year. Taken together, the total annual cost per patient in our series was approximately RMB 19,730 (USD 3,132). The direct and indirect costs represented 95.6 and 4.4 % of the total cost, respectively.
Except for the inpatient costs, the main item of expenditure was drug treatment, followed by diagnostic tests, home care, traffic expenses, and out-of-work losses, among other reasons. The annual total costs were highest in patients with hip fractures (RMB 27,283 or USD 4,330), followed by patients with vertebral fractures (RMB 21,474 or USD 3,409) and patients with wrist fractures (RMB 8,828 or USD 1,401). Hip fracture patients have the highest inpatient costs, with an average of RMB 16,869 per patient during the year after fracture, and patients with a wrist fracture showed the lowest inpatient costs, with RMB 1,223 per patient (P < 0.001). The annual western drug costs averaged RMB 4,292 per patient and were not significantly different between the fracture categories (P = 0.12). Vertebral fracture patients had the highest costs for investigation items (P < 0.001).
The patterns of resource use in the categories were not completely uniform (as shown in Table 4). In patients with hip fractures and vertebral fractures, the main cost was for inpatient costs, whereas in patients with wrist fractures, the highest cost was for western drugs.
Discussion
Estimates of the costs of an osteoporotic fracture are increasingly required by governmental agencies to determine the best allocation of resources and to assess the cost–benefit and cost-effectiveness ratios of diagnostic and therapeutic interventions. To the best of our knowledge, this is the first study to provide data on the cost of an osteoporotic fracture in a developing area in China and confirm that an osteoporotic fracture was a relevant socioeconomic burden at the individual, family, health service, and societal level in China. In addition, the cost of an osteoporotic fracture may also vary significantly according to its fracture location. The hip, vertebrae, and wrist are three of the most common osteoporotic fracture types. Knowledge of the total cost of illness may be required in addition to the cost for patients with different fracture locations. Thus, this study also compared the costs of the disease in referral patients with fractures in the three most common locations.
Our estimates were consistent with a series of Swedish studies [8, 17]. Both of us used prospectively collected estimates on fracture-related costs for the three most common osteoporotic fracture types. The economic approach of this study was a common cost of disease approach. The advantages of using this approach were that it is possible to include all of the relevant cost items and it might be easy to determine whether the resource is related to the fracture. A retrospective study design has also been used in several previous cost studies [5, 9], where the costs were estimated based on registry data. The advantage was that registry studies often use fairly large sample sizes. The main disadvantage with such studies is that it is hard to collect all of the relevant resource use; for example, it is rare for information regarding indirect costs and informal care to be available from any registry. Thus, further research will be needed to evaluate the cost-effectiveness of different therapeutic strategies in the prevention of fractures and inpatient stays in osteoporosis patients.
A modest estimate of the mean cost of osteoporotic fractures in China based on this study was RMB 19,730 (USD 3,132) per person per year. The mean annual income in the Sichuan province of China was only RMB 32,784 (5,203 USD). A few studies performed in China indicated that the prevalence of osteoporosis was approximately 13 %, and the incidence of hip osteoporotic fracture in people older than 50 years was between 138 and 254 per 100,000 people [18–20]. The incidence of a vertebral osteoporotic fracture in people older than 50 years was approximately 430 per 100,000 individuals. There were at least 169 million people with osteoporosis in China [21, 22]. Thus, osteoporotic fracture is a cost-intensive disorder and the economic burden of it to both Chinese patients and the nation is heavy.
Despite the composition proportion of the costs, there are many similar features between our study and those of developed countries [5, 8, 9]; for example, hospitalization accounts for more than 40 % of the total cost, although there are still some noteworthy differences. First, in this study, the cost of drugs account for 25.2 % of the direct cost of the osteoporotic fracture, which is approximately five to 17 times the cost found in the USA and in European countries [5, 8, 9]. In addition, anti-osteoporosis drugs (bisphosphonates, calcitonin, estrogens, SERMs, PTH, etc.) were mostly used in patients with fresh fractures (<4 months after fractures), and their use tended to decrease with the healing of the fractures. Moreover, most patients in our study stated that they stopped using anti-osteoporosis drugs due to the economic burden of these drug types. Thus, high drug costs in China deprived many people of the opportunity to receive drug treatment.
Second, in developed countries, rehabilitation and physical therapy is normally a consumptive item (more than 10 % of total costs) among patients with a fracture [5, 8, 9]. However, it accounts for only a very small component of the costs in the present study (0.1 %). It appears that only a small number of people received rehabilitation or physical therapy after a fracture in China. Furthermore, most patients in our study stated that they did not receive rehabilitation or physical therapy because they did not think it was necessary. The most possible reason was that, thus far, people in China lack knowledge and concepts regarding this type of therapy. This phenomenon may be reversed not only in Chinese patients but also in Chinese practitioners.
Limitations in this study should be noted. First, although information of the medical insurance for each patient was recorded, all costs presented in the study did not exclude the medical insurance reimbursement. So far, there is a fact that the medical insurance coverage in China is still low and the medical insurance of China can only reimburse part of the costs for inpatients (from 30 to 70 %, depending on different medical security systems), not for outpatients. However, the data still might exaggerate the economic burden to some patients. Second, although our series was a multiple center study, the data came from only hospitals of west China. So, the estimates may not be generalizable to other areas of China. Third, the patients included in the study had osteoporotic fractures occurring within 30 days prior to the first osteoporosis diagnosis or anytime thereafter. However, costs may be different between fracture cases with and without known osteoporosis. The main difference of cost item would be the anti-osteoporosis drugs after fractures have occurred, but prior to the first osteoporosis diagnosis (however, no more than 30 days).
Although it is difficult to directly compare our China estimates with burden of illness studies performed outside of China due to differences in demographic variables (e.g., age, sex), methods (e.g., identification of osteoporosis-related fractures, cost categories included in the estimates), or healthcare delivery systems (e.g., long-term care), in our study, the absolute value was generally smaller compared to the values obtained from developed countries; for example, the mean annual incremental direct cost per non-vertebral fracture patient was US $13,387 in the USA [5] and the mean fracture-related cost per year after a hip, vertebral, and wrist fracture were estimated, in euros (€), at €14,221, €12,544, and €2,147, respectively, in Sweden. It seems that this is because the unit cost, but not the resource utilization, i.e., the length of hospital stay, in China is longer than in other developed countries, while the cost per day is much cheaper. However, the fact that the average household income in China was only 1/34 of that in Sweden and 1/43 of that in the USA should not be ignored. The findings of this study indicated that the economic burden for Chinese epileptic patients was heavy. However, the cost of osteoporotic fractures and its effect on the national economy may potentially be reduced by popularizing the knowledge of osteoporosis, improving the care of osteoporosis, and thus preventing the rate of fracture.
References
Looker AC, Orwoll ES, Johnston CC Jr, Lindsay RL, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP (1997) Prevalence of low femoral bone density in older U.S. adults from NHANES III. J Bone Miner Res 12:1761–1768
Kanis JA, Johnell O, Oden A, Jonsson B, De Laet C, Dawson A (2000) Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 27:585–590
Ballard PA, Purdie DW, Langton CM, Steel SA, Mussurakis S (1998) Prevalence of osteoporosis and related risk factors in UK women in the seventh decade: osteoporosis case finding by clinical referral criteria or predictive model? Osteoporos Int 8:535–539
Wang Y, Tao Y, Hyman ME, Li J, Chen Y (2009) Osteoporosis in China. Osteoporos Int 20:1651–1662
Pike C, Birnbaum HG, Schiller M, Sharma H, Burge R, Edgell ET (2010) Direct and indirect costs of non-vertebral fracture patients with osteoporosis in the US. Pharmacoeconomics 28:395–409
Guillemin F, Martinez L, Calvert M et al (2013) Fear of falling, fracture history, and comorbidities are associated with health-related quality of life among European and US women with osteoporosis in a large international study. Osteoporos Int 24:3001–3010
Harvey NC, Matthews P, Collins R, Cooper C, Group UKBMA (2013) Osteoporosis epidemiology in UK Biobank: a unique opportunity for international researchers. Osteoporos Int 24:2903–2905
Borgstrom F, Zethraeus N, Johnell O et al (2006) Costs and quality of life associated with osteoporosis-related fractures in Sweden. Osteoporos Int 17:637–650
Haussler B, Gothe H, Gol D, Glaeske G, Pientka L, Felsenberg D (2007) Epidemiology, treatment and costs of osteoporosis in Germany—the BoneEVA Study. Osteoporos Int 18:77–84
Tarride JE, Hopkins RB, Leslie WD, Morin S, Adachi JD, Papaioannou A, Bessette L, Brown JP, Goeree R (2012) The burden of illness of osteoporosis in Canada. Osteoporos Int 23:2591–2600
Luo LZ, Xu L (2005) Study on direct economic-burden and its risk factors of osteoporotic hip fracture. Zhonghua Liu Xing Bing Xue Za Zhi 26:669–672
Dai K, Zhang Q, Fan T, Sen SS (2007) Estimation of resource utilization associated with osteoporotic hip fracture and level of post-acute care in China. Curr Med Res Opin 23:2937–2943
Ma J, Guo H, Yang X (2009) Epidemiology of primary osteoporosis. Chin Gen Pract 12:1744–1746
Borgstrom F, Lekander I, Ivergard M et al (2013) The International Costs and Utilities Related to Osteoporotic Fractures Study (ICUROS)—quality of life during the first 4 months after fracture. Osteoporos Int 24:811–823
Chen Z, Maricic M, Aragaki AK, Mouton C, Arendell L, Lopez AM, Bassford T, Chlebowski RT (2009) Fracture risk increases after diagnosis of breast or other cancers in postmenopausal women: results from the Women’s Health Initiative. Osteoporos Int 20:527–536
Abelson A (2008) A review of Paget's disease of bone with a focus on the efficacy and safety of zoledronic acid 5 mg. Curr Med Res Opin 24:695–705
Strom O, Borgstrom F, Zethraeus N et al (2008) Long-term cost and effect on quality of life of osteoporosis-related fractures in Sweden. Acta Orthop 79:269–280
Wang H, Li C, Xiang Q, Xiong H, Zhou Y (2012) Epidemiology of spinal fractures among the elderly in Chongqing, China. Injury 43:2109–2116
Zhu H, Zhang Y, Zhu X, Chen X, Yang J, Zhang X, Cheng Q (2003) Osteoporotic fracture and change of its iccidence in the elderly during 8 years. Geriatr Health Care 9:89–92
Nevitt MC, Xu L, Zhang Y, Lui LY, Yu W, Lane NE, Qin M, Hochberg MC, Cummings SR, Felson DT (2002) Very low prevalence of hip osteoarthritis among Chinese elderly in Beijing, China, compared with whites in the United States: the Beijing osteoarthritis study. Arthritis Rheum 46:1773–1779
Shang W, Yu W, Xu L, Lin Q, Tian JP (2005) Correlation between prevalent and incident osteoporotic vertebral fractures in Beijing male elderly. Zhonghua Yi Xue Za Zhi 85:84–87
Bow CH, Cheung E, Cheung CL et al (2012) Ethnic difference of clinical vertebral fracture risk. Osteoporos Int 23:879–885
Acknowledgments
This work was supported by grants obtained from the National Natural Science Fund of China (no. 30900471) and Sichuan Science and Technology Support Program (no. 2013SZ0003).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Qu, B., Ma, Y., Yan, M. et al. The economic burden of fracture patients with osteoporosis in western China. Osteoporos Int 25, 1853–1860 (2014). https://doi.org/10.1007/s00198-014-2699-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2699-0