
Abstract
Summary
The present meta-analysis shows no clear association between coffee consumption and the risk of hip fractures. There was a nonlinear association between tea consumption and the risk of hip fracture. Compared to no tea consumption, drinking 1−4 cups of tea daily was associated with a lower risk of hip fracture.
Introduction
Prospective cohort and case–control studies have suggested that coffee and tea consumption may be associated with the risk of hip fracture; the results have, however, been inconsistent. We conducted a meta-analysis to assess the association between coffee and tea consumption and the risk of hip fracture.
Methods
We performed systematic searches using MEDLINE, EMBASE, and OVID until February 20, 2013, without limits of language or publication year. Relative risks (RRs) with 95 % confidence intervals (CI) were derived using random-effects models throughout all analyses. We conducted categorical, dose–response, heterogeneity, publication bias, and subgroup analyses.
Results
Our study was based on 195,992 individuals with 9,958 cases of hip fractures from 14 studies, including six cohort and eight case–control studies. The pooled RRs of hip fractures for the highest vs. the lowest categories of coffee and tea consumption were 0.94 (95 % CI 0.71–1.17) and 0.84 (95 % CI 0.66–1.02), respectively. For the dose–response analysis, we found evidence of a nonlinear association between tea consumption and the risk of hip fracture (p nonlinearity < 0.01). Compared to no tea consumption, 1–4 cups of tea per day may reduce the risk of hip fracture by 28 % (0.72; 95 % CI 0.56–0.88 for 1–2 cups/day), 37 % (0.63; 95 % CI 0.32–0.94 for 2–3 cups/day), and 21 % (0.79; 95 % CI 0.62–0.96 for 3–4 cups/day).
Conclusions
We found no significant association between coffee consumption and the risk of hip fracture. A nonlinear association emerged between tea consumption and the risk of hip fracture; individuals drinking 1–4 cups of tea per day exhibited a lower risk of hip fractures than those who drank no tea. The association between 5 daily cups of tea, or more, and hip fracture risk should be investigated.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip fractures may lead to increased mortality, especially when they occur with other systemic diseases [1–5]. Therefore, identifying and confirming the modifiable risk factors for the prevention of hip fractures is of significant importance for public health research [6, 7].
The possible risk factors for hip fractures, such as daily calcium intake, physical activity level, body mass index (BMI), smoking, alcohol consumption, and dietary coffee and tea consumption, are hypothesized to be potential risk factors [7, 8]. Coffee and tea—among the most widely used psychoactive substances in the world—are now the main sources of dietary caffeine intake. Epidemiological studies have, however, found that high dietary caffeine intake is associated with reduced bone mineral density and increased body calcium loss [9]. Polyphenols and catechins in tea, meanwhile, had favorable effects on bone biology [10, 11].
An earlier meta-analysis by Liu and colleagues suggested that coffee consumption has an overall harmful effect of increasing the risk of fractures [12]. However, they did not provide the results of the subtypes of fractures, which may have reduced the strength of their conclusions. Moreover, the authors included coffee consumption only and did not refer to tea consumption [12]. Other prospective cohort studies targeted different outcomes and reported that the association between coffee and tea consumption and the risk of hip fracture was statistically nonsignificant [8, 13]. Additional research is, therefore, required to establish the role of both coffee and tea consumption in hip fractures.
We performed a meta-analysis of prospective cohort and case–control studies for the following purposes: (1) assess the link between coffee consumption and the risk of hip fractures and (2) to conduct an overview of the relationship between tea consumption and the risk of hip fractures.
Methods
We performed a systematic review of the available literature according to a meta-analysis: the MOOSE guidelines and the PRISMA statement [14, 15].
Search strategy
We searched MEDLINE (1966 to February 20, 2013), EMBASE (1980 to February 20, 2013), and OVID (1950 to February 20, 2013) for prospective cohort and case–control studies, with no language or publication years restrictions. All of the relevant studies were performed using medical subject headings (MeSH) or free text words. We followed MeSH search strategies and combined search terms for the outcome (hip fracture) and the influencing factor (caffeine, coffee, and tea). Additionally, we searched the reference lists and reviewed all of the studies that our search identified as relevant publications. We inspected the full text of relevant citations. We searched, by hand, through abstracts of meetings related to nutrition and osteoporosis that provided printed or electronic publications (no meeting abstracts, however, were pertinent to the present study).
Selection criteria
Reviewers independently evaluated all studies that presented quantitative estimates regarding the association between coffee and tea consumption, and the risk of hip fracture; the studies that met our criteria were included in this meta-analysis. Discrepancies between their decisions regarding study inclusion and data interpretation were resolved by arbitration, and consensus was reached after discussion. Studies were included in the meta-analysis if they met the following criteria: (1) prospective cohort or case–control design, (2) adult population, (3) the independent variables of interest were coffee or tea consumption, (4) the outcome of interest was hip fracture, and (5) the risk estimates, such as relative risks (RRs), odds ratios, hazard ratios, or incidence rate ratio with 95 % confidence intervals (CI), were reported. Those studies that did not meet the inclusion criteria were excluded during the initial review.
Data extraction
Two reviewers using a standardized data collection form independently extracted all data. We resolved discrepancies in judgment by discussion and consulting the original articles. The following data were collected from each study: the first author's last name, publication year, country, duration of follow-up, recruitment time, size of study population, participant sex and age, the number of cases, the measure and range of exposure, the adjustment variables, and the risk estimates with corresponding CIs for categories of consumption variables. We extracted the RRs and 95 % CIs that reflected the greatest degree of control for potential confounders and used these values in our main analyses. We collected data for the categories of coffee or tea consumption (e.g., 1, 2, 3 cups/day). A third reviewer served to resolve disagreement regarding the abstracted data.
Statistical analyses
We used RRs as the means of measuring association across studies. Hazard ratios and odds ratios were transformed into RRs [16, 17]. We pooled the RRs to summarize associations between the highest and the lowest coffee and tea consumption categories, and to conduct the dose–response analyses.
For the meta-analysis, we used random-effects models. We assessed the heterogeneity of selected studies using Cochran I 2 statistics [18]. As suggested by Higgins et al., we considered I 2 values of 25 % as low, 50 % as moderate, and 75 % as high [19]. To summarize the association between coffee and tea and the risk of hip fracture, we pooled the effect measures for the highest vs. the lowest categories, and the dose–response relationship for coffee and tea consumption. We used restricted cubic splines (three knots at fixed percentiles of 10, 50, and 90 % of the distribution) by employing generalized least-squares regression to examine the potential nonlinear dose–response associations between coffee and tea consumption and the risk of hip fracture [20, 21]. A probability value for nonlinearity was calculated by testing the null hypothesis that the coefficient of the second spline was equal to 0 [20].
We employed subgroup analyses to find associations between the risk of hip fracture and relevant study characteristics (i.e., participants' ages, geographical location, study design, duration of follow-up, sex, and adjustment for calcium intake) as possible sources of heterogeneity. Funnel plot asymmetry, which we used to explore publication bias, was measured by Egger and Begg's regression tests. To assess the possible effect of publication bias in our meta-analysis, we also performed the “trim and fill” procedure. This method considers the possibility of hypothetical “missing” studies, imputing their RRs, and obtaining a pooled RR that included the hypothetical missing studies as though they had actually been performed [22, 23]. We used Stata 11 (StataCorp, College Station, TX, USA) to perform all of the analyses, and considered p < 0.05 to be statistically significant.
Results
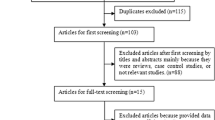
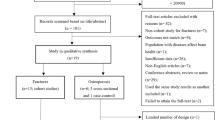
Figure 1 presents the process of the study selection. After we evaluated titles and abstracts, 35 studies remained. We excluded several studies because of the cross-sectional design or a lack of data and included a total 14 studies in the meta-analysis [8, 13, 24–35]. Observers reached agreement on which studies should be included (Cohen's unweighted κ = 0.88).

Flowchart for the study selection
The characteristics of included studies
The characteristics of the included studies are summarized in Table 1. After a review of 1,723 abstracts, we included 14 studies: six of these were prospective cohort studies, and eight were case–control studies. Ten of the total 14 studies reported data for both coffee and tea; additionally, three studies reported data for coffee only, and one study reported data for tea only. There were 195,992 participants in this meta-analysis, and 9,958 hip fractures. The MEDOS study conducted by Johnell and Kanis was a multicenter study enrolling participants from several European countries. The remaining studies took place across nice different countries (four studies from the USA, and one each from Canada, Australia, Italy, Japan, Norway, Finland, Sweden, and India). Five studies recruited male and female participants, two studies recruited only males, and seven studies recruited only females. All participants were ≥19 years old. The follow-up time of the cohort studies ranged from 6 to 30 years. All the information was obtained from self-reported food frequency or self-administered questionnaires for daily coffee or tea consumption. Fractures were identified using self-report of fracture experience, radiologic diagnosis, or hospital admission records. The covariates most commonly taken into account were age, BMI, smoking, calcium intake, alcohol consumption, and estrogen-replacement therapy (only in female participants). Physical activity was adjusted in four studies.
Coffee consumption and risk of hip fracture
A total of 13 studies including 195,792 individuals reported on the association between coffee consumption and the risk of hip fractures. The sum of all of the selected studies, the multivariate-adjusted RRs of each study, and the categories of the highest vs. the lowest coffee consumption are presented in Fig. 2a. The pooled RR of hip fractures for the highest vs. the lowest categories of coffee consumption was 0.94 (95 % CI 0.71–1.17), with moderate heterogeneity between studies (p < 0.01; I 2 = 56.3 %). The Egger test exhibited a publication bias (p < 0.01), and Begg's test demonstrated a borderline evidence of publication bias (p = 0.05). The “trim and fill” method confirmed that the six possibly missing studies could alter the pooled estimation of RR to 0.82 (95 % CI 0.59–1.06).

Adjusted relative risk (RR) of coffee (a) and tea (b) (95 % CI) and hip fracture (highest vs. lowest categories) using the random-effects mode
For the dose–response analysis, we found no association between coffee consumption and the risk of hip fracture (p nonlinearity = 0.89). Compared with no coffee consumption, the pooled RRs of hip fracture were 0.95 (95 % CI 0.69–1.20) for 1–2 cup of coffee per day, 0.91 (95 % CI 0.77–1.06) for 2–3 cups/day, 0.92 (95 % CI 0.70–1.15) for 3–4 cups/day, 1.07 (95 % CI 0.61–1.53) for 4–5 cups/day, and 0.71 (95 % CI 0.41–1.01) for 5–6 cups/day (Fig. 3a).

Adjusted relative risk (RR) of coffee (a) and tea (b) (95 % CI) and hip fracture (every category, the reference levels are 0 cups/day) using the random-effects model
Tea consumption and risk of hip fracture
A total of 11 studies with information on 147,488 individuals examined the association between tea consumption and the risk of hip fracture. The multivariate-adjusted RRs of each study and categories of the highest vs. the lowest tea consumption are available in Fig. 2b. The pooled RR of hip fractures for the highest vs. the lowest categories of tea consumption was 0.84 (95 % CI 0.66–1.02), with moderate heterogeneity between studies (p = 0.05; I 2 = 45.3 %). The Egger test exhibited a potential publication bias (p = 0.06), while Begg's test demonstrated no publication bias (p = 0.14). The trim and fill method confirmed that the three potentially missing studies could alter the pooled estimation of RR to 0.73 (95 % CI 0.52–0.94).
The dose–response analysis showed evidence of a nonlinear association between tea consumption and risk of hip fracture (p nonlinearity < 0.01). Compared to no tea consumption, the pooled RRs of hip fractures were 0.72 (95 % CI 0.56–0.88) for 1–2 cup of tea per day, 0.62 (95 % CI 0.32–0.94) for 2–3 cups/day, 0.79 (95 % CI 0.62–0.96) for 3–4 cups/day, 0.95 (95 % CI 0.62–1.29) for 4–5 cups/day, 0.95 (95 % CI: 0.48–1.41) for 5–6 cups/day, and 1.25 (95 % CI 0.40–2.10) for more than 6 cups/day (see Fig. 3b).
Subgroup analyses
Results of the subgroup analyses for the association between coffee or tea consumption and the risk of hip fracture are presented in Table 2. The analyses demonstrated that the participants' age, geographical location, study design, adjustment for calcium intake, and follow-up period did not influence the association between dietary coffee consumption and the risk of hip fracture. The pooled analysis in male participants demonstrated a 34 % lower risk of hip fracture (RR 0.66, 95 % CI 0.43–0.89). However, only three studies were performed, for a total of 49,144 male participants. This may have led to a lower statistical power in assessing the relationship between coffee consumption and risk of hip fractures in males. This result should be interpreted with caution and would benefit from being verified by further research. The analyses demonstrated that geographical location, the follow-up period, adjustment for calcium intake, and gender did not influence the inverse associations between dietary tea consumption and the risk of hip fracture, whereas the pooled analysis of five studies that examined participants whose mean age (at the time of recruitment) was more than 70 years showed a 33 % lower risk of hip fractures (RR 0.67, 95 % CI 0.55–0.79). Furthermore, eight case–control studies showed a 20 % lower risk of hip fracture (RR 0.80, 95 % CI 0.60–1.00).
Discussion
Our meta-analysis was based on 195,992 individuals with 9,958 hip fractures and indicated that coffee consumption has no significant statistical association with the risks of hip fracture. In the dose–response analysis of tea consumption, however, we found a nonlinear association between tea consumption and the risk of hip fracture. Most interestingly, our results showed that in comparison to individuals who drank no tea, drinking 1–4 cups of tea daily was associated with lower risks of hip fracture. The association between 5 or more cups of tea per day and hip fracture risks remains unclear, and may benefit from further research.
Coffee—one of the most widely consumed beverages in the world—has been linked to many pathological conditions, such as cancer, cardiovascular and cerebrovascular diseases, and type 2 diabetes mellitus [20, 36–38]. Our meta-analysis focused on hip fractures and demonstrated that hip fractures were not significantly associated with coffee consumption. In a subgroup analysis, we found 34 % lower risk of hip fracture in men with the highest amount of coffee consumption compared to men with the lowest amount of coffee consumption. Due to the limited relevant data pertaining to men, we note that the inverse association might be attributed to chance or result from systematic error (e.g., residual confounding or selection bias). This finding should be interpreted carefully, and additional well-designed and stratified cohort studies should be conducted in men.
Regarding tea consumption, our results showed a nonlinear association with the risk of hip fractures; compared to no tea consumption, drinking 1–4 cups of tea daily appeared to show a significant and independent protective effect. However, due to small numbers and low statistical power for the higher intake categories (reflected in the wide confidence intervals in Fig. 3), the association between 5 cups or more of tea per day and hip fracture risk deserves further attention.
Several plausible mechanisms have been proposed to explain the relationship between tea consumption and fracture benefits, including biologically active compounds, such as tea polyphenols (or catechins), fluoride content, and the phytoestrogenic content. Catechins, including epigallocatechin gallate, epicatechin gallate, epicatechin, epigallocatechin, and essential elements, such as chromium, manganese, selenium, and zinc, are biologically active tea components that may improve bone mineral density. These compounds may act by enhancing osteoblastic proliferation, differentiation, and mineralization, and by suppressing osteoclastic differentiation and promoting osteoclast apoptosis. This would result in increased bone density, thus reducing the risk of hip fractures [10, 11, 39, 40].
Not all components contained in tea have positive effects. Caffeine, contained therein, has detrimental effects on bone biology. The majority of studies demonstrated that middle-to-high concentrations of caffeine (1 to 10 mM) dose-dependently enhanced osteoclast differentiation by enhancing RANKL-induced osteoclastogenesis, modulating intracellular calcium levels, or by decreasing vitamin D receptor expression, leading to reduced bone mineral density [41–43]. In contrast, other studies suggested that low-concentrations caffeine (lower than 1 mM) enhanced osteoblast viability and osteoblastic mineralization without affecting osteoclastic bone resorption activity [42].
Previous meta-analytic research by Liu et al. [12] examining the relationship between coffee and fractures (10 studies), including various fracture subtypes (7 assessed hip fractures and 3 examined different subtypes of fractures), and suggested an overall weak destructive effect of coffee intake on the total risk of fractures (RR 1.03, 95 % CI 1.00, 1.06). The authors, however, did not provide the results of their meta-analysis on fracture subtypes, which may have reduced the strength of their conclusions. Moreover, Liu and colleagues only examined coffee consumption, but did not assess that of tea. Our meta-analysis, meanwhile, focused on both and demonstrated that coffee consumption has no significant statistical association with the risk of hip fracture; tea consumption, however, exhibited a nonlinear association with the risk of hip fracture.
Our meta-analysis had several limitations. First, because our work consisted of several individual studies, the quality of each study varied, and the adjustments for potential statistical confounding factors fluctuated. Our meta-analysis was subjected to the influence of confounders which could be innate in the included studies. Although most of the selected studies were adjusted for gender, age, BMI, menopause statement, estrogen-replacement therapy, alcohol intake, education, marital status, physical activity, and caloric consumption, the factors we controlled could, theoretically, offer a possible explanation for our results. Nevertheless, it is difficult to determine whether other types of consumption, the specific effects of coffee or tea, or the possible beneficial nutrients in these beverages were responsible for the observed outcomes.
Moreover, the classification of coffee or tea consumption is difficult to evaluate, which directly weakens the strength of the observed relationship. In the dose–response analysis, it is difficult to single out variations in effects at high levels; we therefore used common categorization of coffee/tea consumption (refer to previous dose–response meta-analyses) that may affect the validity of the results [20, 36]. Moreover, whether the participants consumed coffee with or without tea could not be assessed. Because the consumption of coffee and tea was primarily estimated by self-administered and self-reported food frequency, and the content of affecting factors varied, errors were difficult to avoid; the underestimation of the RRs was, therefore, difficult to avoid.
Third, the heterogeneity in the present study may be introduced by methodological differences among the studies selected for inclusion. Although many of the I 2 values we estimated were assessed as moderate in the subgroup analysis, we explored age, study design, and sex for potential sources of heterogeneity in the analysis of coffee; only age was considered for the analysis of tea. These issues may reduce the strength of our conclusions.
Fourth, the abstainer bias should be considered [44, 45]. People decrease their caffeine consumption as they age and become ill or frail, or increase their use of medications. If these individuals are included in the no coffee or tea consumption categories, results may be erroneous. This also relates to the unexpected finding of Trimpou et al. concerning coffee (Fig. 2a), where the most frequent coffee drinkers had an RR for hip fracture of 0.55 (95 % CI 0.42–0.73) compared with non-drinkers. None of the selected studies, however, reported the numbers of abstainers. Thus, well-designed cohort studies with controls for abstainer factors are needed.
We are, lastly, concerned about publication bias because smaller studies reporting null results tend not to be published. As we have demonstrated in the funnel plot and Egger's test in the analysis of the association between tea consumption and the risk of hip fracture, a potential publication bias may exist, altering the pooled estimation of RR to 0.73 (95 % CI 0.52–0.94); this implies that an inverse association may exist between tea consumption and the risk of hip fractures. Our findings, therefore, should be interpreted with caution.
Conclusion
Our meta-analysis found no statistical association between dietary coffee consumption and risk of hip fracture. In the dose–response analysis, however, there was a nonlinear association between tea consumption and the risks of hip fracture: we found that compared with no tea consumption, 1–4 cups of tea daily may reduce the risks. The association between five cups or more and hip fracture risk, however, should be examined further. Due to the presence of publication bias, our results may underestimate the true magnitude of this association. Additional well-designed and stratified cohort studies with wide coverage of controls for confounding factors are, therefore, required to elucidate the link between coffee and tea consumption, and the risk of hip fractures.
References
Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C (2009) Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 20:1633–1650
Kanis JA, Oden A, McCloskey EV, Johansson H, Wahl DA, Cooper C, IOF Working Group on Epidemiology and Quality of Life (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23:2239–2256
Qu X, Zhang X, Qin A, Liu G, Zhai Z, Hao Y, Li H, Zhu Z, Dai K (2013) Bone mineral density and risk of breast cancer in postmenopausal women. Breast Cancer Res Treat 138:261–271
Qu X, Huang X, Jin F, Wang H, Hao Y, Tang T, Dai K (2013) Bone mineral density and all-cause, cardiovascular and stroke mortality: a meta-analysis of prospective cohort studies. Int J Cardiol 166:385–393
Qu X, Zhang X, Zhai Z, Li H, Liu X, Li H, Liu G, Zhu Z, Hao Y, Dai K (2013) Association between physical activity and risk of fracture. J Bone Miner Res. doi:10.1002/jbmr.2019
Watts NB, Adler RA, Bilezikian JP, Drake MT, Eastell R, Orwoll ES, Finkelstein JS (2012) Osteoporosis in men: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 97:1802–1822
Johansson H, Kanis JA, Oden A, Johnell O, McCloskey E (2009) BMD, clinical risk factors and their combination for hip fracture prevention. Osteoporos Int 20:1675–1682
Trimpou P, Landin-Wilhelmsen K, Oden A, Rosengren A, Wilhelmsen L (2010) Male risk factors for hip fracture—a 30-year follow-up study in 7,495 men. Osteoporos Int 21:409–416
Rapuri PB, Gallagher JC, Kinyamu HK, Ryschon KL (2001) Caffeine intake increases the rate of bone loss in elderly women and interacts with vitamin D receptor genotypes. Am J Clin Nutr 74:694–700
Yun JH, Kim CS, Cho KS, Chai JK, Kim CK, Choi SH (2007) (−)-Epigallocatechin gallate induces apoptosis, via caspase activation, in osteoclasts differentiated from RAW 264.7 cells. J Periodontal Res 42:212–218
Oka Y, Iwai S, Amano H, Irie Y, Yatomi K, Ryu K, Yamada S, Inagaki K, Oguchi K (2012) Tea polyphenols inhibit rat osteoclast formation and differentiation. J Pharmacol Sci 118:55–64
Liu H, Yao K, Zhang W, Zhou J, Wu T, He C (2012) Coffee consumption and risk of fractures: a meta-analysis. Arch Med Sci 8:776–783
Hansen SA, Folsom AR, Kushi LH, Sellers TA (2000) Association of fractures with caffeine and alcohol in postmenopausal women: the Iowa Women's Health Study. Public Health Nutr 3:253–261
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Zhang J, Yu KF (1998) What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 280:1690–1691
McNutt LA, Wu C, Xue X, Hafner JP (2003) Estimating the relative risk in cohort studies and clinical trials of common outcomes. Am J Epidemiol 157:940–943
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Larsson SC, Orsini N (2011) Coffee consumption and risk of stroke: a dose–response meta-analysis of prospective studies. Am J Epidemiol 174:993–1001
Orsini N, Bellocco R, Greenland S (2007) Generalized least squares for trend estimation of summarized dose–response data. Stat J 6:40–57
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR (2000) Empirical assessment of effect of publication bias on meta-analyses. BMJ 320:1574–1577
Kreiger N, Gross A, Hunter G (1992) Dietary factors and fracture in postmenopausal women: a case–control study. Int J Epidemiol 21:953–958
Nieves JW, Grisso JA, Kelsey JL (1992) A case–control study of hip fracture: evaluation of selected dietary variables and teenage physical activity. Osteoporos Int 2:122–127
Johnell O, Gullberg B, Kanis JA et al (1995) Risk factors for hip fracture in European women: the MEDOS Study. Mediterranean Osteoporosis Study. J Bone Miner Res 10:1802–1815
Tavani A, Negri E, La Vecchia C (1995) Coffee intake and risk of hip fracture in women in northern Italy. Prev Med 24:396–400
Suzuki T, Yoshida H, Hashimoto T et al (1997) Case–control study of risk factors for hip fractures in the Japanese elderly by a Mediterranean Osteoporosis Study (MEDOS) questionnaire. Bone 21:461–467
Kanis J, Johnell O, Gullberg B et al (1999) Risk factors for hip fracture in men from southern Europe: the MEDOS study. Mediterranean Osteoporosis Study. Osteoporos Int 9:45–54
Hernandez-Avila M, Colditz GA, Stampfer MJ, Rosner B, Speizer FE, Willett WC (1991) Caffeine, moderate alcohol intake, and risk of fractures of the hip and forearm in middle-aged women. Am J Clin Nutr 54:157–163
Meyer HE, Pedersen JI, Loken EB, Tverdal A (1997) Dietary factors and the incidence of hip fracture in middle-aged Norwegians. A prospective study. Am J Epidemiol 145:117–123
Kiel DP, Felson DT, Hannan MT, Anderson JJ, Wilson PW (1990) Caffeine and the risk of hip fracture: the Framingham Study. Am J Epidemiol 132:675–684
Jokinen H, Pulkkinen P, Korpelainen J, Heikkinen J, Keinanen-Kiukaanniemi S, Jamsa T, Korpelainen R (2010) Risk factors for cervical and trochanteric hip fractures in elderly women: a population-based 10-year follow-up study. Calcif Tissue Int 87:44–51
Cumming RG, Klineberg RJ (1994) Case-control study of risk factors for hip fractures in the elderly. Am J Epidemiol 139:493–503
Jha RM, Mithal A, Malhotra N, Brown EM (2010) Pilot case-control investigation of risk factors for hip fractures in the urban Indian population. BMC Musculoskelet Disord 11:49
Huxley R, Lee CM, Barzi F, Timmermeister L, Czernichow S, Perkovic V, Grobbee DE, Batty D, Woodward M (2009) Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch Intern Med 169:2053–2063
Larsson SC, Wolk A (2007) Coffee consumption and risk of liver cancer: a meta-analysis. Gastroenterology 132:1740–1745
Je Y, Liu W, Giovannucci E (2009) Coffee consumption and risk of colorectal cancer: a systematic review and meta-analysis of prospective cohort studies. Int J Cancer 124:1662–1668
Yun JH, Pang EK, Kim CS, Yoo YJ, Cho KS, Chai JK, Kim CK, Choi SH (2004) Inhibitory effects of green tea polyphenol (−)-epigallocatechin gallate on the expression of matrix metalloproteinase-9 and on the formation of osteoclasts. J Periodontal Res 39:300–307
Kamon M, Zhao R, Sakamoto K (2010) Green tea polyphenol (−)-epigallocatechin gallate suppressed the differentiation of murine osteoblastic MC3T3-E1 cells. Cell Biol Int 34:109–116
Rapuri PB, Gallagher JC, Nawaz Z (2007) Caffeine decreases vitamin D receptor protein expression and 1,25(OH)2D3 stimulated alkaline phosphatase activity in human osteoblast cells. J Steroid Biochem Mol Biol 103:368–371
Liu SH, Chen C, Yang RS, Yen YP, Yang YT, Tsai C (2011) Caffeine enhances osteoclast differentiation from bone marrow hematopoietic cells and reduces bone mineral density in growing rats. J Orthop Res 29:954–960
Shankar VS, Pazianas M, Huang CL, Simon B, Adebanjo OA, Zaidi M (1995) Caffeine modulates Ca2+ receptor activation in isolated rat osteoclasts and induces intracellular Ca2+ release. Am J Physiol 268:F447–454
Fillmore KM, Stockwell T, Chikritzhs T, Bostrom A, Kerr W (2007) Moderate alcohol use and reduced mortality risk: systematic error in prospective studies and new hypotheses. Ann Epidemiol 17:S16–23
Chikritzhs T, Fillmore K, Stockwell T (2009) A healthy dose of scepticism: four good reasons to think again about protective effects of alcohol on coronary heart disease. Drug Alcohol Rev 28:441–444
Acknowledgments
This study was supported by the Fund for Key National Basic Research Program of China (grant 2012CB619101), Major Basic Research of Science and Technology Commission of Shanghai Municipality (grant no. 11DJ1400303), Key Disciplines of Shanghai Municipal Education Commission (grant no. J50206), Scientific Research from the National Natural Science Foundation for the Youth of China (grant no. 81201364), and Innovative Research from Shanghai Municipal Education Commission (grant no. 13YZ031). The funding sources had no role in the study design, collection, analysis, data interpretation, or the writing of the report.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Jing Sheng, Xinhua Qu, and Xiaoyu Zhang contributed equally as first coauthors.
Rights and permissions
About this article
Cite this article
Sheng, J., Qu, X., Zhang, X. et al. Coffee, tea, and the risk of hip fracture: a meta-analysis. Osteoporos Int 25, 141–150 (2014). https://doi.org/10.1007/s00198-013-2563-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2563-7