
Abstract
Summary
We used Danish registers to identify patients with osteoporosis, who had been treated with parathyroid hormone and evaluated the probability of developing cancer. We did not find an increased risk of cancer among the patients treated with parathyroid hormone.
Introduction
We evaluated the incidences of malignancies and mortality in osteoporotic patients treated with rPTH.
Methods
Using Danish nationwide registers, we identified patients diagnosed with osteoporosis in the period 1995 through 2010. Each patient treated with rPTH (“case”) was compared with 10 gender- and age-matched patients who did also have osteoporosis but did not receive rPTH (“control”).
Results
A total of 4,104 cases (80.3 % females) were identified. The mean age at the beginning of rPTH treatment was 70.9 (SD 9.7) years. During a follow-up time of 10,118 person-years for the cases and 88,005 person-years for the controls, a total of 255 cases (6.2 %) compared with 2,103 controls (5.1 %) experienced a cancer (Chi square, p = 0.003). We found an adjusted cancer related HR of 1.1 (95 %CI 0.9–1.4) among the cases. Lung cancer was the only cancer type with a significantly increased rate among patients receiving rPTH (HR 1.7; 95 % CI 1.3–2.3). No cases developed osteosarcomas and nine controls developed osteosarcoma. During follow-up, 627 (15.3 %) cases died and 4,175 (10.2 %) controls died, which yielded an excess mortality risk of 26 % (95 % CI 16–37 %). This could be due to differences in the prevalence of vertebral fractures between the rPTH-treated and non-treated patients.
Conclusion
This study did not support the hypothesis describing a possible link between rPTH treatment and the development of cancer. We also conclude that osteosarcoma has not been diagnosed in any Danish patient receiving rPTH since the year 2003 when it was introduced on the market.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recombinant parathyroid hormone analogs (rPTH) for the treatment of osteoporosis (OP) have widened the clinical spectrum for which improvement of bone mineral density and reduced fracture risk can be achieved [1]. Teriparatide (1-34-PTH) was approved by the US Food and Drug Administration (FDA) in 2002 and intact parathyroid hormone (1-84-PTH) obtained approval in the European Union in 2006 [2]. However, the approval of rPTH for the treatment of osteoporosis did not come without controversy because preclinical studies on rats had raised the concern that exposure to 1-34-PTH and 1-84-PTH was related to the development of osteosarcoma [3, 4]. Nevertheless, no scientific data has hitherto demonstrated an rPTH-related cancer risk of neither osteosarcoma nor any other cancer in humans [5]. Only few inconclusive case reports have described a possible link between rPTH treatment and carcinogenesis [6] and of the 549 patients with osteosarcoma, who replied to the questionnaire in the US Postmarketing Surveillance Study, no patient had a history of 1-34-PTH treatment [7]. Since the introduction of rPTH, several hundreds of thousands of patients have been treated [2].
It was our aim with the present study to evaluate the impact of rPTH treatment primarily on the risk of cancer. Our secondary endpoints were mortality and other comorbidities. We did a retrospective longitudinal cohort study using nationwide Danish registers.
Materials and methods
Study population
We compared patients receiving treatment with rPTH (“case”) with 10 age- and gender-matched patients that had not been treated with rPTH (“controls”). We identified patients with osteoporosis in the period January 1, 1995 to December 31, 2010 from the Danish National Patient Register that contains discharge diagnoses from all inpatient and outpatient contacts from the year 1995 [8]. We used the international classification of disease (ICD) 10th edition codes for osteoporosis, M80 and M81. We retrieved redeemed prescriptions on rPTH (ATC code H05AA02: 1-34-PTH, H05AA03: 1-84-PTH) through the Danish Prescription Database [9].
Outcome variable
The primary event was defined as the first registered cancer that occurred after the initiation of rPTH treatment, and we disregarded patients for whom a cancer had been diagnosed prior to rPTH treatment. We used ICD-10 discharge codes from the Danish National Patient Register to identify multiple myeloma (C90) and osteosarcoma (C40–C41) along with cancers of the lungs (C34), colon (C18), skin (C43–C44), urinary bladder (C67), breast (C50), and prostate (C61). The following ICD-10 codes were used for mortality diagnoses: Cxx: malignancies, Kxx: alimentary tract, Ixx: circulatory system, Jxx: respiratory system, Fxx: psychiatric, A0/A2–A9/Bxx: infectious diseases, and V/X1–X5/Y1–Y7/Y80–Y86/Y872/Y8: external lesion.
We evaluated the following other complications: myocardial infarction (MI) (I21-I23), cerebrovascular disease (I60-I69/G45/G46), and chronic pulmonary disease (CPD) (J40-J47/J60-J67/J684/J701/J703/J841/J920/J961/J982/J983).
Covariates
We retrieved birthdates, gender, and socioeconomic status from the Danish Civil Registration System, which is updated daily and tracks changes in demographic characteristics of Danish citizens [10]. We calculated the Charlson index as a measure of comorbidity [11]. For the analyses of cancer incidences we used a modified Charlson index as covariate that did not include malignancies. We assessed the users of bisphosphonates using the Danish Prescription Database (ATC codes M05BA or M05BB).
Statistics
Baseline characteristics are presented as means (SD) or medians (Q1–Q3). Risk time is expressed in person-years (PY) and defined as the time from start of rPTH treatment (cohort entry) until the occurrence of an event of or end of follow-up, whichever came first. The risk time was split into decades of lifetime to adjust for age dependent covariates. Each control patient was assigned with a cohort entry date identical to the matching case’s entry date. All events—mortality, cancer, and other comorbidity—were reported in prevalences and incidence rates (IR) in numbers per 1,000 PY. We used multivariate Cox proportional hazard models to assess the hazard ratio (HR) with 95 % confidence interval (CI). Persons with missing data were excluded from the analyses. All analyses were done using SAS 9.2 (SAS Institute Inc., Cary, NC, USA). The study was approved by the Danish Health and Medicines Authority and followed the regulations set up by the Danish Data Protection Agency.
Results
Baseline characteristics are presented in Table 1. A total of 4,104 patients (80.3 % females) with osteoporosis receiving rPTH were identified. The mean age at initiation of rPTH treatment was 70.9 (SD 9.7) years and the median duration of rPTH treatment was 477 (Q1–Q3, 238–530) days. The number of patients who began rPTH treatment increased with approximately 90 patients per year from 406 patients in the year 2004 to 846 patients in 2010 (p < 0.0001) and the mean age when initiating rPTH treatment remained unaltered throughout the observation period. Teriparatide was used in 86 % of the cases and 1-84-PTH in 12 % of the cases, while 2 % had received both rPTH types. The age at initiation of rPTH was slightly higher among the patients receiving 1-34-PTH compared with the patients using 1-84-PTH (71.0 vs. 70.0 years, p = 0.02). Bisphosphonates had been used prior to the initiation of rPTH treatment in 87 % of the cases, while 13 % of the cases redeemed prescriptions on bisphosphonates only after ending the rPTH therapy.
Cancer
Cancer incidences and relative risks are presented in Table 2. A total of 255 cases (6.2 %) compared with 2,103 controls (5.1 %) were diagnosed with a cancer (Chi square, p = 0.003) after the initiation of rPTH treatment. The cancer incidence was 25.2 (95 %CI 22.3–28.5) per 1,000 PY among the cases and 23.9 (95 %CI 22.9–24.9) per 1,000 PY among the controls, yielding an HR of 1.1 (95 %CI 0.9–1.4) in our model, which was adjusted for gender, age, and the modified Charlson index. The relative risk of cancer remained constant independently of time since initiation of treatment with rPTH (p = 0.3). The median time (Q1–Q3) between the initiation of rPTH treatment and the diagnosis of cancer was 1.7 (0.8–3.0) years.
We investigated the association between the two different rPTH types and cancer and found that 6.6 % of the patients using 1-34-PTH experienced a cancer compared with 4.1 % among the patients using 1-84-PTH (Chi square, p = 0.04). However, when considering the risk time and adjusting for covariates, no significant excess risk was found (p = 0.8).
The most frequently reported type of malignancy was lung cancer, which was found among 1.4 % of the cases compared with 0.7 % of the controls. The prevalence of CPD was slightly higher among the cases compared with controls (26 % vs. 24 %, p < 0.0001) and this difference was accounted for by adjusting with the Charlson index that includes CPD. We found the use of rPTH to be associated with 70 % (95 %CI 30–130 %, p = 0.0003) increased risk of lung cancer. The increased risk of lung cancer remained constant independently of time with rPTH treatment (p = 0.8). We did not find any increased risk for any other cancer types, but demonstrated a 40 % (95 %CI 10–60 %, p = 0.02) reduced rate of breast cancer among the women being treated with rPTH. In total, 108 patients were registered with multiple myeloma, which occurred at the same rate among the cases and controls (p = 0.3). No patients in the rPTH group were registered with osteosarcoma compared with nine patients among the controls (Chi square, p = 0.3).
Male gender was associated with an increased risk of cancer of 23 % (95 %CI 12–36 %) and the gender related cancer risk was similar between the cases and controls (p = 0.8). The index of comorbidity was also related to cancer risk and for every increase of one in Charlson score, an increase in cancer risk of 45 % (95 %CI 43–47 %) was found. The association between comorbidity index and cancer risk was comparable between cases and controls (p = 0.1).
Mortality
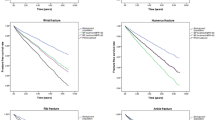
Death occurred more frequently among the patients who received treatment with rPTH. During follow-up, 627 cases died (15.3 %) and among the matched controls a total of 4,175 died (10.2 %). The age of death was comparable between cases and the controls (76.0 vs. 75.6 years, p = 0.3). The mortality rate was 56 per 1,000 PY among the cases and 41 per 1,000 PY among the controls (HR 1.4, 95 %CI 1.3–1.5) and we found an increased risk of death of 26 % (95 % CI 16–37 %) among the cases compared with the controls when we adjusted for gender, age, Charlson score, and socioeconomic status. The most frequent causes of death were circulatory, respiratory, and cancer diseases among both cases and controls (Table 3).
The relationship between the relative mortality rate and rPTH treatment was not constant throughout the age groups. With increasing age, the death rate among persons in rPTH treatment declined significantly towards being similar with the death rate among the controls (p < 0.0001).
Other morbidity than cancer
We found increased rates of MI among the cases compared with the controls with an HR of 1.3 (95 %CI 1.1–1.6). For cerebrovascular diseases, the rates were not significantly different (HR 1.1, 95 %CI 0.9–1.3). Chronic pulmonary disease also occurred at higher rates after the initiation of rPTH among the patients compared with controls (HR 1.3, 95 % 1.1–1.5) besides being more prevalent at the beginning of follow-up (26 % vs. 24 %, p < 0.0001; Table 1).
Discussion
This study is the largest population study that systematically evaluates the relationship between rPTH treatment and cancer risk. We did not find any excessive cancer risk, with the exception of lung cancer, in our cohort of mainly elderly patients with osteoporosis, who had received treatment with rPTH. The weakness of this study is its retrospective design and non-standardized diagnostics of the investigated cancer types. Furthermore, the groups of cases and controls were not comparable in all aspects. The patients using rPTH and the controls were gender and age matched, but the two groups differed undoubtedly with regard to the severity of osteoporosis. The clinical criteria from the Danish Health and Medicines Authority for obtaining reimbursement of the expenses resembles the inclusion criteria used in the phase-3 study by Neer et al. [1], and hence, we expect severe osteoporosis and vertebral compression fractures to be more frequent among the rPTH-treated patients. The cases were furthermore characterized by the absence of prior radiation therapy, bone cancer or bone metastases, which all are contraindications to rPTH treatment.
The first use of 1-34-PTH for osteoporosis dates back to 1980 when Reeve et al. exposed 22 patients with osteoporosis to once-daily subcutaneous injections of 1-34-PTH for 6–24 months and demonstrated histomorphometric signs of bone formation [12]. The phase-3 trial was published in 2001, and documented a decrease of 65 % in vertebral fractures in the 1-34-PTH treatment group compared with placebo [1]. This study was terminated prematurely due to the finding of osteosarcomas in rats exposed to 1-34-PTH at a dosing 3–60 times human doses for a duration equivalent to 75 human years [3]. For that reason, the final approval by the FDA included several limitations in the use of 1-34-PTH for osteoporosis and the manufacturer undertook a 10-year follow-up study to evaluate the relevance in humans [2]. Preliminary data from that study has recently been published, and among 549 patients with osteosarcoma from 15 US centers, none had received treatment with 1-34-PTH [7]. Also the relationship between endogenous PTH production and cancer has been investigated, but no convincing association has been demonstrated between circulating PTH levels and breast cancer [13], colorectal cancer [14], or prostate cancer [15]. These cross-sectional studies were undertaken due to the finding of elevated cancer incidences among patients with hyperparathyroidism in Danish and Swedish nationwide epidemiological studies [16, 17]. However, studies on treatment with PTH and hyperparathyroidism are not comparable due to the different actions of continuous endogenous and transient exogenous PTH [18].
The suspicion of an rPTH related carcinogenetic effect has thus not been abandoned, but the evidence suggesting a linkage is far from convincing. The present study further weakens this hypothesis. For cancer of any type we found equal incidence rates between patients in rPTH treatment and controls. Lung cancer turned out to be more frequent among the patients in rPTH treatment but a causal relationship with rPTH treatment is unlikely due to many reasons. We presume that a higher fraction of smokers was present among the rPTH-treated patients, who had more severe osteoporosis, and we attempted to address this confounder by adjusting for the CPD prevalence, but this diagnosis does not embrace all smokers [19]. Another more likely explanation for the increased incidence of lung cancer among rPTH-treated patients is more regular examinations by the physician. It should also be noted that the median time from initiation of rPTH treatment until the diagnosis of any cancer in our study was only 1.7 years, which further argues against any causal relationship between rPTH and cancer development. The lower incidence of breast cancer in women treated with rPTH could be an accidental finding (p value 0.02). Earlier reports have indicated an increased risk of breast cancer in patients with hyperparathyroidism [17, 20], but the relationship between PTH and breast cancer could not be verified in a nested case–control study with 764 women with breast cancer [13]. Earlier epidemiologic studies on Danish and Swedish registers have reported higher rates of lung cancer and lower rates of breast cancer among patients with osteoporosis compared with the general population [21, 22]. This could also be the cause to our findings taking into account the probability of baseline differences in the severity of osteoporosis in our material.
Osteosarcoma is a rare cancer form with a projected incidence of 2.5–3.5 per 100,000 in the United States population [23] and less than one per 100,000 person-years in Denmark (www.cancer.dk). Given this assumption, we estimate that our study has a power of 95 % of detecting an increase of 50 % in the incidence of osteosarcoma in the rPTH-treated group. With a hypothesized increase of 10 % of the incidence of osteosarcoma in the rPTH-treated group, the power would be as low as 13 %. This illustrates clearly the epidemiological challenges when studying this disease even in nationwide studies. However, the total lack of osteosarcoma among the rPTH-treated patients is in concordance with the newly published the US Postmarketing Surveillance Study, which further undermines the postulated relationship between rPTH and osteosarcoma [7]. The discrepancy between the development of osteosarcoma in rats and humans due to rPTH treatment may be explained by the differences in bone homeostasis between the species. The rat is a continuously growing animal with open epiphysis until time of death, while humans receive rPTH treatment long time after the closure of the epiphysis. The low background prevalence of osteosarcoma results in high number-needed-to-harm (NNH). We estimate that the NNH would be approximately 12,000, had one patient from each of our groups developed osteosarcoma when considering the background prevalence. This number should be compared with a number-needed-to-treat (NNT) of 29 to avoid fractures based on the numbers from study by Neer et al. [1].
When it comes to mortality, we found higher incidences for several causes of death. We suspected that the patients receiving rPTH were in worse general physical condition than the controls, although the Charlson index indicated otherwise. Hence, the Charlson index does not explain the differences in mortality, but baseline differences in the prevalence of vertebral compression fractures between the rPTH-treated and non-treated rPTH patients may interfere since this fracture type is related to increased risk of death [24].The incidences of MI and CPD were higher among the rPTH treated, which we attribute to differences in baseline characteristics rather than rPTH treatment. We tried to account for the baseline difference adjusting for gender and age, together with Charlson comorbidity index, but information on lifestyle factors such as alcohol consumption, smoking, physical activity, and vitamin intake was not available. Especially alcohol consumption and smoking are well-known risk factors that may be overrepresented among patients in rPTH treatment [25, 26]. Lower bone mineral density has been related to increased risk of MI in other studies and hence, our finding does not vouch for a causal relationship between rPTH treatment and MI [27].
Finally, we conclude that neither previous studies nor the present study supports a relationship between the use of rPTH and cancer development. We also conclude that osteosarcoma has not been diagnosed in any Danish patient receiving rPTH since the year 2003 when it was introduced on the market. Even though this study in theory comprises all Danish patients receiving rPTH it is hampered by the fact that the follow-up time for each patient was short in terms of carcinogenesis. The safety of rPTH treatment is after ten years of clinical experience not put in doubt but it is hence too soon to make any conclusions on the long-term safety of rPTH and the present study should be considered a preliminary report.
References
Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, Hodsman AB, Eriksen EF, Ish-Shalom S, Genant HK, Wang O, Mitlak BH (2001) Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 344:1434–1441
Tashjian AH Jr, Gagel RF (2006) Teriparatide [human PTH(1–34)]: 2.5 years of experience on the use and safety of the drug for the treatment of osteoporosis. J Bone Miner Res 21:354–365
Vahle JL, Sato M, Long GG, Young JK, Francis PC, Engelhardt JA, Westmore MS, Linda Y, Nold JB (2002) Skeletal changes in rats given daily subcutaneous injections of recombinant human parathyroid hormone (1–34) for 2 years and relevance to human safety. Toxicol Pathol 30:312–321
Jolette J, Wilker CE, Smith SY, Doyle N, Hardisty JF, Metcalfe AJ, Marriott TB, Fox J, Wells DS (2006) Defining a noncarcinogenic dose of recombinant human parathyroid hormone 1–84 in a 2-year study in Fischer 344 rats. Toxicol Pathol 34:929–940
Cipriani C, Irani D, Bilezikian JP (2012) Safety of osteoanabolic therapy: a decade of experience. J Bone Miner Res 27:2419–2428
Subbiah V, Madsen VS, Raymond AK, Benjamin RS, Ludwig JA (2010) Of mice and men: divergent risks of teriparatide-induced osteosarcoma. Osteoporos Int 21:1041–1045
Andrews EB, Gilsenan AW, Midkiff K, Sherrill B, Wu Y, Mann BH, Masica D (2012) The US postmarketing surveillance study of adult osteosarcoma and teriparatide: study design and findings from the first 7 years. J Bone Miner Res 27:2429–2437
Lynge E, Sandegaard JL, Rebolj M (2011) The Danish National Patient Register. Scand J Public Health 39:30–33
Kildemoes HW, Sorensen HT, Hallas J (2011) The Danish National Prescription Registry. Scand J Public Health 39:38–41
Pedersen CB, Gotzsche H, Moller JO, Mortensen PB (2006) The Danish Civil Registration System. A cohort of eight million persons. Dan Med Bull 53:441–449
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Reeve J, Meunier PJ, Parsons JA, Bernat M, Bijvoet OL, Courpron P, Edouard C, Klenerman L, Neer RM, Renier JC, Slovik D, Vismans FJ, Potts JT Jr (1980) Anabolic effect of human parathyroid hormone fragment on trabecular bone in involutional osteoporosis: a multicentre trial. Br Med J 280:1340–1344
Almquist M, Bondeson AG, Bondeson L, Malm J, Manjer J (2010) Serum levels of vitamin D, PTH and calcium and breast cancer risk-a prospective nested case–control study. Int J Cancer 127:2159–2168
Fedirko V, Riboli E, Bueno-de-Mesquita HB, Rinaldi S, Pischon T, Norat T, Jansen EH, van Duijnhoven FJ, Tjonneland A, Olsen A, Overvad K, Boutron-Ruault MC, Clavel-Chapelon F, Engel P, Kaaks R, Teucher B, Boeing H, Buijsse B, Trichopoulou A, Trichopoulos D, Lagiou P, Sieri S, Vineis P, Panico S, Palli D, Tumino R, van Gils CH, Peeters PH, Chirlaque MD, Gurrea AB, Rodriguez L, Molina-Montes E, Dorronsoro M, Bonet C, Palmqvist R, Hallmans G, Key TJ, Tsilidis KK, Khaw KT, Romieu I, Straif K, Wark PA, Romaguera D, Jenab M (2011) Prediagnostic circulating parathyroid hormone concentration and colorectal cancer in the European Prospective Investigation into Cancer and Nutrition cohort. Cancer Epidemiol Biomark Prev 20:767–778
Brandstedt J, Almquist M, Manjer J, Malm J (2012) Vitamin D, PTH, and calcium and the risk of prostate cancer: a prospective nested case–control study. Cancer Causes Control 23:1377–1385
Nilsson IL, Zedenius J, Yin L, Ekbom A (2007) The association between primary hyperparathyroidism and malignancy: nationwide cohort analysis on cancer incidence after parathyroidectomy. Endocr Relat Cancer 14:135–140
Pickard AL, Gridley G, Mellemkjae L, Johansen C, Kofoed-Enevoldsen A, Cantor KP, Brinton LA (2002) Hyperparathyroidism and subsequent cancer risk in Denmark. Cancer 95:1611–1617
Aslan D, Andersen MD, Gede LB, de Franca TK, Jorgensen SR, Schwarz P, Jorgensen NR (2012) Mechanisms for the bone anabolic effect of parathyroid hormone treatment in humans. Scand J Clin Lab Invest 72:14–22
Powell HA, Iyen-Omofoman B, Baldwin DR, Hubbard RB, Tata LJ (2012) Chronic Obstructive Pulmonary Disease and Risk of Lung Cancer: The Importance of Smoking and Timing of Diagnosis. J Thorac Oncol
Michels KB, Xue F, Brandt L, Ekbom A (2004) Hyperparathyroidism and subsequent incidence of breast cancer. Int J Cancer 110:449–451
Ji J, Sundquist K, Sundquist J (2012) Cancer risk after hospitalization for osteoporosis in Sweden. Eur J Cancer Prev 21:395–399
McGlynn KA, Gridley G, Mellemkjaer L, Brinton LA, Anderson KC, Caporaso NE, Landgren O, Olsen JH (2008) Risks of cancer among a cohort of 23,935 men and women with osteoporosis. Int J Cancer 122:1879–1884
Lahat G, Lazar A, Lev D (2008) Sarcoma epidemiology and etiology: potential environmental and genetic factors. Surg Clin North Am 88:451–481, v
Lau E, Ong K, Kurtz S, Schmier J, Edidin A (2008) Mortality following the diagnosis of a vertebral compression fracture in the Medicare population. J Bone Joint Surg Am 90:1479–1486
Gonzalez-Calvin JL, Garcia-Sanchez A, Bellot V, Munoz-Torres M, Raya-Alvarez E, Salvatierra-Rios D (1993) Mineral metabolism, osteoblastic function and bone mass in chronic alcoholism. Alcohol Alcohol 28:571–579
Kanis JA, Johnell O, Oden A, Johansson H, De LC, Eisman JA, Fujiwara S, Kroger H, McCloskey EV, Mellstrom D, Melton LJ, Pols H, Reeve J, Silman A, Tenenhouse A (2005) Smoking and fracture risk: a meta-analysis. Osteoporos Int 16:155–162
Wiklund P, Nordstrom A, Jansson JH, Weinehall L, Nordstrom P (2012) Low bone mineral density is associated with increased risk for myocardial infarction in men and women. Osteoporos Int 23:963–970
Acknowledgments
We thank Henrik Hansen for revising manuscript content.
Conflicts of interest
Ulrich Bang has no conflicts of interest. Lars Hyldstrup has been an advisory board member for Eli-Lilly and is advisory board member of Takeda. He has received research funding from both companies. Jens-Erik Beck Jensen has served as a member of advisory boards and has been on the speaker’s bureau for Eli Lilly, Takeda, Nycomed, Amgen Inc., Novartis, and MSD.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bang, U.C., Hyldstrup, L. & Jensen, J.E.B. The impact of recombinant parathyroid hormone on malignancies and mortality: 7 years of experience based on nationwide Danish registers. Osteoporos Int 25, 639–644 (2014). https://doi.org/10.1007/s00198-013-2470-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2470-y