
Abstract
Summary
Adjusted for age, gender, height and weight, calcaneal quantitative ultrasound (QUS) and serum 25-hydroxyvitamin D (S-25(OH)D) proved to be significant predictors of hip fracture among subjects aged ≥50 years. Even if their contribution to the predictive power was modest, they may be useful in the assessment of hip fracture risk in the elderly.
Introduction
This study assessed calcaneal QUS measurements, S-25(OH)D and several other factors for the prediction of hip fracture risk in a nationally representative population sample.
Methods
The study population consisted of 3,305 subjects (1,872 women), aged 50 years or over, who had participated in a comprehensive health survey. QUS measurements were made by means of the Hologic Sahara device. S-25(OH)D was measured by radioimmunoassay. Emerging cases of hip fracture were identified from the National Hospital Discharge Register.
Results
During a mean follow-up of 8.4 years, 95 subjects sustained a hip fracture. After adjusting for age, gender, height, weight and each other, a 1 standard deviation increment in the quantitative ultrasound index (QUI) (21.7) and in S-25(OH)D (17.5 nmol/L) reduced the risk of hip fracture by 40 % (hazard ratio [HR] = 0.60, 95 % confidence interval [CI] = 0.42–0.86) and by 31 % (HR = 0.69, 95 % CI = 0.55–0.87), respectively. The predictive power of a model including age, gender, height and weight was improved by about 8 % after the addition of QUI and S-25(OH)D. Among subjects aged 75 years or over, the corresponding improvement was about 130 %.
Conclusions
QUI and S-25(OH)D were significant and independent predictors of hip fracture. However, their ability to increase the predictive power of a statistical model including readily available simple variables such as age, gender, height and weight was rather modest. Still, our findings suggest that QUI and S-25(OH)D may be of clinical use in the assessment of hip fracture risk particularly in the elderly.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fragility fractures constitute a growing health problem in elderly people and an ever-increasing burden for health services in many countries. Hip fractures, in particular, are disabling and costly [1–4].
Bone mineral density measured by means of dual-energy X-ray absorptiometry (DXA) is widely used for the diagnosis of osteoporosis and assessment of fracture risk [5]. Fracture risk can also be assessed on the basis of age and a number of other risk factors, such as body build (weight, height and body mass index), prior fragility fracture, smoking, heavy alcohol use and certain diseases and medications [5–7]. Combinations of risk factors of this kind (so-called clinical risk factors) and bone mineral density are likely to improve the performance of such risk assessments for various fragility fractures, including hip fracture [8].
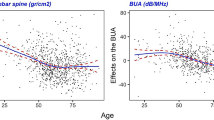
Although not suitable for diagnosing osteoporosis, calcaneal quantitative ultrasound (QUS) has been shown to predict hip fractures in elderly men and women even independently of bone mineral density assessments by DXA [9–15]. The measurements of broadband ultrasound attenuation (BUA) and speed of sound (SOS) across the calcaneus partially reflect bone strength since the ultrasound propagation largely depends on the structure and quality of the medium being studied. From the global point of view, it is of importance that QUS devices are transportable, much less expensive than dual-energy X-ray scanners and do not involve ionising radiation.
Because of technical differences, various brands and models of QUS devices do not necessarily yield directly comparable information on BUA and SOS to be used in the assessment of bone strength or fragility [16, 17]. This complicates comparisons of results obtained with different QUS devices, since there are no methods for standardisation or cross-calibration of measurements between two or more commercially available brands. However, according to a recent meta-analysis based on prospective studies, QUS devices from various manufacturers appear to predict risks of hip and other fractures with similar performance in elderly people, both men and women [18]. Overall, these prospective studies on fracture risk assessment have been rather heterogeneous with respect to the methods for recruitment of participants, gender of the study population (predominantly women), fracture outcomes and the risk factors for which the authors have been able to adjust the risk [9–15]. Only a few prospective studies have taken into account risk factors other than age, body build and fracture history [11, 15]. For example, in this context, little information is available on physical activity, smoking, alcohol intake, or vitamin D status. Moreover, for the prediction of hip fracture risk, the follow-up periods have been short, on average, rarely in excess of 3 years.
Thus far, only a few prospective studies have combined the use of the Hologic Sahara QUS device with other risk factors in the prediction of hip fracture [13–15]. Using the Hologic Sahara device in a cross-sectional population-based study [19], we found significant associations of the calcaneal QUS variables with serum 25-hydroxyvitamin D (S-25(OH)D) and a number of other known risk factors for bone fragility [20]. The present study assesses the baseline findings in this nationally representative population sample of men and women for the prediction of hip fractures during a mean follow-up of 8.4 years.
Methods
Study design and subjects
A comprehensive health survey, the Health 2000 Survey, was conducted in Finland in 2000–2001 [21]. The survey was based on a stratified two-stage cluster sample (N = 8,028) representative of the Finnish population aged 30 years or over. Those aged 80 years or over were oversampled (2:1) relative to their proportion in the population. A total of 6,354 subjects participated in health examinations carried out by specially trained professionals in 80 localities throughout the country.
The present follow-up study is based on the participants aged 50 years or over at baseline for whom information on QUS measurement was available. After the exclusion of all victims of high-energy hip fractures (n = 20), the present study population consists of 3,305 subjects aged 50 years or over (75 % of those within this age range in the original sample).
The study was approved by the ethics committee for epidemiology and public health in the hospital districts of Helsinki and Uusimaa, Finland. All participants gave their signed informed consent.
Risk factors
Weight and height were measured with light clothing without shoes, with height to the nearest 0.5 cm and weight to the nearest 0.1 kg. S-25(OH)D concentrations were measured by radioimmunoassay as described previously [20].
The information about previous hip fractures was drawn from the National Hospital Discharge Register covering all hospitals in the country. Smoking reported in a health interview [20] was classified into three categories: never smokers, former smokers (those who had quit smoking at least 1 month prior to the survey) and current smokers. Alcohol use, expressed as absolute ethanol in grams per week, was estimated on the basis of the reported average consumption during the past month and classified into three categories: no use, moderate use and heavy use. The limit of heavy use was set at 280 g/week in men and 140 g/week in women, as proposed by the Finnish guidelines [22]. A questionnaire [19] elicited information on leisure-time physical activity which was classified into three categories: active, moderately active and sedentary.
Quantitative ultrasound measurement
QUS measurements were made by means of the Hologic Sahara device (Hologic, Bedford, MA, USA) recording BUA (in decibels per megahertz) and SOS (in metres per second) transmitted in a mediolateral direction across the calcaneus. The device was checked for performance quality daily before the first participant using the phantom provided by the manufacturer. The reliability and validity of the measurements were good as reported earlier [20, 23]. A composite variable, the quantitative ultrasound index (QUI) was calculated from the values of BUA and SOS [13].
Hip fractures
The follow-up information about hip fractures was drawn from the National Hospital Discharge Register. The patients admitted to the hospital for primary treatment of hip fracture (codes S72.0–S72.2 as primary or secondary diagnoses according to ICD-10) were identified, excluding those with high-energy fractures (i.e. fractures following falls exceeding 1 m from one level to another or traffic accidents or casualties alike). A hip fracture was considered to be ‘the first’ if no hip fracture had been registered during the 10 years preceding the baseline. The follow-up period continued until hospitalisation due to a hip fracture, until the end of 2009 or until the date of death, whichever came first.
Statistical methods
Comparisons between men and women and between subjects with and without incident hip fracture were performed using Student’s t test for continuous variables and chi-square test for categorical variables. Pearson’s partial correlation coefficients (r) adjusted for gender were calculated to assess associations of age with QUS and S-25(OH)D. A probability value <0.05 was considered statistically significant. Predictors of hip fracture were estimated by adjusted hazard ratios (HR) with 95 % confidence intervals (CI) using Cox’s proportional hazards models. Mutually similar analyses were first made separately for men and women. Because of the relatively small number of hip fractures in men, the gender cohorts were combined for the final risk assessment models. Moreover, owing to small numbers, the history of a previous hip fracture could not be used as a covariate in the final model. Thus, the subjects who had previously fractured their hip were excluded from the final risk analyses (n = 31, including 6 subjects who sustained a new fracture during the follow-up).
Statistical significance of each covariate or interaction term was tested with the likelihood ratio test and expressed as an exact p value. The performance of the models (including various combinations of risk factors with and without the QUS measurements) was further assessed by means of coefficients of determination (R 2) [24]. All analyses were performed with the SAS system (version 9.3; SAS Institute Inc., Cary, NC, USA) and SUDAAN which takes into account the sampling design including the oversampling of those aged 80 years or over (Research Triangle Institute, Release 10.0.1).
Results
Table 1 presents the baseline characteristics of the study population. All QUS values were significantly higher in men compared to women. Smoking habits and alcohol consumption clearly differed between men and women, whereas there was no significant difference in physical activity nor in the proportion of those with previous hip fracture or in the concentration of S-25(OH)D.
During a mean follow-up of 8.4 years (27,757 person-years), 95 (2.9 %) of the subjects sustained a hip fracture at the mean age of 79.4 years. Of these, 89 were considered first hip fractures. As expected, fracture of the femoral neck was the most common type of hip fracture representing 64 % of all first hip fractures (Table 2).
Subjects who sustained a hip fracture had lower QUI values than those who remained free from this fracture (84.3 ± 23.1 vs. 99.6 ± 21.2 in men, p = 0.0002 and 73.3 ± 17.7 vs. 89.9 ± 20.8 in women p < 0.0001). Likewise, S-25(OH)D concentrations were lower among those who fractured their hip compared to those who escaped the fracture (37.1 ± 14.0 vs. 47.0 ± 18.2 nmol/L in men, p = 0.01 and 39.4 ± 13.7 vs. 47.0 ± 17.1 nmol/L in women, p = 0.0005). Previous hip fracture appeared to be more common among men and women who fractured their hip during the follow-up compared to those who did not. However, this difference did not reach statistical significance (p value = 0.178 for men and 0.102 for women).
Table 3 presents the HR of hip fracture in subjects who had not previously fractured their hip (n = 3,274). In the gender-adjusted and age-adjusted model (Table 3), an increment of 1 standard deviation (SD) in QUI (21.7) indicated a reduction of 35 % in the hip fracture risk. When adjustments were made for all other significant risk factors (fully adjusted model; Table 3), an increment of 1 SD in QUI was associated with a 40 % lower risk of hip fracture. Conversely, a reduction of 1 SD in QUI increased the risk of hip fracture by 67 % (fully adjusted HR = 1.67, 95 % CI = 1.16–2.34). The results were similar for models with BUA and SOS in place of QUI (data not shown).
An increment of 1 SD in S-25(OH)D (17.5 nmol/L) was associated with a 31 % lower risk of hip fracture in the model adjusted for gender and age as well as in the fully adjusted model including all other significant factors (Table 3). A reduction of 1 SD in S-25(OH)D, on the other hand, increased the hip fracture risk by 46 % (fully adjusted HR = 1.46, 95 % CI = 1.15–1.83). Other significant and independent predictors of hip fracture in the model were female gender, high age, tallness and low weight.
The coefficients of determination (R 2) indicated that age alone explained 66 % of the variation in the observed hip fracture risk (Table 4). This figure increased to 72 % when gender, height and weight were added to the model. The coefficient was further improved by an increment of 4 percentage units (a 6 % relative increase) after the addition of QUI and, correspondingly, by increments of 3 percentage units (a 4 % relative increase) after the addition of S-25(OH)D and of 6 percentage units (a 8 % relative increase) after the addition of both of these. Among subjects aged 75 years or over, age alone explained 6 % of the variation in the hip fracture risk, whereas age with gender, height and weight explained 10 % of the variation. The coefficient of determination was improved by 7 percentage units (a 70 % relative increase) after the addition of QUI or S-25(OH)D and by 13 percentage units (a 130 % relative increase) after the addition of both of these variables (Table 4).
Along with increasing age, the risk of hip fracture increased, while QUI and S-25(OH)D decreased (gender-adjusted Pearson’s partial r = −0.30, p < 0.0001 for QUI and r = −0.12, p < 0.0001 for S-25(OH)D). Adjusted for gender, height and weight, the cumulative hazards of hip fracture were fairly similar in the quintiles of QUI and S-25(OH)D until the age of 75 years, after which the hazards showed substantial divergence between the quintiles (Fig. 1a, b). The quintiles of QUI and S-25(OH)D were further examined to explore whether these variables should pass some threshold values to show significant contributions to the hip fracture risk along with increasing age. Adjusted for gender, age, height and weight, QUI values <74.3 (the upper limit of the lowest quintile) were found to be associated with a significantly higher risk of hip fracture (HR = 2.14, 95 % CI = 1.21–3.78) compared to values ≥74.3. Correspondingly, values of S-25(OH)D <60.0 nmol/L (the lower limit of the highest quintile) indicated a significantly higher risk of hip fracture (HR = 2.53, 95 % CI = 1.17–5.46) compared to values ≥60.0 nmol/L.

a Adjusted cumulative hazard of hip fracture by quintiles of QUI according to age (adjusted for gender, height and weight) (Q1–Q5 refer to mean values [limits] of quintiles; Q1 = 63.4 [23.1–74.3], Q2 = 81.5 [74.3–87.5], Q3 = 92.8 [87.5–98.2], Q4 = 103.8 [98.2–110.3], Q5 = 124.1 [110.4–243.5]). b Adjusted cumulative hazard of hip fracture by quintiles of S-25(OH)D (in nanomoles per liter) according to age (adjusted for gender, height and weight) (Q1–Q5 refer to mean values [limits] of quintiles; Q1 = 24.7 nmol/L [5.0–32.0 nmol/L], Q2 = 36.5 nmol/L [33.0–40.0 nmol/L], Q3 = 44.9 nmol/L [41.0–49.0 nmol/L], Q4 = 54.3 nmol/L [50.0–59.0 nmol/L], Q5 = 72.1 nmol/L [60.0–134.0 nmol/L])
Discussion
In this nationally representative population sample of men and women, the results of QUS measurement and the concentrations of S-25(OH)D were significant and independent predictors of hip fracture. One SD reduction in QUI (21.7) and S-25(OH)D (17.5 nmol/L) increased the hip fracture risk by 67 and 46 %, respectively. However, their ability to improve the predictive power of the Cox model including age, gender, height and weight was rather modest: a relative increase of about 6 % by QUI, 4 % by S-25(OH)D and 8 % by both of these together. The hip fracture hazards associated with QUI and S-25(OH)D showed increasing divergence with advancing age (Fig. 1a, b). Interestingly, among subjects aged 75 years or over, both QUI and S-25(OH)D improved the predictive power of the Cox model by about 70 % and the two together by as much as 130 % (Table 4).
The (gel-coupled) Hologic Sahara (Hologic, Bedford, MA, USA) device was chosen to be used in our survey not only for the qualities of measurement but also for the comfort and ease of use. So far, few prospective studies have used the Hologic Sahara device to assess the QUS variables in conjunction with clinical risk factors for the prediction of hip fractures [13–15]. To our knowledge, this is the first study to assess the independent roles of the QUS measurements and S-25(OH)D in hip fracture prediction by means of models including age, gender, height and weight.
Our results on the QUS variables measured with the Hologic Sahara device agree with those from earlier prospective studies using various QUS devices [9–15, 18]. According to a recent meta-analysis, QUS devices from various manufacturers appear to predict hip fracture risk with similar performance [18]. The HR of 1.67 for QUI in our study agrees with the risk gradient of 1.99 (95 % CI = 1.49–2.67) reported in the previously mentioned meta-analysis. In accordance with several earlier studies [25–29], we also found a significant and independent association between serum 25(OH)D and hip fracture risk.
The R 2 values of our models were closely comparable with those reported from recent prospective studies on models for hip fracture prediction [30–32] in which the same calculation method [24] has been used.
There are no universally agreed threshold values of the QUS measurements for the identification of subjects at high risk of hip fracture. In our study, the HR for the quintiles of QUI (adjusted for gender, age, height and weight) indicated a higher hip fracture risk in subjects with QUI values below 74.3. In a previous study based on a large dataset from three case–control studies [33], the threshold of QUI for the Sahara device was calculated at 63.2 to classify subjects as being at high risk of hip fracture. The difference between these threshold values can be at least partly explained by differences in the designs and study populations of the two studies. Only women aged 65 years or over were involved in the cross-sectional study by Hans et al. [33], whereas our prospective study comprised both men and women aged 50 years or over.
For bone health, the optimum level of S-25(OH)D is considered to lie between 50 and 80 nmol/L [34]. In the present study, we found that, in subjects with S-25(OH)D values below 60 nmol/L, the risk of hip fracture was more than twice that observed in subjects with values 60 nmol/L or above (HR = 2.53, 95 % CI = 1.17–5.46). Higher cutoff points could not be evaluated in our study since the highest S-25(OH)D value was 74 nmol/L among those who developed a hip fracture. Anyhow, comparisons between different studies should be made with reservation because the S-25(OH)D values measured in different laboratories with different assays cannot be assumed to be directly comparable [35].
Age was the most powerful predictor of hip fracture risk. Nevertheless, later in life, selective mortality and cumulative differences in morbidity, functional capacity and frailty obviously gain significance with regard to old age as such. QUI and S-25(OH)D improved the predictive power of the Cox model more markedly among the old than among the younger subjects. Our study thus suggests that measurements of QUI and S-25(OH)D may be of clinical use in the assessment of hip fracture risk especially among subjects aged 75 years or over.
In agreement with earlier studies, we found tallness to be an independent risk factor for hip fracture (Table 3) [6, 36–38]. This might be related to biomechanical factors, such as hip axis length [39].
Alcohol consumption and smoking showed no significant association with hip fracture risk. This was probably attributable to the small proportions of heavy alcohol users and current smokers among study subjects; neither did physical activity show a significant association with the fracture risk. This result parallels those from two recent prospective studies which, similarly to our study, assessed physical activity along with QUS and other factors for fracture risk [11, 15]. Nevertheless, a sedentary lifestyle was not so far from statistical significance in our gender-adjusted and age-adjusted model (Table 3). Anyhow, as Moayyeri recently pointed out [40], an association between physical activity and fracture does not necessarily result from a causal link between lack of exercise and fracture. Such an association may also result from confounding by poor health as well as by genetically inherited stronger bones and better qualifications for a physically active lifestyle.
The small number of hip fracture cases is a major limitation of our study. We could not perform the final risk analyses separately for men and women. However, in the combined analysis, the addition of gender did not significantly improve the predictive performance of the model. Moreover, it should be noted that results of QUS measurement evidently predict hip fracture risk with similar performance in elderly men and women [18]. A further limitation of our study is that the risk analyses were based solely on the baseline findings, as no information was available on the later developments of the potential risk factors in the study population.
Owing to low proportions in the study population, subjects with previous hip fracture (0.8 %) could not be included in the risk assessments. According to earlier studies, a history of previous fragility fracture clearly predicts future hip fracture risk [11, 41]. In our study population, previous hip fracture appeared to be more common among subjects who sustained a hip fracture compared to those who did not, although this difference was not statistically significant (data not shown). The prevalence of other potential risk factors, such as rheumatoid arthritis and use of systemic glucocorticoids, was also low, and these variables were, therefore, not included in our risk assessment models.
The strengths of our study were its national representativeness and high participation rate. In addition, the information on hip fractures was obtained from the National Hospital Discharge Register, a reliable and accurate source which covers all fractures requiring hospital treatment in our country [42, 43].
In conclusion, the results of QUS measured by means of the Hologic Sahara device and the measurements of S-25(OH)D concentrations significantly and independently predicted hip fractures in this nationally representative population sample of subjects aged 50 years and over. When the previously mentioned variables were added to a model including age, gender, height and weight, the predictive power of the model was improved but only rather modestly. In practice, such a model including results from QUS and S-25(OH)D measurements probably would not be much more useful than a simple risk assessment based on readily available variables such as age, gender, height and weight. Nevertheless, our findings suggest that QUI and S-25(OH)D might be useful in the assessment of hip fracture risk particularly in the elderly. Further prospective studies in elderly study populations with larger numbers of incident cases of hip fracture are needed to assess calcaneal QUS and S-25(OH)D for the prediction of hip fractures preferably along with a wider range of simple, well-defined risk factors related to morbidity, functional capacity and frailty.
References
Johnell O, Kanis JA, Odén A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jönsson B (2004) Mortality after osteoporotic fractures. Osteoporos Int 15(1):38–42
Nurmi I, Narinen A, Lüthje P, Tanninen S (2003) Cost analysis of hip fracture treatment among the elderly for the public health services: a 1-year prospective study in 106 consecutive patients. Arch Orthop Trauma Surg 123(10):551–554
Lüthje P, Kataja M, Nurmi I, Santavirta S, Avikainen V (1995) Four-year survival after hip fractures—an analysis in two Finnish health care regions. Ann Chir Gynaecol 84(4):395–401
Melton LJ, Gabriel SE, Crowson CS, Tosteson ANA, Johnell O, Kanis JA (2003) Cost-equivalence of different osteoporotic fractures. Osteoporos Int 14(5):383–388
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359(9321):1929–1936
Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, Cauley JC, Black D, Vogt TM (1995) Risk factors for hip fracture in White women. N Engl J Med 332(12):767–773
Kanis JA, Borgstrom F, De Laet C, Johansson H, Johnell O, Jönsson B, Oden A, Zethraeus N, Pfleger B, Khaltaev N (2005) Assessment of fracture risk. Osteoporos Int 16(6):581–589
Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J, Burckhardt P, Cooper C, Christiansen C, Cummings S, Eisman JA, Fujiwara S, Gluer C, Goltzman D, Hans D, Krieg MA, La Croix A, McCloskey E, Mellstrom D, Melton LJ, 3rd, Pols H, Reeve J, Sanders K, Schott AM, Silman A, Torgerson D, van Staa T, Watts NB, Yoshimura N (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18(8):1033–1046. doi:10.1007/s00198-007-0343-y
Hans D, Schott AM, Duboeuf F, Durosier C, Meunier PJ (2004) Does follow-up duration influence the ultrasound and DXA prediction of hip fracture? The EPIDOS prospective study. Bone 35(2):357–363
Fujiwara S, Sone T, Yamazaki K, Yoshimura N, Nakatsuka K, Masunari N, Fujita S, Kushida K, Fukunaga M (2005) Heel bone ultrasound predicts non-spine fracture in Japanese men and women. Osteoporos Int 16(12):2107–2112
Hans D, Durosier C, Kanis JA, Johansson H, Schott-Pethelaz AM, Krieg MA (2008) Assessment of the 10-year probability of osteoporotic hip fracture combining clinical risk factors and heel bone ultrasound: the EPISEM prospective cohort of 12,958 elderly women. J Bone Miner Res 23(7):1045–1051. doi:10.1359/jbmr.080229
Hans D, Dargent-Molina P, Schott AM, Sebert JL, Cormier C, Kotzki PO, Delmas PD, Pouilles JM, Breart G, Meunier PJ (1996) Ultrasonographic heel measurements to predict hip fracture in elderly women: the EPIDOS prospective study. Lancet 348(9026):511–514
Krieg MA, Cornuz J, Ruffieux C, Van Melle G, Buche D, Dambacher MA, Hans D, Hartl F, Hauselmann HJ, Kraenzlin M, Lippuner K, Neff M, Pancaldi P, Rizzoli R, Tanzi F, Theiler R, Tyndall A, Wimpfheimer C, Burckhardt P (2006) Prediction of hip fracture risk by quantitative ultrasound in more than 7000 Swiss women > or =70 years of age: comparison of three technologically different bone ultrasound devices in the SEMOF study. J Bone Miner Res 21(9):1457–1463
Bauer DC, Ewing SK, Cauley JA, Ensrud KE, Cummings SR, Orwoll ES (2007) Quantitative ultrasound predicts hip and non-spine fracture in men: the MrOS study. Osteoporos Int 18:771–777
Diéz-Pérez A, Gonzalez-Macias J, Marin F, Abizanda M, Alvarez R, Gimeno A, Pegenaute E, Vila J (2007) Prediction of absolute risk of non-spinal fractures using clinical risk factors and heel quantitative ultrasound. Osteoporos Int 18(5):629–639. doi:10.1007/s00198-006-0297-5
Engelke K, Glüer CC (2006) Quality and performance measures in bone densitometry: part 1: errors and diagnosis. Osteoporos Int 17(9):1283–1292. doi:10.1007/s00198-005-0039-0
Njeh CF, Hans D, Li J, Fan B, Fuerst T, He YQ, Tsuda-Futami E, Lu Y, Wu CY, Genant HK (2000) Comparison of six calcaneal quantitative ultrasound devices: precision and hip fracture discrimination. Osteoporos Int 11(12):1051–1062
Moayyeri A, Adams JE, Adler RA, Krieg MA, Hans D, Compston J, Lewiecki EM (2012) Quantitative ultrasound of the heel and fracture risk assessment: an updated meta-analysis. Osteoporos Int 23(1):143–153. doi:10.1007/s00198-011-1817-5
Heistaro S (ed) (2008) Methodology report: health 2000 survey. National Public Health Institute, Publications of the National Public Health Institute B26/2008, Helsinki. Available at http://www.terveys2000.fi/doc/methodologyrep.pdf
Kauppi M, Impivaara O, Mäki J, Heliövaara M, Marniemi J, Montonen J, Jula A (2009) Vitamin D status and common risk factors for bone fragility as determinants of quantitative ultrasound variables in a nationally representative population sample. Bone 45(1):119–124. doi:10.1016/j.bone.2009.03.659
Aromaa A, Koskinen S (eds) (2004) Health and functional capacity in Finland. Baseline results of the health 2000 health examination survey. National Public Health Institute, Publications of the National Public Health Institute B12/2004, Helsinki. Available at http://www.terveys2000.fi/julkaisut/baseline.pdf
(2005) Finnish current care guideline for treatment of alcohol abuse. Duodecim 121:788–803. Updated 15 April 2010
Haara MM, Arokoski JP, Kröger H, Kärkkäinen A, Manninen P, Knekt P, Impivaara O, Heliövaara M (2005) Association of radiological hand osteoarthritis with bone mineral mass: a population study. Rheumatol (Oxford) 44(12):1549–1554
Royston P (2006) Explained variation for survival models. Stata J 6(1):83–96
Nurmi I, Kaukonen JP, Lüthje P, Naboulsi H, Tanninen S, Kataja M, Kallio ML, Leppilampi M (2005) Half of the patients with an acute hip fracture suffer from hypovitaminosis D: a prospective study in southeastern Finland. Osteoporos Int 16(12):2018–2024
Partanen J, Heikkinen J, Jämsä T, Jalovaara P (2002) Characteristics of lifetime factors, bone metabolism, and bone mineral density in patients with hip fracture. J Bone Miner Metab 20(6):367–375
Looker AC, Mussolino ME (2008) Serum 25-hydroxyvitamin D and hip fracture risk in older U.S. White adults. J Bone Miner Res 23(1):143–150. doi:10.1359/jbmr.071003
Cauley JA, LaCroix AZ, Wu L, Horwitz M, Danielson ME, Bauer DC, Lee JS, Jackson RD, Robbins JA, Wu C, Stanczyk FZ, LeBoff MS, Wactawski-Wende J, Sarto G, Ockene J, Cummings SR (2008) Serum 25-hydroxyvitamin D concentrations and risk for hip fractures. Ann Intern Med 149(4):242–250
Cauley JA, Parimi N, Ensrud KE, Bauer DC, Cawthon PM, Cummings SR, Hoffman AR, Shikany JM, Barrett-Connor E, Orwoll E (2010) Serum 25-hydroxyvitamin D and the risk of hip and nonspine fractures in older men. J Bone Miner Res 25(3):545–553. doi:10.1359/jbmr.090826
Hippisley-Cox J, Coupland C (2009) Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ 339:b4229
Collins GS, Mallett S, Altman DG (2011) Predicting risk of osteoporotic and hip fracture in the United Kingdom: prospective independent and external validation of QFractureScores. BMJ 342:d3651
Byberg L, Gedeborg R, Cars T, Sundstrom J, Berglund L, Kilander L, Melhus H, Michaelsson K (2012) Prediction of fracture risk in men: a cohort study. J Bone Miner Res 27(4):797–807. doi:10.1002/jbmr.1498
Hans D, Hartl F, Krieg MA (2003) Device-specific weighted T-score for two quantitative ultrasounds: operational propositions for the management of osteoporosis for 65 years and older women in Switzerland. Osteoporos Int 14(3):251–258
Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R (2005) Estimates of optimal vitamin D status. Osteoporos Int 16(7):713–716
Lips P, Chapuy MC, Dawson-Hughes B, Pols HAP, Holick MF (1999) An international comparison of serum 25-hydroxyvitamin D measurements. Osteoporos Int 9(5):394–397
Farahmand BY, Michaëlsson K, Baron JA, Persson PG, Ljunghall S (2000) Body size and hip fracture risk. Epidemiology 11(2):214–219
Trimpou P, Landin-Wilhelmsen K, Odén A, Rosengren A, Wilhelmsen L (2010) Male risk factors for hip fracture-a 30-year follow-up study in 7,495 men. Osteoporos Int 21(3):409–416. doi:10.1007/s00198-009-0961-7
Meyer HE, Tverdal A, Falch JA (1993) Risk factors for hip fracture in middle-aged Norwegian women and men. Am J Epidemiol 137(11):1203–1211
Faulkner KG, Cummings SR, Black D, Palermo L, Glüer CC, Genant HK (1993) Simple measurement of femoral geometry predicts hip fracture: the study of osteoporotic fractures. J Bone Miner Res 8(10):1211–1217. doi:10.1002/jbmr.5650081008
Moayyeri A (2008) The association between physical activity and osteoporotic fractures: a review of the evidence and implications for future research. Ann Epidemiol 18(11):827–835
Khaw KT, Reeve J, Luben R, Bingham S, Welch A, Wareham N, Oakes S, Day N (2004) Prediction of total and hip fracture risk in men and women by quantitative ultrasound of the calcaneus: EPIC-Norfolk prospective population study. Lancet 363(9404):197–202
Sund R, Nurmi-Lüthje I, Lüthje P, Tanninen S, Narinen A, Keskimäki I (2007) Comparing properties of audit data and routinely collected register data in case of performance assessment of hip fracture treatment in Finland. Methods Inf Med 46(5):558–566
Lüthje P, Nurmi I, Kataja M, Heliövaara M, Santavirta S (1995) Incidence of pelvic fractures in Finland in 1988. Acta Orthop Scand 66(3):245–248
Acknowledgments
This work was partly funded by a research grant from the Juho Vainio Foundation, Helsinki, Finland.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kauppi, M., Impivaara, O., Mäki, J. et al. Quantitative ultrasound measurements and vitamin D status in the assessment of hip fracture risk in a nationally representative population sample. Osteoporos Int 24, 2611–2618 (2013). https://doi.org/10.1007/s00198-013-2355-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2355-0