
Abstract
Summary
In a prospective cohort study of 395 geriatric outpatients, mortality after 3 years was associated with prevalent vertebral fractures at baseline. The mortality risk was independently associated with the presence of three or more vertebral fractures at baseline. In the surviving patients, the risk of incident fractures was noteworthy, occurring in 26 % of these patients.
Introduction
The purpose of this study is to determine mortality rate and the incidence of vertebral fractures in a geriatric outpatient group, during a 3-year follow-up period, in a teaching hospital in Amsterdam, The Netherlands.
Methods
This study includes a prospective cohort study of 395 geriatric patients who had their baseline visit at a diagnostic day hospital in 2007 and 2008. They were invited for follow-up 3 years later. Lateral X-rays of the lumbar spine and chest were performed at baseline and after 3 years; vertebral fractures were scored in all patients according to the semi-quantitative method of Genant.
Results
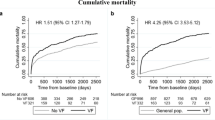
After 3 years, mortality was 46 % and associated with prevalent vertebral fractures at baseline (odds ratio (OR), 1.83; 95 % CI, 1.23–2.74). The presence of three or more vertebral fractures at baseline was an independent risk factor for mortality (OR, 3.32; 95 % CI, 1.56–7.07). Other independently associated risk factors were greater age, higher co-morbidity score, and having more prescriptions. Higher cognitive capacity protected against mortality after 3 years. In 72 patients, radiography was repeated. Nineteen patients (26 %) had an incident radiographic vertebral fracture: 16 in those with a prevalent fracture, and 3 in those without a prevalent vertebral fracture at baseline.
Conclusions
In geriatric outpatients, mortality after 3 years was associated with prevalent vertebral fractures at baseline, and the mortality risk was independently associated with 3 or more vertebral fractures at baseline. In survivors, the risk of incident fractures was noteworthy, since these occurred in 26 % of the patients, particularly in those with a prevalent vertebral fracture.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vertebral fractures are caused by severe osteoporosis, and prevalence in older subjects is up to 40 % in various population-based studies [1, 2]. Prevalence of vertebral fractures among geriatric patients who visit a diagnostic day clinic is even higher: in two different cohorts, prevalence was approximately 50 % (Van Hengel et al., unpublished data) [3]. Little is known about the incidence of vertebral fractures during a follow-up period in the very old. However, in placebo-controlled trials for anti-osteoporotic medication with older patients at high risk for incident vertebral fractures, the incidence of vertebral fractures was in the range of 15–31.5 % after 3 years [4–7]. In these trials, all patients had prevalent vertebral fractures, but they were selected for not having chronic diseases and therefore differed considerably from the majority of geriatric patients.
Vertebral fractures are associated with high morbidity such as pulmonary involvement, back pain, and a lower quality of life [8]. Moreover, they are associated with increased mortality in both older men and women [9–12]. These findings are from population-based studies and usually in community-dwelling elderly populations. The question arises whether geriatric patients suffer from the same morbidities and mortality risk. It could be hypothesized that geriatric patients, who have high comorbidity, have different risk factors for an incident or prevalent vertebral fracture. It was postulated that the frailty syndrome as a clinical entity could be associated with incident vertebral fractures in old age.
The present study was conducted to investigate the incidence of vertebral fractures after 3 years of follow-up in a geriatric population. Secondly, this study aims to investigate whether prevalent vertebral fractures at baseline were associated with a higher mortality rate. Thirdly, quality of life, burden of pain, mobility and frailty were investigated among the patients after 36 months of follow-up to identify possible associations for incident vertebral fractures in this patient group.
Methods
Participants
Consecutive geriatric outpatients who visited the diagnostic day hospital at the Slotervaart Hospital for the first time between April until August 2007 and between January until February 2008 were invited to participate. Baseline characteristics and methodology were published recently [3]. Their general practitioner referred them for various reasons including: memory complaints, mobility problems, or to help reduce polypharmacy. A comprehensive geriatric assessment was performed as a standard procedure on all these patients. Patients were included in the present study if they gave written informed consent, or in case of incapacity to consent, their legal substitute decision makers did. Patients were excluded if they were not able to undergo radiographs. The regional research ethical committee of the Slotervaart Hospital approved the study.
Measurements
At baseline, all patients had a chest X-ray (posterior–anterior and lateral) and a lateral lumbar spine X-ray. Comorbidity was scored using the Charlson Index score [13], the most extensively studied comorbidity index for predicting mortality [14]. Functional mobility was measured by the timed get-up-and-go test (TUG) [15], which is associated with increased fall risk [16]. Cognitive function was assessed by the minimal mental state examination (MMSE) [17]. Furthermore, blood samples for albumin and 25 OH-vitamin D were taken.
Three years after baseline measurements, patients were invited to attend a follow-up visit. Reasons for non-attendance at follow-up were recorded. For all patients who declined the follow-up visit, medical files were searched for spinal radiography in the follow-up period. In case of mortality, the general practitioner was asked for cause of death. At the follow-up visit, radiography was repeated. Medication was documented. Quality of life was investigated by the Qualeffo, a 41 self-reporting questionnaire [18]. The perceived burden of pain was assessed with a visual analogue scale for pain (VAS). The geriatric depression scale (15 items) [19] was assessed. Frailty was scored according to the Fried criteria [20]. Frailty was defined as the presence of three of the next five items: unintentional weight loss (5 kg in the past year), self-reported exhaustion, weakness (grip strength), slow walking speed (less than 0.76 m/s), and low physical activity (kilocalories spent per week for males, <383 and for women, <270 or more than 4 h/day sitting in a chair without walking a longer distance once per month or biking or jogging [20]).
Diagnosis of vertebral fractures
Two investigators (HJ and MV) scored vertebral fractures using the semi-quantitative method of Genant [21]. This method is validated in comparison to quantitative morphometry in various studies [22, 23]. Fractures were categorized by severity (grade 1—mild, 20–25 % loss of height; grade 2—moderate, 25–40 % loss of height; and grade 3—severe, >40 % loss of height) and fracture type (wedge, biconcave, or crush fracture). When patients had more than one fracture, the most severe fracture was categorized. The two observers scored every X-ray separately for vertebral fractures. In cases where the conclusion did not match, consensus was reached by discussion. This diagnosis was considered as gold standard. Discussion was needed in 7 % of the cases, which matches a kappa of 0.73. Incident vertebral fractures were defined as a new vertebral fracture, in a vertebra without a preexisting fracture. Vertebral fractures with progression during follow-up, e.g., a grade 1 vertebral fracture became a grade 2 or 3 vertebral fracture, were categorized separately.
Statistics
The Statistical Package for the Social Sciences (version 18.0 for Windows, SPSS, Inc., Chicago IL.) was used for statistical analyses. Baseline data were analyzed for two groups: patients alive after 3 years and those deceased during follow-up. In addition, baseline characteristics were compared between the group of non-returners who were still alive after 3 years and could have returned and patients who did return for follow-up. The patients examined at follow-up were categorized into two groups: those with incident vertebral fractures and those without.
Values of TUG above two standard deviations of the mean (>40 s) were considered outliers and left out of further analysis. After this adjustment, all variables met the normality assumptions and parametric tests were used. For univariate analyses, Chi-square tests were used for categorical variables and independent t tests were used for continuous variables. Thereafter, binary logistic regression analysis was performed to select risk factors for mortality. All variables with p < 0.10 were included in the multivariate analysis, adjusted for sex. The TUG was completed by less than 50 % of the patients, due to severe immobility, and was therefore left out of the regression analysis. Both forward and backward analysis was used, and both methods showed the same risk factors. A two-sided probability of p < 0.05 was considered statistically significant.
For group differences between the returners and the non-returners who might have returned, (leaving out the deceased, terminally ill, the severe immobile patients, and the dementia patients), the Chi-square test for categorical variables was used, and one-way ANOVA for continuous variables. Because of the selection of returned patients in comparison to the non-returners and the small groups size, we did not perform a multivariate regression in this group. To describe the chance of an incident vertebral fracture for patients with a prevalent fracture, the Chi-square test was used.
Results
At baseline, 442 patients were screened, of whom 395 were included in the study. The baseline characteristics of the cohort are described in Table 1. Fifty-two percent of the patients had prevalent vertebral fractures, the mean age was 82 years, and 63 % was female. After a follow-up period of 3 years, 182 (46 %) patients had died, 47 % of the men and 45 % of the women.
Mortality
The baseline characteristics of the deceased patients and of the patients alive after 3 years are shown in Table 1. Both groups differed significantly at baseline: deceased patients were older (84 vs. 81 year; p < 0.001), had a higher risk of previous hip fracture (18 % vs. 6 %; p = 0.005), more chronic diseases (mean, 2.8 vs. 1.7; p < 0.001), more prescriptions per patient (6.1 vs. 4.9; p = 0.002), a lower serum albumin (35.0 vs. 36.9.0 g/l; p < 0.001), and more often a prevalent vertebral fracture (61 % vs. 46 %; p = 0.003).
In the second column of Table 1, the univariate analyses are shown. The odds ratio (OR) for the chance of dying in the follow-up period for patients with a prevalent vertebral fracture is 1.83 (95 % CI, 1.23–2.74), compared with the patients without a vertebral fracture at baseline. The presence of a more severe prevalent vertebral fracture raises the odds of mortality during follow-up: patients with a grade 3 fracture as their most severe fracture had an OR for death of 3.12 (95 % CI, 1.76–5.52) compared with no vertebral fracture at baseline. The number of prevalent vertebral fractures raises the OR of mortality to 3.07 (95 % CI, 1.61–5.84) for three or more vertebral fractures.
Multivariate regression analysis (third column of Table 1) showed several independent risk factors for mortality in this cohort. For every year of incremental age at baseline, the odds of dying is raised by a factor of 1.06 (95 % CI, 1.02–1.27). For every point on the Charlson index, the risk of dying was also elevated (OR, 1.46; 95 % CI, 1.18–1.82). Likewise, every additional prescription elevated the chance of dying too (OR, 1.15; 95 % CI, 1.04–1.28). A higher score on the MMSE (every point in this test above the mean of 21 points) was independently associated with survival (OR, 0.94; 95 % CI, 0.89–0.99). Presence of a grade 3 vertebral fracture at baseline was not independently associated with mortality at 3 years, but the presence of three or more vertebral fractures at baseline was after multivariate regression independently associated with mortality (OR, 3.32; 95 % CI, 1.56–7.07).
Cause of death was known in 48 % (88 of 182) of the cases. There were no differences between deceased patients with and without prevalent vertebral fractures for cause of death (p value of 0.53; data not shown).
Incident vertebral fractures
Of the 395 included patients at baseline, only 149 could have attended a follow-up visit (182 deceased, 15 severe immobile patients, 44 patients with dementia or living in nursing homes, and 5 terminally ill (395–246 = 149; Table 2). Only 50 patients, of whom 37 were women, were able and willing to come back to the hospital for a follow-up visit after invitation. The non-returned patients had multiple reasons for declining the invitation (Table 2). Twenty-two non-returning patients (of whom 13 women) from the cohort had radiography of the chest and or lumbar spine during follow-up time for various reasons. The mean time to follow-up of the 22 patients was 29 months (range, 10–39 months; median, 28 months). The baseline characteristics of the 50 and 22 patients (72/149 = 48 % of the total baseline cohort) are described in Table 3. Compared with non-returners who could have attended a follow-up, the returners and the 22 who had radiography, had a higher prevalence of vertebral fractures at baseline (p = 0.04). Their cognitive function measured with the MMSE was higher than the non-returners (p = 0.01). Four patients used anti-osteoporotic medication at the return visit.
Incident vertebral fractures occurred in 19 of the 72 (26 %) patients; three patients had a worsening of their prevalent vertebral fracture, and 50 had no change on their radiography (Fig. 1). Sixteen of the 39 (41 %) patients with a prevalent vertebral fracture had an incident fracture. Of the 33 patients without a prevalent vertebral fracture, only 3 (9 %) had a new vertebral fracture. The OR that a patient with a prevalent fracture at baseline suffers from an incident vertebral fracture in the next 3 years, compared with the patient without a prevalent vertebral fracture was 6.4 (95 % CI, 1.68–24.77; p value of 0.006).

Distribution of the patients with radiography during follow-up and after 3 years. Nineteen incident vertebral fractures (VF) have occurred; 16 in the group with prevalent VF at baseline
Quality of life, pain, mobility, and frailty
Of the 50 patients who had a return visit, quality of life, pain, functional mobility, and frailty were assessed among 45 patients. Of the remainder, four patients had severe cognitive impairments and did not understand and complete the tests and one patient gave consent for radiography but did not complete the questionnaire. The scores of the Qualeffo, VAS pain score, TUG, walking speed test, and the frequency of frailty, were not significantly different between the group with incident vertebral fractures and the group without incident fractures (Table 4).
Discussion
The present study was conducted to determine the mortality and the incidence of vertebral fractures after 3 years among geriatric outpatients. There was a high mortality rate in this cohort (as expected), and mortality was independently associated with three or more vertebral fractures at baseline.
In the surviving patients who were reassessed, there was a high incidence of vertebral fractures (26 %). This is particularly remarkable since the returning patients at the outpatient clinic after 3 years of follow-up were healthier at baseline than the non-returners.
To our knowledge, this is the first study that investigated prevalent vertebral fractures and the association with mortality in geriatric outpatients. There are recent studies showing the association between (asymptomatic) vertebral fractures and mortality [10–12], but none of these studies had predominantly patients of this high age.
High mortality rates of 46 % after 3 years are not surprising in geriatric outpatients who were over 82 years at baseline, with high frequencies of functional impairment and chronic diseases. Compared with the Dutch national statistics, mortality in this study was doubled for both sexes, because in the general population of Dutch population of persons aged 82 years, 3-year mortality rates were 28 % for men and 19 % for women [24]. Although a lot of risk factors for mortality were present, which reflect the underlying health status in this population, it is striking that in this patient group mortality was also independently and strongly associated with three or more vertebral fractures at baseline. There are studies showing that clinical fractures are independently associated with mortality [25, 26], but there are also studies showing the opposite [27–30]. There are two other studies [31, 32] which showed that prevalent vertebral fractures and mortality in older women is independently associated. It has also been reported earlier that there is an association between the number of vertebral fractures and mortality [10, 11, 33] but not independently.
Vertebral fractures in geriatric patients appear to affect mortality, but its pathway is not fully elucidated. It could be that mortality and vertebral fractures are outcomes of the same underlying factor: age is probably the most important one. One possibility we did not test was that increasing the number of vertebral fractures had an adverse affect on respiratory function through the deforming effects of spinal kyphosis. In addition, the so-called frailty syndrome is another option. Frailty was identified as independent predictor for recurrent falls, hip fracture, and death in a population-based study of women over 80 years old [30]. Unfortunately, several definitions of the frailty syndrome exist. It is a limitation of this study that the frailty syndrome was not measured at baseline.
Only 50 patients had a return visit, and 45 % (72/159) of the patients who could have returned after 3 years, had radiography during follow-up period. This low number is typical for this patient group and shows the difficulty of follow-up studies with a long interval in patients with high comorbidity, severe immobility, and limited life expectancy. Although this study did not have many returners, it was a strength that data of the lost to follow-up patients were collected.
This study also shows that the patients who did come back for the return visit were the healthier members of the cohort—the so-called healthy cohort effect [34]. They were significantly younger, had less comorbidity, and less cognitive disorders at baseline than patients who were not able to return. Remarkably, returning patients had a higher prevalence of vertebral fractures at baseline.
The returning patients had a high incidence rate for vertebral fractures, but there was a possible underestimation of the high incidence in the present study. The 22 patients with radiography during follow-up had a mean follow-up time of 29 months, and the patients without an incident vertebral fracture in this group could have had an incident vertebral fracture some time later but within the 36 months.
In particular, the geriatric patients with prevalent vertebral fractures had a very high chance (41 %) of suffering from an incident vertebral fracture in the next 3 years. This high rate exceeds the incidence rates of placebo-controlled trials in osteoporotic patients [4–7] and has not been described before. Although these patients would quite likely have been offered anti-osteoporotic medication, they were not taking such medication at the return visit. Non-adherence for oral anti-osteoporotic medications in the general population is reportedly up to 50 % at 1 year [35]; theoretically, it can be expected that the non-adherence rate is even higher in the elderly. Because of the high incidence of vertebral fractures in this patient group with prevalent vertebral fractures at baseline, anti-osteoporotic medication should be proposed more energetically. There are several well-tolerated anti-osteoporotic drugs, which are also effective in the older population [36].
Our hypothesis that the patients with an incident vertebral fracture had more pain, lower quality of life, and were more frail, was not confirmed in this study, probably related to the small proportions of patients returning for follow-up. Quality of life scores were adverse in both groups, suggesting that in the oldest old who come to attention of this clinical service quality of life is generally poor. Frailty was more often present in the group of patients with incident vertebral fractures and had a trend to significance.
Conclusions
In geriatric hospital outpatients aging an average of 82 years, about half had at least one vertebral fracture at recruitment. Mortality at 3 years was associated with prevalent vertebral fractures at baseline, and the risk of death was independently associated with three or more vertebral fractures. In survivors who lived for 3 years and were examined radiologically, the incidence of new vertebral fractures was remarkably high at 41 % of those with a prevalent vertebral fracture at baseline vs. 9 % in those without. The presence of vertebral fractures in this age group increases substantially the risk of further vertebral fractures and is associated with increased mortality when they become multiple. The opportunity to protect these frail patients with anti-fracture medication is currently being missed.
References
Melton LJ 3rd, Atkinson EJ, Cooper C, O’Fallon WM, Riggs BL (1999) Vertebral fractures predict subsequent fractures. Osteoporosis Int 10:214–221
Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB et al (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285:320–323
der Jagt-Willems V, van Hengel M, Vis M et al (2012) Why do geriatric patients have so many vertebral fractures? Exploring prevalence and riskfactors. Age Ageing 41:200–206
Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC et al (1996) Randomized trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet 348:1535–1541
Ettinger B, Black DM, Mitlak BH, Knickerbocker RK, Nickelsen T, Genant HK, Christiansen C et al (1999) Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: result from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA 282:637–645
Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML et al (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral efficacy with Risedronate Therapy (VERT) Study Group. Osteoporosis Int 11:83–91
Reginster JY, Seeman E, De Vernejoul MC, Adami S, Compston J, Phenekos C et al (2005) Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: Treatment of Periferal Osteoporosis (TROPOS) Study. J Clin Endocrinol Metab 90:2816–2822
Ross PD (1997) Clinical consequences of vertebral fractures. Am J Med 103:30S–42S
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR (1999) Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 159:1215–1220
Trone DW, Kritz-Silverstein D, Von Muhlen DG, Wingard DL, Barrett-Connor E (2007) Is radiographic vertebral fracture a risk factor for mortality? Am J Epidemiol 166:1191–1197
Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR (2009) Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA 301:513–521
Charlson ME, Pompei P, Ales K, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 40:373–383
De Groot V, Beckerman H, Lankhorst GJ, Bouter LM (2003) How to measure comorbidity. A critical review of available methods. J Clin Epidemiol 56:221–229
Podsiadlo D, Richardson S (1991) The timed up and go: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39:142–148
Shumway-Cook A, Brauer S, Woollacott M (2000) Predicting the probabillity for falls in community-dwelling older adults using the timed up & go test. Phys Ther 80:896–903
Folstein MF, Robins LN, Helzer JE (1983) The mini-mental state examination. Arch Gen Psychiatry 40:812
Lips P, Cooper C, Agnusdei D, Caulin F, Egger P, Johnell O et al (1999) Quality of life in patients with vertebral fractures: validation of the Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO). Working Party for Quality of Life of the European Foundation for Osteoporosis. Osteoporosis Int 10:150–160
van Marwijk HWJ, Wallace P, De Bock GH, Hernans JO, Kaptein AA, Mulder JD (1995) Evaluation of the feasibility, reliability and diagnostic value of shortened versions of the geriatric depression scale. Br J Gen Pract 45:195–199
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J et al (2001) Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 56:M46–M56
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Black DM, Palermo L, Nevitt MC et al (1995) Comparison of methods for defining prevalent vertebral deformities: the study of osteoporotic fractures. J Bone Miner Res 10:890–902
Grados F, Roux C, de Vernejoul MC, Utard G, Sebert JL, Fardellone P (2001) Comparison of four morphometric definitions and a semiquantitative consensus reading for assessing prevalent vertebral fractures. Osteoporos Int 12:716–722
Statline (2007). http://statline.cbs.nl/StatWeb/publication/?VW=T&DM=SLNL&PA=70701NED&D1=85&D2=a&D3=83&D4=57&HD=120622-0916&HDR=G1,T&STB=G2,G3
Cauley JA, Thompson DE, Ensrud KC, Scott JC, Black D (2000) Risk of mortality following clinical fractures. Osteoporos Int 11:556–561
Pongchaiyakul C, Nguyen ND, Jones G, Center JR, Eisman JA, Nguyen TV (2005) Asymptomatic vertebral deformity as a major risk factor for subsequent fractures and mortality: a long-term prospective study. J Bone Miner Res 20:1349–1355
Tosteson AN, Gottlieb DJ, Radley DC, Fisher ES, Melton LJ 3rd (2007) Excess mortality following hip fracture: the role of underlying health status. Osteoporos Int 18:1463–1472
Browner WS, Seeley DG, Vogt TM, Cummings SR (1991) Study of osteoporotic fractures research group. Non-trauma mortality in elderly women with low bone mineral density. Lancet 338:355–358
Kado DM, Duong T, Stone KL et al (2003) Incident vertebral fractures and mortality in older women: a prospective study. Osteoporos Int 14:589–594
Ensrud KE, Ewing SK, Taylor BC, Fink HA, Stone KL, Cauley JA et al (2007) Frailty and risk of falls, fracture and mortality in older women: the study of osteoporotic fractures. J Gerontol A Biol Sci Med 62:744–751
Ismail AA, O’Neill TW, Cooper C, Finn JD, Bhalla AK, Cannata JB et al (1998) Mortality associated with vertebral deformity in men and women: results from the European Prospective Osteoporosis Study (EPOS). Osteoporos Int 8:291–297
Ensrud KE, Thompson DE, Cauley JA et al (2000) Prevalent vertebral deformities predict mortality and hospitalization in older women with low bone mass. Fracture Intervention Trial Research Group. J Am Geriatr Soc 48:241–249
Bruyere O, Roux C, Nicolet D et al (2012) Severity of incident vertebral fracture and future fracture risk: a 3 year prospective study. Abstract OC6 on ECCEO
Posthuma WF, Westendorp RG, Vandenbroucke JP (1994) Cardioprotective effect of hormone replacement therapy in postmenopausal women: is the evidence biased? BMJ 308:1268–1269
Netelenbos JC, Geusens PP, Ypma G, Buijs SJ (2011) Adherence and profile of non-persistence in patients treated for osteoporosis—a large scale, longterm retrospective study in the Netherlands. Osteoporosis Int 22:1537–1546
Inderjeeth CA, Foo AC, Lai MM, Glendenning P (2009) Efficacy and safety of pharmacological agents in managing osteoporosis in the old: review of the evidence. Bone 44:744–751
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
van der Jagt-Willems, H.C., Vis, M., Tulner, C.R. et al. Mortality and incident vertebral fractures after 3 years of follow-up among geriatric patients. Osteoporos Int 24, 1713–1719 (2013). https://doi.org/10.1007/s00198-012-2147-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-012-2147-y