
Abstract
Summary
While the association of lean mass (LM) with bone mass is well understood, the association of fat mass (FM) with bone mass is controversial. Our results support that adolescents with higher levels of adiposity have greater bone mass, but this association is fully explained by their higher levels of LM.
Introduction
We aimed (1) to study the independent association of FM and LM with bone mass and (2) to study the differences in bone mass by weight status in adolescents, after controlling for relevant confounders, such as physical activity (PA), calcium intake, and LM.
Methods
Participants were 330 adolescents (167 boys, 12.5–17.5 years) from the HELENA study. The relationships of FM (DXA, n = 330; BodPod, n = 282) and LM (DXA, n = 330) with different bone variables (whole body, total hip, lumbar spine, and femoral neck) were analyzed by linear regression, and differences between weight status were analyzed by ANCOVA.
Results
Fat mass (DXA) was positively associated with bone variables in both sexes, after adjustment for height, calcium intake, and sexual maturation. Additional adjustment by PA slightly increases the associations. However, adjustment for LM inverted these associations. Similar results were obtained using BodPod instead of DXA for assessing FM. Overweight/obese adolescents had higher BMC than their non-overweight peers in most of regions studied. Additional adjustment for PA slightly increased the differences between weight status groups, while adjusting for LM inverted the associations. LM was strong and positively associated with all bone variables in both sexes. Additional adjustment for PA or FM did not change the results.
Conclusions
Adolescents with higher levels of adiposity have greater bone mass, but this association is explained by their higher levels of LM.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a disease characterized by decreased bone mass and bone tissue deterioration [1]. Acquiring a high bone mass during childhood and adolescence is a key determinant of adult skeletal health [2] and it may decrease the risk of osteoporotic fractures by 50% [3, 4]. Although genetics plays an important role on bone mass, environmental and lifestyle factors such as physical activity (PA) [5] and nutrition, i.e., calcium intake [6] have important osteogenic effects.
Lean mass (LM) is a major predictor for bone mineral content (BMC) and for bone accumulation during puberty [7, 8]. During this period of life, increases in LM contribute to increase bone mass, as explained by the mechanostat theory (bigger muscles exert higher tensile forces on the bones they attach) [9, 10]. Therefore, PA and sport participation could indirectly increase bone mass via increasing LM. In addition, sport participation has a direct influence on bone mass because of the extra load that some sport activities have on the bone [11, 12].
While the role of LM in bone formation is well understood, much less is known about fat mass (FM) and bone mass. Some studies have suggested that FM is positively related to bone mass in girls [13, 14], which has been longitudinally confirmed [15, 16]; whereas, others have observed that FM is negatively associated with bone mineral density (BMD) in boys [13, 17].
Whether overweight and obese people have a better or worse bone health is unknown. Hypothetically, both a positive and negative association could be reasonable. Overweight and obese people are known to have both greater body weight and LM, involving an extra load on the skeleton and higher tensile forces on bones. As a consequence of this greater LM, they could have higher bone mass. On the other hand, overweight and obese people are known to be less active than their normal peers [18], and because of these low activity levels, they could be at a higher risk for low bone mass. However, the literature on this topic is contradictory. Therefore, it could be hypothesized that, independently of their PA levels, overweight and obese people could have greater bone mass, result of the higher LM developed as consequence of their higher FM, which is a new point of view on this topic.
Several studies have shown that overweight and obese children and adolescents have higher levels of BMC and BMD [19-22], while others have observed the opposite [23, 24]. Most of previous studies have not properly adjusted for relevant confounders, such as PA, calcium intake, or LM. Since adolescence is a key period of life for bone development, to analyze the role of FM and LM on bone mass as well as to know whether this relationships depends on weight status are of high interest. This is especially important in girls, as they are less active [25], with higher FM, lower LM, and at higher risk for developing osteoporosis in adulthood than boys [26].
Therefore, we aimed (1) to study the association of FM and LM on bone mass in adolescents after adjusting for each other, PA and calcium intake, and (2) to study the differences in bone mass by weight status in adolescents, after controlling for relevant confounders, such as PA, calcium intake, and LM.
Methods
Subjects
The Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA) study is a European Union-funded project that included a cross-sectional, multicentre study (HELENA-CSS) conducted on adolescents aged 12.5–17.5 yrs from 10 European cities in 2006–2007 [27]. The general characteristics of the HELENA-CSS have been described in detail elsewhere [28]. In this report, we focus on the sample from Zaragoza, one of the 10 centres involved in the HELENA study, where BMC and BMD were measured by dual-energy X-ray absorptiometry (DXA). After exclusion of 60 subjects since they did not fulfill all the inclusion criteria for our study, a total of 167 boys and 163 girls with complete data on DXA (bone, FM, and LM), height, objective PA, calcium intake, and sexual maturation assessment were included in the analyses. Fat mass was also measured by air displacement plethysmography using the BodPod device in a subsample of 282 adolescents (48 missing values). The participants included in the study did not differ from those excluded in weight, height, and body mass index (BMI, p > 0.3). Signed informed consent was obtained from parents and adolescents, and the protocol was approved by the ethics committee of clinical research from the government of Aragón (CEICA, Spain) [29].
Anthropometric measurements
International guidelines for anthropometry in adolescents were used in the HELENA study [30]. While the participants were barefoot and clad in light indoor clothing, body weight (in kilograms) and height (in centimeters) were measured with an electronic scale (Type SECA 861), precision 100 g, range 0–150 kg, and a stadiometer (Type Seca 225), precision 0.1 cm, range 70–200 cm, respectively.
Definition of weight status
Body mass index was calculated as body mass (in kilograms) divided by height (in meters) squared. Participants were categorized according to the international gender and age-specific BMI (in kilograms per square meter) cutoff points [31, 32]. The cutoff points were equivalent to those internationally accepted for adult population, i.e., underweight (BMI <18.5 kg/m2), normal weight (BMI = 18.5–24.9 kg/m2), overweight (BMI = 25–29.9 kg/m2), and obesity (BMI ≥30 kg/m2). Weight status was recoded as a dichotomic variable: non-overweight (underweight + normal weight) and overweight/obese (overweight + obese), because of the low sample size in the underweight and obese groups.
Pubertal development
Physical examination was performed by a physician aiming to classify the adolescents in one of the five stages of pubertal maturity defined by Tanner and Whitehouse [33].
Bone, lean and fat mass (DXA)
Adolescents were scanned with DXA (Hologic Explorer scanner, using a pediatric version of the software QDR-Explorer; Hologic Corp., software version 12.4, Bedford, MA, USA). DXA equipment was calibrated using a lumbar spine phantom as recommended by the manufacturer. For the whole body measurement, subjects were scanned in supine position and the scans were performed at high resolution [34]. The BMD (in grams per square centimeter), area (in square centimeters), FM (in grams), and LM (in grams) [body mass – (FM + bone mass)] were determined for each individual from total and regional analysis of the whole body scan. Bone mineral content (in grams) was calculated using the formula BMC = BMD × area. Two additional examinations were conducted to estimate bone mass at the lumbar spine (mean L1–L4) and proximal region of the femur (total hip and femoral neck) as previously described [7].
We have previously examined the test–retest (with repositioning) precision error for regional analysis of the complete body scan, using coefficients of variation (CV) in 49 adolescents. The CV were: BMC = 2.3%, BMD = 1.3%, bone area = 2.6%, and fat-free lean mass = 1.9% [35].
Fat mass (BodPod)
Body volume was measured by BodPod (Body Composition System; Life Measurement Instruments, Concord, CA) using standardized procedures [36]. The BodPod was calibrated daily according to the manufacturer's guidelines. Subjects wore clothing according to the manufacturer's recommendation (a swimsuit and a swim cap) to rule out air trapped in clothes and hair. Adolescents were weighted on the BodPod calibrated digital scale and then entered the BodPod chamber. Body volume was measured two times by the machine to ensure measurement reliability. If the first two readings for body volume differed by more than 150 ml, a third measurement was taken. If additional readings were needed, the BodPod was recalibrated and the measurements were repeated for that subject [37]. Percentage of whole body FM was calculated using the equation reported by Siri [38, 39]. Thoracic gas volume was measured following the manufacturer's recommendations [36]. This value was integrated into the calculation of body volume. Whole body FM was calculated as percentage of whole body FM multiplied by body mass (in kilograms) and then divided by 100.
Calcium intake
Mean daily calcium intake was estimated from a two non-consecutive, 24-h recalls using the HELENA-DIAT (Dietary Assessment Tool) software [40]. For the assessment of calcium intake, the food composition tables published by Farrán et al. [41] were used for the Spanish adolescents. The calcium intake/LM ratio (in milligrams per kilogram) was also calculated.
Physical activity
A uniaxial accelerometer (Actigraph GT1M; Manufacturing Technology Inc. Pensacola, FL, USA) was used to assess PA. Adolescents were instructed to place the monitor underneath the clothing, at the lower back, using an elastic waist band and wear it for seven consecutive days. They were also instructed to wear the accelerometer during all times awake and only to remove it during water-based activities. At least 3 days of recording with a minimum of 8 h registration per day was set as an inclusion criterion. The time sampling interval (epoch) was set at 15 s. Average PA was calculated as the total number of counts per epoch divided by total daily registered time (counts per minute) [37].
Statistics
All the residuals showed a satisfactory pattern (normal distribution). Data are presented as mean values ± standard deviation unless otherwise stated. Gender differences were assessed by one-way analysis of variance (ANOVA). Relationships of FM (measured with DXA and BodPod) with different bone mass related variables (i.e., whole body, total hip, lumbar spine, and femoral neck) were analyzed using multiple linear regression models, including height, calcium intake, and sexual maturation as covariates (model 0). Model 1 included model 0 + average PA to test the role of PA in this association. Model 2 included model 1 + LM to test the role of LM in this association. The same procedure was used to analyze the relationships of LM with bone mass, but with adjustment for FM instead of LM (model 2).
In order to analyze the role of body composition in the association between bone mass related variables and weight status, one-way analysis of covariance (ANCOVA) was performed. The categorized variable of BMI was entered as a fixed factor, bone mass related variables were entered as dependent variables, and, in addition to the previous confounders (i.e., height, calcium intake, and sexual maturation), the average PA and LM were gradually entered as confounders.
All the analyses were performed using the Statistical Package for Social Sciences software (SPSS, v. 15.0 for WINDOWS; SPSS Inc., Chicago, IL, USA), and values of p < 0.05 were considered statistically significant.
Results
Table 1 shows descriptive characteristics (mean ± SD) of the study sample. The ANOVA showed that there were no differences between boys and girls in the mean age, BMD, BMI, and calcium intake/lean mass ratio; however, most traits differed by gender.
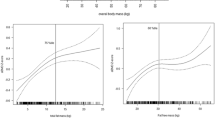
Table 2 shows the association between FM (DXA and BodPod) and bone mass after adjusting by potential sets of confounders. Fat mass (DXA) was positively associated with whole body and femoral neck BMC in boys [semi-partial correlation (semip corr), 0.200 and 0.130; p = 0.001 and 0.05, respectively]. Additional adjustment by PA slightly increases the positive association between FM and whole body BMC, femoral neck BMC, and BMD (semip corr, 0.139 to 0.213; p < 0.001 to 0.049). Finally, the inclusion of LM as a covariate inverted the associations between FM and most of bone mass related variables (semip corr, −0.112 to −0.270; p < 0.001 to 0.012). Similarly, FM was positively associated with most of bone mass related variables in girls (semip corr, 0.155 to 0.295; p < 0.001 to 0.018), except for total hip and lumbar spine BMC (p = 0.057 to 0.339). Additional adjustment for PA slightly increase the positive association between FM and all bone mass related variables (semip corr, 0.163 to 0.302; p < 0.001 to 0.014), except for the lumbar spine BMC (p = 0.071). Finally, additional adjustment for LM inverted the associations between FM and total hip and lumbar spine BMC (semip corr, −0.130 to−0.156; p = 0.006 to 0.025). Similar results were obtained when using BodPod instead of DXA for assessing FM.
Table 3 shows the association between LM and bone mass after adjusting by potential sets of confounders. Lean mass was strong and positively associated with all bone mass related variables in boys (semip corr, 0.426 to 0.632; all p < 0.001). Additional adjustment for PA (semip corr, 0.409 to 0.615; all p < 0.001) as well as FM (semip corr, 0.395 to 0.587; all p < 0.001) did not change the results. Slightly weaker associations were obtained between LM and bone mass in girls (semip corr, 0.358 to 0.626; all p < 0.001). Additional adjustment for PA (semip corr, 0.339 to 0.601; all p < 0.001) as well as FM (semip corr, 0.247 to 0.534; all p < 0.001) did not change the results.
Figure 1a shows the differences in bone-related variables by weight status in boys. Overweight/obese boys (n = 42) had higher BMC at the whole body than their non-overweight peers (n = 125). Additional adjustment for PA showed slightly higher differences between weight status groups. However, when adjusting for LM, the association between weight status and most of bone-related variables (both BMC and BMD) was inverted (p < 0.05).


Bone mineral content and density in relation to weight status in boys (a) and girls (b). Whole body, total hip, lumbar spine, and femoral neck scans.  adjusted by confounders (height, calcium intake, and sexual maturation),
adjusted by confounders (height, calcium intake, and sexual maturation),  adjusted by confounders + average PA,
adjusted by confounders + average PA,  adjusted by confounders + average PA + lean mass. Lines between points are shown only to facilitate the interpretation of the figure, i.e., which means (points) belong to a same model, and how the difference between means is modified after adjustment for several confounders
adjusted by confounders + average PA + lean mass. Lines between points are shown only to facilitate the interpretation of the figure, i.e., which means (points) belong to a same model, and how the difference between means is modified after adjustment for several confounders
Figure 1b shows that overweight/obese girls (n = 30) had higher BMC and BMD than their non-overweight peers (n = 133) in most of the regions analyzed. Additional adjustment for PA resulted in slightly higher differences between weight status groups, while adjusting for LM, inverted the associations between weight status and BMC (p < 0.05) and eliminated the association with BMD (p > 0.1).
Discussion
The findings of the present study indicate that adolescents with higher levels of adiposity have greater bone mass, yet this association is fully explained by their higher LM. In fact, once LM is accounted for, the association between FM and bone mass become negative in most of the bone variables studied. This finding is consistent when using two accurate methods to assess FM, i.e., DXA and BodPod. Physical activity does not seem to have an important confounding role in these associations.
Some studies have analyzed the association of FM on bone mass, obtaining contradictory results [13-17, 42], probably due to adjustment or not for key confounders. Some studies have reported positive associations between FM and bone mass in children and adolescents, after controlling for age, sex, and height [14, 15]. However, the study of Weiler et al. [42] showed a negative relationship between FM and BMC and BMD in 10–19-year girls, after controlling for age, weight, and height. Others have reported a positive association between FM and whole body BMD in girls and negative associations with whole body and lumbar spine BMD in boys [13], after adjusting for LM. In our study, the positive associations between FM and bone mass became inverse after including LM as a confounder, both in boys and girls. The relationship between bone mass and weight status has been widely discussed. Some studies have shown that BMC and BMD are higher in overweight or obese children and adolescents [19-22]. In contrast, opposite results have been found after controlling for some potential confounders such as sexual maturation [23] or LM [24]. The present study took into account a set of potential confounders that have been shown to be associated with bone mass, such as height, calcium intake, sexual maturation, average PA and LM. Further ANCOVA's were performed including LM as a covariate (in addition to the previous confounders), in order to analyze the influence of LM in the association bone–weight status.
The results of the present study show that overweight/obese boys had higher BMC at the whole body than their non-overweight peers, and overweight/obese girls had higher BMC and BMD in most of analyzed regions than their non-overweight peers. Additional adjustment for PA (counts per minute) did not result in remarkable changes. Therefore, in spite that overweight and obese adolescents have shown to be less active than their normal peers [18], these differences in activity levels do not seem to be enough to have an adverse effect on bone mass. After controlling for LM, the association between weight status and bone was inverted in most of analyzed regions, indicating that the higher levels of bone mass in overweight/obese adolescents were explained by their higher LM. Our results support previous studies that used LM as a confounder [24, 43].
Two main mechanisms might explain the observed associations: (1) obese people had larger muscles and larger muscles determine higher bone mass and (2) the bones of heavier people could be more stimulated than those from normal weight people, due to the extra load that a high weight has in everyday life activities, like walking, jumping, etc. With our data we can mainly support the first mechanism but we could not confirm or reject the second one. This suggests that FM could indirectly increase bone mass via LM. However, once LM is controlled, most of the associations between FM and bone were inverted and became negative, indicating that FM per se has no beneficial effect on bone mass.
The role of LM as a major predictor of bone mass during puberty is well understood [7, 8]. The present study confirms the strong and positive association between LM and bone mass previously reported [14, 15], even after controlling for PA, calcium intake, and FM. The association was stronger in boys than in girls, also in agreement with previous studies [14, 16].
Limitations and strength
Some limitations of this study deserve comment. Although we controlled for several potential confounders, we cannot be certain that other unmeasured confounders such as dietary intake or genetic variation have not influenced our observations. Cross-sectional studies only can provide suggestive evidence concerning causal relationships. However, in this specific case, it seems reasonable to think that FM or LM can influence BMC or BMD, whereas it is not so clear the mechanisms by which bone mass could determine higher or lower levels of FM or LM.
The use of sophisticated methods, such as DXA to assess body composition, BodPod to assess FM (recognized as the “gold standard” method), and the use of accelerometers to assess PA are strengths of the study. This study includes a rather complete set of confounders, i.e., height, sexual maturation, calcium intake, average PA, FM and LM, which is crucial to examine the current research question.
Conclusions
Adolescents with higher levels of adiposity have greater bone mass, but this is not the result of their higher FM. Our results suggest that this association is fully explained by their higher levels of LM. In fact, after controlling for LM, the association between bone mass and FM is inverse, indicating a proportional lower BMD and BMC for a same body LM unit in those overweight/obese adolescents.
References
Ferrari SL (2005) Osteoporosis: a complex disorder of aging with multiple genetic and environmental determinants. World Rev Nutr Diet 95:35–51
Rizzoli R, Bianchi ML, Garabedian M, McKay HA, Moreno LA (2010) Maximizing bone mineral mass gain during growth for the prevention of fractures in the adolescents and the elderly. Bone 46:294–305
Cummings SR, Black DM, Nevitt MC, Browner W, Cauley J, Ensrud K, Genant HK, Palermo L, Scott J, Vogt TM (1993) Bone density at various sites for prediction of hip fractures. The Study of Osteoporotic Fractures Research Group. Lancet 341:72–75
Marshall D, Johnell O, Wedel H (1996) Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 312:1254–1259
Branca F, Valtuena S (2001) Calcium, physical activity and bone health—building bones for a stronger future. Public Health Nutr 4:117–123
Vicente-Rodriguez G, Ezquerra J, Mesana MI, Fernandez-Alvira JM, Rey-Lopez JP, Casajus JA, Moreno LA (2008) Independent and combined effect of nutrition and exercise on bone mass development. J Bone Miner Metab 26:416–424
Vicente-Rodriguez G, Ara I, Perez-Gomez J, Dorado C, Calbet JA (2005) Muscular development and physical activity as major determinants of femoral bone mass acquisition during growth. Br J Sports Med 39:611–616
Courteix D, Lespessailles E, Loiseau-Peres S, Obert P, Ferry B, Benhamou CL (1998) Lean tissue mass is a better predictor of bone mineral content and density than body weight in prepubertal girls. Rev Rhum Engl Ed 65:328–336
Rauch F, Bailey DA, Baxter-Jones A, Mirwald R, Faulkner R (2004) The ‘muscle-bone unit’ during the pubertal growth spurt. Bone 34:771–775
Schoenau E, Frost HM (2002) The “muscle-bone unit” in children and adolescents. Calcif Tissue Int 70:405–407
Vicente-Rodriguez G, Ara I, Perez-Gomez J, Serrano-Sanchez JA, Dorado C, Calbet JA (2004) High femoral bone mineral density accretion in prepubertal soccer players. Med Sci Sports Exerc 36:1789–1795
Daly RM, Saxon L, Turner CH, Robling AG, Bass SL (2004) The relationship between muscle size and bone geometry during growth and in response to exercise. Bone 34:281–287
El Hage RP, Courteix D, Benhamou CL, Jacob C, Jaffre C (2009) Relative importance of lean and fat mass on bone mineral density in a group of adolescent girls and boys. Eur J Appl Physiol 105:759–764
Pietrobelli A, Faith MS, Wang J, Brambilla P, Chiumello G, Heymsfield SB (2002) Association of lean tissue and fat mass with bone mineral content in children and adolescents. Obes Res 10:56–60
Sayers A, Tobias JH (2010) Fat mass exerts a greater effect on cortical bone mass in girls than boys. J Clin Endocrinol Metab 95:699–706
Young D, Hopper JL, Macinnis RJ, Nowson CA, Hoang NH, Wark JD (2001) Changes in body composition as determinants of longitudinal changes in bone mineral measures in 8 to 26-year-old female twins. Osteoporos Int 12:506–515
El Hage R, Moussa E, El Hage Z, Theunynck D, Jacob C (2010) Influence of age and morphological characteristics on whole body, lumbar spine, femoral neck and 1/3 radius bone mineral apparent density in a group of Lebanese adolescent boys. J Bone Miner Metab. doi:10.1007/s00774-010-0246-4
Martinez-Gomez D, Ruiz JR, Ortega FB et al (2010) Recommended levels of physical activity to avoid an excess of body fat in European adolescents: the HELENA Study. Am J Prev Med 39:203–211
Reid IR (2002) Relationships among body mass, its components, and bone. Bone 31:547–555
Cobayashi F, Lopes LA, Taddei JA (2005) Bone mineral density in overweight and obese adolescents. J Pediatr (Rio J) 81:337–342
Ellis KJ, Shypailo RJ, Wong WW, Abrams SA (2003) Bone mineral mass in overweight and obese children: diminished or enhanced? Acta Diabetol 40(Suppl 1):S274–S277
Leonard MB, Shults J, Wilson BA, Tershakovec AM, Zemel BS (2004) Obesity during childhood and adolescence augments bone mass and bone dimensions. Am J Clin Nutr 80:514–523
Goulding A, Taylor RW, Jones IE, Manning PJ, Williams SM (2002) Spinal overload: a concern for obese children and adolescents? Osteoporos Int 13:835–840
Rocher E, Chappard C, Jaffre C, Benhamou CL, Courteix D (2008) Bone mineral density in prepubertal obese and control children: relation to body weight, lean mass, and fat mass. J Bone Miner Metab 26:73–78
Gracia-Marco L, Tomas C, Vicente-Rodriguez G, Jimenez-Pavon D, Rey-Lopez JP, Ortega FB, Lanza-Saiz R, Moreno LA (2010) Extra-curricular participation in sports and socio-demographic factors in Spanish adolescents: the AVENA study. J Sports Sci 28:1383–1389
Campion JM, Maricic MJ (2003) Osteoporosis in men. Am Fam Physician 67:1521–1526
Moreno LA, Gonzalez-Gross M, Kersting M et al (2008) Assessing, understanding and modifying nutritional status, eating habits and physical activity in European adolescents: the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr 11:288–299
Moreno LA, De Henauw S, Gonzalez-Gross M et al (2008) Design and implementation of the Healthy Lifestyle in Europe by Nutrition in Adolescence Cross-Sectional Study. Int J Obes (Lond) 32(Suppl 5):S4–S11
Beghin L, Castera M, Manios Y et al (2008) Quality assurance of ethical issues and regulatory aspects relating to good clinical practices in the HELENA Cross-Sectional Study. Int J Obes (Lond) 32(Suppl 5):S12–S18
Nagy E, Vicente-Rodriguez G, Manios Y et al (2008) Harmonization process and reliability assessment of anthropometric measurements in a multicenter study in adolescents. Int J Obes (Lond) 32(Suppl 5):S58–S65
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320:1240–1243
Cole TJ, Flegal KM, Nicholls D, Jackson AA (2007) Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ 335:194
Tanner JM, Whitehouse RH (1976) Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 51:170–179
Vicente-Rodriguez G, Jimenez-Ramirez J, Ara I, Serrano-Sanchez JA, Dorado C, Calbet JA (2003) Enhanced bone mass and physical fitness in prepubescent footballers. Bone 33:853–859
Gracia-Marco L, Vicente-Rodriguez G, Casajus JA, Molnar D, Castillo MJ, Moreno LA (2011) Effect of fitness and physical activity on bone mass in adolescents: the HELENA Study. Eur J Appl Physiol (in press)
McCrory MA, Gomez TD, Bernauer EM, Mole PA (1995) Evaluation of a new air displacement plethysmograph for measuring human body composition. Med Sci Sports Exerc 27:1686–1691
Moliner-Urdiales D, Ruiz JR, Ortega FB, Rey-Lopez JP, Vicente-Rodriguez G, Espana-Romero V, Munguia-Izquierdo D, Castillo MJ, Sjostrom M, Moreno LA (2009) Association of objectively assessed physical activity with total and central body fat in Spanish adolescents: the HELENA Study. Int J Obes (Lond) 33:1126–1135
Siri WE (1961) Body composition from fluid spaces and density: analysis of methods. In: Brozek J, Henschel A (eds) Techniques for measuring body composition. National Academy of Sciences, National Research Council, Washington, pp 223–234
Siri WE (1961) Body composition from fluid spaces and density: analysis of methods. Nutrition 9:480–491, discussion 480, 492
Vereecken CA, Covents M, Sichert-Hellert W et al (2008) Development and evaluation of a self-administered computerized 24-h dietary recall method for adolescents in Europe. Int J Obes (Lond) 32(Suppl 5):S26–S34
Farrán A, Zamora R, Cervera P (2004) Tablas de Composición de Alimentos del Centre d'Ensenyament Superior de Nutrició i Dietètica (CESNID). Barcelona
Weiler HA, Janzen L, Green K, Grabowski J, Seshia MM, Yuen KC (2000) Percent body fat and bone mass in healthy Canadian females 10 to 19 years of age. Bone 27:203–207
Janicka A, Wren TA, Sanchez MM, Dorey F, Kim PS, Mittelman SD, Gilsanz V (2007) Fat mass is not beneficial to bone in adolescents and young adults. J Clin Endocrinol Metab 92:143–147
Acknowledgments
The HELENA study takes place with the financial support of the European Community Sixth RTD Framework Programme (Contract FOOD-CT-2005-007034). The writing group takes sole responsibility for the content of this article. This study was also supported by a grant from the Spanish Ministry of Health: Maternal, Child Health and Development Network (number RD08/0072), grants from the Spanish Ministry of Science and Innovation (EX-2008-0641; JCI-2010-07055), and the Swedish Heart-Lung Foundation (20090635). Finally, this study was also supported (LGM, GVR, LAM) by a grant from Mutua de la Agrupación de Propietarios de Fincas Rústicas de España (Fundación MAPFRE), Spain. We gratefully acknowledge all participating adolescents and their parents for their collaboration.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
http://www.helenastudy.com/research.php
Research groups from Zaragoza and Granada were involved in the preparation of this paper.
Rights and permissions
About this article
Cite this article
Gracia-Marco, L., Ortega, F.B., Jiménez-Pavón, D. et al. Adiposity and bone health in Spanish adolescents. The HELENA study. Osteoporos Int 23, 937–947 (2012). https://doi.org/10.1007/s00198-011-1649-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-011-1649-3