
Abstract
Summary
We examined ethnic difference in the association of body fat and trunk fat with bone mineral density (BMD) among Chinese, white, and black subjects. We found that, with greater body and trunk fat, both white and black subjects were more likely to have a low BMD than Chinese subjects.
Introduction
Ethnic differences in body fat, abdominal fat distribution, and BMD have been found in previous studies between Chinese and white subjects. However, the associations of body fat and abdominal fat distribution with BMD have not been studied, and whether the ethnic differences have an effect on these associations is unclear.
Methods
We evaluated 1,147 subjects aged ≥18 years (805 Chinese, 193 whites, and 149 blacks). Percent body fat (%BF), percent trunk fat (%TF), and total and regional BMD including that of head, arm, leg, trunk, rib, spine, and pelvis were measured by dual-energy X-ray absorptiometry. Linear regression models were developed to test the association of ethnicity, %BF, and interaction between ethnicity and %BF with BMD. The models were repeated again, replacing %BF with %TF.
Results
Chinese subjects showed lower BMD in total and most regions compared with black and white subjects; however, these differences were eliminated between Chinese and whites within both sexes and between Chinese and black men when age, weight, height, and %BF were added. %BF and %TF were negatively associated with most regional body BMD. The interactions between %BF, %TF, and ethnicity were found in most regional body BMD among Chinese, white, and black subjects for both men and women.
Conclusion
Both %BF and %TF have negative associations with BMD. With greater accumulation of %BF and %TF, both white and black subjects may experience a higher risk of low BMD than Chinese subjects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis and fractures have become a major public health concern worldwide [1, 2]. Low bone mineral density (BMD) has been identified as an important risk factor for fracture and osteoporosis. Body fat (BF) was found to be strongly associated with BMD [3]. Some studies reported that BF was positively related to BMD [4–7], while others revealed an opposite relationship after body weight was considered [8, 9], and moreover, the effect of BF on low BMD was found to be independent of lean mass and physical activity [10, 11]. In addition, abdominal fat accumulation was considered to be independently associated with bone mineral content (BMC) in prepubertal children [12]. A recent epidemiologic study using waist circumference as the index of abdominal fat showed a negative association between abdominal fat accumulation and BMD [13]. Furthermore, a newly published study divided abdominal fat into visceral and subcutaneous adiposity and found a negative correlation between visceral adiposity and BMD [14]. However, the evidence of the association between BMD and abdominal fat distribution was still limited.
Compared with white and black subjects, Asians such as Chinese, Japanese, and Singaporeans were reported to be thinner but with higher percent body fat (%BF) levels and more abdominal fat [15–22]. Some studies reported that there was no significant difference in BMD between Chinese and white subjects when body size was taken into account [23–25]. In addition, the prevalence of osteoporosis and fractures in some body regions in Chinese people was even lower than that in whites [1, 26]. To our knowledge, no study has investigated the ethnic differences in the relationship of %BF and abdominal fat distribution with BMD.
The present study was designed to examine the relationship of %BF and percent trunk fat (%TF) with BMD. We are particularly interested to learn whether ethnic differences in %BF and %TF may influence BMD among Chinese, black, and white subjects.
Methods
Subjects
This study included 1,029 Chinese (403 men and 626 women), 207 white (89 men and 118 women), and 152 black (73 men and 79 women) subjects aged 18–87 years old. Chinese participants were voluntarily enrolled between November 2008 and May 2009 through leaflets and posters provided by the local department of the Center for Disease Control and Prevention in Hangzhou, China. The data on blacks and whites were obtained between August 1998 and January 2001 from St. Luke’s-Roosevelt Hospital Center, Columbia University in the city of New York, USA. Details of the measurements from the USA were previously published [16]. Subjects who had missing information on dual-energy X-ray absorptiometry (DXA) (n = 47) and menopausal status in women (n = 27) were excluded from the analysis. We also excluded subjects who had conditions known to affect bone mass (n = 167), such as diseases of the thyroid, diabetes mellitus, and previous bone fractures. A total of 468 men (323 Chinese, 75 white, and 70 black subjects) and 679 women (482 Chinese, 118 white, and 79 black subjects) were included in the analysis. The subjects who were excluded from the study were not significantly different from subjects who met the inclusion criteria in age, weight, and height, except that the Chinese men excluded from the study were older than the Chinese men who remained in the study. Each participant gave informed consent in writing. The study was approved by the internal review boards of the Second Affiliated Hospital of Zhejiang University School of Medicine and St. Luke's-Roosevelt Hospital Center in New York, USA.
Anthropometry
Weight and height were measured with subjects dressed in light clothes. Body weight was measured to the nearest 0.1 kg (Detecto, USA). Body height was measured with a hypsometer to the nearest 0.1 cm. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared.
DXA measures
Total and body regional BMD, i.e., head, arm, leg, trunk, rib, spine, and pelvis, were measured by DXA (software version 11.40.004; Lunar Prodigy, WI, USA). Regional fat mass and whole-body fat mass were also measured. %BF was calculated as (BF in kilogram/body weight in kilogram). %TF, which was considered to represent the abdominal fat distribution, was calculated as (trunk fat (TF) in kilogram/body weight in kilogram). DXA was standardized daily against a phantom, with the manufacturer’s precision standards of ≤0.8% for BMD and BF in Chinese and approximately 1.5% for BMD and 3~4% for BF in black and white subjects in the Obesity Research Center at Columbia University.
Statistical methods
Variables were presented as means ± standard deviations (SD) by sex and ethnicity. Comparisons of BMD, %BF, and %TF among the three ethnicities by sex were carried out using analysis of variance. The p values of the multiple comparisons between each pair of these three ethnicities were calculated using Fisher’s least significant difference (LSD) method [27].
Two sets of multiple linear regression models, a main model and an interaction model, were developed to test the associations of total and body regional BMD with ethnicity, %BF, and %TF. Due to high collinearity between %BF and %TF (variance inflation factor between %BF and %TF was approximately 13 in men and 9 in women), the effects of %BF and %TF on total and body regional BMD were examined separately in the regression models. In the main model, ethnicity, age, weight, height, %BF, and menopausal status in women were considered as independent variables, total and each body regional BMD were considered as the dependent variables. In the interaction model, the interaction between ethnicity and %BF was added into the main model. The main model and interaction model were repeated, replacing %BF with %TF. Sensitivity analysis was done using BMC subtracted from weight as the denominator to calculate %BF and %TF. The Chinese subjects were set as the reference group for ethnic comparisons in each model. Both main and interaction regression models were repeated which set white subjects as the reference group.
Statistical significance level was set at p < 0.05 (two-tailed). All analyses were performed using SPSS (version 16.0, SPSS Inc., Chicago, IL).
Results
Descriptive statistics
Table 1 shows the sex- and ethnicity-specific characteristics of the study subjects. In our sample, Chinese men were older than white and black men. In both sexes, the Chinese subjects had the lowest weight, height, and BMI compared with white and black subjects. In men, there was no difference in %BF among the three ethnicities, whereas Chinese men showed a significantly higher %TF than black men. In women, the Chinese subjects had a much lower %BF than black subjects and a significantly higher %TF than white subjects.
The means and SD of the total and each body regional BMD are also presented by ethnicity and sex in Table 1. For men, Chinese subjects showed lower BMD in total and all body regions except for head compared with black and white subjects. For women, Chinese subjects had the lowest BMD in total and all body regions among three ethnicities.
Multiply linear regression model
Main model
The β coefficients of each independent variable for BMD in total and all body regions from linear regression models are summarized in Table 2. After adjusting for age, weight, height, and %BF, Chinese men showed a higher level of head, arm, and trunk BMD than white men (p < 0.05) and a higher level of spine BMD than black men (p < 0.05). Chinese women showed a lower level of BMD in all regions, except for leg, than black women (p < 0.05). %BF was negatively associated with BMD in total and all body regions except head for men and head and spine for women.
The main model was repeated with %TF instead of %BF (Table 3). Chinese men showed a higher level of head, arm, and trunk BMD than did white men (p < 0.05) and a higher level of arm, leg, and spine BMD than did black men (p < 0.05). Chinese women showed a higher level of arm BMD than did white women and a lower level of BMD at all regions except for head and leg than black women (p < 0.05). In men, %TF was negatively associated with BMD in all body regions (p < 0.05) except for spine and pelvic. In women, %TF was negatively associated with total, arm, leg, and pelvic BMD (p < 0.05).
Interaction model
Interactions between ethnicity and %BF (Table 2), or ethnicity and %TF (Table 3), were included in the interaction models to test for ethnic differences in associations. In men, the interactions between ethnicity and %BF were significant in all regions except for head between Chinese and white subjects and in trunk, rib, spine, and pelvic BMD between Chinese and black subjects, while in women, the interactions were found to be significant in leg, trunk, rib, and spine BMD between Chinese and white subjects and in trunk and rib BMD between Chinese and black subjects.
The interactions between ethnicity and %TF are shown in Table 3. In men, the interaction terms were significant in all regional BMD except for head between Chinese and white subjects and in all regional BMD between Chinese and black subjects. In women, the interactions between ethnicity and %TF were significant in all regional BMD except for pelvic BMD between Chinese and white subjects and in arm, leg, trunk, rib, and spine BMD between Chinese and black subjects. Sensitivity analysis was done using BMC subtracted from weight as the denominator to calculate %BF and %TF; the results remained identical.
When white subjects were set as reference group, both main and interaction models were repeated. The result showed that the ethnic differences in the association of %BF and %TF with BMD between white and black subjects were not significant, whereas the differences between Chinese and white subjects remained significant (data not shown).
Discussion
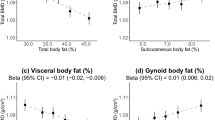
The present study indicates that both %BF and %TF were negatively associated with total and most body regional BMD. This adverse association was independent of age, ethnicity, height, and weight. Compared with white and black subjects, both Chinese men and women have a lower decrement of BMD with increasing %BF and %TF. In addition, the ethnic differences in the associations between %TF and BMD can be found in more body regions than that between %BF and BMD.
There are discrepancies in the results on the relationship between BF and BMD. Our study showed that %BF was negatively correlated with BMD at most body regions independent of body weight, which was consistent with some of the previous studies [8, 9]. The effect of %BF on BMD can be separated into biomechanical and biochemical ways. After mechanical loading, which can be a function of body weight, was controlled, the negative correlation between BMD and %BF implied that the excessive BF may not have a beneficial effect on BMD, and an adipocytes-derived bone active hormone, such as leptin and adiponectin [28], may have a detrimental effect on bone mass [5].
Abdominal fat distribution is a well-known risk for metabolic diseases, such as metabolic syndrome, diabetes, and cardiovascular diseases [29–31]. Recent studies showed a strong relationship between BMD and abdominal fat distribution; however, these results are inconsistent [13, 14, 32], and how abdominal fat influences bone metabolism is not clear. An effect of abdominal fat distribution on BMD may be caused by the secretions from the abdominal adipocyte and, additionally, obesity-related metabolic diseases also associated with BMD [32]. Our study found that %TF was negatively correlated with most body regional BMD, and %TF showed a stronger relationship with BMD than %BF. It may be considered that compared with %BF, the pattern of fat distribution may have a closer relationship with BMD.
To our knowledge, there was no study investigating the ethnic differences in the relationship of %BF and %TF with body regional BMD. The major strength of this study was that it found a significant difference between Chinese and other ethnicities in the relationship of %BF and %TF with BMD within both sexes. The ethnic differences in the associations between %TF and BMD were found in total and more regions than that between %BF and BMD. It may suggest that %TF plays a more important role in predicting ethnic differences in BMD than %BF. The ethnic difference in the relationship between %TF and BMD may be due to the reciprocal effect of visceral and subcutaneous fat masses on BMD [14]. With the same increment of BF, Chinese people were reported to have more subcutaneous fat accumulated compared with their European counterparts [21], and the positive correlation between subcutaneous fat and BMD was found to be slightly stronger than the negative correlation between visceral fat and BMD [14]. The opposite associations between subcutaneous fat and visceral fat with BMD are mainly due to the different expressions of biochemical factors. Leptin and aromatase were reported to be the protective factors on BMD which were secreted more in subcutaneous than in visceral adipose tissue [33, 34]. The factors secreted by visceral adipose tissue may easily cause insulin resistance, which is detrimental to BMD [35]. These may partially explain the lower decrement of BMD in Chinese subjects than in white and black subjects for the same increment of %TF.
The results of this study should be interpreted in light of several limitations. First, cross-validation of the DXA measurements was not performed at the Zhejiang University and the Columbia University. However, both of the two study centers used the same DXA scanners (Lunar Prodigy, WI, USA) and followed the same standardized measurement procedure, which may technically reduce the bias from scanner difference as far as possible. Second, due to the lack of data, we did not adjust for lifestyle factors, such as physical activity and dietary habits. These factors may play an important role in body regional BMD and should be taken into account in future studies. Third, the current DXA technique does not allow the separation of TF into visceral and subcutaneous compartments. Because the biochemical factors secreted by visceral and subcutaneous adipocytes may have different effects on BMD, further studies are encouraged to address the different metabolic effects of visceral and subcutaneous fat on BMD. Forth, the present study did not measure the femoral neck or lumbar spine BMD to define the diagnosis of osteoporosis. However, mean BMD can also be used to test the relationship between body composition and osteoporosis [36, 37].
Conclusion
Increased %BF and %TF appear to be related to decreased BMD even after controlling for age, ethnicity, height, and weight. With an increase in %BF and %TF, both white and black subjects were more likely to decrease their BMD than Chinese subjects within both sexes. In addition, the ethnic differences between %TF and BMD were observed in more body regions than that between %BF and BMD. This study enhanced our understanding of the relationship of %TF and %BF with total and body regional BMD and the effect of ethnic differences of this association.
References
Wang Y, Tao Y, Hyman ME, Li J, Chen Y (2009) Osteoporosis in China. Osteoporos Int 20:1651–1662
US Dept. of Health and Human Services (2004) Bone health and osteoporosis: a report of the Surgeon General Public Health Service, Office of the Surgeon General, Washington, D.C. http://www.surgeongeneral.gov/libarary/bonehealth/content.html. Accessed 10 November 2009
Zhao LJ, Jiang H, Papasian CJ et al (2008) Correlation of obesity and osteoporosis: effect of fat mass on the determination of osteoporosis. J Bone Miner Res 23:17–29
Gnudi S, Sitta E, Fiumi N (2007) Relationship between body composition and bone mineral density in women with and without osteoporosis: relative contribution of lean and fat mass. J Bone Miner Metab 25:326–332
Reid IR (2008) Relationships between fat and bone. Osteoporos Int 19:595–606
Heiss CJ, Sanborn CF, Nichols DL, Bonnick SL, Alford BB (1995) Associations of body fat distribution, circulating sex hormones, and bone density in postmenopausal women. J Clin Endocrinol Metab 80:1591–1596
Stewart KJ, Deregis JR, Turner KL et al (2002) Fitness, fatness and activity as predictors of bone mineral density in older persons. J Intern Med 252:381–388
Zhao LJ, Liu YJ, Liu PY, Hamilton J, Recker RR, Deng HW (2007) Relationship of obesity with osteoporosis. J Clin Endocrinol Metab 92:1640–1646
Janicka A, Wren TA, Sanchez MM et al (2007) Fat mass is not beneficial to bone in adolescents and young adults. J Clin Endocrinol Metab 92:143–147
Hsu YH, Venners SA, Terwedow HA et al (2006) Relation of body composition, fat mass, and serum lipids to osteoporotic fractures and bone mineral density in Chinese men and women. Am J Clin Nutr 83:146–154
Fu X, Ma X, Lu H, He W, Wang Z, Zhu S (2010) Associations of fat mass and fat distribution with bone mineral density in pre- and postmenopausal Chinese women. Osteoporos Int 22:113–119
Afghani A, Goran MI (2006) Racial differences in the association of subcutaneous and visceral fat on bone mineral content in prepubertal children. Calcif Tissue Int 79:383–388
Kim CJ, Oh KW, Rhee EJ et al (2009) Relationship between body composition and bone mineral density (BMD) in perimenopausal Korean women. Clin Endocrinol Oxf 71:18–26
Gilsanz V, Chalfant J, Mo AO, Lee DC, Dorey FJ, Mittelman SD (2009) Reciprocal relations of subcutaneous and visceral fat to bone structure and strength. J Clin Endocrinol Metab 94:3387–3393
Wang J, Thornton JC, Russell M, Burastero S, Heymsfield SB, Pierson RN Jr (1994) Asians have lower BMI but higher percent body fat than do whites: comparisons of anthropometric measurements. Am J Clin Nutr 60:23–28
Gallagher D, Heymsfield SB, Heo M, Jebb SA, Murgatroyd PR, Sakamoto Y (2000) Healthy percentage body fat ranges: an approach for developing guidelines based on body mass index. Am J Clin Nutr 72:694–701
Lear SA, Humphries KH, Kohli S, Birmingham CL (2007) The use of BMI and waist circumference as surrogates of body fat differs by ethnicity. Obesity 15:2817–2824
Wang J, Thornton JC, Burastero S et al (1996) Comparison for BMI and body fat percent among Puerto Ricans, Blacks, Whites and Asians living in the New York City area. Obes Res 4:377–384
Deurenberg P, Deurenberg YM, Guricci S (2002) Asians are different from Caucasians and from each other in their body mass index/body fat per cent relationship. Obes Rev 3:141–146
Wang LD (2005) The status of nutrition and Health in China. People’s Medical Publishing House, Beijing, pp 13–27
Lear SA, Humphries KH, Kohli S, Chochalingam A, Frohlich JJ, Birmingham CL (2007) Visceral adipose tissue accumulation differs according to ethnic background: results of Multicultural Community Health Assessment Trial (M-CHAT). Am J Clin Nutr 86:353–359
Park YW, Allison DB, Heymsfield SB, Gallagher D (2001) Larger amounts of visceral adipose tissue in Asian Americans. Obes Res 9:381–387
Ross PD, He Y, Yates AJ et al (1996) Body size accounts for most differences in bone density between Asian and Caucasian women. The EPIC (Early Postmenopausal Interventional Cohort) study group. Calcif Tissue Int 59:339–343
Russell-Aulet M, Wang J, Thornton JC, Colt EW, Pierson RN (1993) Bone mineral density and mass in a cross-sectional study of white and Asian women. J Bone Miner Res 8:575–582
Wu XP, Liao EY, Huang G, Dai RC, Zhang H (2003) A comparison study of the reference curves of bone mineral density at different skeletal sites in native Chinese, Japanese, and American Caucasian women. Calcif Tissue Int 73:122–132
Xu L, Lu A, Zhao X, Chen X, Cummings SR (1996) Very low rates of hip fracture in Beijing, People’s Republic of China, the Beijing osteoporosis project. Am J Epidemiol 144:901–907
Jason CH (1996) Multiple comparisons: theory and methods. Chapman & Hall, London
Kontogianni MD, Dafni UG, Routsias JG, Skopouli FN (2004) Blood leptin and adiponectin as possible mediators of the relation between fat mass and BMD in perimenopausal women. J Bone Miner Res 19:546–551
Larsson B, Svärdsudd K, Welin L, Wilhelmsen L, Björntorp P, Tibblin G (1984) Abdominal adipose tissue distribution, obesity, and risk of cardiovascular disease and death: 13 year follow up of participants in the study of men born in 1913. Br Med J Clin Res Ed 288:1401–1404
Rexrode KM, Carey VJ, Hennekens CH et al (1998) Abdominal adiposity and coronary heart disease in women. JAMA 280:1843–1848
Wei M, Gaskill SP, Haffner SM, Stern MP (1997) Waist circumference as the best predictor of noninsulin dependent diabetes mellitus (NIDDM) compared to body mass index, waist/hip ratio and other anthropometric measurements in Mexican Americans—a 7-year prospective study. Obes Res 5:16–23
Kinjo M, Setoguchi S, Solomon DH (2007) Bone mineral density in adults with the metabolic syndrome: analysis in a population-based U.S. sample. J Clin Endocrinol Metab 92:4161–4164
Gordeladze JO, Drevon CA, Syversen U, Reseland JE (2002) Leptin stimulates human osteoblastic cell proliferation, de novo collagen synthesis, and mineralization: impact on differentiation markers, apoptosis, and osteoclastic signaling. J Cell Biochem 85:825–836
Klein KO, Larmore KA, de Lancey E, Brown JM, Considine RV, Hassink SG (1998) Effect of obesity on estradiol level, and its relationship to leptin, bone maturation, and bone mineral density in children. J Clin Endocrinol Metab 83:3469–3475
Krakauer JC, McKenna MJ, Buderer NF, Rao DS, Whitehouse FW, Parfitt AM (1995) Bone loss and bone turnover in diabetes. Diabetes 44:775–782
Genaro PS, Pereira GA, Pinheiro MM, Szejnfeld VL, Martini LA (2010) Influence of body composition on bone mass in postmenopausal osteoporotic women. Arch Gerontol Geriatr 51:295–298
Shen W, Chen J, Punyanitya M, Shapses S, Heshka S, Heymsfield SB (2007) MRI-measured bone marrow adipose tissue is inversely related to DXA-measured bone mineral in Caucasian women. Osteoporos Int 18:641–647
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
H. Lu and X. Fu contributed equally to this study.
Rights and permissions
About this article
Cite this article
Lu, H., Fu, X., Ma, X. et al. Relationships of percent body fat and percent trunk fat with bone mineral density among Chinese, black, and white subjects. Osteoporos Int 22, 3029–3035 (2011). https://doi.org/10.1007/s00198-010-1522-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-010-1522-9