
Abstract
Summary
We determined the effect of antioxidants and resistance training on bone mineral density of postmenopausal women. After 6 months, we observed a significant decrease in the lumbar spine BMD of the placebo group while other groups remained stable. Antioxidants may offer protection against bone loss such as resistance training.
Introduction
The purpose of this pilot study was to determine the effects of antioxidant supplements combined to resistance training on bone mineral density (BMD) in healthy elderly women.
Methods
Thirty-four postmenopausal women (66.1 ± 3.3 years) were randomized in four groups (placebo, n = 7; antioxidants, n = 8; exercise and placebo, n = 11; and exercise and antioxidants, n = 8). The 6-month intervention consisted in antioxidant supplements (600 mg vitamin E and 1,000 mg vitamin C daily) or resistance exercise (3×/week). Femoral neck and lumbar spine BMD (DXA) and dietary intakes (3-day food record) were measured before and after the intervention. A repeated measure ANOVA and non-parametric Mann–Whitney U tests were used.
Results
We observed a significant decrease in the placebo group for lumbar spine BMD (pre, 1.01 ± 0.17 g/cm2; post, 1.00 ± 0.16 g/cm2; P < 0.05 respectively) while it remained stable in all other groups. No changes were observed for femoral neck BMD.
Conclusions
Antioxidant vitamins may offer some protection against bone loss in the same extent as resistance exercise although combining both does not seem to produce additional effects. Our results suggest to further investigate the impact of antioxidant supplements on the prevention of osteoporosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a major public health problem that is characterized by a loss of bone mass associated with aging [1]. This process contributes to functional impairment since it increases susceptibility to fractures, primarily of the hip, spine, and wrist [2]. Hip fractures are a major problem as they lead to complication-associated death in more than 20% of cases and about 50% of individuals who survive remain disable [3]. Women are particularly affected by osteoporosis owing to the important role that estrogens play on bone turnover as they stimulate bone formation and inhibit bone resorption [4].
Resistance training has been associated with osteoporosis and the maintenance of bone mass [5] and to positively impact on multiple risk factors for osteoporotic fractures in previously sedentary postmenopausal women [6]. In this sense, exercise favors bone formation and contributes to increase bone density [7, 8]. However, the positive effects of resistance training could be limited by exercise-induced oxidative stress observed in older individuals.
In fact, moderate to high-intensity exercise has been shown to increase reactive oxygen species (ROS) and nitric oxide derivatives (NO) production in contracting skeletal muscle [9, 10]. The extent of oxidative stress is dependent on several factors, including age, oxygen consumption, antioxidant levels, and the presence of adequate repair systems [11]. Although regular exercise training is effective to enhance adaptive responses thereby diminishing oxidative stress in younger individuals [12–14], it appears that aging may partly attenuate these adaptations [15, 16]. It thus has been proposed that elders who exercise have greater requirements for dietary antioxidant [17] such as vitamins C and E [18].
Antioxidants have also been associated with bone health. When compared to matched controls, elderly osteoporotic women presented lower levels of dietary and endogenous antioxidants [19]. In accordance, epidemiological studies have shown low vitamin C intakes to be associated with a low bone mineral density (BMD) [20, 21] and an increased bone loss in postmenopausal women [22]. Moreover, low intakes of vitamin C and E have been related to an increased risk of hip fractures in smokers [23].
Up until now, no studies have examined changes in BMD in response to high intensity resistance exercise combined with vitamins C and E, specifically in postmenopausal women. Actually, it remains unclear whether exogenous antioxidants supplements are beneficial for BMD gains in exercising older individuals. Therefore, the purpose of this pilot study was to investigate if 6 months of resistance training combined with antioxidant treatment could counteract the loss of bone mass as compared to exercise alone.
Materials and methods
Subjects
Thirty-four healthy women aged between 61 and 73 years were recruited from local newspaper advertisements in Sherbrooke, Quebec (Canada) to participate in a large trial which objective was to evaluate the efficiency of a combination of antioxidant supplements and resistance training on sarcopenia and insulin sensitivity in elderly men and women. Subjects had to meet the following criteria: (1) healthy, caucasian, and without major physical incapacity; (2) taking no medication that could influence metabolism; (3) non-smoker and moderate drinker (15 g of alcohol/day maximum, the equivalent of one alcoholic beverage/day); (4) body mass index (BMI) between 18 and 30 kg/m2; (5) no consumption of antioxidant supplements (i.e. vitamins C, E) during the last month; and (6) postmenopausal and not taking hormone replacement therapy. A phone interview was conducted to screen for the aforementioned inclusion criteria. In the present study, data from 34 women were used for analysis purposes. After the nature and goals of the study were thoroughly explained, subjects provided written informed consent. This study was approved by the Ethics Committee of the Sherbrooke Geriatric University Institute.
Overview of experimental protocol
After screening by telephone, volunteers were invited for a visit at the Research Centre on Aging (Sherbrooke Geriatric University Institute). Upon arrival, body weight, height, and body composition (DXA) were assessed and instructions were provided for the 3-day dietary record. Following the visit, subjects were randomized in one of four groups (placebo, n = 7; antioxidants, n = 8; exercise and placebo, n = 11; and exercise and antioxidants, n = 8) and exercise groups were enrolled in the 6-month resistance training program. Subjects were instructed to maintain usual food and physical activity habits. After 6 months of intervention, subjects were submitted to a post-test session identical to the one conducted at baseline.
Resistance training program
The 6-month resistance training program consisted in supervised 60-min exercise sessions performed three times per week on alternating days. Each session consisted of two components: 15 min of warming-up, treadmill or cycle ergometer followed by static stretching; and 45 min of resistance training comprising exercises targeting large and small muscle groups including abdominals: leg press, bench press, leg extension, shoulder press, sit up, seated row, triceps extension, and biceps curl. Subjects performed three sets (eight repetitions per set) at 80% of a one repetition maximum (1 RM) for each exercise. Resting periods of 90–120 s separated each set. The 1 RM was assessed every 4 weeks in order to adjust exercise intensity for strength gains throughout the training program. A maximum of one missed exercise session per month was accepted for compliance purposes.
Antioxidant and placebo supplements
Participants were randomly assigned to receive either the antioxidant supplement (600 mg/day of vitamin E (dl-α-tocopherol) and 1,000 mg/day of vitamin C (ascorbic acid) or the placebo (lactose). Antioxidants and placebos were supplied for 50-day periods and new capsules were given at the end of each period to ensure compliance of subjects. Vitamin E and placebos were supplied by Arkopharma (Arkopharma, Carros, France) while vitamin C and placebos were purchased at the Sherbrooke Geriatric Institute hospital pharmacy (Wampole Brands, Toronto, ON, Canada).
Body composition and anthropometric measurements
Body weight was determined using an electronic scale (SECA, Hamburg, Germany). Height was measured using a tape measure fixed to the wall with the subject in stocking feet. Body mass index was calculated as weight (kg) relative to height (m2). Determination of fat mass (FM) and fat-free mass (FFM) was assessed in a supine position, using the dual-energy X-ray absorptiometry method (GE Prodigy Lunar, Madison, WI, USA). In our laboratory, the coefficients of variations for repeated determinations of BMD, FM, and FFM in ten adults (measured 1 week apart) were 0.9%; 5.7%, and 1.1% respectively.
Dietary intake
Each subject was instructed to maintain normal dietary habits throughout the period of data collection as previously mentioned[24]. Subjects were provided with a 5 kg (11 lb) food scale and instructed on how to complete a 3-day dietary record. Diets were recorded on 2 weekdays and 1 weekend-day. It has been demonstrated that a 3-day dietary record is valid to estimate dietary intakes in older adults without cognitive impairments [24]. Dietary analyses were completed by using Candat system, version 6.0 software (Candat, London, ON, Canada) to determine daily energy, macronutrients, and micronutrients intakes.
Statistical methods
Values are displayed as means ± standard deviation (±SD). A one-way ANOVA was performed to assess differences between groups at baseline. A repeated measure ANOVA was used to examine differences between pre-test and post-test BMD. Because of the small sample size, changes between pre- and post-intervention values were also examined with the use of non-parametric Mann–Whitney U tests. We also compared the delta BMD (post-intervention BMD − pre-intervention BMD) between groups with the use of a one-way ANOVA. In all cases, a P value below 0.05 was considered significant. All analyses were performed with the SPSS software version 11.0.
Results
Mean age was 66.1 ± 3.3 years. As shown in Table 1, at baseline, groups were similar for body composition and dietary intake variables, and no strength difference was found between both exercise groups for all 1 RM (results not shown). Body weight and BMI decreased significantly in placebo group but remained stable in other groups. Caloric intake in exercise and placebo group decreased significantly while it remained relatively stable in other groups. No significant difference was observed in baselines values for calcium and vitamin E intakes (excluding intervention). The daily consumption of vitamin D increased significantly in exercise and antioxidants group but remained similar in other groups. Finally, while daily intakes of vitamin C decreased significantly in antioxidants group, it remained stable for other groups.
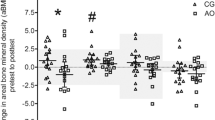
As shown in Table 2, we examined femoral neck and lumbar spine following 6 months of intervention. While the placebo group displayed a significant loss in lumbar spine BMD (P < 0.05), all other groups remained stable (Fig. 1). Accordingly, delta lumbar spine BMD was significantly greater in the placebo group than the three other groups (P < 0.05), indicating that lumbar spine BMD was maintained in all groups except for the placebo group. These results were confirmed with non-parametric analyses. However, no significant difference was observed between groups for changes in femoral neck BMD.

BMD variation pre- and post-intervention between each experimental group
Conclusions
The aim of this pilot study was to investigate if the combination of resistance training and antioxidant supplements could impact on bone mass loss in postmenopausal women. We observed a bone loss in the placebo group corresponding to the typical average loss for postmenopausal women [25, 26]. Hence, it seems that antioxidants exerted a beneficial effect on BMD in postmenopausal women, to the same extent as resistance training. However, no interaction effect was observed when combining resistance training and antioxidant supplements. Groups were similar for calcium, vitamin D, vitamin E, and vitamin C intakes. Differences between groups in BMD could thus not be attributed to differences in dietary intakes.
The findings of this study support that, in postmenopausal women, high resistance training is effective to stop or limit the loss of lumbar spine BMD but possibly not femoral neck BMD. It may be in part attributable to the metabolic properties of these two different skeletal regions of interest. In fact, the lumbar spine comprises a greater proportion of cancellous (or trabecular) bone as compared to femoral neck [27].On the other hand, femoral neck comprises a greater proportion in cortical (or compact) bone [27]. Bone turnover is greater in cancellous bone than in cortical bone [27] which may explain why resistance exercise exerts a greater effect in this region. In support of that, a previous animal study showed that resistance exercise resulted in a significant increase in cancellous bone markers but not in cortical bone [28].
Antioxidant supplements
Our results suggest that vitamins C and E may favorably impact on lumbar spine BMD. A previous study suggested that the use of vitamins C and E supplements is associated with decreased levels of serum CTx, a marker of bone resorption [29], bone loss occurring when resorption exceeds formation. In accordance, in vitro cell models demonstrate that ROS stimulate osteoclast differentiation [30, 31] and inhibit osteoblast differentiation [32]. Conversely, antioxidants may reduce the damaging effects of oxidative stress on bone mass by reducing the upregulated osteoclastic differentiation and enhancing the downregulated osteoblastic differentiation. Our results suggest to further study the role of antioxidants in the regulation of both osteoclastic bone resorption and formation.
Limitations
Our study had some limits that need to be mentioned. First, the small sample size may have reduced the statistical power. Nevertheless, we used non-parametric statistical tests to confirm the results. Secondly, our pilot study was of short duration but strongly supports to use a longer intervention period to (1) assure long-term effect and (2) examine if, on the long run, the combination of resistance exercise and antioxidants is beneficial as compared to exercise or antioxidants alone.
Recommendations
It is not appropriate to elaborate formal nutritional recommendations based on this pilot study, it provides some insights as to the nutritional parameters that may be beneficial for bone health. Further research is needed to determine appropriate recommendations for this population especially since nutrition and exercise are two effective and accessible strategies towards health maintenance in the aging population.
Our results demonstrated that 6 months of antioxidant supplementations may have the same positive effect on lumbar spine BMD than 6 months of resistance training although antioxidant supplementations combined with resistance training did not provide any additional effect. These results are interesting because this is the first study to examine the combination of these interventions in healthy elderly women suggesting another effective strategy to delay age-related BMD loss. Further investigations are necessary to confirm our findings.
References
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Garnero P, Sornay-Rendu E, Claustrat B, Delmas PD (2000) Biochemical markers of bone turnover, endogenous hormones and the risk of fractures in postmenopausal women: the OFELY Study. J Bone Miner Res 15(8):1526–1536
Thwaites J, Mann F, Gilchrist N, McKie J, Sainsbury R (2007) Older patients with hip fractures: evaluation of a long-term specialist orthopaedic medicine service in their outcomes [see comment]. N Z Med J 120:U2535
Weitzmann MN, Pacifici R (2006) Estrogen deficiency and bone loss: an inflammatory tale. J Clin Invest 116:1186–1194
Layne JE, Nelson ME (1999) The effects of progressive resistance training on bone density: a review. Med Sci Sports Exer 31:25–30
Nelson ME, Fiatarone MA, Morganti CM, Trice I, Greenberg RA, Evans WJ (1994) Effects of high-intensity strength training on multiple risk factors for osteoporotic fractures. A randomized controlled trial. JAMA 272:1909–1914
Maddalozzo GF, Snow CM (2000) High intensity resistance training: effects on bone in older men and women. Calcif Tissue Int 66:399–404
Zehnacker CH, Bemis-Dougherty A (2007) Effect of weighted exercises on bone mineral density in post menopausal women. A systematic review. J Geriatr Phys Ther 30:79–88
Reid MB (2001) Nitric oxide, reactive oxygen species, and skeletal muscle contraction. Med Sci Sports Exer 33:371–376
Jackson MJ (2005) Reactive oxygen species and redox-regulation of skeletal muscle adaptations to exercise. Philos Trans R Soc Lond B Biol Sci 360:2285–2291
Vollaard NB, Shearman JP, Cooper CE (2005) Exercise-induced oxidative stress: myths, realities and physiological relevance. Sports Med 35:1045–1062
Parise G, Brose AN, Tarnopolsky MA (2005) Resistance exercise training decreases oxidative damage to DNA and increases cytochrome oxidase activity in older adults. Exp Gerontol 40:173–180
Powers SK, Ji LL, Leeuwenburgh C (1999) Exercise training-induced alterations in skeletal muscle antioxidant capacity: a brief review. Med Sci Sports Exerc 31:987–997
McArdle A, Jackson MJ (2000) Exercise, oxidative stress and ageing. J Anat 197(Pt 4):539–541
Rousseau AS, Margaritis I, Arnaud J, Faure H, Roussel AM (2006) Physical activity alters antioxidant status in exercising elderly subjects. J Nutr Biochem 17:463–470
Fielding RA, Meydani M (1997) Exercise, free radical generation, and aging. Aging Clin Exp Res 9:12–18
Manfredi TG, Fielding RA, O’Reilly KP, Meredith CN, Lee HY, Evans WJ (1991) Plasma creatine kinase activity and exercise-induced muscle damage in older men. Med Sci Sports Exer 23:1028–1034
Flora SJ (2007) Role of free radicals and antioxidants in health and disease. Cell Mol Biol 53:1–2
Maggio D, Barabani M, Pierandrei M, Polidori MC, Catani M, Mecocci P, Senin U, Pacifici R, Cherubini A (2003) Marked decrease in plasma antioxidants in aged osteoporotic women: results of a cross-sectional study. J Clin Endocrinol Metab 88:1523–1527
Hall SL, Greendale GA (1998) The relation of dietary vitamin C intake to bone mineral density: results from the PEPI study. Calcif Tissue Int 63:183–189
Wang MC, Luz Villa M, Marcus R, Kelsey JL (1997) Associations of vitamin C, calcium and protein with bone mass in postmenopausal Mexican American women. Osteoporos Int 7:533–538
Kaptoge S, Welch A, McTaggart A, Mulligan A, Dalzell N, Day NE, Bingham S, Khaw KT, Reeve J (2003) Effects of dietary nutrients and food groups on bone loss from the proximal femur in men and women in the 7th and 8th decades of age. Osteoporos Int 14:418–428
Melhus H, Michaelsson K, Holmberg L, Wolk A, Ljunghall S (1999) Smoking, antioxidant vitamins, and the risk of hip fracture. J Bone Min Res 14:129–135
Luhrmann PM, Herbert BM, Gaster C, Neuhauser-Berthold M (1999) Validation of a self-administered 3-day estimated dietary record for use in the elderly. Eur J Nutr 38:235
Okano H, Mizunuma H, Soda M, Kagami I, Miyamoto S, Ohsawa M, Ibuki Y, Shiraki M, Suzuki T, Shibata H (1998) The long-term effect of menopause on postmenopausal bone loss in Japanese women: results from a prospective study. J Bone Miner Res 13:303–309
Shipman AJ, Guy GW, Smith I, Ostlere S, Greer W, Smith R (1999) Vertebral bone mineral density, content and area in 8789 normal women aged 33–73 years who have never had hormone replacement therapy. Osteoporos Int 9:420–426
Eastell R, Mosekilde L, Hodgson SF, Riggs BL (1990) Proportion of human vertebral body bone that is cancellous. J Bone Min Res 5:1237–1241
Westerlind KC, Fluckey JD, Gordon SE, Kraemer WJ, Farrell PA, Turner RT (1998) Effect of resistance exercise training on cortical and cancellous bone in mature male rats. J Appl Physiol 84:459–464
Pasco JA, Henry MJ, Wilkinson LK, Nicholson GC, Schneider HG, Kotowicz MA (2006) Antioxidant vitamin supplements and markers of bone turnover in a community sample of nonsmoking women. J Women’s Health 15:295–300
Suda N, Morita I, Kuroda T, Murota S-I (1993) Participation of oxidative stress in the process of osteoclast differentiation. Biochim Biophys Acta (BBA) General Subjects 1157:318–323
Aitken CJ, Hodge JM, Nishinaka Y, Vaughan T, Yodoi J, Day CJ, Morrison NA, Nicholson GC (2004) Regulation of human osteoclast differentiation by thioredoxin binding protein-2 and redox-sensitive signaling. J Bone Miner Res 19:2057–2064
Mody N, Parhami F, Sarafian TA, Demer LL (2001) Oxidative stress modulates osteoblastic differentiation of vascular and bone cells. Free Radic Biol Med 31:509–519
Acknowledgments
We would like to express our thanks to the nurse Martine Fisch for her contribution to data collection and all study participants. We also gratefully acknowledge Arkopharma for providing vitamin supplements, the Canadian Institute of Health Research and Fonds de la recherche en santé du Québec.
Funding
This work was supported by the Canadian Diabetes Association. IJD holds a salary grant from the Canadian Institute of Health Research and AK from the Fonds de la recherche en santé du Québec.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chuin, A., Labonté, M., Tessier, D. et al. Effect of antioxidants combined to resistance training on BMD in elderly women: a pilot study. Osteoporos Int 20, 1253–1258 (2009). https://doi.org/10.1007/s00198-008-0798-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0798-5