
Abstract
Summary
Large regional differences in hip fracture rates within Norway have previously been shown. However, regional differences in hip bone mineral density (BMD) have not yet been assessed. In this study including 10,504 hip scans, there were significant regional differences in BMD. Further studies to address reasons for the regional differences in hip fracture risk are warranted.
Introduction
Bone mineral density (BMD) at the hip is an important determinant of hip fracture. While regional differences in Norwegian hip fracture rates have previously been shown, no comparative studies of hip BMD have been conducted.
Methods
Total hip BMD was measured by DXA in two population-based studies across Norway during 1997–2002. Valid hip scans with in vivo calibration were obtained from 5127 subjects in Tromsø (age 30–89 years) and 5377 subjects in Bergen (age 47–50 and 71–75 years).
Results
Women ≥60 years in Tromsø had 0.052 g/cm2 higher age-adjusted BMD than women in Bergen, whereas BMD among women <60 years was similar in Tromsø and Bergen. Age-adjusted total hip BMD was 0.035 g/cm2 lower in men ≥60 years in Bergen compared with Tromsø, and the corresponding figure for men <60 years was 0.028 g/cm2. While adjustment for body mass index explained some, but not all of the differences, smoking, physical activity, diabetes prevalence, self-perceived health, intake of alcohol and estrogen use did not.
Conclusions
Regional differences in BMD at the hip were found in Norway. Reasons for this and potential impact on hip fracture rates should be explored in further studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Norway and the other Scandinavian countries have the highest hip fracture rates ever reported [1, 2]. Large regional differences in hip fracture rates have previously been shown within Norway [1–6]. For example, the age-adjusted fracture rates per 10,000 for the age group >50 years were in 1996–1997 118 for women and 44 for men in the city of Oslo in southern Norway [2], and 82 for women and 38 for men in central Norway in 1997–1998 [3]. The regional differences reflected to a large degree differences between urban and rural areas; rural areas generally have lower hip fractures rates than urban [1–6]. Studies from other western countries have also shown lower hip fracture rates in rural than urban districts [7–11]. Urban-rural differences have recently also been shown for forearm fractures [12–14].
Low bone mineral density (BMD) is widely recognized as a major risk factor for fractures [15]. It has been shown that risk of fracture is best predicted by BMD at the same anatomical site [16, 17].
From a public health point of view, a central question is whether risk factors for fractures vary between different regions of the country, and whether differences in these factors may explain varying fracture rates. BMD is very interesting in this context, as hip BMD has been shown to predict hip fracture with a gradient risk comparable to that of blood pressure measurements in predicting cerebral stroke [16]. We have previously shown that in Norway, rural dwellers had higher forearm BMD compared with urban dwellers [18]. However, whether there are regional differences also in hip BMD, the strongest predictor of hip fractures, has not yet been studied.
BMD from different dual energy X-ray absorptiometry (DXA) manufacturers may differ up to 18%, whereas measures on devices from the same brand typically differ up to 5% [19]. There are only a few population-based studies comparing BMD between different study sites [18, 20]. Considering the small variation in population BMD, uncalibrated results from different DXA devices can easily result in wrong conclusions when comparing BMD in different populations. The International Society for Clinical Densitometry recommends cross-calibration before BMD from different models or makes are quantitatively compared [21].
The aim of this study was to compare in vivo calibrated hip BMD in two Norwegian cities (Tromsø and Bergen). Tromsø and Bergen are situated at ∼70° north and ∼60° north, respectively. The latitude may play a role in relation to different sun exposure and cutaneous vitamin D production [22]. We also wanted to assess whether potential regional differences could be attributed to differences in lifestyle factors such as cigarette smoking, body mass index (BMI) or level of physical activity, diabetes prevalence, self-perceived health, intake of alcohol or use of hormonal replacement therapy.
Methods
The Norwegian Epidemiological Osteoporosis Studies (NOREPOS) is a collaboration between four large population-based studies in Norway. These are sub-studies of large population-based multipurpose studies in Oslo, Bergen, Tromsø and Nord-Trøndelag.
The selection of the study population included here are described in Table 1 [23, 24]. Data were collected as part of the Tromsø V study and the Hordaland Health Study.
Tromsø is situated in northern Norway (∼70° north) and has approximately 65,000 inhabitants. The county consists of a large geographic area, 2558 km2. The majority of the participants in Tromsø live in the city center, whereas ∼20% of the population lives in rural districts. Bergen is situated at ∼60° north and has 245,000 inhabitants. Bergen and the three neighboring suburban municipalities included in this study consist of a geographic area of 813 km2 [25].
Study population in Tromsø
Data were collected in the fifth Tromsø survey (Tromsø V) conducted during 2001–2002. The source population for the bone mineral density sub-study included all individuals aged 30–90 years in the municipality of Tromsø, and a sample of 6969 subjects were invited [23]. Dual hip scans were performed. Ineligible scans were excluded, leaving 9732 valid right and left hip scans. After including right hip scans if valid left scans were missing, we were left with 5127 hip scans.
Participants were divided into two groups; urban and rural Tromsø as previously described [18]. The majority of participants resided in the city center, and 18.6% in areas defined as rural.
Study population in Bergen
Data were collected in the Hordaland Health Study (HUSK) conducted during 1997–2000 [24]. The source population for the bone mineral density sub-study included all individuals born 1925–1927 and 1950–1951 residing in Bergen and three neighboring suburban municipalities. These age groups were determined by the main health study. The left hip was scanned unless there was a history of previous fracture or surgery. If the left hip could not be scanned, the right hip was used. Ineligible scans were excluded, and a total of 5377 valid scans were obtained.
BMD measurements
Two different GE Lunar scanners were used to measure BMD: Prodigy in Tromsø and EXPERT-XL in Bergen (GE Lunar, Madison, Wisconsin). We have previously shown that the precision is better for total hip compared with femoral neck measurements [26], and for this reason we chose to include total hip measurements.
Daily calibration was performed on the machines using a phantom supplied by the manufacturer. The scans were performed after the same protocol by different personnel at the two study sites. All scans were reviewed and reanalysed if necessary. Technically incorrect scans (e.g., scans that did not include the region of interest or movement artefacts), scans with metal in the region of interest and scans of hips with severe deformities were excluded from the analysis.
Generally, scans of the left hip were used for analyses. However, if the left hip measurement was missing, the right hip scan was used if valid. Right hip scans were used in 4.6% and 3.9% in Tromsø and Bergen, respectively. Excluding the right hip scans in an additional analysis did not change the results (data not shown).
We did not exclude participants with non-Caucasian background, as we did not have comparable information about ethnicity at both study sites. The number of nonethnic Norwegians in Bergen was small (0.7%), whereas equivalent numbers from Tromsø were not available.
Calibration of BMD data
In order to make the BMD data from the two study sites comparable, we have performed a cross-calibration study with 16 subjects who had three repeated measurements on the devices in both places [26].
When performing the calibration study, the Expert device in Bergen had been replaced by a Prodigy, whereas the Prodigy used in Tromsø was the same as used in this study. The Prodigy in Tromsø was, therefore, chosen as the reference device, whereas the data from Bergen were adjusted to make them comparable with the Tromsø data.
The data in Bergen were first translated into the “Prodigy scale” in Bergen. The Expert–Prodigy comparison was based upon hip scans of 27 individuals measured on both devices within 3 months. After evaluating a Bland & Altman plot for the Expert–Prodigy comparison, the following equation was calculated to calibrate the data: \(BMD_{{\text{Pr}}\,odigy} = 0.986\left\lfloor {BMD_{Expert} } \right\rfloor + 0.007\). As the difference between the Prodigy devices in Bergen and Tromsø was considered clinically insignificant, no further adjustments were made [26]. The coefficient of variation (CV) for total hip measurements on the Expert in Bergen was 1.20%, whereas the corresponding CV for the Prodigy in Bergen was 0.82%. The CV for total hip measurements on the Prodigy in Tromsø was 1.14%.
Other measures
Both studies were part of the CONOR (COhort of NORway) collaborative study [27]. The CONOR protocol includes a common set of questions and standard anthropometric measurements. Weight and height were measured in light indoor clothing without shoes. BMI was calculated as weight (in kg) divided by squared height (in m). Standard information about physical activity levels, smoking, use of hormone replacement therapy, self-perceived health, alcohol intake and diabetes were collected through self-administered questionnaires. Physical activity was assessed by two questions (hours per week of light and hard physical activity with four alternatives (0 to 3≥ hours) for each question). Information on smoking was dichotomized (current cigarette smokers or not). Self-perceived health in the questionnaire had four categories: poor/fair/good or excellent. Alcohol intake frequency was collected as times of alcohol intake per month. Diabetes status was collected as a yes/no question. Use of hormonal replacement therapy was classified as current, previous or non-users. Women not answering the questions regarding hormonal replacement therapy (n = 1190) were treated as non-users.
Statistics
Linear regression analyses were used to compare BMD, BMI and body height between study sites and age was included as an independent variable in all multivariate analyses. As the association between age and BMD was different for subjects <60 years and subjects ≥60 years, separate analyses for the two age groups were performed. The main regression analyses were restricted to subjects with valid total hip BMD and BMI measurements and who, in addition, had answered the question on smoking. Due to low response rate regarding physical activity, additional analysis for physical activity were performed where all subjects had valid information on BMI, smoking and physical activity (both low and high activity). We also performed additional analysis to evaluate whether alcohol, diabetes and self-perceived health could explain the differences in BMD between the cities.
Analyses of variances with adjustments for age were used to compare prevalences of known risk factors for low BMD between the cities.
Based on the linear regression results, we calculated new 95% confidence intervals for the differences in BMD between the cities where the variances from the calibration steps were included. These variances were based on the individual prediction error, and averaged over the cities. Separate variances were calculated for subjects <60 years and ≥60 years. The differences in BMD between the cities remained significant also after correction for the calibration (Appendix), and we therefore did not include variances from the calibration steps in the rest of the analyses.
We calculated a T-score for each participant (measured BMD minus young adult BMD divided by the standard deviation of the young adult BMD). The sex specific young adult (20–39 years) reference material from Lunar was used as reference material. If using the NHANES III reference group for women [28], the proportion of women classified as osteoporotic was almost unchanged. Separate analyses were performed for men and women. Logistic regression was used to calculate the odds ratio of having osteoporosis (T-score ≤-2.5) and osteopenia (-2.5 < T-score ≤ -1.0). Separate analyses were performed for individuals <60 years and subjects ≥60 years old.
Ethics
Written informed consent was collected from all participants. The individual studies were evaluated by the appropriate regional committee for medical research ethics and approved by the Norwegian Data Inspectorate.
Results
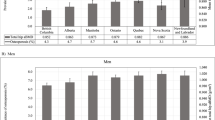
Table 2 and Fig. 1 show total hip BMD for different age groups. Table 3 shows that age-adjusted BMD in Tromsø and Bergen was similar for women under the age of 60, whereas mean age-adjusted BMD was 0.052 g/cm2 higher for elderly women (≥60 years) residing in Tromsø than in Bergen. The latter difference corresponds to approximately one-third standard deviation. In men, the age-adjusted total hip BMD was significantly higher in Tromsø compared with Bergen in the age groups studied.

Total hip bone mineral density (g/cm2) (A,B) and prevalence of BMD ≤-2.5 SD (osteoporosis) (C,D) in women and men by age. The NOREPOS study
For women, age-adjusted mean BMI was 1.2 kg/m2 (95% CI 1.0–1.4) higher in Tromsø than in Bergen. Similarly, age-adjusted BMI in men in Tromsø was 0.8 kg/m2 (95% CI 0.6–1.0) higher than in Bergen. After adjustments for age and BMI, women in Bergen <60 years had a significantly higher BMD than women in Tromsø <60 years, whereas the difference in BMD between men <60 years in Bergen and Tromsø was halved (Table 3). Similar adjustments in women ≥60 years resulted in a reduced BMD difference between Tromsø and Bergen, indicating that the differences in BMI can explain some, but not all, of the BMD differences between Tromsø and Bergen for the younger men and elderly women. Conversely, there were only minor changes in the corresponding BMD difference for elderly men when adjusting for BMI.
After adjusting for age, we found that the body height in Tromsø was 1.0 cm (95% CI 0.7–1.3) and 1.6 cm (95% CI 1.2–2.0) lower in women and men, respectively, compared with Bergen. Adjusting for body height in addition to age resulted in a larger BMD difference between men <60 years in Bergen and Tromsø, whereas the other estimates for the differences between the cities remained almost unchanged (Table 3).
The age-adjusted prevalence estimate of smoking in Tromsø was higher in both women (p = 0.015) and men (p = 0.001) compared with that in Bergen. Adjustments for current smoking status did not change the estimates of BMD difference between the cities neither in women nor in men. Likewise, differences in hormone replacement use could not explain the differences between Tromsø and Bergen in the younger (<60 years) or elderly (≥60 years) women. Adjustment for physical activity among participants with complete data (79.3% of all subjects) led to negligible changes in the total hip BMD differences between the cities (data not shown).
The age-adjusted prevalence of self-reported diabetes was not different between the cities. A higher age-adjusted proportion of women (p < 0.001) and men (p < 0.001) in Tromsø reported poor/fair self-perceived health compared with Bergen, but adjustments for self-perceived health did not change the differences in BMD between Bergen and Tromsø neither in women nor in men (data not shown). After adjustments for age, women in Tromsø reported to drink alcohol more often than women in Bergen (p < 0.001), whereas this was not true for men (p = 0.218). However, adjusting for alcohol frequency did not affect the differences in BMD between the cities.
Participants in Tromsø were divided into two groups; those residing in rural versus urban areas. No differences in mean BMD between the two areas were found, except in elderly women where the age-adjusted total hip BMD was 0.020 g/cm2 higher in women living in the rural compared with the urban part of Tromsø (p = 0.006). Excluding subjects in Tromsø living in rural areas did not change the differences between the cities.
The prevalences of osteoporosis are shown in Fig. 1. The odds ratio of osteoporosis and osteopenia was higher in Bergen compared with Tromsø in both women and men ≥60 years (Table 4). The odds ratio of osteoporosis and osteopenia in women <60 years in Tromsø and Bergen was not significantly different. Men in Bergen <60 years had a doubled odds ratio of osteopenia compared with those in Tromsø, whereas the corresponding odds ratio of osteoporosis was not significantly different.
Discussion
In the present study we have shown a higher total hip BMD among men and elderly women (≥60 years) living in Tromsø compared to men living in Bergen, while no differences were seen for women under 60 years. A higher body mass index in Tromsø compared with that in Bergen could explain some but not all of the differences in younger men and elderly women. The BMD differences were not attributable to different levels of physical activity, cigarette smoking, diabetes prevalence, self-perceived health, intake of alcohol or use of hormone replacement therapy among women.
This large comparative study, involving 10,504 hip scans, is the first to demonstrate regional differences in hip BMD within Norway. The available literature suggests that Oslo has higher hip fracture incidences than any other region in Norway [1, 4, 29]. In 1994–1995 the incidence of hip fracture in subjects ≥65 years (men and women combined) in Hordaland county (where Bergen is situated) was 11.6 per 1000 person years, whereas the corresponding incidence in Troms county (Tromsø) was 10.3 [4]. The results from this study can be questioned due to some methodological problems. However, forearm fracture rates in Bergen and Oslo have previously been shown to be similar [30, 31], both being the highest ever reported internationally. Anyhow, there is an urgent need for further fracture incidence studies in Norway.
We calculated predicted hip fracture risks in the cities to evaluate potential consequences of the differences in BMD. In these calculations, we used a relative risk of 2.6 per standard deviation decrease in BMD based on a meta-analysis by Marshall et al. [16]. Compared with the data in Tromsø, the age-adjusted BMD differences in elderly women translates to a 42% increased risk of hip fractures in Bergen, whereas the differences in elderly men in Bergen correspond to a ∼25% increased risk. A recent meta-analysis showed that hip BMD was less effective in predicting fractures with advancing age [17]. They found a relative risk of 3.7 at the age of 50 for women and men combined, whereas the risk was 2.6 at the age of 75. However, since no separate risk for men and women with advancing age was presented, we chose the conservative estimate of 2.6 for both men and women. If anything, we may have underestimated the predicted risk of hip fracture.
Although the participation rates were generally quite high, the proportion of subjects who were scanned differed between age groups and study sites (Table 2), we cannot exclude the possibility that selection bias might have affected our results.
The International Society for Clinical Densitometry recommends in vivo calibration when BMD from different models or makes are quantitatively compared [21]. We followed this recommendation and adjusted our data according to our own vivo calibration studies. It is possible that the extensive calibration might have introduced errors. However, when including the errors from the calibration in our analyses (Appendix), there were only minor changes in the results, indicating that the observed BMD differences are real and not merely measurement artefacts.
BMD measurements are corrected for the area scanned but not for the true volume of the bones [32]. Due to larger volume, larger skeletons generally appear to have greater BMD, even though the actual volumetric tissue density of bone may not be higher. In this study, the population of Tromsø had the lowest body height and the highest BMD. Thus, differences in body height cannot explain the observed differences in BMD.
We did not have comparable information on ethnicity from Tromsø and Bergen, but the number of nonethnic Norwegians in Bergen was small (0.7%). As the non-western population of Bergen is larger than the population of Tromsø (6.6% versus 3.8%) [25], it is not likely that the number of non-western subjects was considerably higher in Tromsø than in Bergen, and even if so the percentage would be very low. On the other hand, other ethnic differences such as the number of subjects with Sami background may have affected our results. The Sami and Finnish populations in Tromsø are mixed with ethnic Norwegians, making the definition of ethnicity very complex. However, the majority of subjects in Tromsø have an ethnic Norwegian background, whereas approximately 10%–20% in Tromsø have a Sami, Finnish or Sami/Finnish background [33]. If the ethnic Norwegians in Tromsø had the same BMD levels as subjects in Bergen, the Sami/Finnish population in Tromsø would have an exceptionally high BMD to fully explain the higher BMD in Tromsø found in this study, which is not likely.
Of the subjects in Tromsø 18.6% lived in areas classified as rural. Subjects living in rural areas in Norway have been shown to have higher forearm BMD [18]. In this study we found differences in hip BMD only between elderly women living in rural and urban areas of Tromsø. Excluding subjects living in rural areas in Tromsø did not change the results. Hence, the BMD differences observed in our study cannot be explained by inclusion of the rural population of Tromsø. On the other hand Tromsø is a small city (65,000 inhabitants) compared with Bergen (245,000 inhabitants), and might not be comparable with respect to urbanization.
Norwegians have a high dietary intake of vitamin D, and diet is very important for the vitamin D status during the winter season when sun exposure is too low to synthesize vitamin D in the skin [34]. Differences in cutaneous vitamin D production due to different latitudes are not likely to explain our findings, as the subjects living furthest north had the highest BMD levels. On the other hand, serum levels of vitamin D could be different between the populations due to different dietary vitamin D intake or differences in time spent outdoors and this should be evaluated in further studies.
In conclusion, we found substantial differences in hip BMD between Tromsø and Bergen in both men and elderly women. Further studies addressing hip fracture incidences in Norway and potential explanatory factors for BMD differences are warranted.
References
Falch JA, Ilebekk A, Slungaard U (1985) Epidemiology of hip fractures in Norway. Acta Orthop Scand 56:12–16
Lofthus CM, Osnes EK, Falch JA et al (2001) Epidemiology of hip fractures in Oslo, Norway. Bone 29:413–418
Finsen VV (2004) Hip fracture incidence in central Norway: a followup study. Clinical orthopaedics and related research:173–178
Bulajic-Kopjar M, Wiik J, Nordhagen R (1998) Regional differences in the incidence of femoral neck fractures in Norway. Tidsskr Nor Laegeforen 118:30–33
Finsen V, Benum P (1987) Changing incidence of hip fractures in rural and urban areas of central Norway. Clin Orthop Relat Res:104–110
Falch JA, Kaastad TS, Bohler G et al (1993) Secular increase and geographical differences in hip fracture incidence in Norway. Bone 14:643–645
Sanders KM, Nicholson GC, Ugoni AM, Seeman E, Pasco JA, Kotowicz MA (2002) Fracture rates lower in rural than urban communities: the Geelong Osteoporosis Study. J Epidemiol Commun Health 56:466–470
Mannius S, Mellstrom D, Oden A, Rundgren A, Zetterberg C (1987) Incidence of hip fracture in western Sweden 1974–1982. Comparison of rural and urban populations. Acta Orthop Scand 58:38–42
Sernbo I, Johnell O, Andersson T (1988) Differences in the incidence of hip fracture. Comparison of an urban and a rural population in southern Sweden. Acta Orthop Scand 59:382–385
Chevalley T, Herrmann FR, Delmi M et al (2002) Evaluation of the age-adjusted incidence of hip fractures between urban and rural areas: the difference is not related to the prevalence of institutions for the elderly. Osteoporos Int 13:113–118
Madhok R, Melton LJ III, Atkinson EJ et al (1993) Urban vs rural increase in hip fracture incidence. Age and sex of 901 cases 1980–89 in Olmsted County, U.S.A. Acta Orthop Scand 64:543–548
Sogaard AJ, Gustad TK, Bjertness E et al (2007) Urban-rural differences in distal forearm fractures: Cohort Norway. Osteoporos Int 18:1063–1072
Sanders KM, Nicholson GC, Ugoni AM et al (2002) Fracture rates lower in rural than urban communities: the Geelong Osteoporosis Study. J Epidemiol Community Health 56:466–470
Jonsson B, Gardsell P, Johnell O et al (1992) Differences in fracture pattern between an urban and a rural population: a comparative population-based study in southern Sweden. Osteoporos Int 2:269–273
Blake GM, Fogelman I (2007) The role of DXA bone density scans in the diagnosis and treatment of osteoporosis. Postgrad Med J 83:509–517
Marshall D, Johnell O, Wedel H (1996) Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 312:1254–1259
Johnell O, Kanis JA, Oden A et al (2005) Predictive value of BMD for hip and other fractures. J Bone Miner Res 20:1185–1194
Meyer HE, Berntsen GK, Sogaard AJ et al (2004) Higher bone mineral density in rural compared with urban dwellers: the NOREPOS study. Am J Epidemiol 160:1039–1046
Kolta S, Ravaud P, Fechtenbaum J et al (1999) Accuracy and precision of 62 bone densitometers using a European Spine Phantom. Osteoporos Int 10:14–19
Lunt M, Felsenberg D, Adams J et al (1997) Population-based geographic variations in DXA bone density in Europe: the EVOS Study. European Vertebral Osteoporosis. Osteoporos Int 7:175–189
Shepherd JA, Lu Y, Wilson K et al (2006) Cross-calibration and minimum precision standards for dual-energy X-ray absorptiometry: the 2005 ISCD Official Positions. J Clin Densitom 9:31–36
Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501
The Tromsø Study. University of Tromsø. http://tromsoundersokelsen.no
Gjesdal CG, Aanderud SJ, Haga HJ et al (2004) Femoral and whole-body bone mineral density in middle-aged and older Norwegian men and women: suitability of the reference values. Osteoporos Int 15:525–534
Statistics Norway. http://www.ssb.no
Omsland TK, Emaus N, Gjesdal CG et al (2008) In Vivo and In Vitro Comparison of Densitometers in the NOREPOS Study. J Clin Densitom 11:276–282
Naess O, Sogaard AJ, Arnesen E et al (2007) Cohort Profile: Cohort of Norway (CONOR). Int J Epidemiol
Binkley N, Kiebzak GM, Lewiecki EM et al (2005) Recalculation of the NHANES database SD improves T-score agreement and reduces osteoporosis prevalence. J Bone Miner Res 20:195–201
Wasmuth HH, Reikeras O, Roald HE (1992) Hip fractures in Troms and Oslo in 1989. Risk development 1978–89. Tidsskr Nor Laegeforen 112:190–193
Hove LM, Fjeldsgaard K, Reitan R et al (1995) Fractures of the distal radius in a Norwegian city. Scand J Plast Reconstr Surg Hand Surg 29:263–267
Falch JA (1983) Epidemiology of fractures of the distal forearm in Oslo, Norway. Acta Orthop Scand 54:291–295
Compston JE (1995) Bone density: BMC, BMD, or corrected BMD? Bone 16:5–7
Berntsen GK, Fonnebo V, Tollan A et al (2001) Forearm bone mineral density by age in 7,620 men and women: the Tromso study, a population-based study. Am J Epidemiol 153:465–473
Brustad M, Alsaker E, Engelsen O et al (2004) Vitamin D status of middle-aged women at 65–71 degrees N in relation to dietary intake and exposure to ultraviolet radiation. Pub Health Nutr 7:327–335
Acknowledgments
This study was supported by a grant from the Research Council of Norway and the Norwegian Osteoporosis Foundation.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
The NOREPOS Core Research Group: Nina Emaus, Guri Grimnes (Tromsø), Haakon E. Meyer, Anne Johanne Søgaard (Oslo), Berit Schei, Siri Forsmo (Nord-Trøndelag), and Grethe S. Tell, Clara Gram Gjesdal (Bergen).
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Omsland, T.K., Gjesdal, C.G., Emaus, N. et al. Regional differences in hip bone mineral density levels in Norway: the NOREPOS study. Osteoporos Int 20, 631–638 (2009). https://doi.org/10.1007/s00198-008-0699-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0699-7