
Abstract
Summary
Replication is a critical step to validate positive genetic associations. In this study, we tested two previously reported positive associations. The low density lipoprotein receptor-related protein 5 (LRP5) Val667Met and lumbar spine bone density are replicated. This result is in line with results from large consortiums such as Genomos. However, the estrogen-related receptor alpha (ESRRA) repeat in the promoter is not replicated although the polymorphism studied was functional and could have been a causative variant.
Introduction
We sought to validate associations previously reported between LRP5 V667M polymorphism and lumbar spine (LS, p = 0.013) and femoral neck (FN, p = 0.0002) bone mineral density (BMD), and between ESRRA 23 base pair repeat polymorphism and LS BMD (p = 0.0036) in a sample of premenopausal Caucasian women using an independent sample.
Methods
For the replication sample, we recruited 673 premenopausal women from the Toronto metropolitan area. All women were Caucasian and had BMD measured. LRP5 V667M was genotyped by allele-specific PCR and ESRRA repeats by sizing of PCR products on agarose gels.
Results
We reproduced the same association as we reported previously between LRP5 V667M and LS BMD (p = 0.015) but not with FN BMD (p = 0.254). The combined data from the two populations indicate an effect size of 0.28SD for LS BMD (p = 0.00048) and an effect size of 0.26 SD for FN BMD (p = 0.00037). In contrast, the association we reported earlier between ESRRA repeats and LS BMD was not replicated in the sample from Toronto (p = 0.645).
Conclusions
The association between LRP5 V667M and LS BMD is confirmed but not that between ESRRA repeats and LS BMD. This result indicates that it is imperative to validate any positive association in an independent sample.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a common disease of later life characterized by reduced bone mass and increased risk of fragility fractures and is responsible for substantial morbidity and mortality among the elderly. The principal determinant of skeletal fragility is bone mineral density (BMD), which is largely under genetic control [1]. In women, who are more prone to suffer from osteoporosis than men, BMD is a function of peak bone mass attained in young adulthood, and the rate of bone loss, much of which occurs predominantly over the 5-year-period following menopause and then by a slower rate of bone loss related to aging which also affects men.
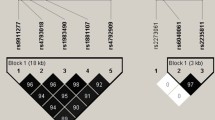
Peak bone mass is under strong genetic influence and is a good phenotype to study gene variants responsible for BMD variation in the normal population [2–4]. The past decade has seen an important increase in the use of association studies with candidate genes for the genetic analysis of complex traits such as bone mineral density and/or osteoporosis. However, this approach has been largely criticized because of non-replication of results [5, 6]. The challenge is to separate true associations from the high number of false positives through attempts to replicate positive findings in subsequent studies but with a clear definition of what constitutes a positive replication [7]. We previously reported on positive associations between BMD and two candidate genes, LRP5 and ESRRA, in a population of premenopausal women from Quebec [8, 9]. We now present a replication study in a different population of premenopausal women from Toronto [10]. These associations were observed with a functional polymorphism in the promoter of the ESRRA gene (rs3217060) and a coding SNP Val667Met (rs4888321) in the LRP5 gene. The missense polymorphism Val667Met in LRP5 gene is thought to be deleterious to the protein given its high conservation among species and its crucial location in the third propeller domain [11]. Numerous studies have reported an association between SNPs in the same linkage disequilibrium block in the LRP5 gene and BMD in males and females [8, 11–17].
The polymorphism studied in the ESRRA promoter is a 23-nucleotide repeat acting as a hormone response element [18, 19]. In 88% of the population the 23-nucleotide repeat is present in two copies and in 12% of the population it is found in three or four copies. Functional studies have shown that ESRRA expression was increased when coupled in cis with a higher number of repeats [19]. Previously, we reported that this polymorphism was associated with a significant difference in lumbar spine BMD in a sample of premenopausal women [9]. Although ESRRA is an attractive candidate gene, based on in vitro studies showing that inhibition of the estrogen-related receptor protein expression in rat calvaria cells results in a decreased mineralized bone nodule number and overexpression of the protein results in an increase [20], our previously observed association remained to be validated in an independent sample.
Here, we use a well-characterized sample of young women to reassess these two previously reported associations and we show that the association of LS BMD is replicated for LRP5 Val667Met, but not for ESRRA.
Methods
Subjects
Between 1995 and 1997, women between 18 and 35 years of age were recruited through advertisements in local newspapers and posted flyers [10, 21]. They were screened by telephone questionnaire before enrolment. Of the 993 subjects assessed, some were excluded because of age or comorbid conditions known to be associated to bone loss (nutritional disorder, alcoholism, pre-existing disorders of bone and mineral metabolism, degenerative bone disease, hepatic disease or renal insufficiency) plus those who had undergone bilateral oophorectomy. Further sample selection was applied so that only unrelated women of Caucasian ancestry were included, and in the end, clinical data and DNA samples were available on 675 subjects. The Ethics Review Office of University of Toronto approved the study protocol. After obtaining written consent, each subject completed a standardized questionnaire about lifestyle factors. For the present study, the variables were regrouped and numbers were rounded in the same way as the data for the previously reported Quebec sample (Table 1).
DXA measurements
As described previously [21], BMD in the Toronto sample was measured at the same sites [L2-L4 of lumbar spine (LS)and FN] as the Quebec sample using the same densitometric instrumentation (DPX-L Absorptiometer, Lunar Corp., Madison WI, USA). The coefficient of variation was 1.2% for the spine and 1.3% for the femur.
DNA preparation and genotyping
Blood samples were collected and total genomic DNA was extracted as described [22]. For about one-third of the samples, only a minute quantity of DNA remained and for those, whole genome amplification was performed using the Genomiphi™ DNA amplification kit version 2 (GE HealthCare Life Sciences).
The DNA was distributed onto bar coded 96-well plates and further diluted with a solution of 10 mM TRIS-HCl pH 7.5 containing 56.3 μM of an inert fluorescent dye, ROX (Molecular Probes, Invitrogen). The final concentration of ROX was 45 μM in each DNA sample and the mean DNA concentration was 5 ng/μl. For each PCR, 5 μl was used regardless of the exact DNA concentration.
LRP5 Val667Met was genotyped by allele-specific PCR. The reaction was performed as described previously [8]. Call rate (percentage of individuals with a genotype) was > 99.5%. Genotyping for the ESRRA promoter repeat sequence was performed as described previously [9]. Call rate was > 99%.
Statistical analyses
Comparisons between proportions were performed by χ2 test, whereas Student test (t-test) was used for comparisons of means (Table 1). The exact test from Guo et al. [23] was used to verify any departure from Hardy–Weinberg equilibrium (HWE). Since the rare homozygote genotype frequency for each of the two polymorphisms was lower than 5%, these genotypes were combined with the heterozygote genotype for all analyses. Differences in BMD among the genotypes groups were tested using covariance analysis with adjustment for age, weight, smoking, age at menarche and physical activities. The magnitude of effect was expressed in standard deviations (SD) and was evaluated using the difference between the two estimated means of compared genotypes divided by the standard deviation of the group studied. Data were analyzed using statistical software package SAS 9.1.3 (SAS Institute, Cary, NC, USA) and statistical software package SPSS 11.0 for Mac OS X (Chicago, IL, USA).
Results
Sample comparisons
The largest contrast between the two samples was age (Table 1). Women in the Toronto sample were on average 17 years younger than their Quebec counterparts, and the large difference in age was reflected in the BMD data (Table 1). It was also reflected in the self-reported level of physical activity that the older Quebec women were more sedentary than the younger Toronto women (26% vs. 9%, respectively). While current smokers were about the same (14% vs. 12%, respectively), past smokers were more numerous in the Quebec sample. Whether this was only a factor of age, or whether it was also due to different smoking patterns in the populations from which the samples were drawn (Statistics Canada, http://www40.statcan.ca/l01/cst01/health07a.htm?sdi=smokers) could not be determined. Finally the difference in age at menarche was also significant, although it was not large.
To correct for the bias introduced by these differences in covariates, a covariance analysis for BMD was performed with the data regrouped (N = 1382) which took into account age, weight, smoking habits, age at menarche and physical activity, and included a dummy variable for sample origin. For lumbar spine, the estimated marginal mean was 1.178 g/cm2 for Quebec and Toronto samples (p = 0.99). For femoral neck, the means were 0.953 g/cm2 for Quebec and 0.951 g/cm2 for Toronto (p = 0.86). Thus no statistically significant difference was observed between these two samples for their adjusted BMD at both sites.
LRP5 polymorphism
In the Toronto sample, the frequencies of the three V667M genotypes (VV, VM, and MM) were 594, 71, and 3, respectively. These frequencies were not different from the Quebec sample (625, 79 and 5 respectively) and the deviation from Hardy–Weinberg equilibrium was not statistically significant (exact Test p = 0.48). Given the low number of MM homozygotes in the Toronto sample, they were combined with the heterozygotes as we did for the Quebec sample (8). Adjusted covariance analysis was performed for each BMD. For lumbar spine (Table 2), the association in the Toronto sample was of the same magnitude and in the same direction (minor allele associated with lower BMD means) as in the Quebec sample [0.28SD (p = .015) vs. 0.27SD (p = .013), respectively]. In the combined data (Table 3), the magnitude of effect was unchanged but the significance was stronger (p = 0.0005, n = 1377).
For the femoral neck (Table 2 and 3), no association was seen in the Toronto sample (p = 0.25), which contrasts with the Quebec sample (p = 0.00019). However, the tendency in the Toronto sample was in the same direction (minor allele associated with lower FN BMD), and after combining the two samples, the overall association was statistically significant (p = .00037).
ESRRA polymorphism
In the Toronto sample, the genotype frequencies for the ESRRA promoter repeats were: 2/2 (566), 2/3 (90), 3/3 (5), 2/4 (1) and 1/2 (1). The frequency of 3- or 4-repeat alleles was slightly higher than in the Quebec sample (7.6% vs. 6.1%). One- and four-repeat alleles were rare (<1% of all alleles). As tested with the exact test from Guo [23], the distribution of genotypes was in Hardy–Weinberg equilibrium (p = 0.54). For the purposes of sample comparison, Toronto women with 1/2 and 2/2 genotypes were combined for contrast with those having 2/3, 3/3 and 2/4 genotypes, as in the previous report [9]. Adjusted covariance analysis indicates no statistically significant difference (p = 0.645) between the estimated means for LS BMD (Table 2). In addition, the frequent genotype tended to be associated with the highest mean, a tendency in the direction opposite to that of the Quebec sample (Table 3). Combining data understandably showed no significant difference (p = 0.074, n = 1373), and the results at the femoral neck were also not statistically significant (Table 2).
Discussion
The main objective of this study was to replicate previously observed associations between BMD and two independent candidate gene polymorphisms—LRP5 V667M and ESRRA rs3217060—in a new sample. Such replication is essential for establishing the generalizability of a genotype-phenotype association. As yet, however, there is no agreement about what constitutes a replication or refutation. Recently, a working group on replication in association studies has suggested criteria for establishing a positive replication [7].
Sample size should be large enough to convincingly distinguish the effect, replication studies should preferably be conducted in independent data sets, the same or very similar phenotype should be analyzed and a similar population should be studied with differences described. Similar magnitude of effect and significance should be demonstrated, in the same direction and with the same SNP, significance should be obtained with the genetic model reported in the initial study, a strong rationale should be provided for selecting SNPs and a joint analysis should lead to a smaller p-value than that seen in the initial report [7].
In the present study, the sample for replication was of similar size to the initial study and the two data sets were independent. The characteristics of the Toronto sample were well established, and significant associations between BMD and polymorphisms of the estrogen receptor alpha (ESR1), the vitamin D receptor (VDR), and the parathyroid hormone receptor (PTHR1) have been reported before [10, 21, 24–26]. Both samples were Caucasian, female and premenopausal. The main difference was age but given that the primary variables of interest–BMD at LS and FN–were quantitative traits influenced by age, then age was an essential covariate in the statistical models. The same phenotype was analysed, that is bone mineral density at lumbar spine and femoral neck and these measures were compared in the two sample populations after adjustment for age, weight, smoking habit, age at menarche and physical activity and no significant difference was observed.
The first variant studied was in a well-studied gene, LRP5. Many studies have now been published showing evidence of an allelic association between polymorphisms in LRP5 and BMD [8, 11–17, 27]. Many variants have been studied, but the most studied and most likely functional candidate according to many authors was an alanine to valine amino acid substitution at position 1330 (A1330V) [28]. However, we have shown with the analysis of haplotypes that V667M, which is in linkage disequilibrium with the previous, was more likely the causative variant [8]. V667M was thus studied in a new sample of premenopausal women and the association was analyzed with the same model as in our initial study. We obtained the same result as previously with the new sample that is a similar magnitude of effect with significance and in the same direction for LS BMD. After combining the data of the two samples, the p-value was reduced from 0.013 to 0.00048 (Table 3). This result was established as a positive replication according to the criteria listed above and gave us confidence that it was a true association. Furthermore, the Genomos Consortium recently reported the results of a meta-analysis with a large sample of more than 35,000 men and women and they found a similar result (LS BMD difference in women of 0.023 g/cm2 with p = 1.06 × 10–8) ([29] and personal communication).
While we obtained replication for LS BMD this was not the case for FN BMD. The initial observation in premenopausal women was very strong with a magnitude of 0.36 SD and a very low p-value. This result could have been obtained by chance rather than representing the true variation in a large population. The analysis of the second premenopausal sample suggests caution interpreting such a result given that we expected a very modest effect from each gene involved in the attainment of peak bone mass. By combining the two samples (1377 women) the magnitude of the effect was 0.26 SD (p = 0.00037) a value similar to what was observed at the lumbar spine. This was not a replication according to the suggested criteria for establishing positive replication [7]. The Genomos consortium obtained a significant association with FN BMD with the very large sample of women but of much lower magnitude (a difference of means of 0.009 g/cm2 with a p = 0.0017) than for LS BMD.
The second polymorphism analyzed in this study was a tandem repeat containing a hormone responsive element and located in the ESRRA gene promoter. It was mainly found in two copies of a 23 base pair element; however, about 12% of the population had three or four copies. It was shown previously that the element was recognized by the protein ERR1 and an increase in expression dependent on repeat number occurred with the help of the protein PGC-1 alpha (peroxisome proliferator-activated receptor γ coactivator-1α) as a co-activator [19]. Thus it was a functional polymorphism controlling the expression of a gene expressed in osteoblasts and with a described function in the proliferation and differentiation of osteogenic precursors [20, 30]. The functional aspect of the polymorphism added credibility to the association observed with the lumbar spine BMD that was also supported by a biological mechanism [9]. However, the absence of any association in the Toronto sample (p = 0.645) and also in the joint sample (n = 1373 and p = 0.0737) suggested that it could not be generalized. The same held true for FN BMD (Table 2 and 3).
Possible limitations of this study included the fact that the Toronto sample had a power of only 63% to observe the difference obtained in the Quebec sample. This power is actually the same as in the Quebec sample (a slightly lower number of women but with a smaller standard deviation) but although the association might be true there was a 37% chance of not observing it in the replication sample. Lack of power may be an explanation for the fact that the association between LRP5 and FN BMD was not replicated. On the other hand, the combined samples had a power > 80% of detecting a difference of 0.28 standard deviation which reduced the risk of having missed a true association with ESRRA.
These two examples showed clearly the importance of replication of a genotype-phenotype association [7, 31]. It gave even more credibility to LRP5 V667M playing a role in the variation of bone mineral density in the normal population and gave precision to the magnitude of the effect while it limited the potential role of the number of ESRRA repeats in the promoter. LRP5 Val667Met might thus be considered as one of the validated marker among numerous genetic factors still to be discovered to identify women with a low peak bone mass, which is a well-known risk factor for developing osteoporosis later in life.
References
Pocock NA, Eisman JA, Hopper JL et al (1987) Genetic determinants of bone mass in adults. A twin study. J Clin Invest 80:706–710
Brown LB, Streeten EA, Shapiro JR et al (2005) Genetic and environmental influences on bone mineral density in pre- and post-menopausal women. Osteoporos Int 16:1849–1856
Danielson ME, Cauley JA, Baker CE et al (1999) Familial resemblance of bone mineral density (BMD) and calcaneal ultrasound attenuation: the BMD in mothers and daughters study. J Bone Miner Res 14:102–110
Hunter DJ, de Lange M, Andrew T et al (2001) Genetic variation in bone mineral density and calcaneal ultrasound: a study of the influence of menopause using female twins. Osteoporos Int 12:406–411
Colhoun HM, McKeigue PM, Davey Smith G (2003) Problems of reporting genetic associations with complex outcomes. Lancet 361:865–872
Tabor HK, Risch NJ, Myers RM (2002) Opinion: candidate-gene approaches for studying complex genetic traits: practical considerations. Nat Rev Genet 3:391–397
Chanock SJ, Manolio T, Boehnke M et al (2007) Replicating genotype-phenotype associations. Nature 447:655–660
Giroux S, Elfassihi L, Cardinal G et al (2007) LRP5 coding polymorphisms influence the variation of peak bone mass in a normal population of French-Canadian women. Bone 40:1299–1307
Laflamme N, Giroux S, Loredo-Osti JC et al (2005) A frequent regulatory variant of the estrogen-related receptor alpha gene associated with BMD in French-Canadian premenopausal women. J Bone Miner Res 20:938–944
Rubin LA, Hawker GA, Peltekova VD et al (1999) Determinants of peak bone mass: clinical and genetic analyses in a young female Canadian cohort. J Bone Miner Res 14:633–643
Ferrari SL, Deutsch S, Choudhury U et al (2004) Polymorphisms in the low-density lipoprotein receptor-related protein 5 (LRP5) gene are associated with variation in vertebral bone mass, vertebral bone size, and stature in whites. Am J Hum Genet 74:866–875
Koller DL, Ichikawa S, Johnson ML et al (2005) Contribution of the LRP5 gene to normal variation in peak BMD in women. J Bone Miner Res 20:75–80
Koay MA, Woon PY, Zhang Y et al (2004) Influence of LRP5 polymorphisms on normal variation in BMD. J Bone Miner Res 19:1619–1627
van Meurs JB, Rivadeneira F, Jhamai M et al (2006) Common genetic variation of the low-density lipoprotein receptor-related protein 5 and 6 genes determines fracture risk in elderly white men. J Bone Miner Res 21:141–150
Ezura Y, Nakajima T, Urano T et al (2007) Association of a single-nucleotide variation (A1330V) in the low-density lipoprotein receptor-related protein 5 gene (LRP5) with bone mineral density in adult Japanese women. Bone 40:997–1005
Xiong DH, Lei SF, Yang F et al (2007) Low-density lipoprotein receptor-related protein 5 (LRP5) gene polymorphisms are associated with bone mass in both Chinese and whites. J Bone Miner Res 22:385–393
Koay MA, Tobias JH, Leary SD, et al. (2007) The effect of LRP5 polymorphisms on bone mineral density is apparent in childhood. Calcif Tissue Int
Liu D, Zhang Z, Teng CT (2005) Estrogen-related receptor-gamma and peroxisome proliferator-activated receptor-gamma coactivator-1alpha regulate estrogen-related receptor-alpha gene expression via a conserved multi-hormone response element. J Mol Endocrinol 34:473–487
Laganiere J, Tremblay GB, Dufour CR et al (2004) A polymorphic autoregulatory hormone response element in the human estrogen-related receptor alpha (ERRalpha) promoter dictates peroxisome proliferator-activated receptor gamma coactivator-1alpha control of ERRalpha expression. J Biol Chem 279:18504–18510
Bonnelye E, Merdad L, Kung V et al (2001) The orphan nuclear estrogen receptor-related receptor alpha (ERRa) is expressed throughout osteoblast differentiation and regulates bone formation in vitro. J Cell Biol 153:971–983
Jamal SA, Ridout R, Chase C et al (1999) Bone mineral density testing and osteoporosis education improve lifestyle behaviors in premenopausal women: a prospective study. J Bone Miner Res 14:2143–2149
Peltekova VD, Rubin L, Uitterlinden AG et al (1997) Direct haplotyping at the vitamin D receptor locus improves genetic resolution. J Bone Miner Res 12:494–495
Guo SW, Thompson EA (1992) Performing the exact test of Hardy–Weinberg proportion for multiple alleles. Biometrics 48:361–372
Scillitani A, Jang C, Wong BY et al (2006) A functional polymorphism in the PTHR1 promoter region is associated with adult height and BMD measured at the femoral neck in a large cohort of young caucasian women. Hum Genet 119:416–421
Hawker GA, Jamal SA, Ridout R et al (2002) A clinical prediction rule to identify premenopausal women with low bone mass. Osteoporos Int 13:400–406
Patel MS, Cole DE, Smith JD et al (2000) Alleles of the estrogen receptor alpha-gene and an estrogen receptor cotranscriptional activator gene, amplified in breast cancer-1 (AIB1), are associated with quantitative calcaneal ultrasound. J Bone Miner Res 15:2231–2239
Xiong DH, Shen H, Zhao LJ et al (2006) Robust and comprehensive analysis of 20 osteoporosis candidate genes by very high-density single-nucleotide polymorphism screen among 405 white nuclear families identified significant association and gene-gene interaction. J Bone Miner Res 21:1678–1695
Ralston SH (2007) Genetics of osteoporosis. Proc Nutr Soc 66:158–165
van Meurs JB et al (2007). ASBMR 29th Annual Meeting Honolulu, Hawaii, USA. Abstract # 1107.
Bonnelye E, Vanacker JM, Dittmar T et al (1997) The ERR-1 orphan receptor is a transcriptional activator expressed during bone development. Mol Endocrinol 11:905–916
Ioannidis JP, Ntzani EE, Trikalinos TA et al (2001) Replication validity of genetic association studies. Nat Genet 29:306–309
Acknowledgments
The authors thank Sylvie Lemieux and Betty Wong for expert technical work and all the women who agreed to participate to this study. Financial support was provided by the Canadian Institutes for Health Research grant # 62913 and a grant from Dairy Farmers of Canada (to DECC). Infrastructure support to the research center was provided by the Fonds de Recherche en Santé du Quebec. FR holds a Fonds de la Recherche en Santé du Quebec national scientist award.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Giroux, S., Elfassihi, L., Cole, D.E.C. et al. Replication of associations between LRP5 and ESRRA variants and bone density in premenopausal women. Osteoporos Int 19, 1769–1775 (2008). https://doi.org/10.1007/s00198-008-0617-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0617-z