
Abstract
Osteoporotic fractures are increasing among Asian populations in both genders, but the risk factors for low bone mineral density (BMD) in Asian men is unclear. To determine the hormonal and lifestyle risk factors for low BMD in Asian men, we studied 407 community-dwelling southern Chinese men aged 50 years and above. Medical history and lifestyle habits were obtained with a structured questionnaire. Dietary calcium and phytoestrogen intake were assessed by a semi-quantitative questionnaire. BMD at the spine and hip were measured by dual-energy X-ray absorptiometry (DXA). Fasting blood was analyzed for 25(OH)D, parathyroid hormone (PTH), total and bioavailable estradiol (bio-E) and testosterone (bio-T). The mean age of the cohort was 68.42±10.4 (50–96) years. In the linear regression model, weight, age, body mass index (BMI), bio-E, PTH, cigarette smoking and weight-bearing exercise were significant determinants of total hip BMD. Together they explained 55% of the total variance of hip BMD, with body weight being the most important determining factor. With age and weight adjustment, height, bio-T and flavonoid intake were identified as additional determinants of total hip BMD. Strategies to prevent bone loss and osteoporosis in Asian men should include lifestyle modification and maintenance of hormonal sufficiency.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporotic fractures are on the increase among both Asian men and Asian women [1]. Among the southern Chinese in Hong Kong, the age-adjusted hip fracture rate had increased by more than two fold during the past two decades [2]. From 1988 to 1992, hip fractures in northern China increased by 33% in men and 34% in women [3]. In Singapore, the incidence increased by 0.7% per year in men and 1.2% per year in women from 1991 to 1998 [4]. The problem of osteoporosis in men has been overlooked in the past [5]. Although not as common as in women, hip and spine fractures in men are associated with higher morbidity and mortality than in women [6]. It has been estimated that up to one-third of all fractures occur in men [7], and the prevalence of vertebral fractures in men is similar to, or even higher than, that in women [8, 9]. With progressive aging of the Asian populations, there will be a vast increase in the number of osteoporotic fractures in Asian men and women [1]. On the basis of population expansion, aging of the people, and estimation of lifetime risk of osteoporotic fractures, it was projected that, by 2050, half of the world’s hip fractures would occur in Asia, with the majority happening in China [10]. The understanding of the pathogenesis of osteoporotic fractures in Asian men will help in the formulation of rational prevention and treatment programs.
Although large-scale epidemiological studies have been conducted in Caucasian men, data on determinants of bone mineral density (BMD) in Asian men are scanty. BMD is an important risk factor for fracture, and it is widely believed that BMD acts as an intermediary variable on the biological pathways linking various anthropometric, lifestyle, dietary and hormonal risk factors with fractures. In view of the paucity of information on BMD and fracture in Asian men, this study aimed to evaluate the relationship of lifestyle and hormonal factors with BMD in a cohort of community-dwelling Chinese men.
Materials and methods
Subjects
Community dwelling southern Chinese men aged above 50 years were recruited during health talks and health fairs held in various districts of Hong Kong between 1998 and 2002. Similarly, healthy young men aged 20 to 39 years were recruited in the same setting for determination of peak BMD values of the population. Subjects with known history of metabolic bone disease or taking any form of medication for the treatment of osteoporosis were excluded from the study. After exclusion, 407 volunteers aged above 50 years and 124 young men were invited to the Osteoporosis Center at Queen Mary Hospital for assessment.
All subjects were instructed by a trained technician to complete a detailed questionnaire on demographic information, various aspects of lifestyle habits, including smoking, alcohol consumption and physical activity, personal and family history of fracture, medical history including that of gastrointestinal, thyroid or parathyroid disease, diabetes mellitus, Parkinsonism, stroke, psychiatric illness; and consumption of medication such as oral and inhaled steroid, diuretics and hypnotics. Fracture history was confirmed by retrieval of X-ray reports and hospital discharge summaries. Calcium and phytoestrogen intake were assessed by a semi-quantitative questionnaire [11]. The standard portion size was specified in commonly used units or portions, as judged by a registered dietitian. Physical activity was assessed as the average number of hours per day each individual spent on walking and other weight bearing exercise such as tai chi, jogging, and calisthenics. Handgrip strength was determined by a hand-held dynamometer. Body weight was measured, with the subject wearing light indoor clothing, by an electronic scales, and height was determined by a wall-mounted stadiometer. The study was approved by the ethics committee of the University of Hong Kong and conducted according to the declaration of Helsinki.
Dual-energy X-ray absorptiometry
BMD was measured at the lumbar spine (L1–L4), femoral neck, trochanter, Ward’s triangle and total hip by dual-energy X-ray absorptiometry (Hologic QDR 2000 Plus, Hologic, Waltham, Mass., USA). The in vivo precision of the machine for lumbar spine, femoral neck and total hip measurement was 1.2%, 1.5% and 1.5%, respectively [12]. The BMD data of the young subjects revealed peak young mean (SD) value at the spine, femoral neck and total hip of 0.837 (0.117) g/cm2, 0.941 (0.115) g/cm2 and 0.969 (0.102) g/cm2, respectively. Those results were used to determine the BMD T scores of the older men.
Hormone assays
Fasting blood was taken for biochemistry and hormone assessment. Both serum total estradiol (E) and testosterone (T) were measured by competitive chemiluminescent immunoassays (Ortho-Clinical Diagnostics, Rochester, New York, USA). Total E assay had an analytical sensitivity of 10 pmol/l, with intra-assay coefficient of variation (CV) of 13.4% at 21 pmol/l, 7.3% at 85 pmol/l, and 6.1% at 236 pmol/l, and inter-assay CV of 16.5% at 23 pmol/l, 8.8% at 87 pmol/l and 9.6% at 232 pmol/l. Total T assay had an analytical sensitivity of 0.03 nmol/l, with intra-assay CV of 8.1% at 1.68 pmol/l, 3.2% at 22.1 nmol/l and 4.2% at 54.9 nmol/l, and inter-assay CV of 8.5% at 1.64 nmol/l, 3.4% at 22.4 pmol/l and 4.5% at 55.7 nmol/l.
Bioavailable E and T (bio-E and bio-T) were measured after ammonium sulfate precipitation. Serum was treated with 50% ammonium sulfate. After centrifugation, the supernatant was assayed by radioimmunoassay (RIA) (T: DSL-4100, E: DSL-4400, Diagnostic Systems Laboratories, Tex., USA). The lowest detection limit for the T assay was 0.05 ng/ml, with intra-assay and inter-assay CV of 7.7% and 10.5% at concentrations of 0.52 ng/ml and 0.57 ng/ml, 8.1% and 5.7% at concentrations of 5.05 ng/ml and 6 ng/ml, and 6.7% and 8.1% at concentrations of 13.77 ng/ml and 13.62 ng/ml, respectively. E assay had an analytical sensitivity of 4.7 pg/ml, and intra-assay CV of 5.3% at 67 pmol/l, 5.3% at 156.4 pmol/l, and 3.2% at 392.5 pmol/l, and inter-assay CV of 8.1% at 68.3 pmol/l, 9.3% at 143.3 pmol/l and 8.1% at 409.2 pmol/l.
Serum parathyroid hormone (PTH) was measured by two-site sandwich chemiluminometric assay with a mouse monoclonal anti-human PTH antibody measuring intact PTH (Chiron Diagnostic Corporation, East Walpole, Mass., USA). Intra-assay CV was 8.5% at 13.4 pg/ml, 7.4% at 43.6 pg/ml and 5.7% at 161.3 pg/ml, while inter-assay CV was 11.8% at 14.1 pg/ml, 9.6% at 46.5 pg/ml and 7.2% at 159.6 pg/ml. 25(OH)D was measured by RIA (DiaSorin, Minn., USA) after extraction with acetonitrile. The sensitivity of the assay was 1.5 ng/ml, with an intra-assay CV of 11.7% at 8.6 ng/ml, 10.5% at 22.7 ng/ml, 8.6% at 33 ng/ml and 12.5% at 49 ng/ml.
Statistical modeling
BMD measurements at the spine, femoral neck and total hip region were analyzed as dependent variables. Correlations between the numerical independent variables and BMD were evaluated with Pearson’s correlation coefficients, while categorical variables were evaluated by independent-samples t-test. For continuous independent variables, they were dichotomized into two groups, using the upper or lower limit of the normal range for young healthy men as the cutoff value. All the significant predictors of BMD were entered into the linear regression model so that their contribution to the total variance in BMD could be determined. All analyses were performed with SPSS for Windows software version 10.0 (SPSS, Chicago, Ill., USA).
Results
Characteristics of the 407 subjects are summarized in Table 1. The mean age of the subjects was 68.4±10.4 (50–96) years. There were 124 (30.4%) subjects that reported at least one low-trauma fracture after the age of 50 years. The mean age at fracture for the whole cohort was 77.5±9.4 (53–95) years. There was a total of 93 hip fractures, 24 symptomatic spine fractures, two distal forearm fractures, two fractures at the clavicles, and three fractures of the humerus. Only 58% of these subjects reported weight-bearing activity for more than 1 h per day. The mean calcium intake was 675±289 mg/day, while the mean isoflavone and flavonoid intakes were 25±30 mg/day and 33±17 mg/day, respectively.
Table 2 shows the BMD and biochemical data of these subjects. The BMD at the spine, femoral neck and total hip was 0.92±0.17 g/cm2, 0.68±0.12 g/cm2, and 0.82±0.14 g/cm2, respectively, and the corresponding T score values were −0.55±1.31, −1.04±0.86, and −0.82±0.14, respectively. The hormone data revealed a mean 25(OH)D level of 22.7±6.6 ng/ml, with 11.5% of the subjects having serum 25(OH)D levels below 15 ng/ml. Serum PTH was negatively correlated with serum 25(OH)D levels (r=−0.155, P=0.03). Of the subjects, 6.6% had PTH levels above the upper normal cutoff value of 54 pg/ml, and among them, 30% had 25 (OH)D levels below 15 ng/ml.
With respect to the sex hormones, 34% had serum total T levels below 10 nmol/l, while 50% had bio-T levels below 6 nmol/l. As for serum total E and bio-E, 92% and 20.4%, respectively, of the subjects had levels below 114 pmol/l and 40 pmol/l, respectively, Only bio-E was associated with urinary calcium excretion (r=−0.167, P<0.02).
Age, weight, height, body mass index (BMI), history of smoking, current drinking, weight-bearing exercise, handgrip strength, intakes of calcium and flavonoids, serum albumin, PTH, bio-T and bio-E all correlated with BMD. Tables 3 and 4 show the simple correlation coefficients between BMD and various risk factors, while Tables 5 and 6 show the partial correlation coefficients between age and weight-adjusted BMD and these factors.
In the multiple regression analysis, weight (P=0.04), age (P=0.008), BMI (P<0.004), PTH (P=0.003), bio-E (P=0.02), smoking history (P=0.03) and weight-bearing exercise (P<0.001) were important determinants for total hip BMD (Table 7). Together, they explained 55% of the total variance of hip BMD. However, body weight alone explained 42% of the variance. For lumbar spine BMD, the significant determinants were weight (P<0.0001), bio-E (P=0.002), PTH (P=0.006) and exercise (P=0.046) (Table 8). Together, they explained 25% of the total variance in lumbar spine BMD.
Discussion
Our data revealed that, apart from age and weight, the independent risk factors associated with BMD in Chinese men were BMI, smoking, weight-bearing exercise, PTH and serum bio-E. To the best of our knowledge, this present report is the first observational study documenting the association between sex hormones and BMD in Asian men. In accordance with the proposed concept that estrogen deficiency is a major cause for the continuous phase of bone loss in elderly men [13], our data demonstrated that serum bio-E was an important predictor for BMD in elderly Chinese men. Apart from age and weight, bio-E was the most important determinants of the variance in total hip BMD in this cohort.
It is interesting to note that serum bio-E was inversely related to urinary calcium excretion in our men, suggesting that estrogen is important in regulating renal calcium conservation in men, as in postmenopausal women [14]. These results confirmed the findings of other observational studies of Caucasian populations that E [15, 16, 17, 18] and bio-E [15, 16, 19, 20], rather than T or bio-T, were the main determinants of BMD in men. Although hypogonadism is one of the major causes for osteoporosis in men, the association of total T and free or bio-T with BMD in elderly men is controversial [21, 22, 23, 24, 25]. It seems that there is a level of T below which there is an increased risk of osteoporosis, and the beneficial effect of T replacement on BMD is also evident only below a certain level of T [26]. Our data also confirmed that the use of the total T measurement alone may under-diagnose hypogonadism in elderly men [27].
Apart from sex steroids, the calcitropic hormones also play an important role in affecting age-related bone loss. The association of secondary hyperparathyroidism with high bone turnover, bone loss, and falls and fractures is well appreciated in postmenopausal women. In this study, we found that elevated PTH was present in 6.6% of the subjects and that PTH was also predictive of both total hip BMD and spine BMD. Among those with elevated PTH, 30% had 25(OH)D levels below 15 ng/ml. Within the whole cohort, 11.5% of the subjects had 25(OH)D levels below 15 ng/ml. This is an important observation, as it has always been thought that vitamin D deficiency is not a problem in subtropical areas where sunshine is adequate [2]. It is difficult to delineate sharp diagnostic criteria for mild vitamin D deficiency or insufficiency. Indeed, there are recent data that suggest that the cutoff value for sufficiency of 25(OH)D may be even higher to maintain positive calcium balance [28, 29].
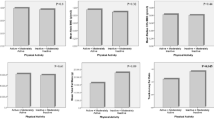
Our findings confirmed that body weight, body mass index, weight-bearing activity and muscle strength were important determinants of BMD. In this present study, we noted that the most commonly reported physical activity of the Chinese men was walking rather than any other forms of strenuous exercise or sports. In spite of the mild nature of this exercise, it remained an important contributor to the variance in BMD, independent of muscle strength. A recent animal study demonstrated that lower intensity but continued exercise was associated with more bone formation and higher mineral apposition rate than in animals randomized to more vigorous training followed by cessation of exercise [30].
As in other studies, we documented the association of smoking with BMD in men [31]. However, unlike in Caucasian populations, alcohol consumption was found not to be an important determinant in Chinese men, probably because the amount of alcohol consumed was small. The relation between calcium intake and fracture risk in men is less clear. We noted a positive relation between calcium intake and total hip BMD in the univariate analysis but not in the multivariate analysis. It was observed that only subjects with very low calcium intake had lower hip BMD, whereas no difference in BMD was observed between those with moderate intake and those with high intake [32]. Low calcium intake is usually associated with low protein and energy intake, which may also contribute partly to the decrease in BMD. Although the serum albumin levels fell with age, our subjects were, on the whole, well nourished, with a mean serum albumin concentration of 43 g/l and a mean calcium intake of 652 mg/day. However, only 4% of the subjects had a daily calcium intake that reached 1,200 mg, as recommended by the National Academy of Science for US men [33].
Our study was limited in that, although the subjects were recruited from the community, they were derived from a convenient sample and not randomly recruited from the population. The number of subjects with osteoporotic fractures in this cohort is high, probably due to self-selection bias. However, the characteristics of the subjects were similar to those in most epidemiology studies performed in the same community, and we believe that the result of this study is applicable to the general population of this community.
In conclusion, this study demonstrated that aging, low body weight and body mass index, hypogonadism, smoking and physical inactivity were the major risk factors for low BMD. Strategies to prevent bone loss and osteoporosis in Asian men should include lifestyle modification and maintenance of hormone sufficiency.
References
Duan Y, Seeman E (2002) Bone fragility in Asian and Caucasian men. Ann Acad Med Singapore 31:1–13
Lau EMC (1997) Epidemiology of osteoporosis in urbanized Asian populations. Osteoporos Int 7 [Suppl 3]:S91–S95
Xu L, Lu A, Zhao X, Chen X, Cummings SR (1996) Very low rates of hip fracture in Beijing, People’s Republic of China—the Beijing osteoporosis projects. Am J Epidemiol 144:901–907
Koh LKH, Saw S-M, Lee JM, Leong K-H, Lee J (2001) Hip fracture incidence rates in Singapore 1991–1998. Osteoporos Int 12:311–318
Seeman E (1993) Osteoporosis in men: epidemiology, pathophysiology, and treatment possibilities. Am J Med 95:22S–28S
Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA (1999) Mortality after all major types of osteoporotic fracture: an observational study. Lancet 353:878–882
Jones G, Nguyen T, Sambrook PN, Gilbert C, Pocock NA, Eisman JA (1994) Symptomatic fracture incidence in elderly men and women: the Dubbo Osteoporosis Epidemiology Study (DOES). Osteoporos Int 4:277–282
Jackson SA, Tenenhouse A, Robertson L, and the CaMos study group (2000) Vertebral fracture definition from population-based data: preliminary results from the Canadian multicenter osteoporosis study (CaMos). Osteoporos Int 11:680–687
Burger H, van Daele PLA, Grashuis K, Hofman A, Grobbee DE, Schütte HE, Birkenhager JC, Pols HA (1997) Vertebral deformities and functional impairment in men and women. J Bone Miner Res 12:152–157
Cooper C, Campion G, Melton LJ III (1992) Hip fractures in the elderly: A worldwide projection. Osteoporos Int 2:285–289
Mei J, Yeung SSC, Kung AWC (2001) High dietary phytoestrogen intake is associated with higher bone mineral density in postmenopausal but not premenopausal women. J Clin Endocrinol Metab 86:5217–5221
Kung AWC, Tang GWK, Luk KDK, Chiu KW (1999) Evaluation of a new calcaneal quantitative ultrasound system and determination of normative ultrasound values in southern Chinese women. Osteoporos Int 9:312–317
Riggs BL, Khosla S, Melton LJ III (1998) A unitary model for involutional osteoporosis: estrogen deficiency causes both type I and type II osteoporosis in postmenopausal women and contributes to bone loss in aging men. J Bone Miner Res 13:763–773
Riggs BL, Khosla S, Melton LJ III (2002) Sex steroids and the construction and conservation of the adult skeleton. Endocr Rev 23:279–302
Szulc P, Munoz F, Claustrat B, Garnero P, Marchand F (2001) Bioavailable estradiol may be an important determinant of osteoporosis in men: the MINOS study. J Clin Endocrinol Metab 86:192–199
Slemenda CW, Longscope C, Zhou L, Hui SL, Peacock M, Johnston CC (1997) Sex steroids and bone mass in older men. J Clin Invest 100:1755–1759
Center JR, Nguyen TV, Sambrook PN and Eisman JA (1999) Hormonal and biochemical parameters in the determination of osteoporosis in elderly men. J Clin Endocrinol Metab 84:3626–3635
Amin S, Zhang Y, Sawin CT, Evans SR, Hannan MT, Kiel DP, Wilson PWF, Felson DT (2000) Association of hypogonadism and estradiol levels with bone mineral density in elderly men from the Framingham study. Ann Intern Med 133:951–963
Khosla S, Melton L, Atkinson EJ, O’Fallon WM, Klee GG, Riggs BL (1998) Relationship of serum sex steroid levels and bone turnover markers with bone mineral density in men and women: a key role for bioavailable estrogen. J Clin Endocrinol Metab 83:2266–2274
Van den BeldI AW, de Jong FH, Grobbee DE, Pols HAP, Lamberts SWJ (2000) Measures of bioavailable serum testosterone and estradiol and their relationships with muscle strength, bone density, and body composition in elderly men. J Clin Endocrinol Metab 85:3276–3282
Murphy S, Khaw K, Cassidy A, Compston JE (1993) Sex hormones and bone mineral density in elderly men. Bone Miner 20:133–140
Rudman D, Drinka PJ, Wilson CR, Mattson DE, Scherman F, Cuisinier MC, Schultz S (1994) Relations of endogenous anabolic hormones and physical activity to bone mineral density and lean body mass in elderly men. Clin Endocrinol (Oxf) 40:653–661
Greendale GA, Edelstein S, Barrett-Connor E (1997) Endogenous sex steroids and bone mineral density in older women and men: the Rancho Bernardo Study. J Bone Miner Res 12:1833–1843
Drinka PJ, Olson J, Bauwens S, Voeks SK, Carlson I, Wilson M (1993) Lack of association between free testosterone and bone density separate from age in elderly males. Calcif Tissue Int 52:67–69
Meier DE, Orwoll ES, Keenan EJ, Fagerstrom RM (1987) Marked decline in trabecular bone mineral content in healthy men with age: lack of association with sex steroid levels. J Am Geriatr Soc 35:189–197
Snyder PJ, Peachey H, Hannoush P, Berlin JA, Loh L, Holmes JH, Dlewati A, Staley J, Santanna J, Kapoor SC, Attie MF, Haddad JG Jr, Strom BL (1999) Effect of testosterone treatment on bone mineral density in men over 65 years of age. J Clin Endocrinol Metab 84:1966–1972
Feldman HA (2002) Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab 87:589–598
Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501
Heaney RP (2003) Long-latency deficiency disease: insights from calcium and vitamin D. Am J Clin Nutr 78:912–919
Wu J, Wang XX, Higuchi M, Yamada K, Ishimi Y (2004) High bone mass gained by exercise in growing male mice is increased by subsequent reduced exercise. J Appl Physiol 97:806–810
Lunt M, Masaryk P, Scheidt-Nave C, Nijs J, Poor G, Pols H, Falch JA, Hammermister G, Reid DM, Benevolenskaya L, Weber K, Cannata J, O’Neill TW, Felsenberg D, Silman AJ, Reeve J (2001) The effects of lifestyle, dietary dairy intake and diabetes on bone density and vertebral deformity prevalence: the EVOS study. Osteoporos Int 12:688–698
Huuskonen J, Vaisanen SB, Kroger H, Jurvelin C, Bouchard C, Alhava E, Rauramaa R (2000) Determinants of bone mineral density in middle aged men: a population-based study. Osteoporos Int 11:702–708
Institute of Medicine (1997) Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, and fluoride. National Academy of Sciences, National Academy Press, Washington, DC, USA, pp 107–110
Acknowledgement
We thank Ego Seeman for helpful comments on the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cheung, E.Y.N., Ho, A.Y.Y., Lam, K.F. et al. Determinants of bone mineral density in Chinese men. Osteoporos Int 16, 1481–1486 (2005). https://doi.org/10.1007/s00198-005-2000-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-005-2000-7