
Abstract
The burden of osteoporotic fractures in older men is significant. The objectives of our study were to: (1) characterize older men with fractures associated with osteoporosis, (2) determine if medication treatment rates for osteoporosis are improving and (3) identify patient, healthcare benefit and utilization, and clinician characteristics that are significantly associated with treatment. This retrospective cohort study assessed 1,171 men aged 65 or older with any new fracture associated with osteoporosis between 1 January 1998 and 30 June 2001 in a non-profit health maintenance organization in the United States. Multiple logistic regression was used to evaluate pre-fracture factors for their association with osteoporosis treatment in the 6-month post-fracture period. The main outcome measure was pharmacologic treatment for osteoporosis in the 6 months after the index fracture. Subjects’ average age was 76.7 years; 3.3% had a diagnosis of osteoporosis and 15.2% a diagnosis or medication associated with secondary osteoporosis. Only 7.1% of the study population and 16.0% of those with a hip or vertebral fracture received a medication for osteoporosis following the index fracture, and treatment rates did not improve over time. In the multivariate model, factors significantly associated with drug treatment were a higher value on the Charlson Comorbidity Index (odds ratio 1.26, 95% confidence interval 1.05–1.51), having an osteoporosis diagnosis (odds ratio 8.11, 95% confidence interval 3.08–21.3), chronic glucocorticoid use (odds ratio 5.37, 95% confidence interval 2.37–12.2) and a vertebral fracture (odds ratio 16.6, 95% confidence interval 7.8–31.4). Bone mineral density measurement was rare ( n =13, 1.1%). Our findings suggest that there is under-ascertainment and under-treatment of osteoporosis and modifiable secondary causes in older men with fractures. Information systems merging diagnostic and treatment information can help delineate gaps in patient management. Interventions showing promise in other conditions should be evaluated to improve care for osteoporosis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although osteoporosis is often considered a “woman’s disease,” the risk and burden of osteoporotic fractures in older men are substantial, and the consequences of a hip fracture may be more severe for a man than a woman [1, 2]. The lifetime risk of any clinical osteoporotic fracture of the hip, wrist or vertebra in white men is 13%, compared to 40% in women [3, 4, 5], and 30% of hip fractures occur in men [6]. Men and women who have sustained a hip fracture are 3–5 times more likely to die in the 12 months after the fracture than those who have not had a fracture [7]. Men have a 70–100% higher mortality rate than women after hip fracture [2, 8, 9]. Osteoporotic fractures, particularly those of the hip, result in significant disability, medical care costs and reduction in quality of life [3, 10]. The numbers of hip fractures are projected to quadruple by 2050, and the effects of osteoporosis will become an increasing human and healthcare system burden [1].
Expert consensus for the evaluation and treatment of osteoporosis in men after a hip fracture includes an evaluation for secondary causes of osteoporosis, bone mineral density (BMD) measurement, calcium and vitamin D supplementation, and a bisphosphonate medication [11]. Although there are effective and approved treatments for osteoporosis in men, the condition is rarely recognized and treated, even after a fracture has occurred [9, 12]. We found that in men aged 65–89 who had sustained a study fracture (any except skull, facial, finger, toe or ankle) during 1998–1999, only 1% received a BMD measurement and 3% a pharmacologic treatment for osteoporosis during the 2 years [12]. We were unable to identify other papers specific to men describing the patient characteristics relevant to risk and treatment, treatment trends and factors associated with treatment across a broad range of fracture types.
We undertook the current study to characterize older men with any fracture associated with osteoporosis and to determine if the pharmacologic treatment of osteoporosis in men after a fracture has improved since the publication of information on the consensus of experts [11], and the availability and FDA approval of effective treatment. We also sought to determine the patient, healthcare benefit and utilization, and clinician characteristics that are significantly associated with treatment. The results should help to inform future interventions.
Materials and methods
Selected details of the study methods have been described previously [13].
Research setting
The study site was a not-for-profit HMO with about 440,000 members in the Northwestern United States. The HMO’s clinical electronic databases capture close to 100% of all medical care and pharmacy services received by members. The electronic medical record contains clinician-entered ICD-9-CM-coded diagnoses and problem list. These databases are linked through the unique health record number that each member receives at the time of his or her first enrollment in the health plan.
Clinicians have access to the HMO’s intranet-based clinical guidelines for osteoporosis, which are consistent with prevailing national guidelines and began to include post-fracture management of osteoporosis in men in January of 2001. Clinicians’ use of national guidelines available on the Internet is voluntary [14, 15, 16, 17, 18, 19].
Study subjects
The study was approved by the HMO’s Institutional Review Board; members provide consent for use of their records for research purposes. Study participants were male members of the HMO who had a new study-defined ICD-9-CM fracture diagnosis and were aged 65 or older at the time of the fracture ( n =1, 526).
“Study-defined” fractures included any closed fracture except skull, facial, finger, toe or ankle that was coded as a diagnosis during a clinical encounter. We did not include open fractures (suggestive of high force). The study-defined fractures have been associated with decreased bone mass [20].
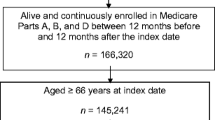
We defined the index date as the date of the clinical encounter during which the fracture was diagnosed. We included only those men who had minimum HMO eligibility for 12 months before and 6 months after the index date ( n =1, 195). This included the exclusion of 203 men who died within 6 months after the index fracture. We excluded those who did not have a pharmacy benefit at the time of the index fracture, resulting in a final study population of 1,171 men.
Analysis variables
We grouped index fractures according to site—hip, vertebra, wrist, humerus, pelvis, other upper extremity (radius, ulna, carpals and metacarpals), other lower extremity (femur, patella, tibia, fibula, tarsals and metatarsals) and other torso (rib or clavicle). For each study subject, we identified an 18-month observation window, beginning 12 months prior to and ending 6 months following the index date. We used a 12-month pre-fracture period to assess medication use and other healthcare utilization, and the 6-month post-fracture period to assess patient management in response to the fracture. We also used at least the 12-month pre-fracture period (all available data from 1 January 1997 through the index fracture) to assess for clinical conditions associated with osteoporosis, fracture risk and the presence of other chronic conditions. We limited our post-fracture evaluation window to 6 months because we were interested in practice patterns in response to a fracture. After about 6 months, other triggers for treatment could intervene, such as additional fractures and visible kyphosis.
We defined use of pharmacologic agents for the treatment of primary osteoporosis as a dispensed prescription for oral bisphosphonates or calcitonin. We did not include treatment of secondary osteoporosis, such as testosterone for hypogonadism. We defined existing treatment as a dispensed prescription for any of these drugs prior to the patient’s index date. New treatment, the primary outcome for analysis, was defined as a dispensed prescription that occurred in the post-fracture period without a dispensed prescription in the pre-fracture period.
BMD measurements were performed by an outside contractor that provided rapid patient access to axial dual X-ray absorptiometry (DXA) and electronic results. We recorded any BMD measurement during the 18-month observation period. BMD is not typically measured frequently; a BMD measurement frequency of 1–2 years is recommended by prevailing clinical guidelines [21].
Pre-fracture comorbidities were identified by searching visit diagnoses and problem list notations in the ambulatory medical record from 1 January 1997, through the date of the index fracture. We were interested in whether or not patient disease burden was associated with treatment for osteoporosis. We included common co-morbidities (diabetes, heart disease, hypertension, hyperlipidemia, malignant neoplasms, COPD/asthma, arthropathies, osteoarthritis and depressive disorders). We used the identified comorbidities to calculate the Charlson Comorbidity Index [22] as adapted for use with ICD-9-CM administrative databases [23].
We were also interested in whether or not patient risk factors for osteoporotic fracture were associated with treatment. To this end, we calculated age on the date of the index fracture and averaged body weight over the entire observation period. We also identified specific diagnoses associated with secondary osteoporosis (hyperthyroidism, hyperparathyroidism, Cushing’s syndrome, vitamin D deficiency, cirrhosis, chronic renal failure, malabsorption, malnutrition, testicular hypofunction and hypogonadism) and conditions associated with risk of fracture due to falls (Parkinson’s disease, rheumatoid arthritis, osteoarthritis, Alzheimer’s, senility and subacute delirium, alcoholism and type 1 diabetes). We examined use of medications prior to the index fracture that are related to the development of osteoporosis. Anti-convulsant drug use, associated with osteomalacia [24], was defined as any single dispensed prescription for phenobarbital, phenytoin or carbamazepine. In accordance with accepted guidelines [18], chronic glucocorticoid use was defined as usage in excess of 5 mg of prednisone or its equivalent per day for more than 90 days prior to the index fracture. We also examined medications related to increased risk of falls and fractures, including long-acting benzodiazepines (chlordiazepoxide, diazepam, flurazepam, triazolam) and tertiary tricyclic antidepressants (amitriptyline, imipramine, doxepin) [21] that were in use at the time of the index fracture. We considered a patient to be a user of these medications at the time of the index fracture if the date the prescription was dispensed plus the days of medication supplied included the index fracture date.
We also evaluated healthcare benefit, patient medical utilization and clinician characteristics for their potential association with receipt of an osteoporosis medication. We hypothesized that high out-of-pocket expenses for care could be associated with lack of treatment. We assessed healthcare benefit variables at the time of the index fracture, including the copayment level for office visits and for filled prescriptions dichotomized into high ($20 or more) and low. We assessed utilization variables in the 12-month pre-fracture period because we were interested in whether the type or frequency of interaction with the healthcare system was associated with treatment. We included whether or not the patient had an office visit for a routine examination; counts of visits to the patient’s personal primary care clinician; visits to any primary care clinician (internal medicine or family practice physicians, nurse practitioners or physician assistants); emergency room visits; hospital admissions; days spent in skilled nursing, intermediate or residential care facilities. We hypothesized that some types of clinicians might be more apt to treat than others. Clinician characteristics were assessed at the time of the index fracture and included the age and gender of the patient’s primary care clinician, whether that clinician was an MD or non-MD (nurse practitioner or physician assistant), the total number of patients on the clinician’s panel and the average number of monthly visits to the clinician.
Statistical methods
All analyses were performed using SAS version 6.12 (SAS Institute, Cary, N.C.). We conducted bivariate comparisons using Student’s t -test for continuous measures and Pearson’s chi-square tests for dichotomous or categorical variables. We used the Mantel-Haenszel chi-square to test trends across index years.
We evaluated 34 potential explanatory variables for their ability to predict receipt of a drug for the treatment of osteoporosis in the follow-up period, limiting the analysis to the 1,143 men who had not received an osteoporosis drug prior to their index fracture. The variables tested included patient clinical characteristics, patient utilization and health benefit variables, primary care clinician characteristics and three interaction terms (age with osteoporosis diagnosis, age with number of ambulatory visits and osteoporosis diagnosis with chronic steroid use). Using the backward selection stepwise option and a 0.05 P -value criterion, we reduced these 34 possible predictor variables to the four-variable model presented here (results for the 30 nonsignificant variables are shown in the Appendix).
Results
Table 1 shows that the mean age of study subjects was 76.7±7.6 years, and body weight was 179±34 pounds. BMD measurement was rare ( n =13, 1.1%). There were 39 patients (3.3%) with a diagnosis of osteoporosis, 178 patients (15.2%) who had a diagnosis or were taking a medication associated with secondary osteoporosis and 484 patients (41.3%) with a diagnosis or medication associated with falls. The most common comorbidities were hypertension ( n =452, 38.6%), heart disease ( n =381, 32.5%), arthropathies ( n =374, 31.9%), and asthma/COPD ( n =327, 27.9%).
Pharmacologic treatment of osteoporosis was uncommon—only 83 (7.1%) of the study population received one or more dispensed prescriptions following the index fracture. Nearly a quarter of these patients were already being treated prior to the fracture, i.e., only 63 (5.4%) received new treatment. In the bivariate analyses, factors strongly associated with receiving a drug after fracture included having received pre-fracture treatment (24.1% vs. 0.7%, P <0.001), having had a BMD measurement (5% vs. 0.8%, P <0.001), lower body weight (164 vs. 180 pounds, P <0.001), having received an osteoporosis diagnosis (28% vs. 1.5%, P <0.001), and chronic glucocorticoid use (24% vs. 3.9%, P <0.001). Men receiving a drug were also older (78.7 vs. 76.6 years, P =0.013) and less healthy, as evidenced by a higher score on the Charlson Comorbidity Index (1.8 vs. 1.3, P =0.005). Patients in the treated group were more likely to have malignant neoplasms (36% vs. 22.6%, P =0.005) and asthma/COPD (40% vs. 27.0%, P =0.013) than those who were not treated.
Table 2 shows the number of fractures by fracture site and the proportion of subjects with each fracture type who received post-fracture osteoporosis medication, BMD measurement and a pre-fracture diagnosis of osteoporosis, secondary osteoporosis or falls risk. The most common type of fracture was other torso (rib or clavicle) with 310 (26.5%), followed by vertebral ( n =204, 17.4%), hip ( n =203, 17.3%) and other lower extremity ( n =200, 17.1%). Although only 7.1% of all subjects received an osteoporosis medication following their fracture, 29.4% ( n =60) of the 204 subjects who had a vertebral fracture received post-fracture treatment. Only 5 of 203 (2.5%) of the men who had a hip fracture received an osteoporosis medication following their fracture. As noted, BMD measurement was rare overall and remained rare for all fracture types. Fractures most frequently associated with an osteoporosis diagnosis were vertebral fractures (11.8%), and those most frequently associated with a diagnosis increasing the risk for secondary osteoporosis or a diagnosis increasing the risk of falls were hip fractures (12.3% and 56.2%, respectively).
We also compared the distribution of fractures in those who did and did not receive an osteoporosis medication and/or a BMD measurement. Most (72.3%) of the 83 subjects who received a drug had vertebral fractures. Of the 13 subjects who had a BMD measurement, 6 (46.2%) had vertebral fractures, 3 (23.1%) had hip fractures, 2 (15.4%) had other torso fractures, and one each (7.7%) had a wrist fracture or other lower extremity fracture. Four (30.8%) had osteoporosis and 8 (61.5%) had osteopenia at any site, while only 1 (7.7%) had normal bone mass. In univariate comparisons, patients who had not received a post-fracture osteoporosis medication were significantly more likely than those who did have such treatment to have had fractures of hip (18.2% vs. 6.0%; P <0.001), other upper extremity (9.9% vs.1.2%; P <0.05), other lower extremity (18.2% vs. 2.4%; P <0.001) or other torso (27.6% vs. 12.1%; P <0.001). Patients who had received an osteoporosis medication or a BMD measurement were more likely than those who had not (72.3% vs. 13.2%; P <0.001 and 46.2% vs. 17.1%; P <0.05) to have had a vertebral fracture.
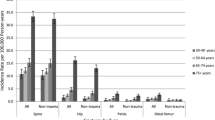
Figure 1 displays the proportion of study subjects who received a BMD measurement and who received new or ongoing pharmacotherapy for osteoporosis by year of index fracture. Although these proportions were relatively stable (the test for trend was not significant), new drug treatment appeared greater in 2001 than in prior years. New drug treatment in men with a hip or vertebral fracture (not displayed) also appeared to improve from 12.7% in 1998 to 18.6% in 2001, although this was also not significant. Figure 2 shows post-fracture pharmacologic treatment by type of treatment, by index year. Calcitonin was the osteoporosis treatment of choice in 1998 and 1999, but bisphosphonates became more common in 2000, and significantly ( P =0.018) more common in 2001.

Post-fracture treatment, by year of index fracture

Post-fracture pharmacological treatment by year of index fracture
Table 3 displays the results of the multivariate logistic regression model predicting new osteoporosis medication use after the index fracture. Of the 34 variables tested in the stepwise fashion, only 4 provided statistically significant predictive value: a higher value on the Charlson Comorbidity Index (OR 1.26, 95% CI 1.05–1.51), an osteoporosis diagnosis (OR 8.11, 95% CI 3.08–21.3), chronic glucocorticoid use (OR 5.37, 95% CI 2.37–12.2) and a vertebral fracture (OR 16.6, 95% CI 7.8–31.4). Individual co-morbidities, those associated with secondary osteoporosis or falls, measures of utilization and healthcare benefit and clinician characteristics did not provide significant predictive value for new osteoporosis medication use.
Discussion
We evaluated patient characteristics and trends in osteoporosis treatment after a fracture in men aged 65 and older. We found very little treatment. Only 7.1% received a medication for osteoporosis anytime in the 18-month window surrounding an index fracture, and only 5.4% received new treatment after an index fracture. Only 1.1% received a BMD measurement in the 18-month window. The trend in pharmacologic treatment over the 3.5 years of index fractures was in a positive direction, but did not significantly improve despite the promulgation of internal guidelines, the availability of effective treatment and the publication of expert consensus treatment recommendations [11]. In fact, we found that even in the fractures that have been most often associated with osteoporosis (hip and vertebral fracture) treatment rates in men were low and did not improve.
Our findings are not dissimilar to another recent evaluation of hip fractures in men [9]. That study found that only 2.7% of 110 men aged 50 and older with hip fracture had had antiresorptive treatment for osteoporosis at hospital discharge. One to five years after the fracture, 9.1% of the men were on treatment. Findings in four other studies of the management of hip fracture and in one of wrist fracture that included men (but did not report results separately for men) also revealed low rates of osteoporosis treatment [11, 25, 26, 27, 28].
Many of our study patients who received a medication (60/83) and almost half (46%) of the patients who received a BMD measurement had a vertebral fracture. Nonetheless, almost 70% of our study patients with a vertebral fracture were untreated. Factors that increased the likelihood of treatment were an increased burden of illness, a prior diagnosis of osteoporosis, vertebral fractures and chronic use of glucocorticoid medications. Interestingly, fracture types other than vertebral were not positively associated with treatment. In fact, those who were treated were less likely to have had a hip fracture (rather than another fracture type) than those who were not treated. Also of interest are the factors that were not significantly associated with treatment: other risk factors for osteoporotic fracture, level of out-of-pocket expenses for care, measures of health care utilization and primary care clinician characteristics.
The causes of the low rates of treatment and potential interventions should be the topic of urgent further research, because treatment significantly reduces future fractures and associated morbidity [2, 8, 9, 29, 30 ]. Although men lose bone mass and suffer osteoporotic fractures at an older age than women [1, 31], once a wrist, hip or vertebral fracture has occurred, osteoporosis is nearly as likely in a man as in a woman [6, 32, 33]. Reduced BMD is a significant risk factor for other fractures in men as well [34, 35]. Although the data in men associating some fractures with low BMD are more limited, most prior fractures increase the risk of future fractures in men and in women [36]. We conclude that BMD measurement, with follow-up treatment as indicated, should be considered across a broad range of fractures in older men.
The clinical characteristics of older men with fractures also assist in defining possible useful future interventions. About 15% of the post-fracture patients in our study had a diagnosis or were taking a medication associated with secondary osteoporosis, and about 41% had a diagnosis increasing the risk of falls. Our findings likely represent under-ascertainment and/or under-documentation of conditions that increase the patient’s risk of fracture. For example, 30–60% of men evaluated for vertebral fracture have been found to have secondary causes for osteoporosis [37]. Tuck et al. [6] found that 51% of men aged 40–80 with distal forearm fracture had identified causes of secondary osteoporosis. Poor et al. [8] retrospectively evaluated the medical records of 232 men who had hip fractures, and although there were some differences in the conditions they and we evaluated, they found a higher prevalence of risk factors for secondary osteoporosis and for falls. Poor et al. also found that these factors appeared to account for 72% of the hip fractures in men. Many of these risk factors are recognizable, and some are modifiable and should be treated when possible to reduce fracture risk.
Preventing osteoporotic fractures can be achieved through several strategies. Alendronate received Food and Drug Administration (FDA) approval in the United States for the treatment of osteoporosis in men in October of 2000 [38]. Another bisphosphonate, risedronate, and calcitonin (considered a second line treatment with lower efficacy) [39, 40, 41] are approved treatments for women and receive off-label use in men. Alendronate reduced the risk of new vertebral fractures by about 45% and other clinical fractures by about 30% in post-menopausal women with osteoporosis [42, 43] and has been demonstrated to increase bone mass and prevent vertebral fractures in men with osteoporosis [38].
Other effective treatments include injections of human parathyroid hormone (1–34) [44], which produced a marked effect on bone mineral density in men [46], and calcium and vitamin D supplementation [46, 47]. It is likely that multiple reasons explain the low rates of BMD measurement and treatment we found. In our HMO, BMD measurement requires a referral outside of the plan, and this requirement might be perceived as discouraging use of this contracted service. However, we do not believe this is a major factor. The contract encourages ease of access and viewing of results, and the health plan’s internal guidelines encourage BMD measurement in older post-fracture patients. Since much of the societal focus in osteoporosis has been on women, male patients and their physicians may not understand the risk of osteoporosis and the future risk of fractures in men who already have sustained one [9]. Even if a fracture raises the suspicion of osteoporosis, male patients may avoid evaluation and treatment because of the stigma that may be associated with a “woman’s disease.” There is evidence that many clinicians are uncomfortable with the diagnosis and treatment of osteoporosis [12, 18, 48, 49].
Although there is a known effective osteoporosis treatment in men, the evidence base regarding the epidemiology of osteoporosis and outcomes of treatment in men is weaker than in women. For example, although clinical guidelines are in place for post-menopausal osteoporosis, only expert consensus guides treatment in men [11]. FDA approval of treatment for men is more recent than that for women, and full diffusion of the treatment into common practice has not occurred.
Our study has several limitations. First, it includes patients from a single HMO and may not reflect patterns of patient management in other geographic areas, especially in other nations. However, the demographics of the HMO’s membership are representative of the insured population in this metropolitan area. For those patients who were hospitalized, the findings also include the post-fracture practices at seven area hospitals. Although the findings may reflect treatment patterns only in this area, the similarities to the findings reported elsewhere suggest that the gaps found here in the management of osteoporosis in men after a fracture are widespread.
Second, the diagnostic data are entered into the electronic medical record as a visit or problem list diagnosis by treating clinicians. These diagnoses could be either under- or over-documented and were not evaluated through review of the medical record text. However, to the extent that documentation relates to recognition and follow-up of diagnoses increasing the risk of future fracture, the data are important.
Third, because this study evaluated existing electronic data, we did not have access to important lifestyle-related treatments, such as calcium and vitamin D intake and exercise. We also did not fully assess evaluation and management of secondary osteoporosis, such as through laboratory data and relevant follow-up treatments (e.g., hypogonadism). This should be the focus of further study. We conclude that even in men with the significant predictors of treatment, treatment was uncommon, so virtually all men with fractures do not receive the BMD measurement or treatment that they should. The disconnect between orthopedic acute treatment of a fracture and the need for preventive care to reduce the risk of re-fracture highlights the benefits of using information systems to merge diagnostic and treatment information and thus delineate gaps in patient management. Interventions could be directed toward the clinician and the patient and could include electronic or paper alerts and reminders, or educational strategies such as academic detailing, critical care pathways or clinical guidelines, or nurse- or pharmacist-based case management programs [50, 51, 52, 53]. Interventions should be applied to prevent this important cause of morbidity and mortality in men.
References
Cooper C, Campion G, Melton LJ III (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353:878–882
Ross PD (1996) Osteoporosis. Frequency, consequences, and risk factors. Arch Intern Med 156:1399–1411
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Lips P (1997) Epidemiology and predictors of fractures associated with osteoporosis. Am J Med 103:3S–8S
Tuck SP, Raj N, Summers GD (2002) Is distal forearm fracture in men due to osteoporosis? Osteoporos Int 13:630–636
Office of Technology Assessment (1994) Hip fracture outcomes in people age fifty and over: background paper. OTA-BP-H-120. US Congress, Office of Technology Assessment, Washington, DC
Poor G, Atkinson EJ, Lewallen DG, O’Fallon WM, Melton LJ III (1995) Age-related hip fractures in men: clinical spectrum and short-term outcomes. Osteoporos Int 5:419–426
Kiebzak GM, Beinart GA, Perser K, Ambrose CG, Siff SJ, Heggeness MH (2002) Undertreatment of osteoporosis in men with hip fracture. Arch Intern Med 162:2217–2222
Ray NF, Chan JK, Thamer M, Melton LJ III (1997) Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 12:24–35
Colon-Emeric C, Yballe L, Sloane R, Pieper CF, Lyles KW (2000) Expert physician recommendations and current practice patterns for evaluating and treating men with osteoporotic hip fracture. J Am Geriatr Soc 48:1261–1263
Feldstein AF, Elmer PJ, Orwoll E, Herson M, Hillier T (2003) Bone mineral density measurement and treatment for osteoporosis in older individuals with fractures: A gap in evidence-based practice guideline. Arch Intern Med 163:2165–2172
Feldstein AF, Nichols GA, Elmer PJ, Smith DH, Aickin M, Herson M (in press) Older women with fractures: patient characteristics and trends in bone mineral density measurement and treatment for osteoporosis. J Bone Joint Surg
Osteoporosis Task Force (1996) AACE (American Association of Clinical Endocrinologists) clinical practice guidelines for the prevention and treatment of postmenopausal osteoporosis. Endocr Pract 2:155-171
National Osteoporosis Foundation (2000) Physicians guide to prevention and treatment of osteoporosis. National Osteoporosis Foundation, Washington, DC
American College of Rheumatology Task Force on Osteoporosis Guidelines (1996) Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Rheum 39:1791–1801
Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D (1997) Guidelines for diagnosis and management of osteoporosis. The European Foundation for Osteoporosis and Bone Disease. Osteoporos Int 7:390–406
American College of Rheumatology Ad Hoc Committee on Glucocoritcoid-Induced Osteoporosis (2001) Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis: 2001 update. Arthritis Rheum 44:1496–1503
National Osteoporosis Foundation (1998) Osteoporosis: Review of the evidence for prevention, diagnosis, and treatment and cost-effectiveness analysis. Executive summary. Osteoporos Int [Suppl] 4:S3–S6
Seeley DG, Browner WS, Nevitt MC, Genant HK, Scott JC, Cummings SR (1991) Which fractures are associated with low appendicular bone mass in elderly women? The Study of Osteoporotic Fractures Research Group. Ann Intern Med 115:837–842
Tinetti ME, Speechley M, Ginter SF (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chron Dis 40:373–383
Deyo RA, Cherkin DC, Ciol MA (1992) Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 45:613–619
Favus MJ (ed) (1999) Primer on the metabolic bone diseases and disorders of mineral metabolism. Lippincott Williams and Wilkins, Philadelphia
Kamel HK, Hussain MS, Tariq S, Perry HM, Morley JE (2000) Failure to diagnose and treat osteoporosis in elderly patients hospitalized with hip fracture. Am J Med 109:326–328
Juby AG, Geus-Wenceslau CM (2002) Evaluation of osteoporosis treatment in seniors after hip fracture. Osteoporos Int 13:205–210
Broy S, Bohren A, Harrington T, Licata A, Shewman D (2000) Are physicians treating osteoporosis after hip fracture. 22nd Annual Meeting of the American Society for Bone and Mineral Research (ASBMR), 23–26 September 2000, AMSBMR, Toronto, Canada
Khan SA, de Geus C, Holroyd B, Russell AS (2001) Osteoporosis follow-up after wrist fractures following minor trauma. Arch Intern Med 161:1309–1312
Desai MM, Zhang P, Hennessy CH (1999) Surveillance for morbidity and mortality among older adults—United States, 1995–1996. MMWR CDC Surveill Summ 48:7–25
Forsen L, Sogaard AJ, Meyer HE, Edna T, Kopjar B (1999) Survival after hip fracture: short- and long-term excess mortality according to age and gender. Osteoporos Int 10:73–78
Melton LJ III, Crowson CS, O’Fallon WM (1999) Fracture incidence in Olmsted County, Minnesota: comparison of urban with rural rates and changes in urban rates over time. Osteoporos Int 9:29–37
Scane AC, Francis RM, Sutcliffe AM, Francis MJ, Rawlings DJ, Chapple CL (1999) Case-control study of the pathogenesis and sequelae of symptomatic vertebral fractures in men. Osteoporos Int 9:91–97
Pande I, O’Neill TW, Pritchard C, Scott DL, Woolf AD (2000) Bone mineral density, hip axis length and risk of hip fracture in men: results from the Cornwall Hip Fracture Study. Osteoporos Int 11:866–870
Nguyen TV, Eisman JA, Kelly PJ, Sambrook PN (1996) Risk factors for osteoporotic fractures in elderly men. Am J Epidemiol 144:255–263
Gardsell P, Johnell O, Nilsson BE (1990) The predictive value of forearm bone mineral content measurements in men. Bone 11:229–232
Klotzbuecher CM, Ross PD, Landsman PB, Abbott TA, III, Berger M (2000) Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15:721–739
Orwoll E, Klein RF (1996) Osteoporosis in men. In: Marcus R, Feldman D, Kelsey J (eds) Osteoporosis. Academic Press, San Diego, pp 745–784
Orwoll E, Ettinger M, Weiss S, Miller P, Kendler D, Graham J et al (2000) Alendronate for the treatment of osteoporosis in men. N Engl J Med 343:604–610
Ettinger B, Black DM, Mitlak BH, Knickerbocker RK, Nickelsen T, Genant HK et al (1999) Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA 282:637–645
Chesnut CH, III, Silverman S, Andriano K, Genant H, Gimona A, Harris S et al (2000) A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: the prevent recurrence of osteoporotic fractures study. PROOF Study Group. Am J Med 109:267–276
Gennari C, Agnusdei D, Camporeale A (1991) Use of calcitonin in the treatment of bone pain associated with osteoporosis. Calcif Tissue Int 49 [Suppl] 2:S9–13
Ensrud KE, Black DM, Palermo L, Bauer DC, Barrett-Connor E, Quandt SA et al (1997) Treatment with alendronate prevents fractures in women at highest risk: results from the Fracture Intervention Trial. Arch Intern Med 157:2617–2624
Cummings SR (1998) Prevention of hip fractures in older women: a population-based perspective. Osteoporos Int 8 [Suppl 1]:S8–12
Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY et al (2001) Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 344:1434–1441
Orwoll ES, Scheele WH, Paul S, Adami S, Syversen U, Diez-Perez A et al (2003) The effect of teriparatide [human parathyroid hormone (1–34)] therapy on bone density in men with osteoporosis. J Bone Miner Res 18:9–17
Dawson-Hughes B, Harris SS, Krall EA, Dallal GE (1997) Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older. N Engl J Med 337:670–676
Chapuy MC, Arlot ME, Duboeuf F, Brun J, Crouzet B, Arnaud S et al (1992) Vitamin D3 and calcium to prevent hip fractures in the elderly women. N Engl J Med 327:1637–1642
Ferguson KJ, Hoegh C, Johnson S (1989) Estrogen replacement therapy. A survey of women’s knowledge and attitudes. Arch Intern Med 149:133–136
Saadi H, Litaker D, Mills W, et al (1999) Practice variation in the diagnosis and treatment of osteoporosis: A case for more effective physician education in primary care. J Womens Health Gender-Based Med 8:767–771
Wagner EH, Austin BT, Von Korff M (1996) Organizing care for patients with chronic illness. Milbank Q 74:511–544
Shiffman RN, Liaw Y, Brandt CA, Corb GJ (1999) Computer-based guideline implementation systems: a systematic review of functionality and effectiveness. J Am Med Inform Assoc 6:104–114
Smith W (2000) Evidence of the effectiveness of techniques to change physician behavior. Chest 118:8S–17S
Costantini O, Huck K, Carlson MD, Boyd K, Buchter CM, Raiz P et al (2001) Impact of a guideline-based disease management team on outcomes of hospitalized patients with congestive heart failure. Arch Intern Med 161:177–182
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Non-significant variables tested in multivariate logistic regression predicting post-fracture osteoporosis drug treatment in subjects without pre-fracture treatment (Table 4).
Rights and permissions
About this article
Cite this article
Feldstein, A.C., Nichols, G., Orwoll, E. et al. The near absence of osteoporosis treatment in older men with fractures. Osteoporos Int 16, 953–962 (2005). https://doi.org/10.1007/s00198-005-1950-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-005-1950-0