
Abstract
Osteoporotic fracture is considered to result from reduced bone strength and to be related to decreased bone mass and impaired bone architecture. Quantitative ultrasound measurements (QUS) of bone, that may reflect certain architectural aspects of bone, have been shown to be associated with fracture, but it is not clear whether the association is independent of bone mineral density (BMD). This study was designed to examine the contributions of cortical QUS and BMD measurements to the prediction of fracture risk in postmenopausal Caucasian women. Speed of sound (SOS) at the distal radius, tibia, and phalanx (Sunlight Omnisense) and BMD at the lumbar spine and femoral neck (GE Lunar) were measured in 549 women, aged 63.2 ± 12.3 years (mean ± SD; range, 49–88 years), including 77 fracture cases. Lower SOS at the distal radius, tibia, and phalanx, which were correlated with each other, were associated with increased risk of fracture. Independent predictors of fracture risk (in multivariate analysis) were distal radius SOS (OR per SD = 1.8; 95% CI, 1.3–2.4), femoral neck BMD (OR per SD = 1.9; 95% CI, 1.4–2.4), and age (OR per 5 years = 1.2; 95% CI, 1.0–1.5). Approximately 30% of the women had distal radius SOS T-scores <−2.5; however, only 6.6% of women had both BMD and SOS T-scores <−2.5. Among the 77 fracture cases, only 14 (18.2%) had both BMD and QUS T-scores below −2.5. These data in postmenopausal women suggest that speed of sound at the distal radius was associated with fracture risk, independent of BMD and age. The combination of QUS and BMD measurements may improve the accuracy of identification of women who will sustain a fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Bone mineral density (BMD) is lower in fracture patients such that each standard deviation deficit of BMD is associated with a twofold increase in fracture risk [1, 2, 3]. Despite the strength of association, BMD alone does not reliably discriminate women with fracture from women without fracture [3]; presumably because it does not capture bone properties such as microarchitecture or tissue elasticity, which may contribute to the risk of fracture, or physical characteristics such as muscle strength and postural instability that relate to falls and fracture risk [2]. Quantitative ultrasonic measurements of bone (QUS), including broadband ultrasound attenuation (BUA) and speed of sound (SOS), have been suggested as measures of bone structure [4].
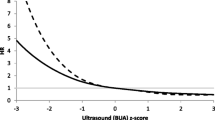
Cross-sectional studies have shown that patients with fractures either at the hip or lumbar spine had about 15% to 30% (or 0.5 standard deviation [SD]) lower BUA than nonfracture subjects [5, 6, 7]. Furthermore, longitudinal epidemiological studies have also shown that subjects with lower BUA at baseline have a higher risk of subsequent hip and vertebral fractures with each SD lower BUA associated with a doubling of hip fracture risk [8, 9].
While the strength of association between QUS and fracture risk is equivalent to that of BMD and fracture risk, it is not entirely clear whether QUS measurements can assess fracture risk independent of BMD. In the case of hip fracture, the combination of both QUS and BMD measurements appeared to improve the discrimination of fracture from nonfracture cases over the use of either measurement alone [8, 9]. However, in other fractures, the combination of BMD and calcaneal QUS measurements did not improve the predictive value compared with either measurement alone [10].
The present study was aimed at examining the association between QUS measurements and fracture risk, and assessing whether the association is independent of BMD in elderly women.
Study design and methods
Study design
Data used in this analysis were derived from the Dubbo Osteoporosis Epidemiology Study (DOES), ongoing since June 1989. The sampling frame for DOES is the city of Dubbo, New South Wales (Australia), a locality of approximately 32,000 people, 98.6% Caucasian, of whom 1,581 men and 2,095 women were aged 60 years or above in 1989. Dubbo’s relative isolation in terms of medical care allows virtually complete ascertainment of all fractures.
After obtaining written informed consent, participants were interviewed by a nurse coordinator who administered a structured questionnaire to collect data including age, anthropometric variables, and lifestyle and clinical data [11]. Bone mineral density (g/cm2) was measured in the lumbar spine and femoral neck by dual-energy X-ray absorptiometry using a Lunar DPX-L densitometer (GE Lunar, Madison, WI, USA). The coefficient of variation of BMD in our institution in normal subjects is 1–2% at the proximal femur and lumbar spine [12]. Speed of sound was measured in long bones at the outer layer surface such as distal radius, proximal phalanx, and tibia using a Omnisense ultrasound instrument (Sunlight Medical). Technical details of this technology have been described elsewhere [13]. The intrasubject coefficient of variation in SOS measurement in a random sample of 30 subjects was between 0.4% and 1%. The T- and Z-scores for both BMD and SOS were derived from the respective manufacturer’s reference ranges.
Symptomatic fractures during the study period were identified for residents of the Dubbo local government area through radiologists’ reports from the only two centers providing X-ray services, as previously described [2]. Fractures were only included if the report of fracture was definite and, on interview, had occurred with minimum or no trauma, including a fall from standing height or less. Fractures clearly due to major trauma, such as motor vehicle accidents or local pathology (e.g., cancer), were excluded from the analysis.
Statistical methods
Descriptive statistical techniques were used to test for the null hypothesis of equivalence between fracture and nonfracture groups. The linear logistic regression model was used to estimate the relative risk conferred by a risk factor (or the strength of association between a quantitative ultrasound measurement and fracture risk). Since there were several potential predictors of fracture risk, independent predictors were sought among the following: age, years postmenopause, and hormonal replacement therapy status (in women), height, weight, bone mineral density, and quantitative ultrasound measurements. Approximate Bayes factors, calculated through the Bayesian information criterion (BIC), were used to select final models [14]. The BIC has been shown to have better out-of-sample predictive properties compared with the usual “backward” and “forward” stepwise procedures. Interaction effects (i.e., testing the assumption of additivity of predictors) and nonlinear terms for the important continuous variables were also analyzed. To assess the discriminatory power of a logistic regression model, the concordance statistic c was calculated as the fraction of individuals with the fracture event among pairs of individuals where one has the fracture and one not, the individual with the highest prediction being classified as the one with the fracture. The c statistic, with values varying from 0.5 to 1, is identical to the area under under the receiver operating characteristic (ROC) curve. All statistical analyses were performed with SAS systems [15].
Results
Among the 549 women aged 65.2 ± 12.3 years (mean ± SD; range, 49–88 years), weight (66.6 ± 11.9 kg; mean ± SD), and height (161.4 ± 6.1 cm) were significantly correlated with SOS, with age and weight accounting for 14%, 20%, and 28% of the variances of SOS measurements at the tibia, distal radius, and phalanx, respectively (Table 1). All SOS measurements were normally distributed with the overall mean at the distal radius, tibia, and proximal phalanx being 4,002 ± 153 m/s, 3,869 ± 147 m/s, and 3,788 ± 210 m/s, respectively. SOS measurements at the tibia, distal radius, and phalanx were significantly correlated with each other, with the linear correlation coefficients being between 0.36 and 0.39 (p<0.001; Fig. 1). The correlation between femoral neck BMD and SOS measurements was lower (0.23 for distal radius, 0.30 for phalanx and tibia).

Matrix plot of intercorrelations among age, speed of sound at the distal radius (DR), tibia, phalanx, and femoral neck BMD (BMD). The diagonal bar graphs for each variable represent the distribution of that variable, with the x-axis showing values of the variable, and y-axis the number of subjects. The upper (or lower) off-diagonal graphs represent the correlation between any two variables
Among the 77 fracture cases, there were 12 hip, 10 vertebrae, 23 humerus, 10 distal radius, 5 wrist, 6 pelvis, 4 ankle, and 7 fractures at other sites such as ribs (4) or patella (3). SOS measurements in fracture cases were significantly lower than in nonfracture subjects (Table 2). Among the SOS measurements, lower distal radius SOS appeared to confer a greater risk of fracture compared with the reduction in tibia or phalanx SOS (Table 3).
In models without age factors and femoral neck BMD, the combination of SOS measurements at different sites significantly improved the fracture diagnostic value. For example, when SOS measurements at both distal radius and phalanx were considered in the logistic regression model, the c statistic was increased to 0.76; similarly, SOS measurements at both tibia and phalanx increased the c statistic to 0.73. However, the combination of distal radius and tibia SOS did not significantly improve the discrimination.
When SOS measurements were considered simultaneously with known fracture predictors such as age, weight, height, and bone mineral density, distal radius SOS was found to be a significant determinant of fracture risk (odds ratio = 1.8; 95% CI, 1.3–2.4), independent of femoral neck BMD and age (Table 4). When tibia or phalanx SOS was included in the model, the effects of age and femoral neck BMD were still significant, but the odds ratio associated with SOS was slightly lower: 1.5 (95% CI, 1.1–2.0) per 140 m/s tibia SOS, and 1.2 (95% CI, 1.0–1.5) per 210 m/s phalanx SOS.
Approximately 16% of women were classified as having “osteoporosis” by femoral neck BMD (T-scores <−2.5), and the relative risk of fracture associated with this criterion was 4.2 (95% CI, 2.5–7.2). The proportion of women with distal radius QUS T-scores <−2.5 was 31%, with a corresponding lower relative risk of fracture of 2.1 (95% CI, 1.3–3.5). Only 6.6% of women had both T-scores <−2.5, and the risk of fracture associated with this small group was increased by 4.5-fold (95% CI, 2.2–9.3) (Fig. 2).

Risk of fracture by category of femoral neck BMD and distal radius QUS. In each variable, a value of 1 indicates a T-score <−2.5 and a value of 0 indicates a T-score ≥−2.5. The number of subjects in each category is shown above each bar
It should be noted here also that using T-score <−2.5 as a diagnostic criterion, more women were classified as osteoporotic by SOS measurement at the distal radius (31%) than by measurement at the phalanx (23%) or tibia (6%).
Discussion
The current understanding of osteoporosis [15] is that it results from a deterioration of both the amount and structure of bone, such that BMD, a quantitative measure of bone strength, is predictive of osteoporotic fracture. Although BMD accounts for between 70% and 75% of the variance of bone strength (the ability to resist an applied load), it alone is not sufficient to accurately identify subjects who are prone to fracture. This suggests that the remaining variance may be due to other factors such as bone architecture and liability to falls [2, 16]. Recent research efforts have focused attention on the role of bone quality in osteoporosis, particularly quantitative ultrasound measurements, as this may give extra information only on bone architecture and elasticity [4, 17, 18]. In this study, QUS did indeed correlate with BMD, but also contributed independently to the prediction of fracture risk over and above of BMD’s contribution.
This finding is consistent with previous observations, in which fracture subjects were found to have significantly lower QUS than controls in retrospective studies [5, 6, 7] as well as in prospective studies [8, 9, 19, 20, 21]. However, the magnitude of association as observed in this study (with odds ratio per SD being less than 2) is lower than previously observed in prospective studies [8, 9] but is not significantly different from retrospective studies [5, 6, 7].
Among the three sites of measurements, speed of sound at the distal radius had the greatest discriminatory power (with the c statistic being 0.71) compared with measurements at the tibia and phalanx (0.67). However, the discrimination of SOS at the distal radius is poorer than measurement of BMD (with c=0.77), but in this sample the difference is not statistically significant.
The correlation between BMD and QUS measurements in this study was moderate (between 0.2 and 0.3), much lower than previously reported (between 0.5 and 0.6) [10]. The inconsistency is likely due to difference in site or types of bone being measured, and the types of QUS instrument. In various heel ultrasound instruments, the measurements at the heel include both cortical and trabecular bones, and this has been shown to be strongly correlated with BMD measurements at the same site [22]. In contrast, the Sunlight Omnisense focuses mainly on the cortical bone at the phalanx, distal radius, and tibia. Such a difference in bone sites and types of bone may explain the differential correlations between QUS and BMD by different technologies.
Does the combination of measurements of SOS at different sites improve the prediction of fracture risk? In this study, the combination of SOS measurements at the distal radius and phalanx, or at the tibia and phalanx (but not the combination of distal radius and tibia) improved the predictive value of fracture risk over SOS measurement at only one site. However, this additive and combined effect was only significant when the effects of age and femoral neck BMD were not considered.
It is unclear whether the combination of QUS and BMD measurements can improve the prediction of fracture, particularly hip fracture [9, 10]. In this study, the poor correlation between QUS (measured by Sunlight Omnisense) and BMD (measured by DXA) suggested that the prediction of fractures could be improved if the two measurements were combined, and this is indeed the case. In multivariate analysis, both BMD and QUS were statistically significant determinants of fracture, independent of age. However, even the combined measurements did not adequately discriminate between those with and without fractures. Although subjects with low values of BMD and QUS were the group at greatest risk having a fracture, there was only 6.6% of such subjects in the population. As a result, the number of fractures “explained” by the two measurements is modest. For example, among the 77 fracture cases, only 14 (or 18.2%) had both BMD and QUS T-scores below −2.5.
The modest strength of association between QUS and fracture risk as observed in this study is probably due to the fact that fracture cases were assessed retrospectively, not prospectively, although the interval between fracture and date of QUS measurement was in almost all (90%) cases, less than 5 years. Also, although our results are consistent with previous findings from prospective studies, the retrospective nature of this study makes a cause-and-effect inference difficult. The subjects of this study are of Caucasian background, whose data may not be generalizable to other populations. Despite these potential limitations, the study was based on a relatively large sample size and a homogeneous, unselected population; thus, differences could reliably be detected, which would not be possible with smaller studies.
In summary, these data in postmenopausal Caucasian women suggest that lower values of quantitative ultrasound measurement (speed of sound) are associated with increased risk of fracture, independent of BMD and age. As a result, a combination of QUS and BMD measurements may improve, albeit modestly, the accuracy of identification of women who will sustain a fracture.
References
Hui SL, Slemenda CW, Johnston CC Jr (1989) Baseline measurement of bone mass predicts fracture in white women. Ann Intern Med 111:355–361
Nguyen T, Sambrook P, Kelly P, Jones G, Lord S, Freund J, Eisman J (1993) Prediction of osteoporotic fractures by postural instability and bone density. BMJ 307:1111–1115
Marshall D, Johnell O, Wedel H (1996) Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 312:1254–1259
Kaufman JJ, Einhorn TA (1993) Ultrasound assessment of bone. J Bone Miner Res 8:517–525
Turner CH, Peacock M, Timmerman L, Neal JM, Johnston CC (1995) Calcaneal ultrasonic mneasurements discriminate hip fracture independent of bone mass. Osteoporos Int 5:130–135
Schott AM, Weill-Engerer S, Hans D, Duboeuf F, Delmas PD, Meunier PJ (1995) Ultrasound discriminates patients with hip fracture equally well as dual energy X-ray absorptiometry and independent of bone mineral density. J Bone Miner Res 10:243–249
Glüer CC, Cummings SR, Bauer DC, Stone K, Pressman A, Mathur A, Genant HK (1996) Osteoporosis: association of recent fractures with quantitative ultrasound findings. Radiology 199:725–732
Bauer DC, Gluer CC, Cauley JA et al (1997) Broadband ultrasound attenuation predicts fractures strongly and independently of densitometry in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 157:629–634
Hans D, Dargent MP, Schott AM et al (1996) Ultrasonographic heel measurements to predict hip fracture in elderly women: the EPIDOS prospective study. Lancet 348(9026):511–514
Frost ML, Blake GM, Fogelman I (2000) Does quantitative ultrasound enhance precision and discrimination? Osteoporos Int 11:425–433
Nguyen TV, Center JR, Eisman JA (2000) Osteoporosis in elderly men and women: effects of dietary calcium, physical activity and body mass index. J Bone Miner Res 15:322–331
Nguyen TV, Sambrook PN, Eisman JA (1997) Source of variability in bone density: implication for study design and analysis. J Bone Miner Res 12:124–135
Hans D, Srivastav SK, Singal C, Barkmann R, Njeh CF, Kantorovich E, Gluer CC, Genant HK (1999) Does combining the results from multiple bone sites measured by a new quantitative ultrasound device improve discrimination of hip fracture? J Bone Miner Res 14(4):644–651
Kass RE, Raftery AC (1995) Bayes factors. JASA 90:773–795
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359(9321):1929–1936
Kleerekoper M, Villaneuva AR, Stanciu J, Rao DS, Parfit AM (1985) The role of three dimensional trabecular microstructure in the pathogenesis of vertebral compression fracture. Calcif Tissue Int 37:594–597
Langton CM, Palmer SB, Porter RW (1984) The measurement of broadband ultrasonic attenuation in cancellous bone. Eng Med 13:89–91
Langton CM, Evans GP (1991) Dependence of ultrasonic velocity and attenuation on the material properties of cancellous bone. Osteoporos Int 1:194
Gregg EW, Kriska AM, Salamone LM, Roberts MM, Anderson SJ, Ferrell RE, Kuller LH, Cauley JA (1997) The epidemiology of quantitative ultrasound: a review of the relationships with bone mass, osteoporosis and fracture risk. Osteoporos Int 7:89–99
Pluijm SMF, Graafmans WC, Bouter LM, Lips P (1999) Ultrasound measurements for the prediction of osteoporotic fractures in elderly people. Osteoporos Int 9:550–556
Ross P, Huang C, Davis J, Imose K, Yates J, Vogel J, Wasnich R (1995) Predicting vertebral deformity using bone densitometry at various skeletal sites and calcaneus ultrasound. Bone 16:325–332
Graafmans WC, Van Lingen A, Ooms ME, Bezemer PD, Lips P (1996) Ultrasound measurements in the calcaneus: precision and its relation with bone mineral density of the heel, hip, and lumbar spine. Bone. 19:97–100
Acknowledgements
We gratefully acknowledge the expert assistance of Janet Watters and Donna Reeves in the interview, data collection, and bone densitometry; and the invaluable help of the staff of Dubbo Base Hospital. This work has been supported by the National Health and Medical Research Council of Australia. We also thank the generous support of Sunlight Ultrasound Technologies, the maker of the Omnisense ultrasound instrument, for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nguyen, T.V., Center, J.R. & Eisman, J.A. Bone mineral density-independent association of quantitative ultrasound measurements and fracture risk in women. Osteoporos Int 15, 942–947 (2004). https://doi.org/10.1007/s00198-004-1717-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-004-1717-z