
Abstract
Case-selection strategies have been advocated for identifying patients who would benefit from primary care to prevent osteoporosis. However, the effectiveness of this approach is unclear. To address this question, we performed a randomized control trial to determine whether a case-selection strategy to identify patients with clinical risk factors for osteoporosis, combined with open access to dual X-ray absorptometry (DXA) scans, influences bisphosphonate prescribing in ten GP practices in Avon. Practices were randomized to two groups: the first identified women aged 45–75 years at high risk of osteoporosis and provided open access to DXA scans for 12 months; the second had no case-finding strategy and no DXA scan access. Bisphosphonate prescribing was ascertained by searching computerized patient records every 3 months during the intervention and a subsequent 6-month follow-up period. Overall, the number of subjects in each practice who were prescribed bisphosphonates increased by 50% (p<0.001), and the proportion of bisphosphonates prescribed as aminobisphosphonates increased 3-fold (p<0.001). The magnitude of these changes was similar in both groups. However, of the patients prescribed bisphosphonates, approximately twice as many in group 1, as compared with group 2, had a previously documented low-trauma fracture, as assessed at the end of the 12-month intervention period (p=0.01). Furthermore, at study’s end, of the 30 patients in group 1 receiving bisphosphonates who had received DXA scans, 80% had osteoporosis as defined by t-score<-2.5. We conclude that use of a case-selection strategy for osteoporosis in primary care, combined with open access to DXA scans, appears to target bisphosphonate therapy to those at high risk of osteoporotic fractures. In contrast, the overall rate of bisphosphonate prescribing is unaffected by this intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Of the several effective treatments available for osteoporosis [1], bisphosphonates are the most widely prescribed class in the UK. In order to target these therapies to the most appropriate patient population, the National Osteoporosis Society (NOS), among others, proposes that primary-care based strategies for osteoporosis be developed to identify patients with specific clinical risk factors, such as previous fragility fracture concurrent treatment with oral glucocorticoids [2]. In addition, dual X-ray absorptometry (DXA) scans have been suggested to be cost-effective in assessing osteoporosis risk and the need for therapy [3]. These may be used in conjunction with case-finding strategies [2]. The NOS recommends offering specific treatment to those diagnosed with osteoporosis following a DXA scan (i.e., t≤−2.5) [2].
However, the use of case-finding strategies and access to DXA scans in primary care still varies widely within the UK. At our local center in Bristol, GPs essentially do not have access to DXA scans under the National Health Service (NHS). One barrier to wider implementation of case-finding strategies for osteoporosis and primary-care access to DXA scans is the uncertainty that surrounds the associated drug costs, which are difficult to estimate accurately. Moreover, although the effectiveness and cost-effectiveness of treatment to prevent osteoporotic fractures is understood [1, 4], this is not yet true for osteoporosis case-finding strategies.
To assess the effectiveness of current recommendations for the identification in primary care of patients at high risk of osteoporosis, we examined the impact of a case-finding strategy combined with direct-access DXA service on bisphosphonate prescribing. In our prospective trial, GP practices were randomized to receive a combined case-finding and direct-DXA-access service, or no active intervention. To ensure that our results would be generalizable, a “real life” case-finding strategy was utilized, in which individual GP practices were responsible for identifying patients for DXA referral within an agreed set of clinical criteria.
Materials and Methods
After the United Bristol Hospitals Trust ethical committee approved this study, 25 GP practices within Avon were invited to participate over a 12 month period. Ten agreed. To be suitable for inclusion, GP practices were required to have computerized case records amenable to searching as described below. A questionnaire about osteoporosis management was completed by the lead GP at each practice. To provide a basis for comparing socioeconomc factors between groups of practices, the Townsend material deprivation score was recorded. This index—a summation of standardized variables, collected in the UK national census, on unemployment, overcrowding and car and home ownership—reflects geographical variations in socioeconomc status [5].
Consent was acquired from individual GPs in the study, after which practices were randomized in pairs to groups 1 or 2. In group 1, participating practices identified patients at high risk of osteoporosis, by searching computerized case records for women 45–75 years of age with a history of fracture, concurrent treatment with prednisolone, or premature menopause (menopause before 45 years of age). After their GPs reviewed their case notes, these individuals were referred for DXA scanning, if indicated, over a 12-month period of open access. Referred patients received an information sheet, an appointment for a DXA scan, and a contact number to change this if required. In addition to subjects identified via this explicit approach, DXA scans were provided in group-1 practices for women aged 45–75 years and found by their GPs to have other risk factors for osteoporosis on an opportunistic basis (e.g., radiological osteopenia).
At their DXA-scan appointments, patients were asked whether they currently received treatment for osteoporosis. The referral indication was recorded. A DXA scan of the lumbar spine and right hip was performed using a Lunar DPX. The report was sent to the referring GP, indicating bone mineral density (BMD) based on WHO criteria—normal (t≥−1.0), osteopenic (t≤−1.0), or osteoporotic (t≤−2.5). In patients found to be osteoporotic, an explicit recommendation was made to commence bisphosphonate treatment [2]. All subjects identified under the study protocol in group 1 were asked to provide consent at the time of their DXA scan. In contrast, in group-2 practices, although basic information about osteoporosis was provided to GPs at an initial meeting to discuss participation in the study, no specific case-finding strategy was employed to identify high-risk patients for osteoporosis, and no open-access DXA scan service was made available.
All patients currently or previously prescribed etidronate, alendronate or risedronate were identified by searching GP computerized case records, using a combination of various drug names. These searches were carried out at baseline (within 1 week of randomization), and every 3 months over the 12 month period of intervention. Additional searches were carried out at 15 and 18 months following randomization, to detect possible delayed effects of the case-finding strategy on bisphosphonate prescribing, and at baseline, to assess use of other possible medications for osteoporosis, such as HRT and calcium and vitamin D supplements. However, change in use of these other therapies was not analyzed, because their prescription was not considered sufficiently specific to osteoporosis. Individual computerized case records were subsequently examined to define the prescribing period. Results were cross-checked against those obtained by asking group-1 patients about their medication, upon their DXA scans. Records were analyzed to identify patients—prescribed bisphosphonates at baseline and at the end of the intervention period at 12 months—who had a history of low-trauma vertebral or non-vertebral fracture, who were receiving treatment with glucocorticoids, or who had other risk factors for osteoporosis, such as a previous finding of radiological osteopenia.
The primary outcome of this study was a difference between groups 1 and 2 for the number of patients prescribed bisphosphonates. In view of the study’s cluster-randomization design, we calculated the number of patients prescribed bisphosphonates as follows. We divided the number of patients prescribed bisphosphonates in each practice by the total list size, then combined results from the five practices in each group to obtain a value for mean + SEM percentage of patients receiving bisphosphonates per practice. Secondary outcome variables consisted of the proportion of subjects treated with aminobisphosphonates in the two groups of practices, and the number of patients prescribed bisphosphonates following a history of low-trauma fracture or glucocorticoid therapy. To examine the basis for any differences in bisphosphonate use between practices in groups 1 and 2, we also investigated the indications for DXA referral in group-1 practices, and outcomes in terms of DXA result and bisphosphonate prescribing.
Repeated-measures analysis of variance was utilized to investigate possible differences, between the two groups, in the number of patients prescribed bisphosphonates over the study period. An unpaired Student’s t-test was used to compare baseline characteristics between groups, as well as the number of patients receiving bisphosphonates following a history of fracture or glucocorticoid therapy at 12 months. All statistical analyses were performed using Statview 5 (SAS Institute). A P value of 0.05 was taken as the cut-off for statistical significance.
Results
Practices in groups 1 and 2 were of comparable list size (Table 1). No practice enrolled in the study was operating an explicit case-finding strategy for osteoporosis, or had a direct-access DXA scan service available to them under the NHS. No significant differences were observed between practice groups with regard to bisphosphonate use at baseline, although a trend towards higher bisphosphonate prescribing was evident in group 1. An equivalent trend was also present with respect to hormone replacement therapy (mean percentage of patients per practice + SEM =4.8 + 0.9 for group 1 vs 2.9 + 0.3 for group 2, P=0.07) and calcium and vitamin D supplements (0.51 + 0.11 for group 1 vs 0.36 + 0.09 for group 2, P=0.3).
A small difference in Townsend score was observed, suggesting slightly greater socio-economic deprivation in group 1 (see Table 1). However, this is unlikely to have contributed to the tendency for greater bisphosphonate prescribing by these practices. The proportion of women aged 45–75 was slightly higher in group 1 (mean percentage of patients per practice + SEM = 15.9 + 3.5 for group 1 vs 13.1 + 3.5 for group 2, P=0.2). However, this did not appear to account for the trend towards higher bisphosphonate prescribing in group 1 compared with group 2, since a similar trend was observed when adjusting for these differences by expressing the rate of bisphosphonate prescribing as the percentage of women aged 45–75 years per practice (mean percentage + SEM = 1.7 + 0.2 for group 1 vs 1.2 + 0.3 for group 2, P=0.2).
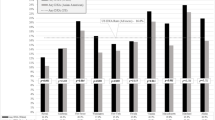
The total number of patients prescribed bisphosphonates per practice was subsequently compared between groups 1 and 2 at each time point. We found that overall use of bisphosphonates increased approximately 50% over the 18-month follow-up period, to a similar extent in both groups (Fig. 1A). Equivalent results were obtained expressing results as the percentage of women aged 45–75 years per practice (results not shown). Although the extent of aminobisphosphonate prescribing increased significantly, the magnitude of this rise was similar in both groups of practices (Fig. 1B).

Bisphosphonate prescribing a Results show mean + SEM percentage of patients prescribed bisphosphonates during study and a 6-month follow-up period. Value was obtained by dividing the number of patients prescribed bisphosphonates in each practice by total list size, then combining results from the five practices in each group. Repeated-measures ANOVA showed a significant time effect on bisphosphonate use, regardless of practice group (p<0.001) b results show mean + SEM proportion of bisphosphonates prescribed as aminobisphosphonates during the study and a 6-month follow-up period. In each practice, the number of patients prescribed alendronate or risedronate was divided by the number prescribed alendronate, risedronate or etidronate. Results were then combined from the five practices in each group. Repeated-measures ANOVA showed a significant time effect on aminobisphosphonate use, regardless of practice group (p<0.001). White squares = group 1 (DXA); black triangles = group 2 (non-DXA)
Prior to the study, the most common indications for bisphosphonate prescribing, as ascertained by analysis of computerized records of patients prescribed bisphosphonates at baseline, were previous vertebral fracture (24%), previous non-vertebral fracture (20%), concurrent steroid therapy (18%) and radiological osteopenia (10%). Based on pooled results of patients with previous vertebral and non-vertebral fractures, the number of patients per practice prescribed bisphosphonates who had a history of low-trauma fracture was significantly higher in group 1 at 12 months, compared with that in group 2 at 12 months and group 1 at baseline (Fig. 2). Similarly, the number of patients with a history of low-trauma fracture who were first prescribed bisphosphonates during the study, as reflected by patients prescribed bisphosphonates at 12 months but not baseline, was significantly higher in group 1 compared with group 2 (0.077 + 0.012% vs 0.025 + 0.011%, p=0.01 by unpaired Student’s t-test). Conversely, no significant differences were observed in the number of patients prescribed bisphosphonates who were receiving glucocorticoids (0.066% + 0.016% for group 1 vs 0.052% + 0.029% for group 2 , 12 months).

Bisphosphonate prescribing in patients with previous fractures. Results show mean + SEM percentage of patients with previous low-trauma fracture prescribed bisphosphonates, as assessed at baseline and 12 months. In each practice, the number of patients prescribed bisphosphonates who had a history of low-trauma vertebral or non-vertebral fracture was divided by the total list size. Results were then combined from the five practices in each group. White squares = group 1 (DXA); black triangles = group 2 (non-DXA). P=0.01 vs group 2 at 12 months (unpaired Student’s t-test) and P=0.03 vs group 1 at baseline (paired Student’s t-test).
A total of 185 patients were referred for DXA scans from practices in group 1 over the 12-month study period, of whom 157 attended. Although history of non-vertebral fracture, glucocorticoid therapy and premature menopause were the most common clinical indications, the referral pattern differed considerably among practices (Table 2). Osteoporosis was observed most commonly in patients with previous non-vertebral fracture (Table 3). Of patients receiving DXA scans in group-1 practices, 30 (19%) were prescribed bisphosphonates as assessed at 12 months, of whom 24 (80%) had osteoporosis diagnosed by DXA.
Discussion
To our knowledge, this investigation represents the first randomized controlled trial to examine the effect of a case-selection strategy combined with open access to DXA scans on bisphosphonate prescribing in primary care. Interestingly, we found that this intervention led to a significant increase in patients who were treated with bisphosphonates and who had a previously documented low-trauma fracture. Bisphosphonate prescribing increased overall, but at a similar rate to that observed in group 2, which did not have access to DXA scans. Our finding of a selective increase of bisphosphonate therapy in group-1 patients with a history of fracture likely reflects the fact that DXA detected osteoporosis in a higher proportion of patients with previous fracture than it did in patients referred for other indications, such as steroid therapy or premature menopause.
Our findings are consistent with previous observations that, in the absence of a specific case-finding strategy, only a small proportion of patients are prescribed bisphosphonates by their GPs following a fracture [6]. In light of evidence that a history of vertebral or non-vertebral fracture is associated with increased risk of future fracture [7, 8], our results suggest that a case-selection strategy results in bisphosphonates being targeted to patients at high risk of osteoporotic fracture. In addition, availability of open-access DXA scans probably targeted treatment to patients at increased risk of osteoporosis as a consequence of a low BMD, since 80% of those in group 1 receiving DXA scans and subsequently prescribed bisphosphonates had been found to have osteoporosis, as defined by t-score≤−2.5.
Since our intervention was applied in a “real life” setting in which individual practices and GPs were responsible for case selection and DXA referral, our results are likely to be generalizable to other GP practices in the UK. Contrary to the present findings that DXA scan access has no overall impact on bisphosphonate prescribing, in a previous observational study in Ottawa, inviting patients for DXA scans in a tertiary center led to a net increase in osteoporosis drug therapy [9]. This discrepancy may reflect a difference in prescribing behavior between the UK and Canada. However, our results also illustrate the importance of randomized controlled trials for assessing the impact of DXA scan access on drug prescribing for osteoporosis, since similar increases were observed in both control and intervention groups. Any increase in use of bisphosphonates in the control group likely reflects general trends in bisphosphonate prescribing within the UK over the study period, and/or the effects of raising awareness of osteoporosis and its treatment in participating GP practices.
A potential limitation is that no information was collected on the number of DXA scans performed at each of the GP practices before our study began. Although no direct access service was available to these practices via our unit, we are unable to exclude the possibility that a small number of scans were performed via other referral routes. In addition, there was a lack of precise matching between practice groups in baseline levels of bisphosphonate prescribing. This likely reflects the limited number of GP practices enrolled into the study and the relatively wide variation among them in terms of bisphosphonate use. Although this study’s drug-prescribing data were based on computerized records, underestimation of bisphosphonate use with this method is unlikely to explain the lack of difference in bisphosphonate prescribing between groups, since in the subgroup of group-1 patients who got DXA scans, no patient was found to be receiving bisphosphonates who had not previously been identified by searching computerized prescribing records.
Based on the variability that we found in bisphosphonate use among practices, our study had an 80% power to detect a 0.14% increase in bisphosphonate use in group 1 compared with group 2, at the P=0.05 significance level [10]. Since 0.22% of patients were prescribed bisphosphonates in group 2 practices at the end of the 12-month intervention period, this increase represents a 64% consequent rise in bisphosphonate use relative to the control group. There are several possible explanations as to why our intervention did not increase bisphosphonate prescribing by this magnitude. For example, a significant minority of patients were referred for DXA scans due to risk factors found to be associated with a relatively low prevalence of osteoporosis, such as premature menopause.
In addition, the case-finding strategies of group-1 practices may have had limited success in identifying patients with stronger risk factors for osteoporosis. For example, only 0.8% of women aged 45–75 in these practices were referred for DXA scans on the basis of concurrent steroid therapy. In contrast, in a recent report, 3.2% of women over 50 were found to be taking steroids in primary care in Shropshire, UK [11]. Although the present study did not routinely collect data on the proportion of patients receiving steroid therapy, this information was available in practices 2 and 3, in which 3.9% of women aged 45–75 took steroids. Taken together, these observations suggest that only a minority of women aged 45–75 who were receiving steroids in group-1 practices were referred for bone densitometry. This may in part reflect the fact that a significant proportion of steroid users identified from prescribing records were not receiving steroids at sufficient dose or duration to be considered at significant risk of osteoporosis.
The number of patients referred for DXA scans with a history of low-trauma fracture also likely represents a relatively small proportion of potentially eligible subjects. For example, in the present study, 1.2% of women aged 45–75 in group-1 practices were referred for DXA scans based on a history of non-vertebral fracture. The annual incidence of distal forearm fracture in the UK increases linearly between the ages of 45 to 75, from 10 to 58 per 10,000 [12]. Thus, the prevalence of this fracture alone in the target population is likely to be approximately 5%. This suggestion of lower-than-expected referral rates for DXA scans in patients with previous fracture is consistent with earlier reports that only a small proportion of patients in this category are evaluated for osteoporosis [13, 14]. A lack of consistent diagnostic coding of computerized primary-care records may contribute to this. According to recent report, searching GP computerized records considerably underestimates the number of patients with risk factors for osteoporosis, such as previous fracture [15].
Bisphosphonate therapy was only recommended explicitly in those found to have a BMD within the range of osteoporosis, with the exception of patients with vertebral fracture. However, it is clear that other strategies can be employed. For example, recent guidelines published by the Royal College of Physicians propose that, in patients with a history of non-vertebral fracture and concurrent steroid therapy, treatment with bisphosphonates should also be considered in those with a t-score of ≤−1.5 [16, 17]. If bisphosphonate therapy had been recommended in patients with a history of non-vertebral fracture or concurrent steroid therapy in those found to have osteopenia as well as osteoporosis, bisphosphonate use in group 1 would likely have been significantly higher.
In summary, our results suggest that when applied in a “real life” primary care setting, currently recommended case-finding strategies for osteoporosis result in bisphosphonate therapy being targeted to high-risk groups for osteoporosis. However, they have little effect on the overall rate of bisphosphonate prescribing. The lack of any net increase in bisphosphonate prescribing in the intervention group likely reflects several factors, including the difficulty in identifying patients with previous fractures based on computerized GP records. In light of our findings, further research is required to improve the methods for identifying patients at risk for osteoporosis in primary care, and to determine whether case-finding strategies for osteoporosis are cost-effective, at least in part by enabling bisphosphonate therapy to be targeted to patients at higher risk of fracture.
References
Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P, Rosen C (2002) Meta-analyses of therapies for postmenopausal osteoporosis. IX: Summary of meta-analyses of therapies for postmenopausal osteoporosis. Endocr Rev 23:570–578
National Osteoporosis Society Primary Care Strategy for Osteoporosis and Falls (2002) National Osteoporosis Society, Radstock, UK
Torgerson DJ, Donaldson C, Reid DM (1996) Bone density measurements: are they worthwhile? J R Soc Med 89:457–461
Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd-Jones M (2002) Treatment of established osteoporosis. a systematic review and cost-utility analysis. Health Technol Assess 6:1–146
Townsend P, Phillimore P, Beattie A (1988) Health and deprivation. Croom Helm, London.
Torgerson DJ, Dolan P (1998) Prescribing by general practitioners after an osteoporotic fracture. Ann Rheum Dis 57:378–379
Ross PD, Davis JW, Epstein RS et al (1991) Pre-existing fracture and bone mass predict vertebral fracture incidence in women. Ann Intern Med 114:919–923
Haentjens P, Autier P, Collins J, Velkeniers B, Vanderschueren D, Boonen S (2003) Colles fracture, spine fracture, and subsequent risk of hip fracture in men and women. A meta-analysis. J Bone Joint Surg Am 85-A:1936–1943
Fitt NS, Mitchell SL, Cranney A, Gulenchyn K, Huang M, Tugwell P (2001) Influence of bone densitometry results on the treatment of osteoporosis. CMAJ 164:777–781
Bland M (2000) An introduction to medical statistics. Oxford University Press, Oxford
Chantler IW, Davie MW, Evans SF, Rees JS (2003) Oral corticosteroid prescribing in women over 50, use of fracture prevention therapy and bone densitometry service. Ann Rheum Dis 62:350–352
O’Neill TW, Cooper C, Finn JD, Lunt M, Purdie D, Reid DM, Rowe R, Woolf AD, Wallace WA (2001) Incidence of distal forearm fracture in British men and women. Osteoporos Int 12:555–558
Siris ES, Bilezikian JP, Rubin MR, Black DM, Bockman RS, Bone HG, Hochberg MC, McClung MR, Schnitzer TJ (2003) Pins and plaster aren’t enough: a call for the evaluation and treatment of patients with osteoporotic fractures. J Clin Endocrinol Metab 88:3482–3486
Sahota O, Worley A, Hosking DJ (2000) An audit of current clinical practice in the management of osteoporosis in Nottingham. J Public Health Med 22:466–472
de Lusignan S, Chan T, Wells S, Cooper A, Harvey M, Brew S, Wright M (2003) Can patients with osteoporosis, who should benefit from implementation of the national service framework for older people, be identified from general practice computer records? A pilot study that illustrates the variability of computerized medical records and problems with searching them. Public Health 117:438–445
Compston J (2002) Glucocorticoid-induced osteoporosis: guidelines for prevention and treatment. Royal College of Physicians of London, Bone and Tooth Society, and National Osteoporosis Society. Royal College of Physicians, London
Compston J, Eastell R, Francis R, McCloskey E, Reid D, Tobias JH, Barlow D, Cooper C, Kanis J, Whitehead M (2000) Osteoporosis: clinical guidelines for prevention and treatment. Royal College of Physicians of London and Bone and Tooth Society. Royal College of Physicians, London
Acknowledgements
We are grateful to Procter and Gamble Pharmaceuticals for financial support, and to the following GP practices: Cadbury Heath Health Centre, Stafford Place Surgery, Heywood Surgery, Montpelier Health Centre, Whitchurch Health Centre, Monks Park Surgery, Lawrence Hill Health Centre, Malago Surgery, St George Health Centre, Gloucester Road Medical Centre. We are also grateful to Pam Brown, Chris Salisbury and Sanjeev Patel for reviewing draft versions of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morrison, L.S., Tobias, J.H. Effect of a case-finding strategy for osteoporosis on bisphosphonate prescribing in primary care. Osteoporos Int 16, 71–77 (2005). https://doi.org/10.1007/s00198-004-1644-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-004-1644-z