
Abstract
To determine if physicians have improved the recognition and treatment of osteoporosis in patients with an acute hip fracture, we performed a retrospective analysis of discharge data from 1995 and 2000 at the University of Pittsburgh Medical Center, a large tertiary care, academic institution. We examined patients admitted with an acute hip fracture in 1995 and 2000 and age- and sex-matched patients admitted with community acquired pneumonia in 2000. Outcomes included age, gender, race, discharge diagnoses (from ICD-9 codes) and discharge medications (from discharge summaries) in all patients. There were 136 acute hip fracture patients (mean age 73±18 years) in 1995, 117 acute hip fracture patients (mean age 76±16 years) in 2000 and 116 patients with community-acquired pneumonia (mean age 78±7 years). Patients admitted in 2000 with an acute hip fracture were more likely to be diagnosed with osteoporosis (18% vs. 4%, P<0.02), more likely to be discharged on calcium (17% vs. 7%, P<0.02) and more likely to be discharged on antiresorptive therapy (15% vs. 2%, P<0.001) than those admitted in 1995. Moreover, patients admitted with community-acquired pneumonia were just as likely to receive calcium, vitamin D or antiresorptive agents at the time of discharge as those with an acute hip fracture in 2000. Patients with a diagnosis of osteoporosis in 2000 were older and more likely to receive antiresorptive agents than those without a diagnosis (29% vs. 11%, P<0.05). None of the patients received a bone mineral density examination while in the hospital. Although there was an improvement in the management of osteoporosis after an acute hip fracture from 1995 to 2000, there was no difference in management of patients with hip fracture versus pneumonia in the year 2000. However, patients with a “diagnosis” of osteoporosis in 2000 were more likely to be discharged on appropriate therapeutic options. We conclude that although we have improved our care of osteoporosis for elderly in general from 1995 to 2000, patients with an acute hip fracture are not receiving any additional treatment unless they have a diagnosis of osteoporosis. Further studies are needed to determine which factors are needed to target patients for appropriate diagnosis and treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is the major contributing factor to fractures in the elderly population [1]. There are approximately 1.3 million osteoporotic fractures involving the spine, hip and distal radius in the U.S. each year [2] at a cost of over 13.8 billion dollars in 1995 (equivalent to 17 billion dollars in 2001) [1, 3]. However, fractures of the hip are associated with the greatest morbidity and mortality. Over 50 percent of patients become institutionalized and up to 20% of patients die within the first year after the hip fracture [1].
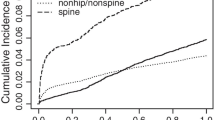
Furthermore, studies have demonstrated that the occurrence of one type of fracture increases the probability of a second type of fracture [4, 5, 6, 7, 8, 9]. The occurrence of a hip fracture increases the risk of a subsequent fracture by up to six-fold [10, 11], and the occurrence of one vertebral fracture increases the risk of a second vertebral fracture by four-fold [5, 6]. Moreover, there are potent antiresorptive medications in our pharmaceutical armamentarium that prevent further bone loss, increase bone mineral density and reduce the risk of vertebral and hip fractures [12, 13, 14, 15, 16, 17, 18, 19]. To date, no clinical trial has tested whether an antiresorptive or anabolic therapy given after a hip fracture will reduce the rate of subsequent fracture; however, a consensus conference statement and guidelines developed by the National Institutes of Health recommended osteoporosis treatment for patients who sustain a hip fracture [20]. Therefore, with the knowledge that osteoporosis is common, associated with significant mortality and morbidity and that a previous fracture is a major risk factor for a subsequent fracture, it would be appropriate to implement osteoporosis preventive and therapeutic measures at the time of admission for a hip fracture.
To determine if hospitalization for hip fracture has an impact on the diagnosis, evaluation and subsequent treatment of osteoporosis, and if the availability of new agents has improved our treatment track record, we performed a retrospective analysis of patients with acute hip fractures admitted to the University of Pittsburgh Medical Center in the years 1995 and 2000. For a hospital control group, we examined the number of elderly patients admitted with community-acquired pneumonia in 2000. Community-acquired pneumonia was chosen to represent a common nonskeletal-related hospitalization in this age group. We postulated that at an academic institution, in which lectures on osteoporosis, National Osteoporosis Foundation guidelines and rehabilitation are frequently presented to the house staff and faculty, the majority of patients with acute hip fracture would be assigned a diagnosis of osteoporosis and sent home on calcium, vitamin D or antiresorptive therapy. We also postulated that patients without this diagnosis would be less likely to receive preventive measures after the fracture, and those without a diagnosis of hip fracture (i.e., those with community-acquired pneumonia) would be less likely to be discharged on preventive or therapeutic alternatives for osteoporosis.
Materials and methods
After obtaining approval by the Institutional Review Board, a retrospective chart analysis was conducted using the ICD-9 diagnosis codes for all acute hip fractures in the years 1995 and 2000, and elderly patients with community-acquired pneumonia in 2000, admitted to the University of Pittsburgh Medical Center (including Presbyterian University Hospital and Montefiore University Hospital—tertiary care, level-1 trauma centers). The hospitals have residency programs in internal medicine and orthopedics, as well as fellowship programs in endocrinology, rheumatology and geriatrics. The data were collected by electronic medical records using discharge diagnosis codes. The codes included those for pathologic femur fracture, intracapsular femur fracture, closed epiphyseal femur fracture, femoral neck fracture, trochanteric fracture, intertrochanteric fracture and subtrochanteric fracture. ICD-9 codes for community-acquired pneumonia were also included.
Collected data included the patient’s age, gender, race, etiology of hip fracture (fall, motor vehicle accident, trauma or unknown), whether the patients received a dual-energy X-ray absorptiometry (DXA) scan as an inpatient or had a DXA scan ordered for the time of follow-up, and medications the patients received at discharge (e.g., calcium, vitamin D, bisphosphonates, calcitonin, hormone replacement therapy or selective estrogen receptor modulators). We assessed if the diagnosis of osteoporosis was assigned to the patient. The patient’s name and medical record number were not provided. Patient data were provided by an honest broker who was not aware of the research question.
The clinical characteristics of all patients were examined, including race, gender and age. Comparison of the categorical data from 1995 and 2000 was performed by Fisher’s exact test as well as acute hip fracture in 2000 and community-acquired pneumonia in 2000. In 2000, patients with hip fracture were divided into two groups according to whether or not they had received a diagnosis of osteoporosis. Fisher’s exact test was performed to determine whether diagnosis of osteoporosis impacted on hip fracture patients receiving calcium, vitamin D or antiresorptive therapy during the year 2000. Characteristics such as race and gender on influence of osteoporosis diagnosis were also assessed. The effect of mean age on influence of diagnosis was analyzed via two-sample t-test. Significance was defined as a P<0.05. Statistical procedures were performed with the SAS 8.1 program (SAS Institute, Cary, N.C., USA).
Results
In 1995, 136 patients were admitted with an acute hip fracture. The majority of patients were Caucasian women (Table 1), and only 4% received a discharge diagnosis of osteoporosis. Overall, 7% of the patients were discharged on calcium, 8% on vitamin D and 2% on antiresorptive therapy (Table 1).
In the year 2000, 117 acute hip fracture patients were admitted to the hospital. The overall mean age was 76±16 years, and the majority of patients were Caucasian women (Table 1). The most common reason for fracture was a fall from standing height. Seventy (60%) patients had a fall from standing height, 15 (13%) fractures were sustained during motor vehicle accidents, 10 (9%) were from other traumas, and the cause was unknown in 22 (19%) of the patients. Only twenty (17%) of the 117 hip fracture patients were discharged home on supplemental calcium in 2000, and 12% were discharged home on vitamin D (Table 1). Seventeen (15%) were discharged home on some form of antiresorptive therapy.
In 2000, 294 patients were admitted with community-acquired pneumonia. A subset of 120 patients was analyzed who were matched for age and sex, but not race (Table 1). The mean age was 78±7 years, and 66% were women. In this group, 20% were discharged home on supplemental calcium, 18% on some form of vitamin D and 10% on antiresorptive therapy (Table 1).
Comparisons between 1995 and 2000
Only 5 patients in 1995 were diagnosed with osteoporosis at the time of discharge, while 21 patients in 2000 had been diagnosed (4% in 1995 vs. 18% in 2000, P<0.001). The average age of the patient with a hip fracture in 1995 was 73±18 years; this was not statistically different from the mean age found in 2000 (76±16). There was a significant difference in the racial composition between the 2 years studied; patients in 1995 were nearly all Caucasian (92% in 1995 vs. 63% in 2000, P<0.001). A multivariate logistic regression was performed to assess the diagnosis of osteoporosis, adjusted for the effects of age, race, gender and date of diagnosis. Hip fracture patients were 2.25 times more likely to be diagnosed with osteoporosis in 2000 than in 1995 (CI 1.29 to 3.94, P<0.01).
Only ten patients were discharged on supplemental calcium in 1995, whereas twice as many received this in the year 2000 (7% in 1995 vs. 17% in 2000, P<0.02, Table 1). There was no statistically significant difference in vitamin D prescribing behavior between these years. This is in contrast to antiresorptive medication, which was much more likely to be prescribed in 2000 versus 1995 (2% in 1995 vs. 15% in 2000, P≤0.001). In 1995, only one patient received alendronate, and two received hormone replacement therapy. No patients in 1995 received DXA scans. In 2000, there were no statistically significant differences between patients with hip fracture or community-acquired pneumonia regarding the number of patients discharged on calcium, vitamin D or antiresorptive therapy.
Comparison of patients with and without a diagnosis of osteoporosis
Of the 117 acute hip fractures in 2000, 21 (18%) were diagnosed with osteoporosis and 96 were not. The patients in the osteoporosis-diagnosed group versus those without this diagnosis had a higher percentage of females than males (81% vs. 65%), but this was not statistically significant (Table 2). There was no difference in racial background. Patients diagnosed with osteoporosis were significantly older than those who did not receive a diagnosis (81±10 vs. 74±16 years, P<0.05).
Patients with a diagnosis of osteoporosis were more likely to be discharged on supplemental calcium (24% vs. 16%, P=0.37), but this was not significantly different. Only 14 patients were discharged home on supplemental vitamin D therapy: 4 (19%) in the osteoporosis diagnosed group and 10 (10%) in the undiagnosed group (P=0.39).
Patients assigned a diagnosis of osteoporosis were more likely than patients without an osteoporosis diagnosis to have been discharged on antiresorptive therapy (29% vs.11%, P<0.05, Table 2). Nine patients were discharged on calcitonin, eight on alendronate, and two on hormone replacement therapy. No patients were prescribed risedronate or raloxifene. None of the patients had a DXA scan scheduled or performed while in the hospital.
Discussion
Between 1995 and 2000, the diagnosis and management of osteoporosis after acute hip fractures has changed in our institution. The rate of diagnosis increased from 4% in 1995 to 18% in 2000. The groups were similar in age and gender, but different in racial composition. This may have been due to expansion in the patient catchment area between 1995 and 2000. More importantly, twice as many patients were discharged on supplemental calcium, and a higher percentage (2% vs. 15%) were being sent home on antiresorptive agents in 2000 compared to 1995. This may have been due to the approval of several new antiresorptive therapies since 1995. However, an unexpected finding was that patients admitted with community-acquired pneumonia were just as likely to be treated with calcium, vitamin D or antiresorptive therapy at discharge as those who were discharged with a diagnosis of hip fracture. This implies that care for skeletal health in older patients may have improved since 1995, but not care specific for elderly patients with a hip fracture.
Patients who were assigned a diagnosis of osteoporosis were more likely to receive some form of therapy. The percentages of patients who received calcium, vitamin D and antiresorptive agents were higher in the group that had the diagnosis, but a statistically significant difference was found only among the patients who received antiresorptive therapy.
Other studies have reported similar findings [21, 22]. Black and colleagues found that the diagnosis of osteoporosis was made in only 14% of patients admitted for hip fracture over a 5-year period at an academic institution [21]. A large retrospective study by Castel and colleagues found that physicians rarely made the diagnosis of osteoporosis even in the setting of a low impact fracture [23]. Only 30 to 40% of the patients received any medication for osteoporosis 6 months after the fracture, and this was primarily calcium supplementation. Kleerekoper reported that the rate of diagnosis of osteoporosis is low even after insurance claims are made for a fracture [24]. Only 21% of nearly 30,000 women over the age of 50 making a claim for a fracture submitted a claim for osteoporosis, indicating that most fractures are not recognized as being related to osteoporosis.
Several other studies have demonstrated that management after osteoporotic fractures is inadequate. Kahn noted that half of the patients who sustained a wrist fracture from minor trauma received no follow-up attention for osteoporosis, and very few received any medications [25]. In another study, after distal radius fractures in over 1,000 women, less than 3% received a DXA scan and less than a quarter were started on at least one form of therapy [26]. As patients grew older, they were less likely to receive any therapy. A medical consultation for a hip fracture patient does not appear to improve osteoporosis therapy or DXA scanning [27]. A recent study identified predictors of osteoporosis treatment in postmenopausal women after distal forearm fractures, and only 17% of these women were started on medications for osteoporosis [28]. Women who were diagnosed with osteoporosis, those with a previous distal radius fracture and smokers were more likely to receive medications. In our institution, no patients received a DXA scan at the time of the fracture, and only 17% received calcium, 12% vitamin D and 15% an antiresorptive agent.
Our study has several limitations. Since discharge diagnosis codes were used, we know how many patients left the hospital with a diagnosis of osteoporosis, but we do not know the number of patients who were admitted to the hospital with that diagnosis. We also do not know the medications on admission. In addition, it is possible that we may have missed some codes for diagnosis, fracture, calcium, vitamin D or any of the antiresorptive agents. There are many over-the-counter supplements containing calcium that we may have overlooked. Although we examined common supplements found in the Physicians Desk Reference for nonprescription drugs that contain vitamin D or pure vitamin D (e.g., multivitamins containing 400 IU vitamin D), we may have missed other supplements that contain vitamin D. Also, we examined only hospitalized patients. It is possible that if we looked at patients after their follow-up orthopedic clinic visit, the number of patients on calcium, vitamin D or other therapy may have been greater. Our analysis may have included patients with hip fracture from other causes besides osteoporosis. Sixty percent of hip fractures occurred after a fall from standing height, consistent with the clinical diagnosis of osteoporosis. Although 13% had a hip fracture after an automobile accident and 9% from other trauma, it is still possible that they had osteoporosis. Cummings and colleagues recently reported data from a prospective study of over 9,700 elderly women and found that traumatic fractures in older women were osteoporotic fractures [29]. Even if we excluded those patients, of the 92 remaining patients, at best only 22, 15 and 18% would have been treated with calcium, vitamin D and antiresorptive therapy, respectively.
There are several strengths to the study as well. There were over 100 patients admitted to the hospital with an acute hip fracture in 1995 and 2000, so we were not analyzing a novel event. Our study included both men and women, whereas many other studies dealing with osteoporosis have concentrated only on women. In fact, men comprised about one-third of the fractures. In addition our institution has a state-of-the-art DXA scan easily available to these patients, so access to bone mineral density imaging would not be an issue in the postoperative management of the patients. Finally, we included a control group of patients with community-acquired pneumonia, a disease unlikely to have a major impact on bone, or to be a reason to start calcium, vitamin D or antiresorptive therapy. This suggests that overall, our osteoporosis prevention or treatment of patients with a hip fracture is no better than the care given to elderly patients admitted with pneumonia.
The findings of this study suggest that the management of osteoporosis may be inadequate, and the diagnosis is made in less than 20% of patients with acute hip fracture. It is encouraging that the diagnosis and treatment have improved over the past 5 years. However, it is discouraging that patients discharged with a diagnosis of community-acquired pneumonia were just as likely to receive calcium, vitamin D or antiresorptive therapy as those with a diagnosis of hip fracture. We found that older patients were more likely to be assigned a diagnosis of osteoporosis. Moreover, the patients who received a diagnosis were more likely to receive appropriate management in the form of calcium, vitamin D and antiresorptive therapy. Therefore, if patients can be recognized as having osteoporosis, there may be improvement in their subsequent management. Further studies are needed to focus on the risk factors, events or hospital identifiers that will improve the chance that a patient with a hip fracture will receive the diagnosis of osteoporosis and receive appropriate preventive and therapeutic alternatives.
References
Cummings SR, Melton LJ III (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Consensus Development Conference (1993) Consensus development conference: diagnosis, prophylaxis and treatment of osteoporosis. Am J Med 94:646–650
Ray NF, Chan JK, Thamer M, et al (1997) Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: Report from the National Osteoporosis Foundation. J Bone Miner Res 12:24–35
Ribot C, Tremollieres F, Pouilles JM, et al (1993) Risk factors for hip fracture. MEDOS study: results of the Toulous Centre. Bone 14:S77–80
Ross P, Genant H, Davis J, et al (1993) Predicting vertebral fracture incidence from prevalent fractures and bone density among non-black, osteoporotic women. Osteoporos Int 3:120–126
Wasnich R, Davis J, Ross P (1994) Spine fracture risk is predicted by non-spine fracture. Osteoporos Int:4:1–5
Cummings SR, Nevitt MC, Browner WS, et al (1995) Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med 332:767–773
Nguyen T, Eisman J, Kelly P, et al (1996) Risk factors for osteoporotic fractures in elderly men. Am J Epidemiol 144:255–263
Klotzbuecher C, Ross P, Landsman P, et al (2000) Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15:721–739
Colon-Emeric CS, Sloane R, Hawkes WG, et al (2000) The risk of subsequent fractures in community-dwelling men and male veterans with hip fracture. Am J Med 109:324–326
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359:1929–1936
Liberman UA, Weiss SR, Broll J, et al (1995) Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. N Engl J Med 333:1437–1443
Black DM, Cummings SR, Karpf DB, et al (1996) Randomized trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet 348:1535–1541
Harris ST, Watts NB, Genant HK, et al (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. JAMA 82:1344–1352
McClung MR, Geusens P, Miller PD, et al (2001) Effect of risedronate on the risk of hip fracture in elderly women. N Engl J Med 344:333–340
The Writing Group for the PEPI Trial (1996) Effects of hormone replacement therapy on bone mineral density: results from the postmenopausal estrogen/progestin (PEPI) interventions trial. JAMA 276:1389–1396
Ettinger B, Black DM, Mitlak BH, et al (1999) Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. JAMA 282:637–645
Chestnut CH, Silverman S, Andriano K, et al (2000) A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: The Prevent Recurrence of Osteoporotic Fractures Study. Am J Med 109:267–276
Delmas PD (2000) Treatment of postmenopausal osteoporosis. Lancet 359:2018–2026
Anonymous (2000) Osteoporosis prevention, diagnosis and therapy. National Institutes of Health Consensus Development Conference Statement, 27–29 March, 2000
Black JN, Follin SL, McDermott MT (2001) Osteoporosis diagnosis and management following hip fracture. J Bone Miner Res 16 (abstract):S214
Juby AG, de Geus-Wenceslau CM (2002) Evaluation of osteoporosis treatment in seniors after hip fracture. Osteoporosis Int 13:205–210
Castel H, Bonneh DY, Sherf M, et al (2001) Awareness of osteoporosis and compliance with management guidelines in patients with newly diagnosed low-impact fractures. Osteoporos Int 12:559–564
Kleerekoper M, Hamre M, Miller V, et al (2000) Age-related fractures and recognition of osteoporosis: Studies from a 3-year database with 29,994 fracture cases in women over 50. J Bone Miner Res 15 [Suppl 1] (abstract):S413
Khan SA, deGeus C, Holroyd B, et al (2001) Osteoporosis follow-up after wrist fractures following minor trauma. Arch Intern Med 161:1309–1312
Freedman KB, Kaplan FS, Bilker WB, et al (2000) Treatment of osteoporosis: Are physicians missing an opportunity? J Bone Joint Surg Am 82:1063–1070
Kamel HK, Hussain MS, Tariq S, et al (2000) Failure to diagnose and treat osteoporosis in elderly patients hospitalized with hip fractures. Am J Med 109:326–328
Cuddihy MT, Gabriel SE, Crowson CS, et al (2002) Osteoporosis intervention following distal forearm fractures: a missed opportunity? Arch Int Med 162:421–426
Cummings SR, Stone KL, Hillier TA, Bauer DC, Genant HK, Harris ST, Cauley JA (2002) Are traumatic fractures osteoporotic? J Bone Miner Res 17 [Suppl 1]:(abstract in press)
Acknowledgements
We gratefully acknowledge the assistance of Melissa Saul, Branden Smith and Amanda Schultz as honest brokers for data procurement.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bahl, S., Coates, P.S. & Greenspan, S.L. The management of osteoporosis following hip fracture: Have we improved our care?. Osteoporos Int 14, 884–888 (2003). https://doi.org/10.1007/s00198-003-1492-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-003-1492-2