
Abstract
Left-handedness has been associated with increased fracture risk in a small number of previous studies. This study reports risks for fractures at the proximal humerus, distal forearm, pelvis, foot, and shaft of the tibia/fibula according to handedness in a case-control study conducted from October 1996 to May 2001 among members of Northern California Kaiser Permanente. Handedness was assessed by questionnaire for 2,841 cases and 2,192 controls, and subjects were categorized as left-handed, right-handed, ambidextrous, or forced to switch from the left to the right hand. Compared to right-handedness, left-handedness was most strongly associated with an increased risk for proximal humerus fractures (adjusted odds ratio (OR)=2.00, 95% confidence interval (CI) 1.33 to 3.01) and less definitively with fractures of the distal forearm (adjusted OR=1.28, 95% CI 0.92 to 1.80), foot (adjusted OR=1.17, 95% CI 0.82 to 1.65), and pelvis (adjusted OR=1.40, 95% CI 0.71 to 2.74). Ambidextrous individuals had elevated risks for fractures of the distal forearm (adjusted OR=2.99, 95% CI 1.42 to 6.30), foot (adjusted OR=2.59, 95% CI 1.13 to 5.97), shaft of the tibia/fibula (adjusted OR=3.91, 95% CI 1.01 to 15.17), and proximal humerus (adjusted OR=2.37, 95% CI 0.85 to 6.65) when compared with right-handed individuals. Those individuals forced to use the right hand demonstrated no increased risk for fractures at any site. These results suggest that handedness does influence fracture risk, but the reasons for this increased risk are unclear.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Approximately 8% of the human population is left-handed [1]. Theories about the development of left-handedness can simplistically be divided into two categories: pathological development of left-handedness and natural left-handedness. Pathological models suggest that left-handedness is a deviation from normal right-handed tendencies and develops as a result of pathological aberrations during gestation that disrupt normal development, altering brain lateralization, and causing the left hand to become the dominant hand [2, 3]. Natural left-handedness is thought to be a natural phenomenon with a familial component, and genetic models have been derived to explain its occurrence [4].
Some evidence suggests that left-handedness, whether pathological or natural, increases risk for fracture. Hemenway et al. [5] found that left-handers had a 56% increased risk for distal forearm fracture compared with right-handers, and those forced to use their right hand despite left-hand dominance had a twofold increased risk. Stellman et al. [6] found in a hospital-based case-control study of cancer and myocardial infarction that men with fractures (who were included in either the case or control group) were more than twice as likely to be left-handed as patients with other diagnoses. left-handedness also has been associated with an increased prevalence of immune and neurodevelopmental disorders [7, 8, 9] and reduced immunity [10] and survivorship [11], although the evidence supporting these relationships is controversial. Individuals with such disorders may be more likely to fall and fracture as a result of diminished health status, particularly if they suffer from a neurodevelopmental disorder such as seizures. Left-handedness is suggested to be associated with other risk factors for osteoporosis and fracture such as heavy drinking [12, 13] and reduced body weight [14], although the evidence is far from convincing. Finally, some studies have found that left-handedness is a risk factor for accident and injury [15, 16, 17], possibly because of an environmental bias toward right-handedness; that is, left-handed people must live in a world designed for right-handed people. For example, often stairways do not have handrails on the left side and gearshifts in both automatic and manual cars are located on the right side of the driver in most countries.
The purpose of this paper is to examine the association between handedness and fracture at five fracture sites: distal forearm, proximal humerus, shaft of the tibia/fibula, pelvis, and foot.
Materials and methods
Cases and controls were selected from five Northern California Kaiser Permanente Medical Centers (San Francisco, Santa Clara, South San Francisco, Oakland, and Hayward) between October 1996 and May 2001.
Cases
Incident cases of age 45 years and older were identified on a weekly basis through computerized radiology, inpatient, and outpatient records. Information on diagnosis and fracture site was obtained from radiology reports and medical records by a trained record abstractor. To be included as a case, the fracture had to be confirmed by X-ray, bone scan, or MRI. Pathological fractures due to specific diseases were excluded. In order to maintain a consistent comparison group, individuals experiencing a fracture at more than one of the specified fracture sites during the study period were included as cases for only the first diagnosed fracture at one of the sites under study. Classification of fractures followed the International Statistical Classifications of Diseases and Related Health Problems, Tenth Revision [18].
Of potential cases, all non-white individuals and a percentage of white individuals were approached to join the study. Until May 1, 2000, we sampled 50% of whites with proximal humerus and distal forearm fractures and 25% of whites with foot fractures as cases. In order to increase numbers, all whites with distal forearm fractures and 50% of whites with foot fractures were sampled after May 1, 2000. Because pelvis and shaft of the tibia/fibula are uncommon fracture sites, all white persons with these fractures were included. In order to increase the representation of racial and ethnic minorities in the study population, 100% of individuals indicated as a minority and those without race/ethnicity recorded in Kaiser records were included as cases for all fracture sites under study. Participation among eligible cases was 72%.
Controls
During the same time period, 2192 controls were selected. Every 3 months Kaiser Permanente members with no previous fractures of the foot, distal forearm, proximal humerus, shaft of the tibia/fibula, or pelvis were stratified into nine 5-year age groups (45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, and 85+) and two gender groups. These groups were randomly ordered and the first 34 females and 7 males in each 5-year age group were selected. All minorities and individuals of unknown race/ethnicity and 39% of white females and 78% of white males were chosen as controls. Participation among the eligible controls was 64%.
Questionnaires
Information about potential risk factors was gathered from a standardized questionnaire administered by trained interviewers in English or Spanish. The questionnaire covered demographic characteristics, immigration history and acculturation, certain aspects medical history, handedness, use of certain medications and nutritional supplements, physical activity, physical function, activities of daily living, home hazards, dietary calcium intake, history of falling, and immediate cause of fracture. Questions referred to the period before fracture for the cases and to the period before interview for the controls. During the first 3 years of the study, most interviews were conducted in person at the participant’s home. To increase participation rates and numbers of subjects interviewed, the interviews were primarily conducted over the telephone after November 15, 2000. Type of interview was not found to be an effect modifier, but is included as a covariate in the multivariate analysis.
The questionnaire assessed handedness by asking, “Do you usually write with your left hand, right hand, or do you use both hands equally well?” Those who indicated they used both hands equally well (ambidextrous) or were right-handed were asked if they had been forced to change from being naturally left-handed to being right-handed. Raczkowski and Kalat [19]validated “Which hand do you write with?” as 96% reliable using test-retest and 100% accurate when comparing responses to performance tests.
Participants who were interviewed in languages other than English and Spanish were excluded. Three participants were excluded because the quality of the interview was determined to be unsatisfactory by the interviewer. Nine additional participants were excluded because of missing handedness data. Finally, 190 proxy respondent interviews were excluded because of missing data and because there were too few proxy respondents to assess adequately interactions involving handedness by self versus proxy status.
Statistical analysis
Following preliminary descriptive analysis, the relationships between handedness and fracture were assessed using unconditional logistic regression with SAS version 8.2 software to calculate adjusted odds ratios. Handedness and having been forced to change hand of preference were separated into five categories: (1) right-handers who had not been forced to change hand of preference or did not know if they had been forced to change, (2) right-handers who had been forced to change hand of preference, (3) ambidextrous individuals who had not been forced to change hand of preference or did not know whether or not they had been forced to change, (4) ambidextrous individuals who had been forced to change hand of preference, and (5) left-handers. Variables that altered the odds ratio for handedness by 10% or more were considered confounders. The model presented here controlled for design variables including type of interview (telephone or in person), 5-year age group, gender, race/ethnicity as indicated by Kaiser records, and confounding variables including self-reported race/ethnicity, age in years, whether the participant took seizure medications, body mass index, and a summary score for frailty. The summary frailty score was computed using information obtained from the questionnaire. Participants scored one point for each illness, each medication, each difficulty with a daily activity, each area of reduced physical function, each mobility aid used, each neuromuscular symptom, and for self-reported poor health. Kaiser-recorded race/ethnicity and 5-year age group were included in the model because subjects were sampled using these variables; self-reported race/ethnicity and age were additionally included in the model to more carefully adjust for these variables.
Self-reported race/ethnicity was categorized into four groups: (1) white, Native American and other, (2) black, (3) Chinese, Filipino, Japanese, Pacific Islander and other Asians, and (4) Hispanic. Those subjects who placed themselves in more than one category were classified into one of the above four categories through their answers to questions on acculturation.
Finally, possible effect modifications by race/ethnicity, age, gender, and type of interview were examined first by stratification and then by including cross-product terms in the multivariate model. There was no evidence of effect modification, indicating that odds ratios were consistent across these groups. We also compared those who enrolled in the study prior to May 1, 2000, with those who enrolled on or after that date to ensure the protocol change in the percentage of whites sampled did not bias results. Again, no effect modification was found.
Results
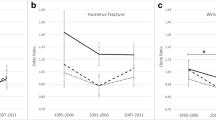
Of 5,033 cases and controls in the total study population, 88.7% were right-handed, 5.8% were left-handed, 1.1% were ambidextrous, and 4.4% were forced to use the right hand instead of the left. (Table 1). The 32 ambidextrous individuals who had been forced to use their right hands were combined with the 191 right-handers who reported having been forced to switch from left-handedness to right-handedness, because these groups had similar odds for fracture. The prevalence of having been forced to switch hand of preference increased with earlier birth cohort. Prevalence of reported left-handedness decreased with earlier birth cohort while the prevalence of right-handedness remained the same. Pacific Islanders and other Asians had a lower prevalence of left-handedness and greater prevalence of having been forced to switch hands compared with other race/ethnicity groups. However, we were unable to examine race/ethnicity as a risk factor because cases and controls were frequency matched on race.
Table 2 shows that left-handed individuals were at a 33% increased odds for fracture at all fracture sites combined. When each fracture site was examined individually, left-handedness was associated with almost a doubling of risk for fracture at the proximal humerus, and a moderately elevated risk for fractures at the distal forearm, foot, and pelvis. There were few pelvis and tibia/fibula cases, resulting in wide confidence intervals.
Ambidextrous individuals were at 2.6 times the risk for fractures at all sites combined compared with right-handers. Ambidextrous individuals were also at greater risk for fractures at each of the five individual sites. Individuals forced to switch hand of preference demonstrated a trend toward a reduced risk for fractures at the proximal humerus, distal forearm, foot, and pelvis, but numbers were small.
Because prior studies suggested that left-handers have compromised immunity and decreased survivorship, we compared the questionnaire-derived medical histories of left-handers, right-handers, and ambidextrous individuals, combining cases and controls. left-handers were more likely to report taking seizure medications (adjusted OR=1.87, 95% CI 1.06 to 3.29) and a history of hypothyroidism (adjusted OR=1.59, 95% CI 1.10 to 2.31) than right-handers. No differences were noted in the prevalence of diabetes, angina, stroke, kidney disease, epilepsy, cataracts, glaucoma, arthritis, depression, cancer, or hyperthyroidism. Likewise, left-handers were no more likely than right-handers to have neuromuscular problems or difficulty performing activities of daily living. Ambidexterity was associated with a greater number of neuromuscular problems such as difficulty balancing and numbness in extremities (adjusted OR=1.24, 95% CI 1.07 to 1.44), but was not associated with the difficulty performing activities of daily living (OR=1.09, 95% CI 0.90 to 1.31) or reduced physical function (OR=1.14, 95% CI 0.90 to 1.44) when ambidextrous individuals were compared with right-handers. Those who were forced to use the right hand instead of the left were slightly more likely to have difficulty performing activities of daily living (adjusted OR=1.10, 95% CI 1.00 to 1.21) than right-handers. Controlling for difficulty performing daily activities, neuromuscular symptoms, average monthly alcohol intake, and body mass index did not alter the relationship between fracture risk and handedness.
Discussion
Our data indicate that left-handed individuals were at an increased risk for fracture of the proximal humerus and suggest that they may also be at greater risk for forearm, foot, and pelvis fracture. These findings support the previous results of Hemenway et al. [5] and Stellman et al. [6] who found elevated odds for fracture among left-handers.
While our study found ambidextrous individuals had the greatest risk for fracture, one previous study [5] found that the odds for distal forearm fractures among ambidextrous individuals was no different from right-handers. Also, we found that those individuals who were forced to switch from the left to the right hand were at no greater risk than right-handers for fractures at five sites. The only previous study to consider individuals who had been forced to switch the hand of preference [5], found that those who had been forced to switch the hand of preference had more than twice the risk of forearm fractures as right-handers.
The reasons for an increased risk for fracture among left-handers and possibly ambidextrous individuals were not clear. We controlled for one pathological problem associated with left-handedness, seizures; however, this association did not explain the observed relationship between fracture risk and handedness. Likewise, disease occurrence, frailty, alcohol intake, and body weight did not account for the association between handedness and fracture risk. Because this study was not designed to assess the disadvantages, if any, left-handers experience by living in a world designed for right-handed people, we could not examine this hypothesis. Little research has been done to characterize ambidextrous individuals specifically, as they are often combined with left-handers as “non right-handers.” The etiology driving either the ability to effectively use either hand for any given task or to prefer different hands for different tasks has not been explored. However, one can learn to use the nondominant hand effectively for specific tasks if those tasks are easy or practiced frequently [20].
That fracture risks for those forced to change hand of preference were similar to risks for right-handers may suggest that living in a world designed for right-handed people creates an increase in fracture risk for non right-handers. If the cause for increased fracture risk were entirely pathological, one would expect that all persons born with a preference for the left hand would be susceptible to these pathological problems and the actual hand used most often would be irrelevant; thus, we would expect both left-handers and those who were forced to switch hand of preference to have similar fracture risks. However, if environmental bias were responsible for the increased fracture risk in non right-handers, we would expect that those using either hand equally well would not differ from right-handers. Instead, we found that ambidextrous individuals were at the greatest risk for fracture. This may suggest that ambidextrous individuals differ from both right and left-handers. Specifically, ambidextrous individuals often report that they are able to use both hands equally well, though they are more adept with one hand [20]. If they frequently use the less adept hand, they may be at greater risk for injury and fracture because they lack dexterity. While true ambidexterity means equal skill in both hands (implying that both hands are equally capable of performing activities), almost everyone favors one hand over the other, though some people do prefer different hands for different tasks [20]. No other studies have reported similar findings for ambidextrous individuals, and further studies are warranted to evaluate whether this is a chance finding.
This study had several limitations. First, we assessed handedness with just two questions, forcing respondents to qualify themselves as left-handed, right-handed, or ambidextrous. However, handedness is not a categorical variable. It exists as a bimodal continuum with many people favoring either the left or the right hand and many people falling in between these extremes. Ideally this variable would be assessed using multiple measures of hand skill and/or hand preference. Also, detailed information regarding all pathological problems associated with left-handedness were not available, and we were able to use only a few measures to examine this hypothesis. The small number of ambidextrous participants and participants who had been forced to change hands precluded a thorough analysis of differences between left-handedness, right-handedness, and ambidexterity, and reduced our power to examine some fracture sites. Finally, as with many case-control studies, the data are subject to recall error.
To our knowledge, this is the first study to examine the relationship between handedness and fracture at the proximal humerus, foot, pelvis, and shaft of the tibia/fibula, and the second to look at the association of handedness and fracture risk at the distal forearm. Handedness is usually a lifelong exposure that is difficult to modify. Thus, there is little concern about temporality. Recall bias may be minimized because this study was addressing handedness only incidentally among many other issues.
Based on these and previous [5, 6] findings, we conclude that left-handedness is probably associated with fracture risk, particularly at the proximal humerus in our study and the distal forearm in the study of Hemenway et al. [5]. The reasons for these associations are unclear. We noted an association between seizures and handedness, but this association did not account for the relationship between fracture and handedness. We also found evidence suggesting that ambidextrous individuals were at an increased risk for fracture at multiple sites, while those who were forced to use the right hand appeared to be no different from natural right-handers; however, these finding are not supported by Hemenway et al. [5]. Studies to distinguish further the differences in risk for fractures between ambidextrous, right-handers, and left-handers are warranted. Moreover, research should be done to determine the extent to which right-handed environmental bias influences the risk for fracture among left-handed and ambidextrous individuals, particularly because this environmental bias is modifiable.
References
Seddon BM, McManus IC (1991) The incidence of left-handedness: a meta-analysis. Unpublished manuscript, University College, London
Geschwind N, Galaburda AM (1985) Cerebral lateralization: biological mechanisms, associations, and pathology (I, II, III). Arch Neurol 42:428–654
Searleman A, Coren S, Porac C (1989) Relationship between birth order, birth stress, and lateral preferences: a critical review. Psychol Bull 105:397–408
McManus C (1991) The inheritance of left-handedness. In: Brock G, Marsh J (eds) Biological asymmetry and handedness. Ciba Foundation Symposium 162. Wiley, New York, pp 251–281
Hemenway D, Azrael DR, Rimm EB, Feskanich D, Willett W (1994) Risk factors for wrist fracture: effect of age, cigarettes, alcohol, body height, relative weight, and handedness on the risk for distal forearm fractures in men. Am J Epidemiol 140:361–367
Stellman S, Wynder E, DeRose D, Muscat J (1997) The epidemiology of left-handedness in a hospital population. Ann Epidemiol 7:167–171
Flannery K, Leiderman J (1995) Is there really a syndrome involving the co-occurrence of neurodevelopmental disorder, talent, non right-handedness and immune disorder in children? Cortex 31:503–515
Kim H, Yi S, San EI, Kim J (2001) Evidence for the psychological right-handedness hypothesis. Neuropsychology 15:510–515
Geschwind N, Behan P (1982) Left-handedness: association with immune disease, migraine, and developmental learning disorder. Proc Natl Acad Sci U S A 79:5097–5100
Morfit NS, Weekes NY (2001) Handedness and immune function. Brain Cogn 46:209–213
Coren S, Halpern DF (1991) left-handedness: a marker for decreased survival fitness. Psychol Bull 109:90–106
Chyatte C, Smith V (1981) Brain asymmetry predicts suicide among navy alcohol abusers. Mil Med 146:277–278
Smith V, Chyatte C (1983) left-handed versus right-handed alcoholics: an examination of relapse patterns. J Stud Alcohol 44:553–555
Coren S, Searleman A, Porac C (1986) Rate of physical maturity and handedness. Dev Neuropsychol 2:17–23
Coren S (1989) Left-handedness and accident-related injury risk. Am J Public Health 79:1040–1041
Graham CJ (1995) Left-handedness as an injury risk factor in adolescents. J Adolesc Health 16:50–53
Taras J (1995) Left hand dominance and hand trauma. J Hand Surg 20A:1043–1045
World Health Organization (1992) International statistical classification of diseases and related health problems, 10th rev, vol 1. World Health Organization, Geneva
Racxkowski D, Kalat JW (1974) Reliability and validity of some handedness questionnaire items. Neuropsychologia 12:43–47
Annett M (2002) Human handedness, discrete types or continuous varieties. In: Annett M (ed) Handedness and brain symmetry: the right shift theory. Psychology Press, New York, pp 23–47
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Luetters, C.M., Kelsey, J.L., Keegan, T.H.M. et al. Left-handedness as a risk factor for fractures. Osteoporos Int 14, 918–922 (2003). https://doi.org/10.1007/s00198-003-1450-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-003-1450-z