
Abstract
Osteoporosis and fragility fractures are believed to be uncommon in Africa. To reevaluate this notion, we documented all patients aged 35 years and older admitted to the two main urban hospitals in Cameroon following a diagnosis of fracture during 2 years. Among 513 patients sustaining fractures (192 women, 321 men), 13.5% of all fractures in women occurred at the hip (n=26), 4.7% at the forearm (n=9), and 81.8% (n=157) at other sites (mainly tibia and femoral shaft). In men, the corresponding figures were 9% (n=29), 1.9% (n=6), and 89.1% (n=286). Of the hip and wrist fractures occurring in women, 80.0% were low energy trauma fractures due to falls, 8.6% were high-energy trauma fractures (road accidents), and 11.4% were undefined. In men, the corresponding figures were 42.9%, 34.3%, and 22.9%. Using the 1997 estimates of the population, the annual incidence rates of low-energy trauma fractures (per 100,000 persons over 35 years and above) were 4.1 in women, 2.2 in men for hip fractures, 1.2 in women, and 0.2 in men for wrist fractures. The pattern of most of the hip and wrist fractures in women is consistent with underlying bone fragility. The low incidence of fragility fractures is confirmed and is likely to be, in part, the result of reduced longevity as only 1.1% of women and 0.7% of men survive beyond 65 years of age.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of osteoporosis is high in developed countries [1, 2]. Thus, fragility fractures and the accompanying morbidity, mortality, and economic burden constitute a major public health problem [3, 4]. In Africa, osteoporosis is reported as being rare so that no preventive or curative measures are taken against the disease [5, 6]. The few studies of osteoporosis or fractures in Africa suggest fragility fractures are uncommon [5, 6, 7]. This disease has been neglected in sub-Saharan Africa in general, and in Cameroon in particular. Although measurements of bone mass cannot be readily performed, hip and wrist fractures are associated with osteoporosis in the elderly. As these endpoints of bone fragility can be reliably ascertained, we assessed the epidemiologic characteristics of hip and wrist fractures in Cameroon.
Materials and methods
This was a retrospective analysis of patients admitted with a diagnosis of fracture during 2 years from 5 August 1996 to 5 August 1998 to two hospitals, Central Hospital of Yaounde, the political capital, and Laquintinie Hospital of Douala, the economic capital of the country, a port town situated 240 km from Yaounde. Both hospitals were the biggest in their area and situated in the center of town serving the total cosmopolitan population from all social groups and all ages. We included all admitted patients with a main diagnosis of fracture. All patients aged 35 years and over with a medical report including age, sex, site of fracture, and the circumstances which lead to the fractures were documented. Hip and wrist fractures were confirmed by surgical and radiologic evidence. Patients lacking this information were excluded. A preestablished technical sheet was completed using data in the medical records. Data was obtained following the consent of the authorities of each hospital. Anonymity was preserved. The proportion of each type of fracture relative to age, sex, and the circumstances of occurrence were calculated. Mean ages of occurrence of hip and wrist fractures and their standard deviation were also calculated.
Fracture incidence was calculated for the total study population (age 35 years and over) and the two sexes separately (sex-specific incidence), and expressed as fractures/100,000 inhabitants/year. Age-specific incidence for age groups 35–49, 50–64, 65 and over was calculated and expressed as fractures/100,000 inhabitants/year. The number in various age groups was calculated using estimates from the 1997 National Statistics Report [8]. The total was estimated at 566,765 persons.
Results
All fractures
Eight patients with fractures were excluded for lack of data. Of the 513 fractures documented (192 in women, 321 in men), 259 (50.5%) occurred before 50 years of age and 254 (49.5%) after 50 years of age. In women, 83 (43.2%) occurred before, and 109 (56.8%) after 50 years of age. In men, the corresponding figures were 176 (54.8%) and 145 (45.2%). Six patients were above 85 years of age—four women and two men.
Hip and wrist fractures
There were 55 hip and 15 wrist fractures. Table 1 shows the distribution of subjects according age, sex, site and circumstance of fracture. Of the 55 patients (26 women, 29 men) presenting with hip fractures, 21 (38.2%) were trochanteric and 34 (61.8%) were cervical.
Of the 26 hip fractures in women 23 (88.5%) occurred after the age of 50 years; and 10 (38.5%) were trochanteric, 16 (61.5%) cervical. The overall mean age of occurrence of hip fractures (± SD) was 68 ±13.3 years, and 72.6 ±9.4 years when only those occurring following low energy trauma were considered. The incidence of low-energy hip fractures increased steeply with age from zero, before 50 years, to 24.4 per 100,000 persons per year after age 65 years (Table 2).
In the 29 men, 17 (58.6%) of the hip fractures occurred after the age of 50 years; 11 (38%) were trochanteric and 18 (62%) were cervical. The incidence of low energy hip fractures increased with age rising from zero before age 50 years to 20.7 per 100,000 per year after the age of 65 years (Table 2). The overall mean age of hip fractures in men was 54.8 ±12.1 and 66.2 ±5.8 years when only those due to low energy-trauma were considered.
There were 15 wrist fractures (9 women, 6 men) (Table 1). In women, 7 (77.7%) occurred after 50 years of age. In men, 5 (83.3%) occurred before age 50 years with no increase in incidence with age (Table 2).
Before 50 years of age, most hip and wrist fractures were traumatic; of the 22 hip and wrist fractures, 12 (54.5%) were due to high-energy trauma (road accidents), 1 low energy, 9 unknown. Other "traumatic" fractures included fights and blows from a cutlass (for wrist fractures). For patients after the age of 50 years, of the 48 hip and wrist fractures, 42 (87.5%) were the result of low energy trauma due to falls, 2 were high trauma fractures, 1 was unknown (Table 1). In 17.1% of all hip and wrist fracture cases, no reason for fracture was documented. In women, falls accounted for 80.0% (28/35) of all hip and wrist fractures. In men, falls were also the most important cause of these fractures (42.8%), but high-energy fractures were common (37.1%) especially below 50 years.
Other fractures
As shown in Table 1, 157 women and 286 men had fractures other than hip and forearm fractures. The most frequent type included tibia (and fibula) (36.1%) and femoral shaft (33.0%). In women, fractures occurred equally before 50 years of age (49.7%) and after (51.3%). In men, 55.6% occurred before 50 years of age. These fractures were mostly due to high trauma.
Discussion
The incidence of fracture is more devastating in black than white women with a higher mortality and disability rate [9]. In metropolitan Cameroon, central Africa, among persons over 35 years, fractures were more common in men than women. In women, most fractures occurred after 50 years of age while in men, over half occurred before 50 years of age. This pattern is similar to that found in Western countries [10]. In women, most hip and wrist fractures occurred after 50 years of age. In men, about half occurred before 50 years. For men and women younger than 50 years, severe trauma was the most common cause of the hip and wrist fractures. After 50 years of age, 90% of the fractures in women and 83.3% in men were fragility fractures associated with falls. For people aged 35 and above, these hip and wrist fractures were the third most common cause of admission for fractures after tibia and femoral shaft fractures. About 10% of all fractures in this age group were low energy hip or wrist fracture consistent with the view that bone fragility is likely to be a problem in Cameroon.
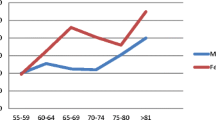
To the best of our knowledge this is the first study describing fragility fractures in sub-Saharan African. In early studies, Aspray et al. reported no minimal trauma fractures in rural Gambia [6]. Adebajo et al., describing fractures of the hip and distal forearm in western Africa, found no evidence of an age-related increase in the rates of hip and distal forearm in women [5]. Draw on a logarithmic scale, the rising incidence of hip fractures for people up to 65 years of age was parallel to that seen in other countries and increases as age advanced, consistent with underlying bone fragility (Fig. 1 and 2). Although risk factors for falls and osteoporosis, such as low calcium intake, multiple pregnancies, and prolonged breastfeeding are common, the incidence of hip and wrist fractures was one or two orders of magnitude lower than in Western or Asian countries. Nevertheless, these figures are the highest recorded in sub-Saharan Africa.

The age-specific incidence (linearized on a logarithm scale) of hip fractures in women, by country. Asterisk indicates incidence for 65 years of age and over; plus indicates incidence for 80 years of age and over. a Loftus et al. [18], b Sanders et al. [19], c Lau et al.[20], and d Adebajo et al. [5]

The age-specific incidence (linearized on a logarithm scale) of hip fractures in men, by country. Asterisk indicates incidence for 65 years of age and over; plus indicates incidence for 80 years of age and over. a Loftus et al. [18], b Sanders et al. [19], c Lau et al. [20], and d Adebajo et al. [5]
Even for people under age 50 (Fig. 1 and 2), the incidence of hip fractures differed from country to country, and these relative differences remained parallel suggesting that a reduced peak bone density at maturity may contribute to fractures in old age.
The incidence of wrist fractures reported in this study was low compared with Western countries [11]. In a previous study in Africa, Adebajo et al. reported an annual incidence per 100,000 persons of 1.9 in women over 50 years, and 2.3 in men over 50 years [5].
Even if ascertainment errors resulted in an underestimate of the numbers of fractures, the incidence in the present study is still unlikely to make rates comparable to those reported in other countries. The most important reason for this is probably reduced longevity. We have no evidence of a higher bone density among Africans. BMC is lower in rural Gambian women [6]. In Cameroon and other sub-Saharan African countries, about 40% of the population is less than 15 years of age, while less than 3% is over 65. The mean age in metropolitan Cameroon is 20.7 years [8]. The life expectancy in Cameroon is 57 years compared to 82 years in Japan [8, 12]. The low mean age of low-energy trauma hip fractures (72.6 years of age in women, 66.2 in men) may also be due to this short life expectancy.
Given the parallel increment in hip fracture incidence before the age of 65 years, as life span increases in Cameroon, it is likely that the incidence of fractures will increase. In Finland, life span has risen in men from 53 years in 1970 to 69 years in 1991 with a commensurate increase in fracture incidence [13]. Westernization with changing lifestyles may also result in an increase in fracture incidence. Worldwide projections suggest a huge increase in fractures rates in developing countries and Africa. The higher incidence we report in this study will shift these estimates [14]. In contrast to the previous studies, more fractures should be expected in women compared with men.
A substantial proportion of hip and wrist fractures were associated with severe trauma, mainly road accidents. However, this does not exclude osteoporosis as contributing to these fractures as patients with fractures due to trauma may also have reduced bone density [15].
Several methodological issues arise from this study. Not all persons with fractures have access to hospitals and the many other hospitals in these regions are difficult to survey. Many cases of fractures may have been misclassified or not reported in the discharge file. Xu et al. in Beijing found that 70% of intertrochanteric hip fractures were miscoded as other femoral fractures [16]. Elffors et al. reported that the final estimate of the hip fracture incidence could result in an underestimate or overestimate ranging from 15% lower to 89% higher than the estimated incidence based on the discharge diagnoses alone [17].In developing countries like Cameroon, because of inadequate infrastructures and lack of motivation of health care workers due to low salaries, this problem is important and many medical files are incomplete.
It was not possible to estimate the number of fractures unreported in the discharge files. However, 1.5% of files could not be used and in 17.2% of cases we could not document the possible cause of the fracture. The population is poor and there is no health insurance program so many individuals can not afford to pay the cost of treatment for fractures and therefore many do not reach hospitals. Among those reaching the hospital, it is likely that a substantial number of patients with forearm fractures refused admission could have been missed. This is unlikely for hip fractures given the seriousness of this accident. Finally, many fractures due to minimal trauma are attributed to witchcraft by a superstitious traditional population and brought to traditional clinics.
The characteristics of hip and wrist fractures described in this study suggest that fragility fractures occur in Africa, although substantially less frequently than in most other countries. The low fragility fracture rates are most likely the result of reduced longevity and underreporting. Studies are needed to increase awareness of this disease in sub-Saharan Africa and to monitor the epidemiology of fractures as longevity improves.
References
Bonjour JP, Burckhardt P, DambaCher M, Kraenzlin ME, Wimpfamer C (1997) Epidemiology of osteoporosis. Schweiz Med Wochenschr 127(16):659–667
Christiansen C (1993) Skeletal osteoporosis. J Bone Miner Res 8(2):S475–S840
Carter J, Eisman J (1997) The epidemiology and pathogenesis of osteoporosis. Bailleres Clin Endocrinol Metab 11(1):23–32
Samsioe G. (1997) Osteoporosis an update Acta Obstet Gynecol Scand 76(3):189–199
Adebajo AO, Cooper C, Grimley EJ (1997) Fractures of the hip and distal forearm in West Africa and the United Kingdom. Age Ageing 20:435–438
Aspray TJ, Prentice A, Timothy JC, Yankuba S, Reeve J, Roger MF (1996) Low bone mineral content is common but osteoporotic fractures are rare in the elderly rural Gambian women. J Bone Miner Res 11(7):1009–1025
Solomon L (1968) Osteoporosis and fracture of femoral neck in the South African Bantu. J Bone Surg 50B:2–13
Annuaire Statistique National, République du Cameroun. Année 1997
Wong PCN (1966) Fracture epidemiology in a mixed Southeastern Asian community (Singapore). Clin Orthop 45:55–61
Kanis JA, Pitt FA (1992) Epidemiology of osteoporosis. Bone 13(1):S7–S15
Melton LJ III, Amadio PC, Crowson CS, O'fallon WM (1998) Long-term trends in the incidence of distal forearm fractures. Osteoporos Int 8:341–348
Hagino H, Yamamoto H, Nakamura H, Kishimoto T (1989) Changing incidence of hip, distal radius, and proximal humerus fractures in Tottori Prefecture, Japan. Bone 24(3):265–270
Kannus P, Parkkari J, Sievanen H, Heinonen A, Jarvinen M (1996) Epidemiology of hip fractures. Bone 18(1):S57-S63
Cooper C, Campion G, Melton LJ III (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 285–289
Sanders KM, Pasco JA, Ugoni AM, et al. (1998) The exclusion of high trauma fractures may underestimate the prevalence of bone fragility fractures in the community: the Geelong Osteoporosis Study. J Bone Miner Res Aug 13(8):1337–1342
Xu L, Lu A, Zhao X, Chen X, Cummunigs SR (1996) Very low rates of hip fractures in Beijing, People's Republic of China. The Beijing Osteoporosis Project. Am J Epidemiol. 144(9):901–907
Elffors L, Allander E, Kanis JA, Gullerg B, Johnell O, Dequeker J (1994) The variable incidence of hip fracture in southern Europe. The MEDOS study. Osteoporos Int 4:253–263
Loftus CM, Osnes EK, Falch JA, et al. (2001) Epidemiology of hip fractures in Oslo, Norway. Bone 29:413–418
Sanders KM, Seeman E, Ugoni AM, et al. (1999) Age- and gender-specific rate of fractures in Australia: a population-based study. Osteoporos Int 10:240–247
Lau EMC, Lee JK, Suriwongpaisal P, Saw SM, Das De S, Khir A, Sambrook P (2001) The incidence of hip fractures in four Asian countries: the Asian Osteoporosis Study (AOS). Osteoporos Int 12:239–243
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zebaze, R.M.D., Seeman, E. Epidemiology of hip and wrist fractures in Cameroon, Africa. Osteoporos Int 14, 301–305 (2003). https://doi.org/10.1007/s00198-002-1356-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-002-1356-1