
Abstract
Introduction and hypothesis
The opioid epidemic is a recent focus of national initiatives to reduce opioid misuse and related addiction. As interstitial cystitis (IC) is a chronic pain state at risk for narcotic use, we sought to assess opioid prescription use in patients with IC.
Methods
Data were accessed from the Virginia All Payers Claims Database. We identified female patients diagnosed with IC from 2011 to 2016 using International Classification of Disease codes. A patient identifier was used to link diagnoses with outpatient prescription claims for opioids using generic product identifiers. We then analyzed opioid prescriptions within 30 days of a claim with a diagnosis of IC.
Results
A total of 6,884 patients with an IC diagnosis were identified. The median number of IC claims per patient was 2 (IQR 1 to 4). Mean patient age was 47.8. Twenty-eight percent of patients received at least 1 opioid prescription, with a median of 2 (IQR 1, 4) per patient. Among those receiving opioids, 185 (9.5%) had more than 10 opioid prescriptions, with a maximum of 129. The most common prescriptions were hydrocodone (n = 2,641, 32.3%), oxycodone (n = 2,545, 31.2%), and tramadol (n = 1,195, 14.6%). There was a decline in opioid prescriptions per month for IC, although the rate per IC diagnosis remained stable.
Conclusions
A significant number of patients with IC are treated with opioids. Although the overall number of opioid prescriptions associated with IC had declined, the prescription rate per IC diagnosis had not. As part of the national initiative to reduce opioid use, our data suggest that IC treatment strategies should be examined.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 2017, the Department of Health and Human Services declared opioid abuse a national emergency in response to dramatically increasing opioid addiction and overdose rates [1]. As a result, a significant focus has been placed on understanding trends contributing to opioid addiction and overuse. Accordingly, the common practice of treating chronic noncancer pain with opioids has been identified as a significant factor underlying increased opioid use. Large-scale study shows that moderate or severe chronic pain afflicts nearly 19% of adult Europeans [2]. Additional data demonstrate that up to 30% of patients with chronic pain receive opioids [3]. Even so, a relatively small amount of focus has been placed on chronic urological disease that may contribute to overall opioid use. In a previously described study on the prevalence of chronic pain, the cause of chronic pain in the vast majority of respondents related rather to orthopedic conditions, including arthritis and spine/back disorders [3].
Interstitial cystitis (IC), or bladder pain syndrome, is a disorder well known to both urologists and gynecologists and is characterized, in part, by chronic pain [4]. Accordingly, patients with IC are at risk for long-term opioid use. Although orthopedic and musculoskeletal conditions described previously have been often emphasized in national conversations regarding outpatient opioid use, it is increasingly important that physicians across all specialties examine their role as prescribers and related conditions that place patients at risk for opioid overuse. Within the urological community, efforts have largely focused on opioid use in the perioperative setting [5]. In contrast, there is a lack of published literature to understand the prevalence of opioid use in chronic urological disorders of pain, including IC. Accordingly, we performed a population-based outpatient analysis to quantify and characterize recent opioid use in patients diagnosed with IC. We placed specific focus on both overall opioid use per patient and also the quantity of opioid use per patient encounter. Our aim was to gain initial insight into the degree of opioid use associated with IC, which is an important step toward the larger goal of preventing potential opioid overuse in this patient population.
Materials and methods
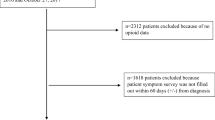
Following institutional review board approval (protocol #20800), we obtained data from the Virginia All Payer Claims Database (VAPCD) from 2011 until 2016. This database includes medical and pharmacy claims from state residents insured through Medicare, Medicaid, and private commercial insurers. A flowchart detailing patient selection and exclusion is provided in Fig. 1. Accordingly, we identified female patients 15 years or older with a diagnosis of IC based on International Classification of Disease (ICD) 9th or 10th generation codes 595.1 and N30.10 respectively. A patient identifier was then used to link these codes with outpatient prescription claims for opioids by using generic product identifiers. Inpatient opioid prescriptions were excluded. For our analysis, we considered an outpatient opioid prescription to be associated with IC if it was prescribed within 30 days of an IC diagnosis claim.

Flowchart of patient selection and exclusion
Cumulative diagnoses of IC during the study period and outpatient opioid prescriptions were assessed. Specific focus was placed on the rate of IC diagnoses and prescriptions over the study period as assessed on a monthly basis. Analysis was performed to assess for trends in opioid use over time by patients with IC, as well as opioid prescriptions associated with each IC patient visit. Additional focus was placed on the type and quantity of opioid prescriptions. A t test was used to compare the age of patients who received opioids and those who did not, with p < 0.05 (two-tailed) considered statistically significant. The R® programming language, version 3.5.2, was used for all analyses.
Results
A total of 6,884 patients were identified with at least one IC diagnosis, with 31,518 total IC diagnoses assigned. Accordingly, over the study period, patients with IC were evaluated a median of 2 (IQR 1, 4; range 1–250) times for a related diagnosis of IC. A total of 8,166 opioid prescriptions were prescribed within 30 days of an IC diagnosis during the study period. The mean patient age was 47.8 (95% confidence interval [CI] 47.6–47.9) years.
Figure 2 demonstrates the number of monthly IC diagnoses and related opioid prescriptions over the study period. In general, a decreased rate of IC diagnoses and related opioid prescriptions were seen. The monthly rate of the opioid prescriptions per IC diagnosis and patient is shown in Fig. 3. Although some degree of rate variance was seen, overall, this rate remained largely unchanged throughout the study. The mean age of IC patients who received at least one opioid prescription was younger (43.8 years) than that of patients who did not (47.2 years; p < 0.0001).

Monthly interstitial cystitis diagnoses and related opioid prescriptions. Monthly interstitial cystitis diagnoses (dotted line, top); monthly opioid prescriptions (solid line, bottom). Rx prescriptions, Dx diagnosis

Monthly rate of opioid prescriptions a per interstitial cystitis diagnosis and b per patient
Among patients identified with IC, 1,944 (28%) had at least one opioid prescription, with 1.19 opioids prescribed per patient with IC over the entire cohort. Each time an IC diagnosis was assigned, there was an opioid associated in 26% of cases. Figure 4 illustrates the distribution of a number of total opioid prescriptions per patient. A median of 2 prescriptions (IQR 1,4) per patient with IC was seen. Notably, 185 (9.5%) patients received more than 10 opioid prescriptions, with a maximum prescription number of 129.

Distribution of total opioid prescriptions received by interstitial cystitis patients
Table 1 demonstrates the types of opioids prescribed. The most common prescriptions were hydrocodone (n = 2,641, 32.3%), oxycodone (n = 2,545, 31.2%), and tramadol (n = 1,195, 14.6%). In addition, a smaller number of prescriptions for methadone (n = 101, 1.2%) and buprenorphine (n = 96, 1.2%) were associated with IC diagnosis.
Discussion
Interstitial cystitis is an often debilitating and refractory chronic pain condition estimated to afflict between 4 and 12 million people in the USA [6]. Despite nationwide concerted efforts over the past decade by groups such as the Multidisciplinary Approach to Study of Chronic Pelvic Pain (MAPP) Research Network, both our understanding of the disease and a generally effective therapy remain limited [7]. The AUA 2014 guideline on IC lists opioids as a second-line therapy when part of a multimodal regimen. Even so, there is limited high-level evidence to support that opioid therapy in this patient population provides sustained benefits for pain and functioning [4, 8]. Accordingly, The Royal College of Obstetrics and Gynecology and British Society of Urogynecology 2016 joint guideline on bladder pain syndrome recommends minimizing opioid use and early referral to a pain center for those with refractory symptoms [9].
This study details the use of opioid prescriptions in patients with IC in Virginia from 2011 to 2016, during the height of the national opioid epidemic. Given the aforementioned paucity of research on opioid use in urological pain disorders, we believe that our data provide an important initial step towards understanding how IC may contribute to the opioid crisis. Our analysis reveals several notable findings.
First, our data demonstrate that a significant number of patients with IC receive opioid prescriptions, with 28% of patients in the cohort receiving at least one throughout the study period. This rate is consistent with a recent study using patient-reported metrics demonstrating that 35% of patients report opioid use for symptom flares related to IC and chronic bladder pain [10]. To our knowledge, there are no other recent studies that quantify generalized outpatient opioid use in IC, with available investigations focused rather on reductions in opioid use following other intervention (e.g., cystectomy) [11].
Related insight is available through investigation on pelvic pain syndrome reported in gynecological literature. Accordingly, Madsen et al. surveyed obstetricians and gynecologists on their opioid prescribing patterns and found that 18% reported regularly prescribing opioids to patients with chronic pelvic pain of unknown origin [12]. Similarly, Cichowski and colleagues demonstrated that 16% of women with chronic pelvic pain used opioids in a study of female patients in the Veteran’s Administration system [13].
A second notable finding of the present study is the significant proportion of outpatient encounters associated with an opioid prescription (26%). Although many patients received opioids, the number of prescriptions per patient was generally low (median of two). These data are most consistent with the use of opioids for symptom flares. That said, a significant subset (9.6%) did receive ten or more prescriptions, with a maximum of 129 prescriptions, suggesting long-term daily maintenance opioid use in these patients. In addition, we analyzed long-acting formulations, such as methadone, as it was believed that this may reflect patients being treated for opioid addiction. Overall, these formulations accounted for a small percentage of opioids prescribed. Certainly, these data may be influenced by the limitations inherent to health claims and it is likely that additional opioid prescriptions associated with other diagnoses are not captured.
The opioid crisis has stimulated a nationwide effort focused on initiatives and guidelines to help to address opioid overuse and addiction. Accordingly, The 2016 Center for Disease Control guideline for prescribing opioids for chronic pain provides education and tools to guide clinicians in the responsible use of opioids [14]. This guideline has been accompanied by those of numerous specialty societies that generally agree on certain pain treatment strategies, including dosing thresholds, attention to drug–drug interactions, and the use of risk assessment tools [14]. Finally, individualized efforts have been undertaken by all 50 states and the District of Columbia and include initiatives to educate the public and providers, expanding access to naloxone, and requirements for provider use of prescription monitoring programs [15].
The American Urological Association (AUA) has worked to raise awareness and spearhead efforts to mitigate the opioid crisis and facilitate the responsible use of opioids by urologists [16]. To date, a significant portion of urological efforts have been focused on the perioperative setting, with comparatively less focus on research and initiatives addressing urological chronic pain conditions [5, 17, 18]. Accordingly, we suggest additional focus on research to quantify and characterize the use of opioids in the treatment of urological chronic pain conditions. Our study provides an initial step towards this goal. Further, we believe that additional research is needed to assess both the efficacy and the role of opioids in IC. Highlighting the paucity of research specific to opioid use in IC is a meta-analysis by Busse and colleagues that included a systematic review of randomized clinical trials of opioids for chronic noncancer pain [19]. The vast majority of the 42 high-quality trials included focus on pain to the back or knee and underlying etiologies such as arthritis and diabetic neuropathy. In contrast, no focused study on IC or urological etiology was presented. In addition, subsequent research focused on optimizing non-opioid-based management of IC is needed. Multidisciplinary pelvic and urological pain clinics promoting a multimodal and holistic approach are reported and it is important to understand whether lower opioid-prescribing rates are associated with this approach [20].
Underscoring the importance of such urological research is our finding that, although the absolute number of opioid prescriptions declined after 2011, the rates of prescriptions per diagnosis code and per patient remained constant. In contrast, as a result of the widespread efforts described above, nationwide opioid-prescribing rates have begun to decline [21]. Further, in Virginia, the number of opioid prescriptions has declined from a peak of 79.6 per 100 people in 2012 to 52.9 in 2017 [21]. The absence of similar trends in patients with IC in Virginia highlights the need for further focused investigation and initiatives.
The scale and severity of the US opioid crisis is unique, but similar trends of rising opioid use and misuse have been noted internationally [22]. This is reflected in a Dutch study published this year demonstrating tripled rates of hospitalization for opioid overdose between 2008 and 2017 [23]. The authors opine that evidence-based guidelines for opioid prescribing are paramount to preventing escalation to overuse to the degree found in the USA.
Limitations of this study include the absence of clinical detail in the VAPCD, preventing our understanding of information such as provider specialty and prescription quantity (e.g., morphine equivalents). Second, as we included prescriptions provided within 30 days of the outpatient encounter, it is possible that some of these were associated with a separate diagnosis. This was done to avoid under-capturing prescriptions that can occur as a result of the VACPD methodology, which can include a delay in the prescription date compared with the visit date. Further, generalizability may be limited, as the database is limited to Virginia state residents. Finally, we were unable to comprehensively assess the considerable number of comorbidities that can serve as confounders for opioid use. Nonetheless, the association between IC and comorbid disease associated with pain is well established [24]. Although further research is needed to more specifically analyze drivers of opioid use in patients with IC and other comorbidities, we believe that our study provides an important initial step towards quantifying opioid use related to IC and how this disorder may have an impact on national efforts to decrease opioid use and addiction.
Conclusions
A significant number of patients with IC are treated with opioids. Although the overall number of opioid prescriptions associated with IC in Virginia has declined between 2011 and 2016, the prescription rate per IC diagnosis has not. As part of the national initiative to reduce opioid use, our data suggest that IC treatment strategies should be examined.
References
Department of Health and Human Sources HHS Acting Secretary Declares Public Health Emergency to Address National Opioid Crisis. 2017. https://www.hhs.gov/about/news/2017/10/26/hhs-acting-secretary-declares-public-health-emergency-address-national-opioid-crisis.html. Accessed 8 May 2019.
Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10:287–333. https://doi.org/10.1016/j.ejpain.2005.06.009.
Dembe A, Wickizer T, Sieck C, et al. Opioid use and dosing in the workers’ compensation setting. A comparative review and new data from Ohio. Am J Ind Med. 2012;55:313–24. https://doi.org/10.1002/ajim.21021.
Hanno PM, Erickson D, Moldwin R, Faraday MM. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J Urol. 2015;193:1545–53. https://doi.org/10.1016/j.juro.2015.01.086.
McGovern FJ, Lieberman GM, Xu R, Anderson TA. The opioid epidemic: urology’s role in solving the crisis. AUA Update Series. 2018;37:337–50.
IC Association. 4 to 12 million may have IC. IC Association. 2015. https://www.ichelp.org/about-ic/what-is-interstitial-cystitis/4-to-12-million-may-have-ic/. Accessed 8 May 2019.
Clemens JQ, Mullins C, Kusek JW, et al. The MAPP research network: a novel study of urologic chronic pelvic pain syndromes. BMC Urol. 2014;14:57. https://doi.org/10.1186/1471-2490-14-57.
Nickel JC. Opioids for chronic prostatitis and interstitial cystitis: lessons learned from the 11th World Congress on Pain. Urology. 2006;68:697–701. https://doi.org/10.1016/j.urology.2006.04.013.
Tirlapur S, Birch J, Carberry C, et al. Management of bladder pain syndrome. BJOG. 2016;124:e46–72. https://doi.org/10.1111/1471-0528.14310.
Lai HH, Vetter J, Song J, et al. Management of symptom flares and patient-reported flare triggers in interstitial cystitis/bladder pain syndrome (IC/BPS)—findings from one site of the MAPP research network. Urology. 2019;126:24–33. https://doi.org/10.1016/j.urology.2019.01.012.
Koslov DS, Vilson F, Colaco M, et al. Impact of cystectomy with urinary diversion upon tracked receipt of opioid prescriptions among patients with interstitial cystitis/bladder pain syndrome. Urology. 2018;114:83–6. https://doi.org/10.1016/j.urology.2017.11.009.
Madsen AM, Stark LM, Has P, et al. Opioid knowledge and prescribing practices among obstetrician-gynecologists. Obstet Gynecol. 2018;131:150–7. https://doi.org/10.1097/AOG.0000000000002407.
Cichowski SB, Rogers RG, Komesu Y, et al. A 10-yr analysis of chronic pelvic pain and chronic opioid therapy in the women veteran population. Mil Med. 2018;183:e635–40. https://doi.org/10.1093/milmed/usy114.
Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016.[erratum appears in MMWR Recomm Rep. 2016;65(11):295]. Morb Mortal Wkly Rep Recomm Rep. 2016;65:1–49. https://doi.org/10.15585/mmwr.rr6501e1.
Wickramatilake S, Zur J, Mulvaney-Day N, et al. How states are tackling the opioid crisis. Public Health Rep. 2017;132:171–9. https://doi.org/10.1177/0033354916688206.
AUA Position Statement: Opioid Use. https://www.auanet.org/guidelines/opioid-use. Accessed 5 July 2019.
Theisen KM, Myrga JM, Hale N, et al. Excessive opioid prescribing after major urologic procedures. Urology. 2018;123:101–7. https://doi.org/10.1016/j.urology.2018.06.057.
Shah AS, Blackwell RH, Kuo PC, Gupta GN. Rates and risk factors for opioid dependence and overdose after urological surgery. J Urol. 2017;198:1130–6. https://doi.org/10.1016/j.juro.2017.05.037.
Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320:2448–60. https://doi.org/10.1001/jama.2018.18472.
Gupta P, Gaines N, Sirls LT, Peters KM. A multidisciplinary approach to the evaluation and management of interstitial cystitis/bladder pain syndrome: an ideal model of care. Transl Androl Urol. 2015;4:611–9. https://doi.org/10.3978/j.issn.2223-4683.2015.10.10.
Centers for Disease Control and Prevention. U.S. Opioid Prescribing Rate Maps. 2018. https://www.cdc.gov/drugoverdose/maps/rxrate-maps.html. Accessed 8 May 2019.
Van Amsterdam J, van den Brink W. The misuse of prescription opioids: a threat for Europe? Curr Drug Abuse Rev. 2015;8:3–14. https://doi.org/10.2174/187447370801150611184218.
Kalkman GA, Kramers C, van Dongen RT, et al. Trends in use and misuse of opioids in the Netherlands: a retrospective, multi-source database study. Lancet Public Health. 2019;4:e498–505. https://doi.org/10.1016/S2468-2667(19)30128-8.
Rodríguez MÁB, Afari N, Buchwald DS. Evidence for overlap between urological and nonurological unexplained clinical conditions. J Urol. 2009;182:2123–31. https://doi.org/10.1016/j.juro.2009.07.036.
Author information
Authors and Affiliations
Contributions
JZ: project development, data analysis, manuscript writing; MBC: project development, data analysis and collection, manuscript writing; CWP: project development, data analysis and collection, manuscript editing; DER: project development, data analysis, manuscript writing/editing.
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zillioux, J., Clements, M., Pike, C.W. et al. Opioid prescription use in patients with interstitial cystitis. Int Urogynecol J 31, 1215–1220 (2020). https://doi.org/10.1007/s00192-019-04214-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-019-04214-2